
Abstract

“Which came first, the phoenix or the flame?” . . . “Well then, I think the answer is that a circle has no beginning.” “Well reasoned,” said the voice, and the door swung open.
The number of people suffering from atherosclerosis-related complications such as peripheral artery disease (PAD) is increasing exponentially, and it is estimated that PAD affects up to 10% of the general population. Of course, only a subset of patients with PAD experiences the typical symptoms of claudication, whereas the vast majority of cases remain asymptomatic and often undetected for a long time. In fact, PAD is rarely diagnosed or risk-stratified in a primary health care setting. This amounts to a sorely missed opportunity for risk factor modification and prevention efforts. Moreover, patients with PAD have an increased probability of suffering eventually from critical limb ischemia, which has a major impact on quality of life and health care expenditures, may require lower extremity amputation, and may carry the risk of life-threatening complications. The latest American College of Cardiology/America Heart Association guidelines suggest considering revascularization procedures, including bypass surgery and percutaneous transluminal angioplasty, well before amputation, as this is not yet the case in all patients. 1 To date, percutaneous transluminal angioplasty or other endovascular procedures remain the most frequent treatment compared to conventional surgery because patients with critical limb ischemia are often burdened by greater comorbidity and advanced age. 2
Atherosclerosis, thrombosis, and the conundrum arising from their combination are the underlying mechanisms for the development of PAD in most patients, as well as the ensuing vascular events, with a common pathophysiological link in inflammation (Figure 1). The pivotal role of inflammatory responses in cardiovascular disease began to emerge several decades ago, remaining at the core of the debate in several cardiovascular settings, such as atherosclerosis, myocardial infarction, myocardial hypertrophy, and vascular diseases.3,4 Several studies have subsequently highlighted the role of inflammatory mediators or markers, such as interleukin 1 (IL-1) and C-reactive protein (CRP), in the development and progression of atherosclerotic plaques, leading to ominous clinical conditions, such as myocardial infarction and heart failure. In fact, although an inflammatory response is the first-line defense against infection and facilitates tissue repair, it may also become a mechanism of progressive injury, impaired healing, and extensive chronic disease. It is likewise well known that inflammation contributes to all phases of the atherothrombotic process and that patients with elevated inflammatory biomarkers have increased vascular risk. 5
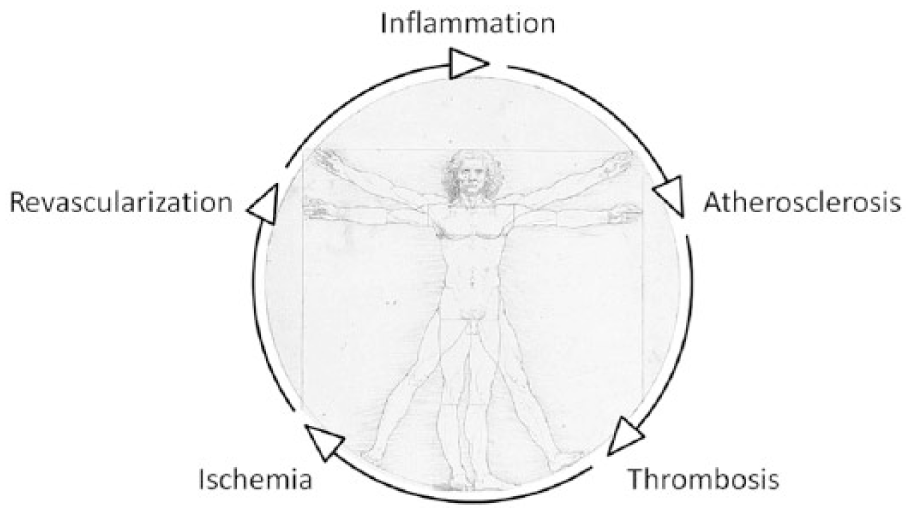
Diagram highlighting the recursive interplay between inflammation, atherosclerosis, thrombosis, ischemia, and revascularization in patients with peripheral artery disease.
Measurement of CRP is a validated method to identify individuals at high risk for both first and recurrent cardiovascular events even in the absence of major risk factors such as dyslipidemia. 6 This holds even truer in subjects with acute coronary syndromes. 7 Moreover, CRP has an important clinical predictive role for postinfarction complications, such as ventricular remodeling, heart failure, and sudden death. 8
Atherosclerosis and inflammatory processes leading to stenosis, embolism, or thrombus formation are the basis for PAD, and CRP is a crucial marker also involved in these clinical phenomena. Moreover, CRP might be useful in predicting the biological and clinical response to revascularization procedures for PAD. 9 Indeed, in this issue of the JEVT, Bleda et al 10 provide incremental knowledge on this important issue by appraising the predictive role CRP has on outcomes following lower extremity endovascular therapy in patients with PAD. In addition, they strive to identify a CRP cutoff that may be useful in identifying patients with a higher risk of failure 1 year after the index procedure. Indeed, in light of the high incidence of restenosis after balloon angioplasty or bare metal stenting, a key issue is to identify those patients who may derive greater benefit from an endovascular procedure. 11 The results provided by Bleda and coworkers show that the baseline CRP level can predict the need for secondary intervention at 1 year and that the CRP value at 1 month had a strong association with the 1-year rate of revascularization. These data also support the hypothesis that systemic inflammation is involved in the pathogenesis of postangioplasty restenosis. However, if it is now demonstrated that inflammation contributes to all phases of the atherothrombotic process and patients with elevated inflammatory biomarkers have increased vascular risk, it remains unclear whether direct inhibition of inflammation, as well as modulation of the redox state, 12 can reduce cardiovascular event rates.
Several clinical trials have investigated the potential effect of anti-inflammatory drugs in slowing the progression of atherosclerosis. Statins are the most widely prescribed drugs worldwide for lowering blood cholesterol levels. This class of drugs reduces synthesis of cholesterol in the liver by competitively inhibiting 3-hydroxy-3-methylglutaryl coenzyme A reductase activity. Apart from the reduction of low-density lipoproteins, statins have demonstrated several pleiotropic effects that result from cholesterol-independent mechanisms. These effects include improvement of endothelial dysfunction, decreased oxidative stress, stabilization of atherosclerotic plaque, modulation of platelet function and smooth muscle cell proliferation, and inhibition of inflammatory responses. 13
In support of the inflammatory hypothesis of atherothrombosis, the JUPITER (Justification for Use of statins in Prevention: an Intervention Trial Evaluating Rosuvastatin) trial also showed that the absolute vascular risk reduction associated with rosuvastatin increased with higher levels of baseline CRP but not with higher levels of low-density lipoprotein. 14 In addition to CRP, a large number of studies have shown that other mediators of inflammation are directly involved in the progression of atherosclerosis. In particular, IL-1, a central mediator in the local and systemic inflammatory response, seems to play a central role in vascular biology and is strictly implicated in atherothrombosis. 15 Accordingly, the use of IL-1 inhibition as a possible method to reduce vascular risk has recently generated considerable interest in the international scientific literature. The MRC-ILA Heart Study has been the first to show that the acute inflammatory response in acute coronary syndrome is IL-1–dependent and that it is modifiable by anakinra, a recombinant IL-1 receptor antagonist, the most widely used IL-1 blocker. 16 Canakinumab, a human monoclonal antibody that selectively neutralizes IL-1β and significantly reduces systemic CRP and other inflammatory biomarker levels, is the focus of the ongoing CANTOS trial, focusing on the long-term risk of recurrent myocardial infarction, stroke, and cardiovascular death among stable patients with coronary artery disease at high vascular risk (persistent levels of CRP >2 mg/L) despite contemporary secondary prevention therapy. 17 These studies, compounded by the pioneering efforts of the Virginia Commonwealth University Pauley Heart Center group to appraise the risk-benefit balance of inflammatory modulation in myocardial infarction and heart failure, have evolved a novel cytokine-based therapy for the secondary prevention of cardiovascular disease, including PAD.18-20
Antithrombotic therapy reduces the risk of cardiovascular events in PAD patients, although the optimal type, duration, and intensity of the antithrombotic regimen remain under debate. Awaiting novel trials on alternative regimens (eg, with novel oral anticoagulants, ticagrelor, or vorapaxar), dual antiplatelet therapy should be always considered after complex endovascular procedures, and it is likely (albeit not yet formally proven) that subjects with higher inflammatory burden are going to benefit from more intense and prolonged antiplatelet regimens.
The link between inflammation, oxidative stress, and the atherothrombotic process is surely a complex one. Atherosclerosis is a chronic inflammatory disease to be considered as the product of several concomitant interplays among different risk factors, such as genetic predisposition, hyperlipidemia, diabetes mellitus, smoking, and hypertension; repeated exacerbations of the inflammatory process within the atherosclerotic plaque may lead to plaque rupture with thrombosis and consequent clinical presentations, such as acute coronary syndrome or PAD. There are many inflammatory markers involved in this process, but at present none of them has emerged as clinically more useful than CRP to predict which patients are at high risk for cardiovascular events in general. Accordingly, and also thanks to the contribution by Bleda et al, 10 CRP emerges as a strong and independent predictor of adverse cardiac and vascular outcomes in patients with PAD.
In conclusion, the complex cascade represented by the intertwining effects of inflammation, atherosclerosis, thrombosis, ischemia, and the iatrogenic injury represented by the revascularization procedure and any indwelling device remains challenging for researchers as well as clinicians interested in PAD (Figure 1). Nonetheless, use of CRP for risk prognostication can guide us through this pathophysiological maze and pinpoint when and how to best use the most modern and potent antithrombotic and, in the near future, anti-inflammatory agents to improve the outlook of our patients with PAD.
Footnotes
Invited commentaries published in the Journal of Endovascular Therapy reflect the opinions of the author(s) and do not necessarily represent the views of the Journal, the