
Abstract
Keywords
Introduction
Research has shown that inflammatory processes are involved in the onset and progression of peripheral artery disease (PAD).1-3 In particular, high-sensitivity C-reactive protein (hsCRP), a surrogate of systemic inflammation, is a powerful marker of this atherosclerotic manifestation.4-7 Although endovascular therapy (EVT) is widely accepted as the first choice of treatment in many patients with PAD, there is uncertainty about the most cost-effective and definitive revascularization option for each individual patient. 8 Clinical data relating CRP to prognosis of EVT are sparse.9-11 Patients with high baseline CRP levels have a lower prognosis of a sustained good outcome after EVT, as well as an increased risk for reintervention or limb amputation. 9 However, there are no data determining the meaning of pre-EVT CRP levels or a threshold for this marker. It may be important to recognize patients in whom EVT will have a poorer prognosis and so stratify which of them would best be treated with EVT versus those better served with open bypass surgery. Therefore, we performed a prospective, single-center cohort study in PAD patients who underwent lower extremity EVT, evaluating the prognostic role of preprocedure CRP values in the risk of EVT failure at 1 year. The goal was to determine a CRP cutoff value with the highest sensitivity and specificity for determining potential EVT failure.
Methods
Study Design
This prospective, single-center cohort study enrolled symptomatic PAD patients who underwent EVT of de novo atherosclerotic lesions in the iliac, femoral, popliteal, or tibial arteries between January 2010 and December 2011. The study recruited patients for a derivation group between January 1, 2010 and June 30, 2011; a validation set was recruited between July 1, 2011 and December 31, 2011. Blood samples were collected before EVT and at 1 month after intervention in all patients to determine CRP levels.
A diagnosis of PAD was based on an ankle-brachial index (ABI) <0.9 or >1.3 and symptoms of intermittent claudication, pain at rest, and/or trophic lesions, according to TASC (TransAtlantic Inter-Society Consensus) guidelines. 12 ABI was measured at rest per the standard technique in the dorsalis pedis and posterior tibial arteries of both lower limbs. 13 To avoid potential confounding factors regarding variables association with CRP levels, patients who had clinical evidence of infection, including cellulitis, osteomyelitis, or deep space infection of the foot (Rutherford category 6), were excluded. Other exclusion criteria were concurrent systemic infections, inflammatory or autoimmune disease, fever, concurrent major hepatic and cancerous disease, immunosuppressive treatment, and acute myocardial infarction, stroke, and any major surgery or severe trauma 30 days before EVT. All patients included in the study provided their written informed consent. The study complied with the Declaration of Helsinki and was approved by the local ethics committee.
Patient Population
In the 2-year recruitment period, 398 patients underwent revascularization procedures for lower limb atherosclerotic lesions. Of these, 160 patients were excluded because they had bypass surgery. Of the 238 EVT patients, 35 were excluded because their ischemia was determined to be Rutherford category 6. Another 29 patients did not fulfill other inclusion criteria, leaving 174 patients (174 lower limbs) suitable for the study. Of these, 121 patients were included in the derivation set and 53 (39 men; mean age 70.1±10.0 years) in the validation set. Subject demographics and risk factor profiles are presented in Table 1. In the derivation set, the indication for revascularization was critical limb ischemia (Rutherford categories 4 and 5) in 94 (77.7%) subjects and intermittent claudication (Rutherford category 3) in 27 (22.3%). The distribution of target lesions included the iliac artery (n=31, 25.6%), superficial femoral artery (n=44, 36.4%), popliteal artery (n=5, 4.1%), infragenicular arteries (n=12, 9.9%), and multiple segments (n=29, 24%).
Baseline Characteristics and Demographic Features of the Study Population in the Derivation and Validation Sets. a
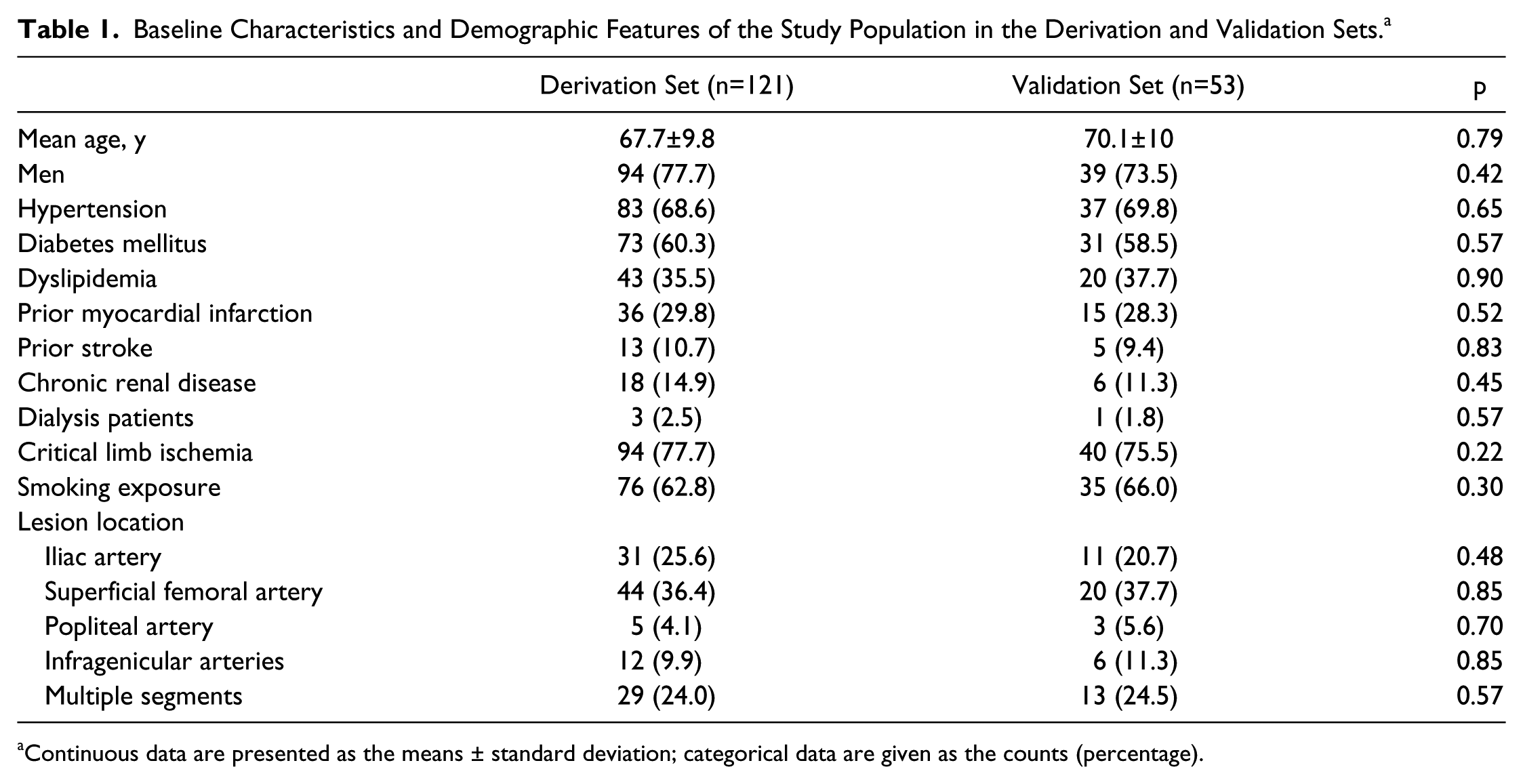
Continuous data are presented as the means ± standard deviation; categorical data are given as the counts (percentage).
Endovascular Therapy Procedure
Angioplasty was performed via a femoral access, and patients received heparin intra-arterially after sheath introduction. Primary stenting was performed in the iliac arteries. 12 Lesions in the infrainguinal arteries were treated with standard balloon angioplasty. Patients with suboptimal results, defined as flow-limiting dissection or residual stenosis >30%, underwent provisional stenting. Immediate technical success was defined as residual stenosis <30%. All patients were begun on a single antiplatelet regimen (aspirin 100 mg/d or clopidogrel 75 mg/d) and statins after EVT for life.
Data Collection, Definitions, and Follow-up
Cardiovascular risk factors and other pertinent data were collected from all patients the day before surgery. Diabetes mellitus was defined by a baseline blood glucose of >126 mg/dL, glycosylated hemoglobin A1c level >0.06 (>6.5%), or the need for glucose-lowering treatment accordingly World Health Organization criteria. 14 Hypertension was defined as having high blood pressure (systolic blood pressure >140 mm Hg and/or diastolic blood pressure >90 mm Hg) and/or receiving antihypertensive treatment for at least 1 year before inclusion in the study. 15 Dyslipidemia was defined as fasting total serum cholesterol >200 mg/dL, low-density lipoprotein ≥140 mg/dL, triglycerides ≥150 mg/dL, high-density lipoprotein <40 mg/dL, or antidyslipidemic treatment. 16 Chronic renal failure was defined as serum creatinine >1.5 mg/dL. 17
Patients were routinely followed for 1 year in the outpatient clinic by a vascular surgeon blinded to the CRP levels. ABI measurement, evaluation of patient complaints, and physical examination were performed at all follow-up visits in every patient. Moreover, all patients underwent duplex ultrasound imaging at 1, 3, 6, and 12 months in an accredited vascular laboratory. Digital subtraction angiography was carried out during follow-up in the event of worsening symptoms, with a 1-category increase in the Rutherford scale, a decrease in the ABI >0.2 from the maximum postprocedure level, clinical worsening of an ulcer, or the diagnosis of restenosis by duplex scan as reflected by a ≥2.4 increase in the peak systolic velocity ratio. 18 Angiographic restenosis was classified as ≥50% diameter reduction at the target vessel segment. A reintervention was defined as any new endovascular or open revascularization procedure or any major amputation (above the ankle).
Blood Collection and Assay
Antecubital venous blood samples were spun at 3000 rpm for 20 minutes and then frozen at −70°C until analysis. Levels of CRP were measured by ultrasensitive automated immunoassay (Roche Diagnostics, Indianapolis, IN, USA), with detection in the lower limit of 0.2 mg/L and a variation rate of 4.2% in 4 mg/L and 6.3% in 1 mg/L. 19 All determinations were done in duplicate and with blinding as to patient status.
Endpoints and Statistical Analysis
The primary endpoint was reintervention within 12 months of EVT as predicted by pre-EVT CRP levels. In order to confirm these results, the relationship between 1 month postprocedure CRP levels and the procedure outcome were also evaluated.
Nonparametric data are presented as the median and interquartile range (IQR). The association between each clinical or laboratory variable and the main endpoint was examined using a chi-square test with Yates correction or Fisher exact test for categorical data as appropriate; an unpaired t test was used for normally distributed continuous variables, while the Mann-Whitney U test was applied for non-normally distributed variables. The Kaplan-Meier method with log-rank testing was employed to estimate the freedom from reintervention rate.
Using data from the derivation set, a cutoff CRP value at which EVT carried the highest sensitivity and specificity for failure based on receiver operator characteristic (ROC) curve analysis was sought using the values obtained before EVT and at 1 month after the intervention. The CRP value having the larger area under the curve (maximum likelihood ratio test) was established as the highest sensitivity and specificity cutoff point for hsCRP as regards EVT prognosis. The area under the curve and 95% confidence interval (CI) for each ROC curve were calculated to provide a measure of the overall diagnostic accuracy of the test. This cutoff point was then prospectively tested in the validation set.
Cox proportional hazards analysis was performed to evaluate the independent contribution of CRP levels to the risk of new reintervention. Univariate predictors of potential significance and CRP values were included in a forward stepwise selection. Results are given as the hazard ratio (HR) and 95% CI. Furthermore, as a consequence of this analysis and to remove possible bias, a bivariate post-hoc analysis was performed to assess the independent contribution of significant variables identified in the univariate analysis to the need for reintervention. Multivariate linear regression was applied to assess the independent effect of each potential risk factor on the need of reintervention. The model included age (cutoff point 68 years), diabetes mellitus, hypertension, dyslipidemia, smoking history, coronary heart disease, cerebrovascular disease, and renal disease. Differences achieving p<0.05 were considered statistically significant. Statistical analysis was performed using SPSS software (version 17.0 for Windows; IBM Corp, Armonk, NY, USA).
Results
There were no differences regarding baseline characteristics or cardiovascular risk factors between patients in the derivation and validation sets (Table 1), and none of the patients was lost to follow-up. As a whole, 46 (38.0%) of the 121 patients in the derivation set needed a reintervention within 1 year after EVT, of which 20 (16.5%) underwent a new EVT, 19 (15.7%) had a bypass graft, and 7 (5.8%) required limb amputation (Table 2). The median CRP levels before and 1 month after EVT in the 75 patients without reintervention were 3.5 (IQR 1.6–5.9) and 2.9 (IQR 1.2–4.1) mg/L, respectively (the normal hsCRP value was <5 mg/L). Among the 46 patients who needed a reintervention during the 1-year follow-up, the levels were 8.5 (IQR 4.0–13.7) mg/L prior to EVT and 6.8 (IQR 5.0–15.1) mg/L at 1 month after EVT. CRP levels elevated at baseline and 1 month after the endovascular procedure were significantly associated with a reintervention (p<0.001; Figure 1).
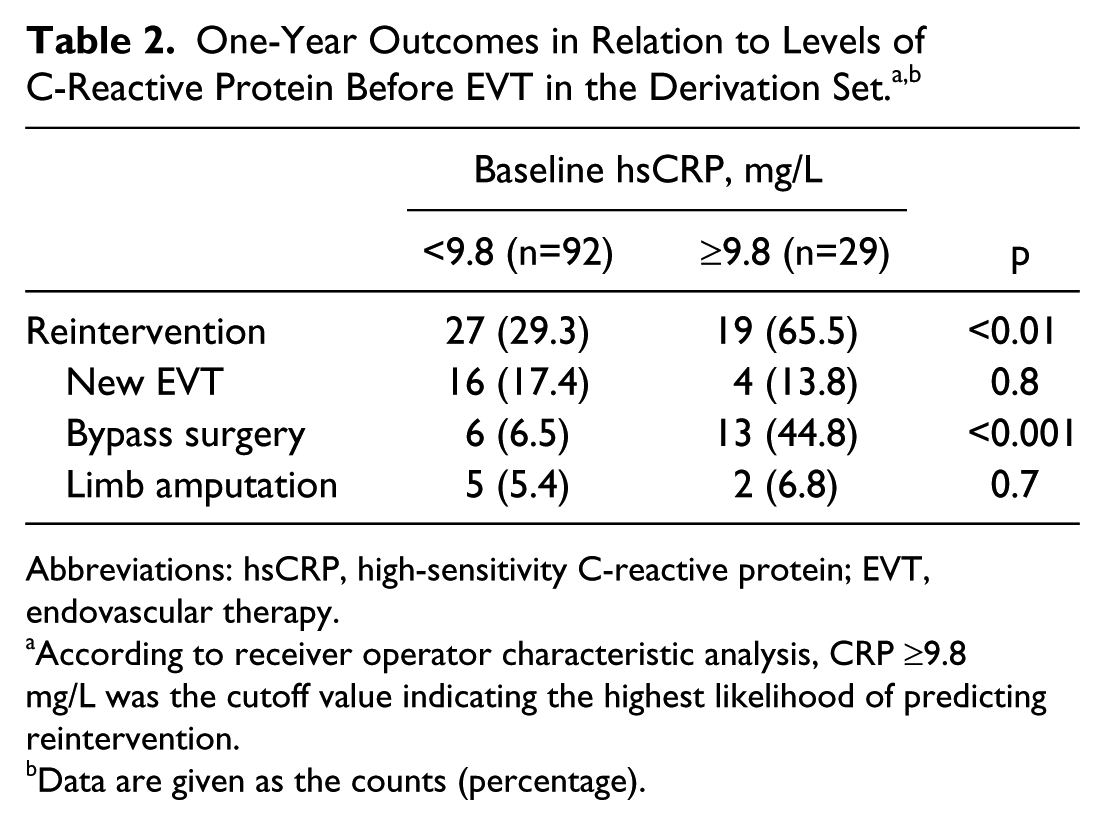
Abbreviations: hsCRP, high-sensitivity C-reactive protein; EVT, endovascular therapy.
According to receiver operator characteristic analysis, CRP ≥9.8 mg/L was the cutoff value indicating the highest likelihood of predicting reintervention.
Data are given as the counts (percentage).
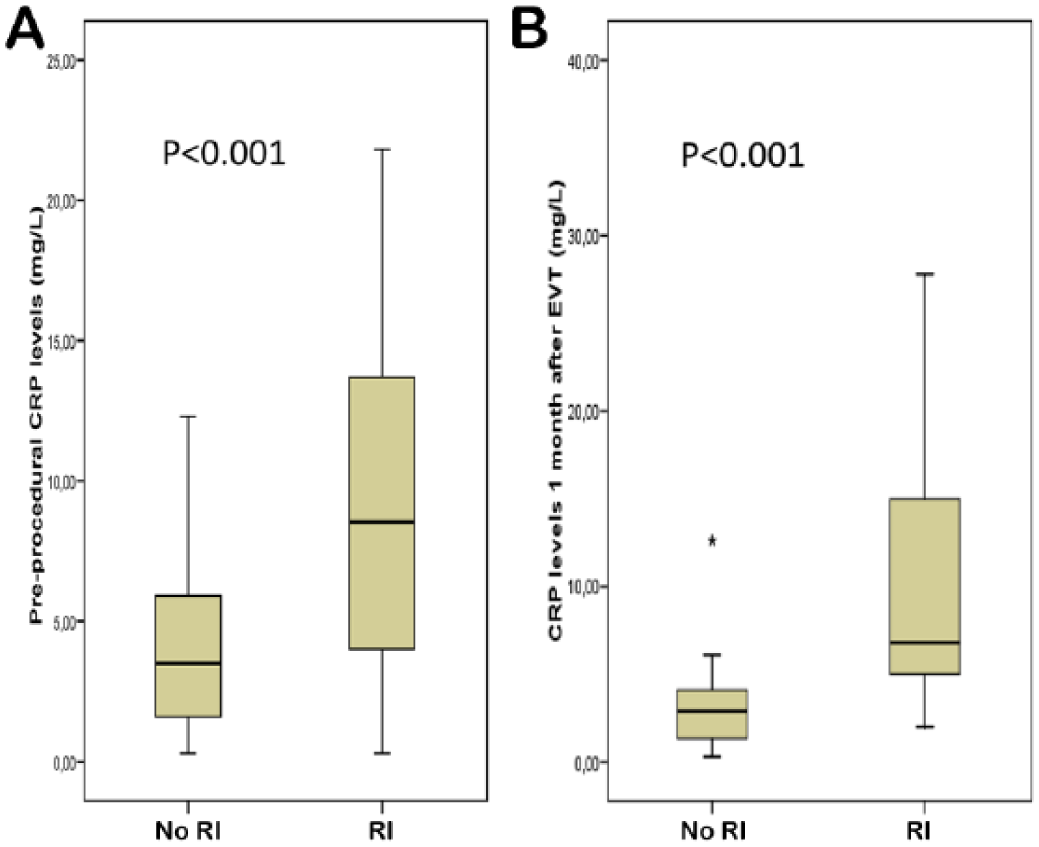
Correlations for (A) preprocedure and (B) 1-month post–endovascular therapy (EVT) C-reactive protein (CRP) levels in patients who had reintervention (RI) within 1 year and those who did not (no RI).
The areas under the ROC curves relating CRP levels to 1-year reintervention at baseline and at 1 month after EVT were 0.77±0.05 and 0.9±0.03, respectively (Figure 2). The highest likelihood ratio corresponded to a basal CRP value of 9.8 mg/L (likelihood ratio test=133, df=1, p<0.001). At 1 month after the procedure, the CRP value was 9.7 mg/L in the ROC curve (likelihood ratio test=117, df=1, p<0.001).
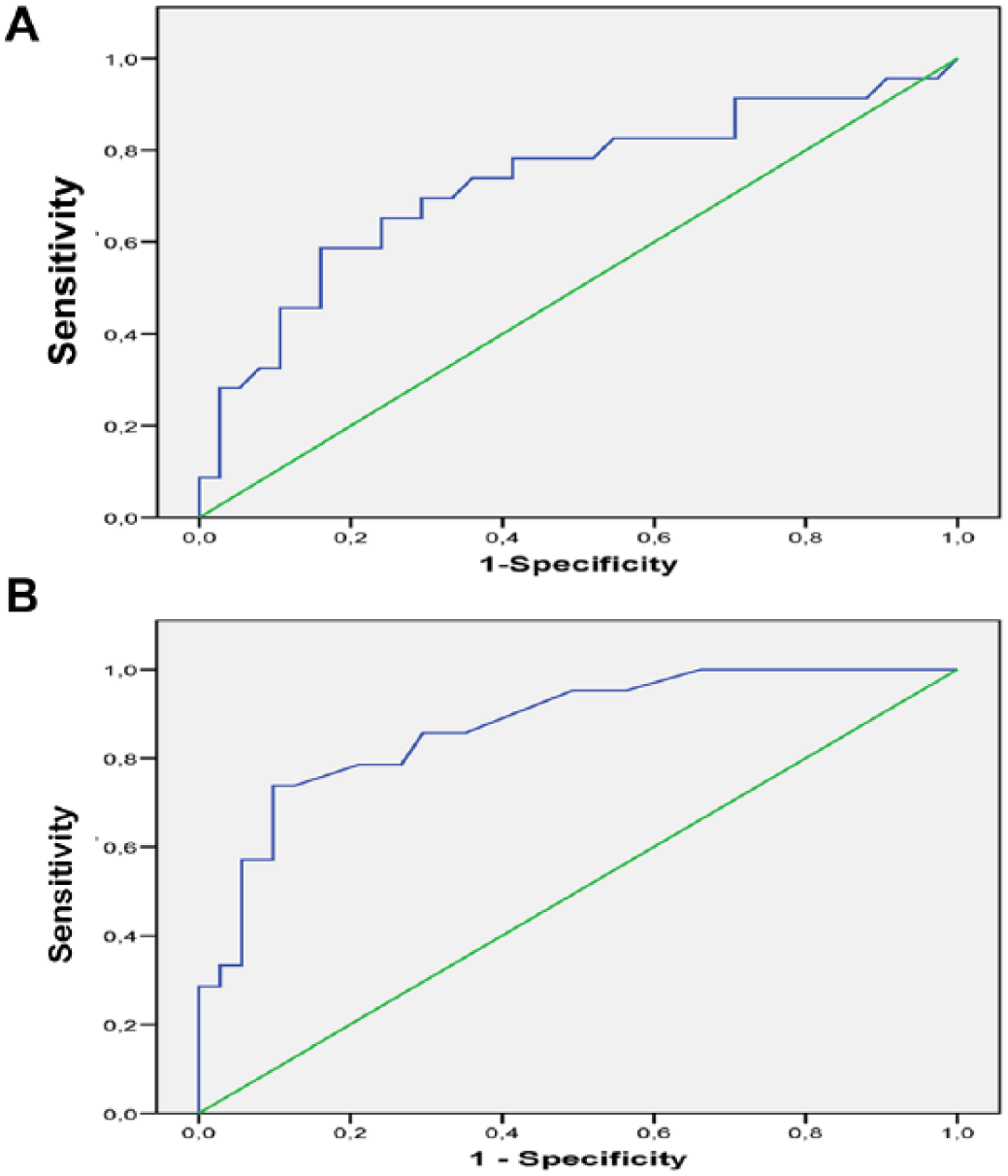
Receiver operator characteristic (ROC) curves relating C-reactive protein (CRP) to 1-year reintervention. (A) The area under the curve for the preprocedure CRP value was 0.77±0.05. (B) The area under the curve for the 1-month post-EVT was 0.9±0.03. Reintervention within a year after EVT was related to preprocedure CRP levels (HR 1.1, 95% CI 1.05 to 1.2; p<0.001). This was strengthened by the association observed between the incidence of reintervention and CRP levels 1 month after EVT (HR 1.08, 95% CI 1.05 to 1.1; p<0.001). Kaplan-Meier estimates of freedom from reintervention for patients with CRP values before and at 1 month after EVT around the cutoff points of 9.8 mg/L and 9.7 mg/L, respectively, are shown in Figure 3.
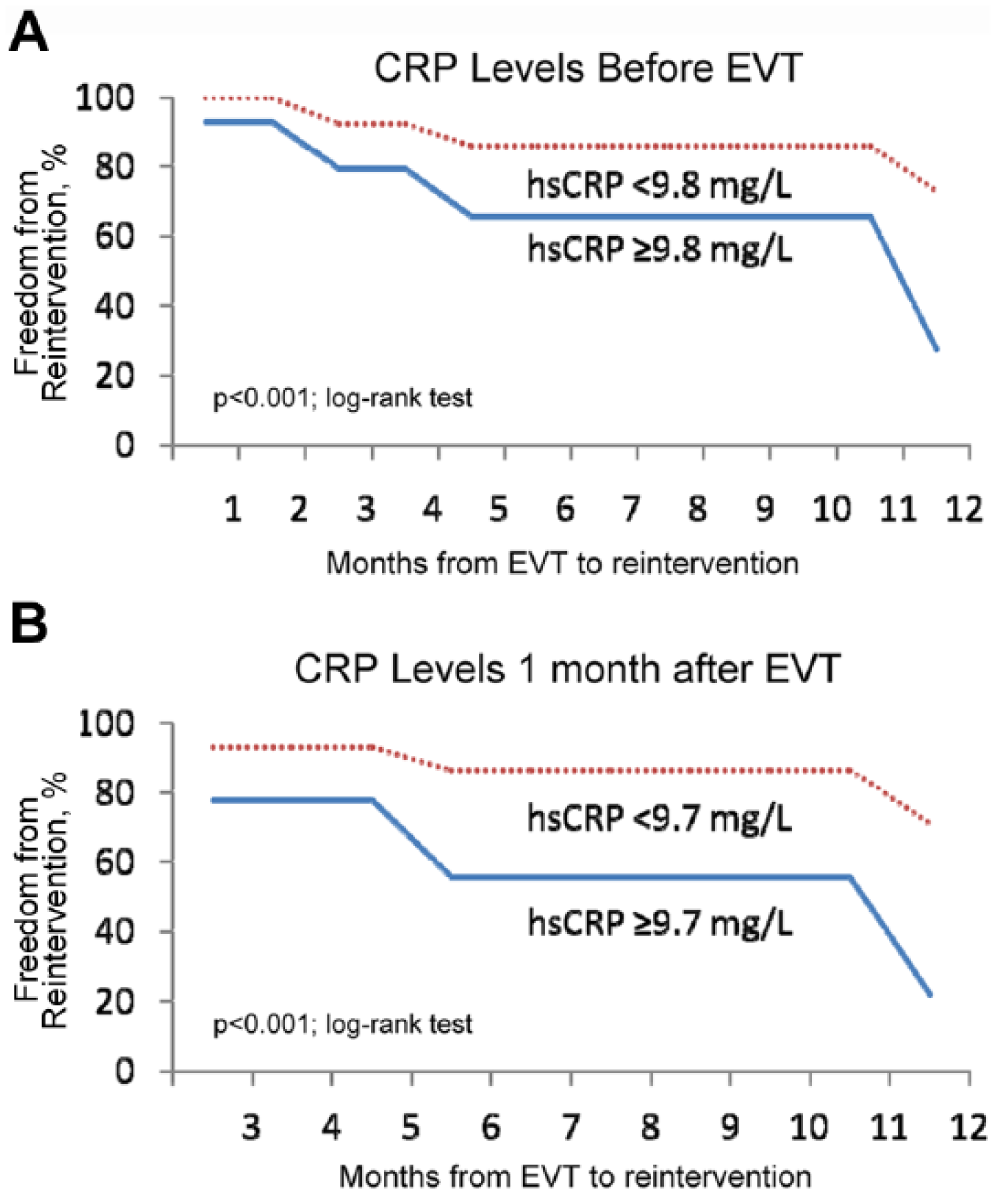
Kaplan-Meier estimate of the freedom from reintervention after endovascular therapy (EVT) within 1 year in patients with (A) high-sensitivity C-reactive protein (hsCRP) levels above or below 9.8 mg/L before treatment and (B) hsCRP levels above or below 9.7 mg/L at 1 month after the procedure.
Univariate markers of worse prognosis were also the presence of previous coronary heart disease (HR 4.5, 95% CI 1.8 to 10.9; p=0.001) and smoking habit (HR 1.5, 95% CI 1.03 to 2.2; p=0.03). There was not a significant association between the incidence of reintervention and age (HR 1.9, 95% CI 0.8 to 4.4; p=0.1), hypertension (HR 0.65, 95% CI 0.3 to 1.02; p=0.08), diabetes mellitus (HR 0.57, 95% CI 0.4 to 1.2; p=0.2), dyslipidemia (HR 2.7, 95% CI 0.9 to 6.6; p=0.12), or chronic renal failure (HR 1.5, 95% CI 0.6 to 3.8; p=0.3). The post-hoc bivariate analysis to clear a potential relation between coronary heart disease, smoking habit, and CRP levels ≥9.8 mg/L did not show statistically significant differences (p=0.19 for coronary heart disease and p=0.12 for smoking). In the multivariate analysis, pre-EVT CRP levels were the only independent predictors of new revascularization events (HR 1.1, 95% CI 1.05 to 1.2; p=0.01).
The distribution of reintervention procedures around the preprocedure CRP cutoff (9.8 mg/L) is shown in Table 2. A greater incidence of secondary interventions was noted in patients with baseline CRP levels ≥9.8 mg/L (65.5% vs. 29.3%, p<0.01). In this subgroup, open bypass was more common (p<0.001). Conversely, reintervention patients with a CRP <9.8 mg/L mostly had another endovascular procedure.
Validation
In the group of patients without reintervention, the CRP values in both sets were similar at baseline [3.5 mg/L (IQR 1.6–5.9 mg/L) in the derivation set vs 3.7 mg/L (IQR 1.9–6.4 mg/L) in the validation set; p=0.8] and at 1 month [2.9 mg/L (IQR 1.2–4.1 mg/L) in the derivation set and 3 mg/L (IQR 1.0–4.1 mg/L) in the validation set; p=0.73]. The same was true in the patients who had a reintervention for both the baseline CRP [8.5 mg/L (IQR 4.0–13.7 mg/L) in the derivation set vs. 7.9 mg/L (IQR 3.5–14.2 mg/L) in the validation set; p=0.9] and the 1-month CRP [6.8 mg/L (IQR 5.0–15.1) in the derivation set vs 7.5 mg/L (IQR 5.5–16.8 mg/L) in the validation set; p=0.65].
In the ROC curve for the validation set, a pre-EVT CRP value of 9.8 mg/L was also significantly associated with the best likelihood ratio of secondary intervention (likelihood ratio test=119; df=1, p<0.001). A pre-EVT CRP value ≥9.8 mg/L was significantly associated with a higher risk of secondary intervention (p=0.009). Likewise, basal CRP levels were a strong independent prognostic marker of 1-year reintervention (HR 1.1. 95% CI 1.02 to 1.18; p=0.008), similar to that shown in the derivation set.
Discussion
Nearly half of patients with an initially successful balloon angioplasty will present with a restenosis in the first 6 months after intervention and will need some kind of reintervention.10,11,20 Therefore, prior to the procedure, it would be crucial to identify patients who are likely to benefit from EVT and those who might need a more definitive solution such as open surgery. 8
The aim of the study was to elucidate a cutoff CRP value at which EVT in PAD patients carries the highest possibility of 1-year failure. We adopted strict enrollment criteria in order to avoid possible confounding factors capable of increasing CRP levels. We found that more than a third of our EVT patients required reintervention within 1 year, which likely reflects the large proportion of critical limb ischemia patients in the study, who have notoriously poor outcomes overall. However, other reasons should be considered, such as diligent case management, complete screening of failing procedures, and extensive vascular and Doppler ultrasound examination in this cohort. From this standpoint, the possible presence of a selection bias is less plausible.
We prospectively validated our findings in another sample of PAD patients to be confident that our threshold could be generalized beyond the group that was studied. According to our data, we have shown that the baseline CRP level can predict the need for secondary intervention at 1 year. In like manner, we found that the CRP value at 1 month had a strong association with 1-year revascularization events. These findings are consistent with previous observations of elevated CRP values reflecting the severity and extent of PAD3,9,10,21,22 and also support the hypothesis that systemic inflammation is involved in the pathogenesis of postangioplasty restenosis. 10
Previous studies have shown that the baseline CRP levels are predictors of adverse events after percutaneous coronary interventions independent of diabetic status.23,24 Primary prevention studies among healthy people have also shown significant cardiac risk prediction by means of elevated CRP levels without correlation to diabetes. These data appear to demonstrate that CRP levels predict cardiac risk independent of diabetic status. 25
The pathophysiological reason for an association between CRP and EVT prognosis is uncertain. However, our data suggest that the effect of the systemic inflammatory process on the results of EVT could be independent of the effect that the surgical procedure can have on the inflammatory process at the arterial wall. Persistently elevated CRP levels may represent either an ongoing inflammatory process or the extension of atherosclerotic lesions in PAD. A growing body of evidence from human studies 3 indicates that inflammatory mechanisms contribute to the onset and extension of the PAD. Elevated CRP levels may also affect coagulation through the important role of tissue factor expression. 26 Thus, high CRP levels are implicated in both development and post-therapeutic prognosis in PAD.
Limitations
First, there is the moderate sample size. Second, the potential association between the severity of restenosis (eg, occlusive vs nonocclusive) and CRP levels was not analyzed. However, the focus of our study was to determine a clinically useful CRP marker, so the morphological characteristics of recurrent lesions were not considered in the study design.
Since the majority of the patients with CRP values >9.8 mg/L requiring reintervention had open surgery, we suggest that this value may be used when planning treatment to stratify which patients would be better served with open surgery. This would indeed augment the existing literature on CRP and PAD.
Conclusion
While there are other studies with similar or larger groups of patients that examined the prognostic value of CRP levels in EVT failure,9-11 our study goes a step further to define a ROC-based cutoff value. Patients with pre-EVT CRP levels >9.8 mg/L would have poorer 1-year prognosis compared to patients with lower CRP levels. Baseline CRP levels >9.8 mg/L are markers for subsequent secondary interventions, which were often open bypass. Thus, this study adds incremental value to the use of pre-EVT CRP levels to determine patients at increased risk for poorer outcomes after EVT.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.