
Abstract
Keywords
Introduction
Popliteal artery aneurysms (PAAs) and their complications have the potential to threaten limb and life. Repair is advocated when symptoms present (compression, embolization, ischemia, or rupture), as well as for asymptomatic disease. The threshold for treatment in asymptomatic patients varies between centers and must be balanced against the patient’s overall clinical status and suitability for intervention. Open repair, in the form of exclusion bypass, is considered the gold standard procedure. However, it has been suggested that continued sac expansion may be found in up to 30% of patients,1–3 continued symptoms in up to 20%,2–4 and reintervention rates may be as high as 21%. 5
Endovascular PAA repair (EVPAR) is an alternative therapy that was first described in 1994. 6 Early systematic reviews and meta-analyses of EVPAR raised concerns over the durability of endovascular therapy, but these investigations were limited by small sample size and evolution in endograft design over time.7,8
Compared with earlier devices, the Hemobahn and Viabahn endoprostheses (W.L. Gore & Associates, Flagstaff, AZ, USA) provide improved flexibility, potentially improving durability despite flexion and extension of the knee joint. 9 The outcomes from these newer generation devices may not be comparable to earlier technology and therefore merit a focused review. The aim of this study was to assess the current literature regarding contemporary Hemobahn/Viabahn stent-graft use in the management of PAAs.
Methods
Searches of the English-language literature were performed using the Embase and Medline databases, according to the Preferred Items for Reporting of Systematic Reviews and Meta-Analyses guidelines. 10 The free-text search terms “endovascular popliteal aneurysm repair,” “EVPAR,” “popliteal,” “aneurysm, “outcome,” “stent,” “patency,” “Hemobahn,” and “Viabahn” were used in combination with the Boolean operators “AND” or “OR.” The reference lists of articles obtained were manually searched to identify further relevant citations. The literature search spanned articles published between 1996 (the date of introduction of the Hemobahn stent-graft) and 2013.
Abstracts identified by the search were scrutinized by two of the authors (S.R.P. and C.H.) to determine eligibility for inclusion in a systematic review and meta-analysis. Disagreements were resolved by consensus overseen by one of the senior authors (A.K.), who arbitrated when necessary.
The inclusion criteria were defined as reports of endovascular PAA repair using either Hemobahn and/or Viabahn stent-grafts in at least 10 subjects. It was deemed essential that studies reported primary patency using a principled statistical method, accounting for loss to follow-up or censoring. The primary outcome measures were primary and secondary patency. Secondary outcome measures were rates of reintervention, endoleak, stent-graft fracture, and limb salvage. A sensitivity analysis was performed comparing primary patency in studies using both Hemobahn and Viabahn stent-grafts compared to studies reporting Viabahn stent-grafts only.
Statistical Analysis
Pooled Kaplan-Meier survival curves were generated for primary and secondary patency; the rates are reported with the 95% confidence intervals (CIs). Interval data from primary and secondary patency survival curves were extracted using the ReadImage and digitize packages within R (R Foundation for Statistical Computing, Vienna, Austria; http://www.r-project.org ), as previously described by Poisot. 11
Random effects meta-analysis was performed for secondary outcomes using the DerSimonian and Laird 12 random effects method. Comparative patency for open and EVT was meta-analyzed using the inverse-variance random effects method to give a pooled hazard ratio (HR). Where necessary, summary time-to-event data were calculated from Kaplan-Meier curves using the methods outlined by Tierney et al. 13
Results
Fourteen studies14-27 published between 2007 and 2014 were identified for pooled analysis (Figure 1); 9 were retrospective case series,16,17,19,20,22,23,25–27 4 were retrospective comparative studies against surgical exclusion bypass,15,18,21,24 and 1 was a randomized trial against surgical exclusion bypass. 14 Data were available for 514 endovascular PAA repairs in patients ranging from 64.3 to 81 years old (Table 1). Three studies14,22,25 excluded symptomatic aneurysms and those associated with acutely ischemic limbs or signs of nerve/vein compression.
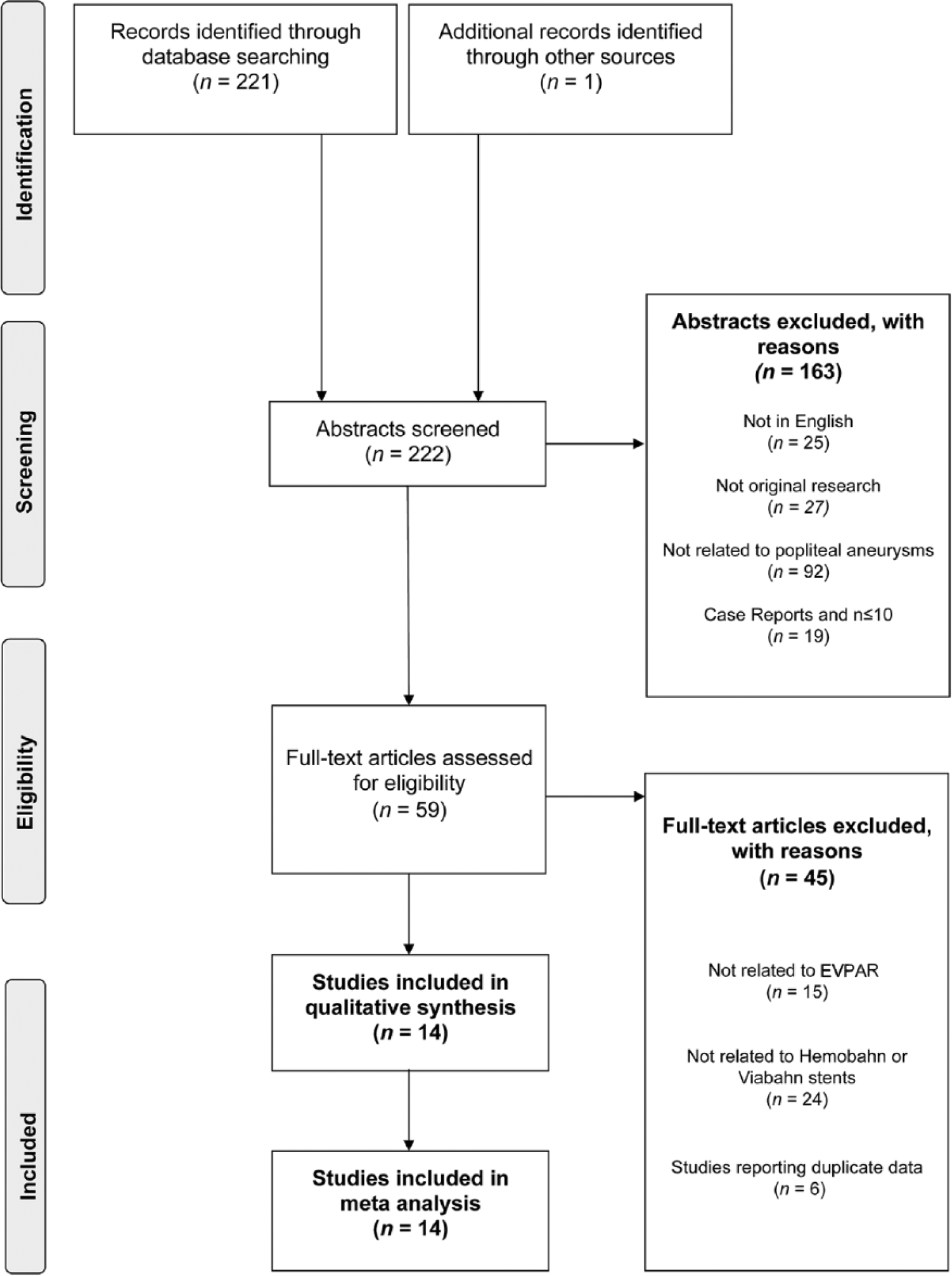
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram. EVPAR, endovascular popliteal aneurysm repair.
Study Characteristics, Patient Demographics, and Eligibility Criteria for EVPAR.
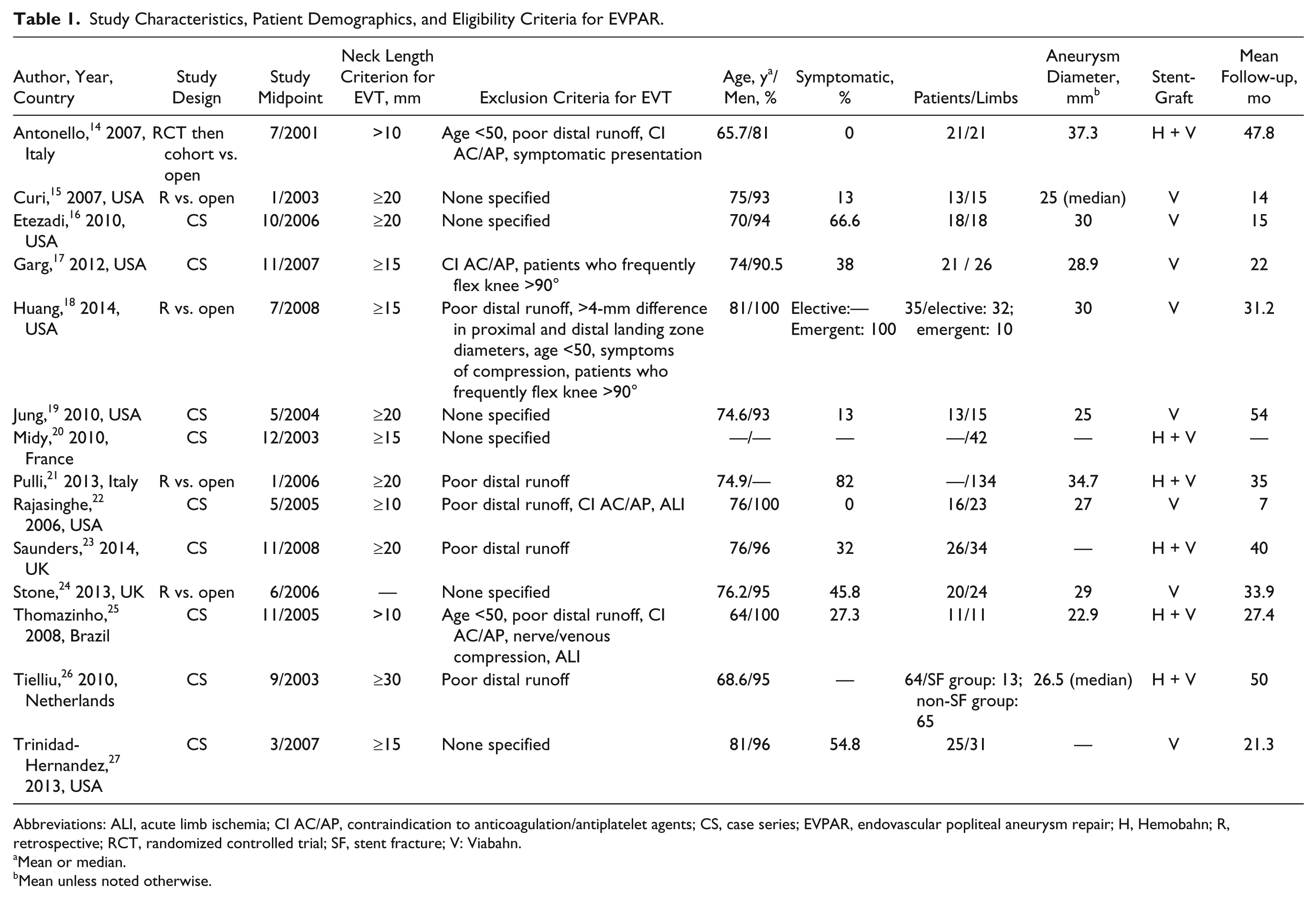
Abbreviations: ALI, acute limb ischemia; CI AC/AP, contraindication to anticoagulation/antiplatelet agents; CS, case series; EVPAR, endovascular popliteal aneurysm repair; H, Hemobahn; R, retrospective; RCT, randomized controlled trial; SF, stent fracture; V: Viabahn.
Mean or median.
Mean unless noted otherwise.
Primary Outcomes
All 14 studies reported primary patency data, while 5 studies14,15,18,21,24 compared EVT and surgical repair. The pooled primary patency rate for EVPAR using Hemobahn or Viabahn stent-grafts was 95.0% (95% CI 92.8% to 98.6%) at 30 days, 85.3% (95% CI 82.0% to 88.8%) at 12 months, and 69.4% (95% CI 63.3% to 76.2%) at 5 years (Figure 2A). There was no significant difference in primary patency for EVPAR compared with surgical repair, with a pooled HR of 1.30 (95% CI 0.79 to 12.14, p=0.189; Figure 2B).14,15,18,21,24 A sensitivity analysis comparing primary patency in studies using both Hemobahn and Viabahn stent-grafts14,20,21,23,25,26 compared to studies reporting Viabahn stent-grafts only15-19,22,24,27 showed no significant difference in primary patency (Figure 2C).
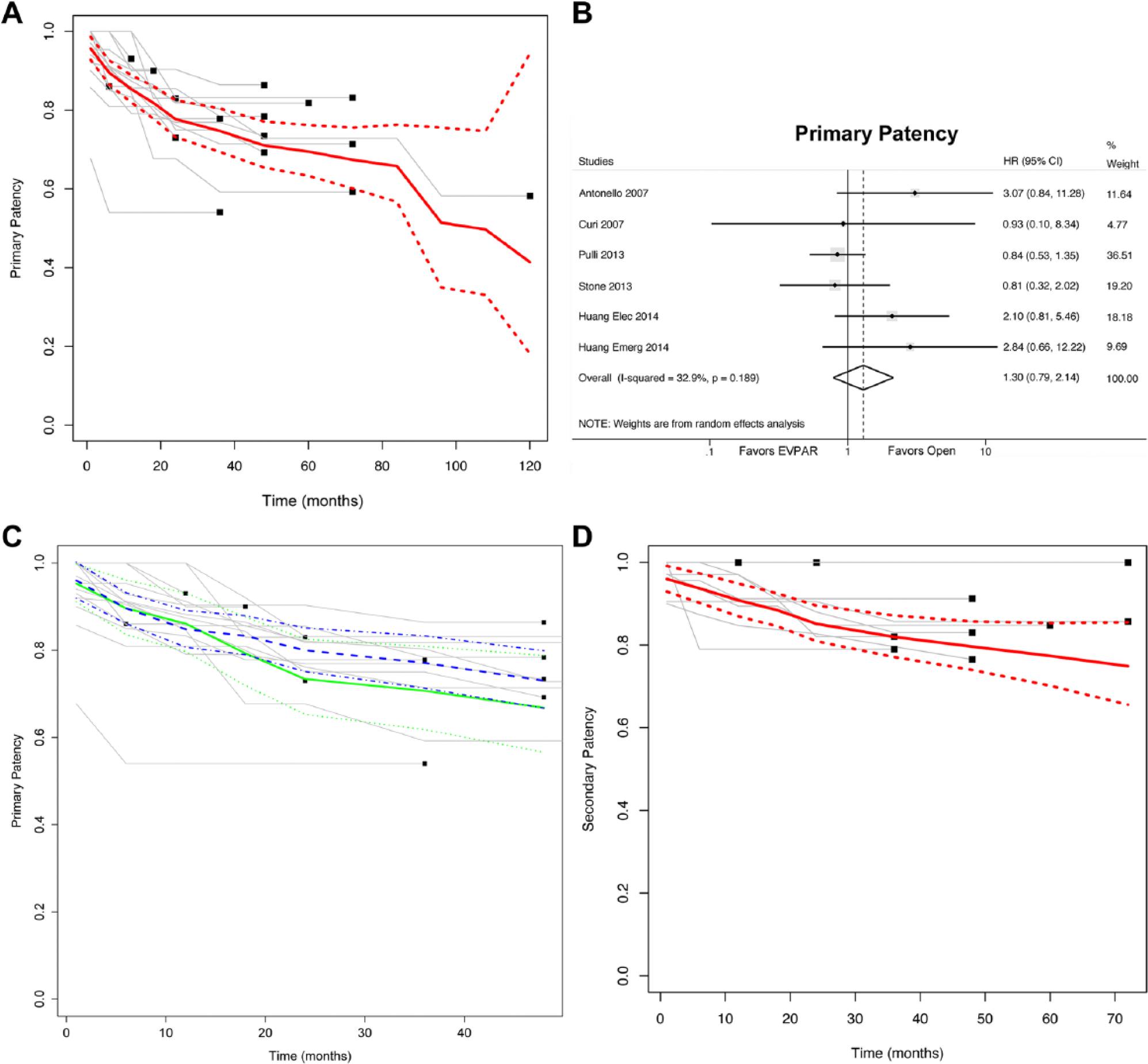
(A) Pooled primary patency rates in endovascular popliteal aneurysm repair (EVPAR). [Solid line, pooled estimate of primary patency; dotted lines, 95% confidence intervals (CIs); gray lines, primary patency survival curves from original studies]. (B) Meta-analysis to determine the hazard ratio for loss of primary patency in EVPAR as compared with open repair. (C) Pooled primary patency rates for Viabahn stent-graft alone (solid green line with dots as 95% CI) vs. Viabahn + Hemobahn stent-grafts (blue dashed with interrupted dots/dashes as 95% CI). Gray lines, primary patency survival curves from original studies. (D) Pooled secondary patency rates in EVPAR. (Solid line, pooled estimate of primary patency; dotted lines: 95% CI; gray lines, primary patency survival curves from original studies). The color version of this figure is available online at http://www.jevt.org .
Secondary patency was reported in 9 of 14 studies.14,15,17–19,21-23,27 The pooled secondary patency rate was 96.0% (95% CI 92.9% to 99.1%) at 30 days, 90.8% (95% CI 86.9% to 94.9%) at 12 months, and 77.4% (95% CI 70.1% to 85.3%) at 5 years (Figure 2D). There were insufficient data to compare secondary patency between surgical repair and EVT.
Secondary Outcomes
Reintervention rates following EVPAR were reported by 6 studies.18,19,21–23,27 In these studies, 4.3% to 40% of cases underwent reintervention in a follow-up that ranged from 7 to 54 months. It was not possible to distinguish reintervention rates for emergent compared with elective cases. The largest multicenter EVPAR series of 134 cases from Italy reported a 30-day reintervention rate of 9.7% and a 4-year freedom from reintervention of 75%. 21 The same study showed a similar 30-day reintervention and 4-year freedom from secondary intervention of 5% and 72.5%, respectively, for surgical repair.
A paucity of data in the other studies did not allow meaningful meta-analysis for comparison of reintervention rates between open repair and EVPAR. The most common indications for reintervention were graft thrombosis or occlusion,14,16,17,22,23,17 restenosis, 14 and type I or III endoleaks.15,19,27 There were a variety of treatment modalities employed for reintervention, including endovascular relining, percutaneous thrombectomy, thrombolysis, surgical bypass, and amputation.
The incidence of endoleak during follow-up was reported in 9 studies14,15,17,19,21,23–25,27 at heterogeneous time points. Endoleaks of all types were reported with an incidence of 0 to 20% between mean follow-up periods of 14 and 54 months; types I and III endoleaks were reported in 0 to 16.7% of the same studies. Four studies14,17,23,24 reported an absence of endoleaks throughout their entire follow-up period (up to a mean follow-up of 47.8 months). All type I or III endoleaks were treated by relining, and all type II endoleaks were managed conservatively. There were insufficient data to compare endoleak incidence or continued sac expansion between open repair and EVT.
Of the 5 studies14,17,23,26,27 reporting the incidence of stent-graft fracture, 314,17,23 had no fractures during follow-up, and the overall reported incidence ranged from 0 to 27.3% in studies with mean follow-up between 21.3 and 50 months.
Limb salvage/amputation rates were reported only in those 8 series14,17,19,21–24,27 reporting emergent presentations. Limb salvage was 100% for the entire duration of 4 studies17,19,22,24; it was <95% in only 1 study at a time point of 3 years. 23
Study Design Characteristics
Inclusion and exclusion criteria for endovascular repair varied considerably. Proximal/distal landing zone length was the most commonly cited consideration in determining eligibility for EVPAR. However, in the 13 studies14–23,25–27 that reported this criterion, the required proximal and distal landing zone lengths varied from ≥1 to ≥3 cm (Table 1). Four studies14,17,18,25 excluded patients younger than 50 years and/or those with high levels of physical activity as these were considered surrogates for increased periods of knee flexion/extension, which would theoretically risk graft complications. Poor distal vessel runoff was an explicitly stated consideration, though not necessarily an absolute exclusion criterion, in 7 studies.14,18,21–23,25,26 In these reports, systems for classifying the quality of distal runoff varied from those reporting the proportion of 3 crural vessels remaining patent to studies proposing validated scoring systems for practice.
Patients with contraindications to anticoagulation or antiplatelet medication were excluded in 4 of the studies14,17,22,25 (Table 1). Other exclusion criteria comprised aneurysmal or stenotic disease in the ipsilateral iliac or femoral arteries or excessive tortuosity of the aneurysm. Computed tomographic angiography (CTA) and duplex ultrasonography were the most commonly employed imaging modalities prior to operation.
Intraoperative Characteristics
Percutaneous access was performed under local anesthesia in 4 studies.14,22,23,25 Open cutdown was performed in 1 study, 26 while 9 articles15-21,24,27 reported a combination of access techniques according to the discretion of the surgical team in each case (Table 2).
Intraoperative and Postoperative Considerations.
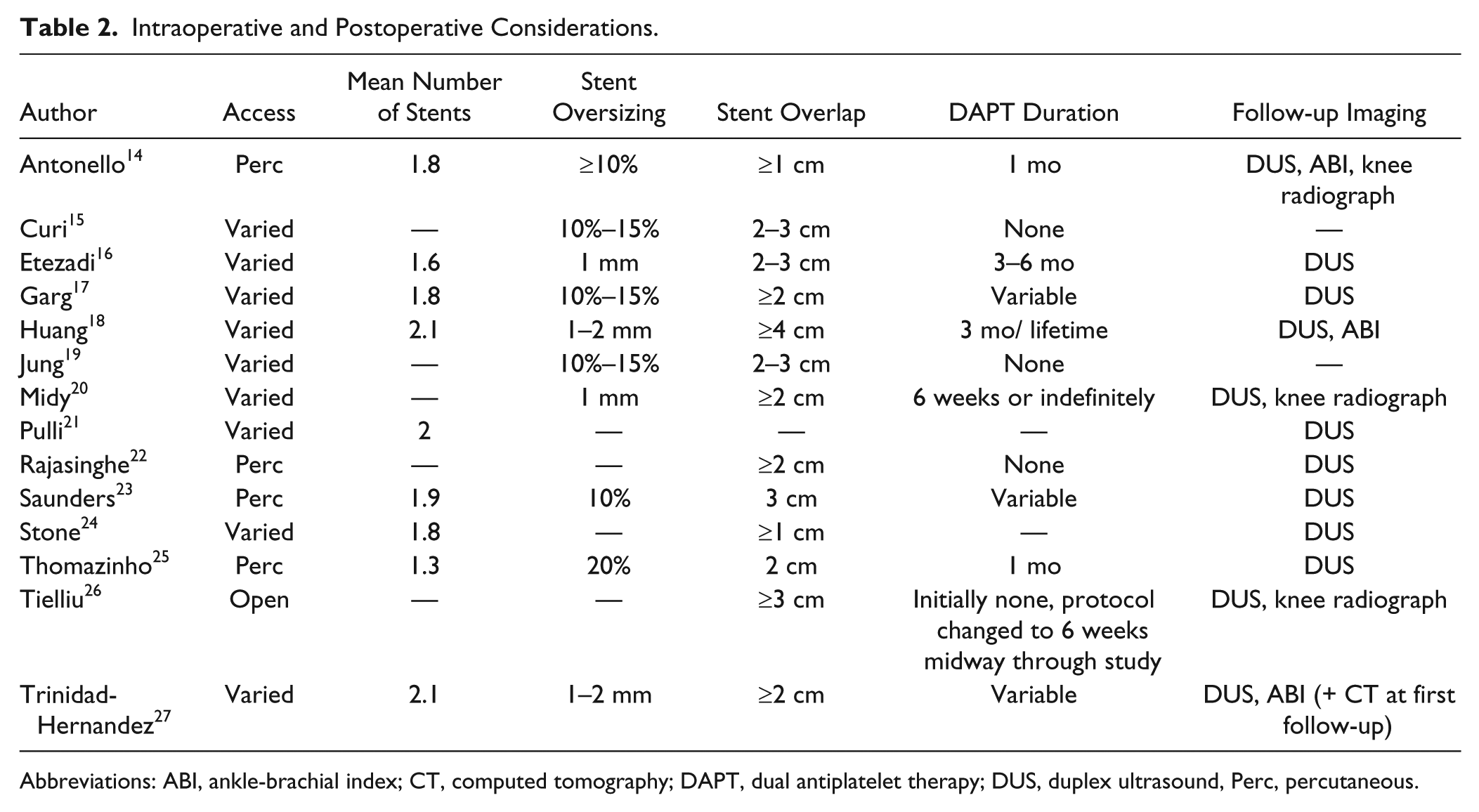
Abbreviations: ABI, ankle-brachial index; CT, computed tomography; DAPT, dual antiplatelet therapy; DUS, duplex ultrasound, Perc, percutaneous.
All studies reported the routine use of >1 stent-graft to achieve successful exclusion of the aneurysm. Nine studies14,16–18,21,23–25,27 reported a mean number of stent-grafts deployed per aneurysm, which ranged from 1.3 to 2.1 (Table 2). Oversizing of the stent-graft was performed at 10%, 10% to 15%, 20%, or an absolute value increase of 1 or 2 mm relative to native neck diameter.15–20,23,25,27 If 2 or more stent-grafts were used, targeted overlap distance between stent-grafts ranged from ≥1 to ≥4 cm among various studies14-20,22–27 (Table 2). Most studies advocated the use of completion angiography with the knee extended and flexed to ensure on-table patency.
Postoperative Characteristics
Twelve studies14,16-18,20–27 specified duplex ultrasonography as the principle surveillance imaging modality; 3 studies14,18,27 additionally used ankle-brachial index measurements and 3 studies14,20,26 additionally used knee radiographs (Table 2). CTA was frequently used to further investigate abnormalities flagged by the principle imaging modality. Follow-up appointments were issued yearly after a variable number of visits in the first postoperative year.
Antiplatelet regimens were inconsistent among studies (Table 2), with duration of dual antiplatelet therapy postoperatively ranging from 1 month,14,25 6 weeks,20,26 3 months, 18 and 6 months 16 to indefinitely/lifetime.18,20 Five studies15,17,19,22,26 reported using only single antiplatelet therapy postoperatively.
Discussion
The main finding of this study was that EVPAR represents a feasible treatment modality, with acceptable midterm safety. The pooled 5-year primary and secondary patency rates for EVPAR (69.4% and 77.4%, respectively) are comparable to patency rates previously reported for open exclusion bypass. For example, a series of 358 open PAA repairs achieved a 5-year patency of 76%, with saphenous vein conduit yielding better patency than prosthetic grafts. 5 A systematic review of 2445 open PAA repairs from 1997 reported 5-year patency from 77% to 100% for saphenous vein grafts. 28
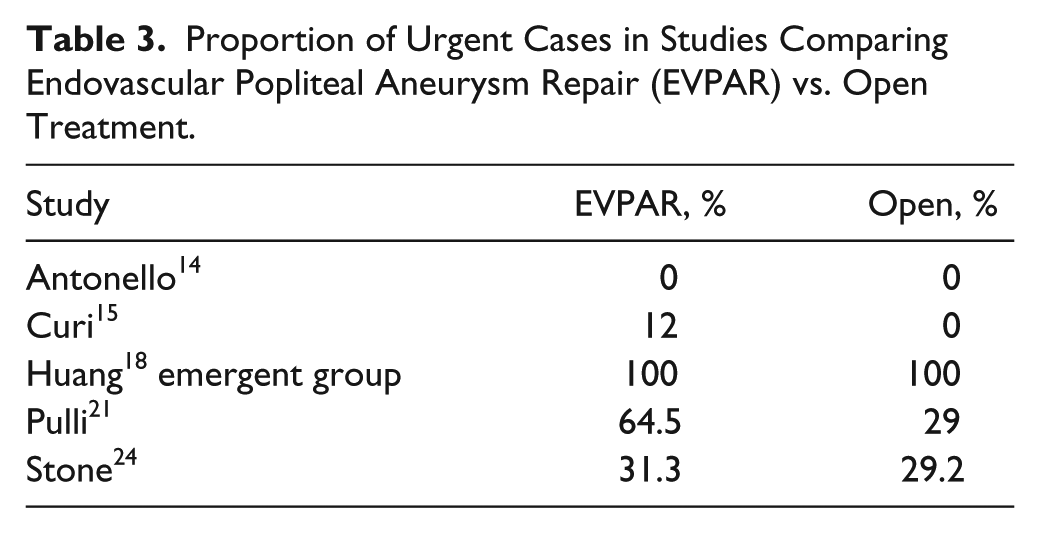
However, EVPAR is still considered an investigational procedure, which is reflected by the paucity of high-quality evidence providing randomized comparison with open repair. Only one randomized controlled trial (RCT) met the inclusion criteria for this review. Although no significant difference was demonstrated between EVPAR and open repair, our pooled comparison of treatment modalities was limited by the inclusion of unbalanced groups of emergency and elective cases within studies (Table 3) as well as the lack of level-1 evidence. This was demonstrated in a recent Cochrane review, which presented a single RCT in an attempt to answer the question of EVPAR vs open repair. 29 Clearly, there is a need for randomized studies of EVPAR vs open repair in morphologically suitable candidates. Separate RCTs should be conducted in the emergent and elective settings, as there are important differences in outcome between these presentations.
Proportion of Urgent Cases in Studies Comparing Endovascular Popliteal Aneurysm Repair (EVPAR) vs. Open Treatment.
Confounding and unmeasured selection bias cannot be excluded, and the existing evidence comparing EVT to open repair should therefore be interpreted in light of these deficiencies in the data. There appeared to be considerable heterogeneity in case selection, intraoperative technique, and follow-up protocols among studies. This reflects the emerging nature of the current evidence base for EVT, and it is likely that our pooled analyses have incorporated institutional learning curves for the procedure and the attendant sequelae.
Endograft durability remains a key concern for the endovascular repair of aortic aneurysms.30–32 In our study, analyses to identify predictors of stent-graft durability were limited by the small sample sizes of existing studies. Trinidad-Hernandez et al 27 did not identify any factors predicting graft failure in their study of 25 patients. In the largest series included in our study, having fewer than two patent crural vessels was a predictor of graft failure in multivariate analysis, 21 a finding that has been demonstrated previously in the setting of infrainguinal angioplasty and lower limb bypass.33,34 However, there was considerable heterogeneity in patient selection and poor distal runoff (with a variable number of patent crural vessels specified among various studies). The absence of postoperative anticoagulation or antiplatelet administration is known to predict graft failure. 35 All studies described the prescription of at least one antiplatelet agent for patients, but the postoperative duration of antiplatelet therapy varied from 3 weeks to lifelong treatment.
Future research should focus on refining selection criteria for EVPAR and identifying the subgroups of patients who will gain most from either open repair or endovascular therapy. Many factors may affect the success of exclusion bypass, including the type of conduit used, the presence of symptoms, and the emergency/elective classification of the procedure.
Endovascular popliteal aneurysm repair therefore should be considered selectively in PAA patients with suitable anatomy on a case by case basis and particularly in patients at high surgical risk, including the elderly or obese, patients with poor cardiorespiratory fitness, patients with bilateral large PAAs and poor availability of autogenous bypass conduit, or those well informed patients who elect to proceed with stent-graft repair in spite of the available weak evidence. Defining the optimal postoperative surveillance and medical management for these patients also appears to be a priority, as does differentiating outcomes between emergent and elective presentations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.