
Abstract
Since the advent of endovascular repair of aortic aneurysms (EVAR), clinical focus has been on preventing loss of sealing at the level of the infrarenal neck, which leads to type I endoleak and repressurization of the aneurysm sac. Enhanced mechanisms for central fixation and seal have consequently lowered the incidence of migration and endoleaks. However, endograft limb thrombosis and its causal mechanisms have not been addressed adequately in the literature. This article reviews the pathophysiological mechanisms associated with limb thrombosis in order to facilitate better clinical judgment to prevent iliac adverse effects.
Keywords
Introduction
Since the advent of endovascular aneurysm repair (EVAR) of abdominal aortic aneurysm (AAA), loss of seal at the level of the infrarenal neck with resultant type I endoleak and repressurization of the aneurysm sac has comprised the most dangerous complication of the method. Therefore, it has always been a matter of priority for clinical investigators and industry to enhance stent-graft stability and resistant to migration and loss of fixation. 1 Certain improvements in central fixation, such as suprarenal stents with hooks and/or barbs and the development of endografts that accommodate onto the aortic bifurcation, have evolved to counteract the displacement forces that predispose to endograft caudal migration.2 –4 As a result, a substantial improvement in the performance of newer endografts has been documented with respect to survival from any type of endoleak, reintervention, or open conversion. 5
Iliac Adverse Effects and Reintervention
Though refinements in endograft design have led to a significant reduction in the need for reinterventions to treat type I endoleak, the issue of endograft limb occlusion has been addressed only minimally in the literature. With the focus on the “traditional” major complication (ie, endograft migration), the incidence and causes of limb thrombosis have drawn little attention,6 –11 though a wide range of graft occlusions (0–7%) has been reported in follow-up studies of EVAR. As van Zeggeren et al 12 recently pointed out, the publication dates, institutional characteristics, follow-up duration, and patient cohorts in EVAR studies are very heterogeneous, contributing to the variability in occlusion rates even within single-graft studies. For example, among a large registry 7 and the 4 prospective, randomized controlled trials8 –11 that constitute the backbone of the EVAR knowledge, the ACE (Anévrysme de l’aorte abdominal: Chirurgie versus Endoprotese) trial reported 16% reinterventions among the 150 patients in the EVAR arm, without discriminating among graft replacement, open or endovascular repair of endoleaks, and management of limb occlusion or stenoses. 8 Accordingly, the OVER (Open versus Endovascular Repair) trial randomized 881 patients to endovascular vs open AAA repair and followed them for up to 9 years (mean 5.2). The authors reported a total of 148 secondary procedures in the 22% of patients treated endovascularly, including 100 endovascular procedures, 9 conversions to open repair, and 19 arterial procedures with an open component; however, the percentage relevant to any thrombotic limb event was not delineated. 9 On the other hand, the DREAM (Dutch Randomized Endovascular Aneurysm Repair) trial reported a limb thrombosis incidence of 7% (12/173 patients) after a median follow-up of 6.4 years. 10 Finally, the long-term results of the United Kingdom EVAR trial identified 20 cases of graft thrombosis, 4 cases of graft stenosis, and 10 cases of graft kinking among 624 patients in the endovascular arm of the study. 11
Iliac Vessel Geometry and Adverse Effects
The importance of aortoiliac angulation and tortuosity (Figure 1) has been addressed only recently in the literature. Carpenter et al 13 estimated that 10% of AAAs presenting for treatment are not eligible for EVAR due to excessive iliac tortuosity. Taudorf et al 14 retrospectively analyzed 504 EVAR patients who completed a median follow-up of 28 months. The authors assessed the influence on graft limb thrombosis of geometrical factors such as AAA diameter, diameter of the iliac artery landing zone, stent-graft limb diameter, distal aortic diameter, iliac tortuosity, and the existence of peripheral outflow occlusion. From these factors the authors identified common iliac artery (CIA) tortuosity as the sole independent geometrical factor (p<0.001) predisposing to limb occlusion. Similarly, Wyss et al 15 showed a significant association of CIA tortuosity with graft-related complications after EVAR (adjusted hazard ratio 5.96) in a series of 217 patients, where iliac limb kinking and/or thrombosis were identified as the leading cause (27%) of reinterventions.
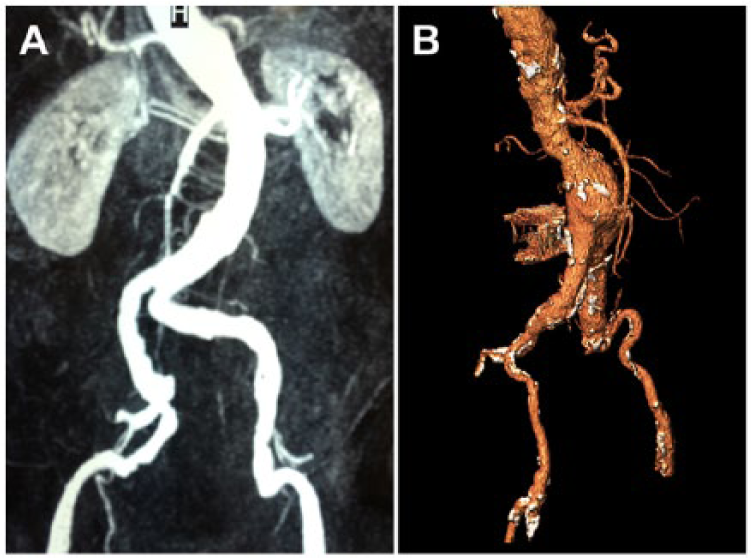
Aortoiliac (A) and (B) left iliac artery tortuosity. The color version of this figure is available online at www.jevt.org .
According to Cochennec et al, 16 the incidence of endograft limb thrombosis ranges between 2.6% and 7.4%, rendering it the third most common reason for readmission after EVAR. Predisposing factors can be categorized as anatomical and technical; the former includes narrow bifurcation and small diameter, stenosis, calcification, tortuosity, and angulation of the iliac arteries (Table 1).17 –22 Technical reasons refer to the use of unsupported graft limbs, extension of the distal landing zone to the external iliac artery (EIA), as well as excessive oversizing of the endograft.17 –21 Moreover, the structural pattern of endograft limbs [adaptation to the individualized AAA anatomy (angulation, tortuosity) and the shape, size, and density of the nitinol supporting stents] may affect limb resistance to occlusive events. In most instances, limb occlusion occurs early within the first few weeks or months, as a result of the aforementioned anatomical factors. In fewer instances, limb kinking and occlusion occur years after the initial intervention, attributed either to downward migration of the endograft or to sac shrinkage due to remodeling. These phenomena alter the configuration of the endograft and result in kinking.7,22
Factors Predisposing to Graft Limb Thrombosis.
Pathophysiological Mechanisms Attributed to Iliac Geometry
Angulation and aortoiliac tortuosity (ie, the difference between the true iliac length and the shortest distance) have certain hemodynamic consequences on the magnitude and direction of displacement forces, as well as on the pressure and shear stress distribution in the iliac limbs over the cardiac cycle.23 –25 Figure 2 illustrates the difference in stress distribution and velocity profiles between the curved and straight renal stent configurations in 2 computational models of fenestrated endografts, as recently shown by our study group. 26 Accordingly, it would be logical to assume that deviation from the straight pattern and adaptation to tortuous or angled geometries can impose altered stress patterns to the endograft limbs (Figure 2E and F). This assumption seems to be in accord with the recently proposed mechanism by Bisdas et al 27 to explain the relation between tortuous iliac geometry and limb occlusion. According to these authors, the excessive tortuosity of the iliac landing zone may lead to suboptimal apposition of the distal limb terminus (Figure 3A and B). The resultant intimal injuries cause subintimal hyperplasia and local stenosis (Figure 3C), which in the long run generate a shear stress gradient at the interface between the stent and intima and altered pressure distribution (Figure 4A–H) during the cardiac cycle. These changes can predispose ultimately to limb occlusion.
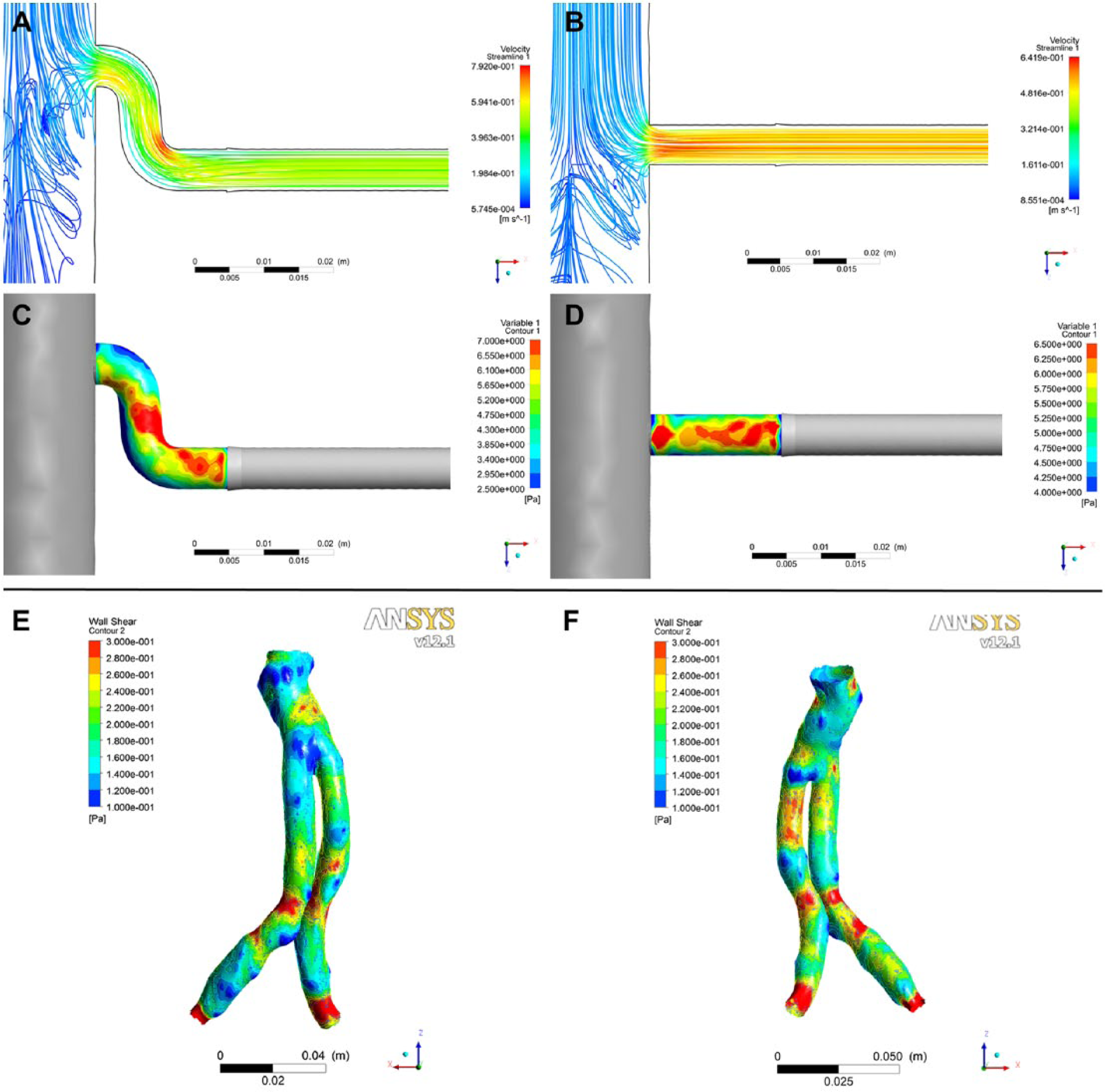
Effect of tortuous geometry on stress values and distribution during the peak systolic phase. (A) The deviation from the straight pattern of the conduit (B) causes different flow fields near the central ostium, sequestration of higher velocity areas near the curve (A), and different stress values between the 2 configurations (C, D). Accordingly, one can detect different shear stress values in the curved iliac limbs of an endograft anteriorly (E) and posteriorly (F) compared with the rest of its surface. The color version of this figure is available online at www.jevt.org .
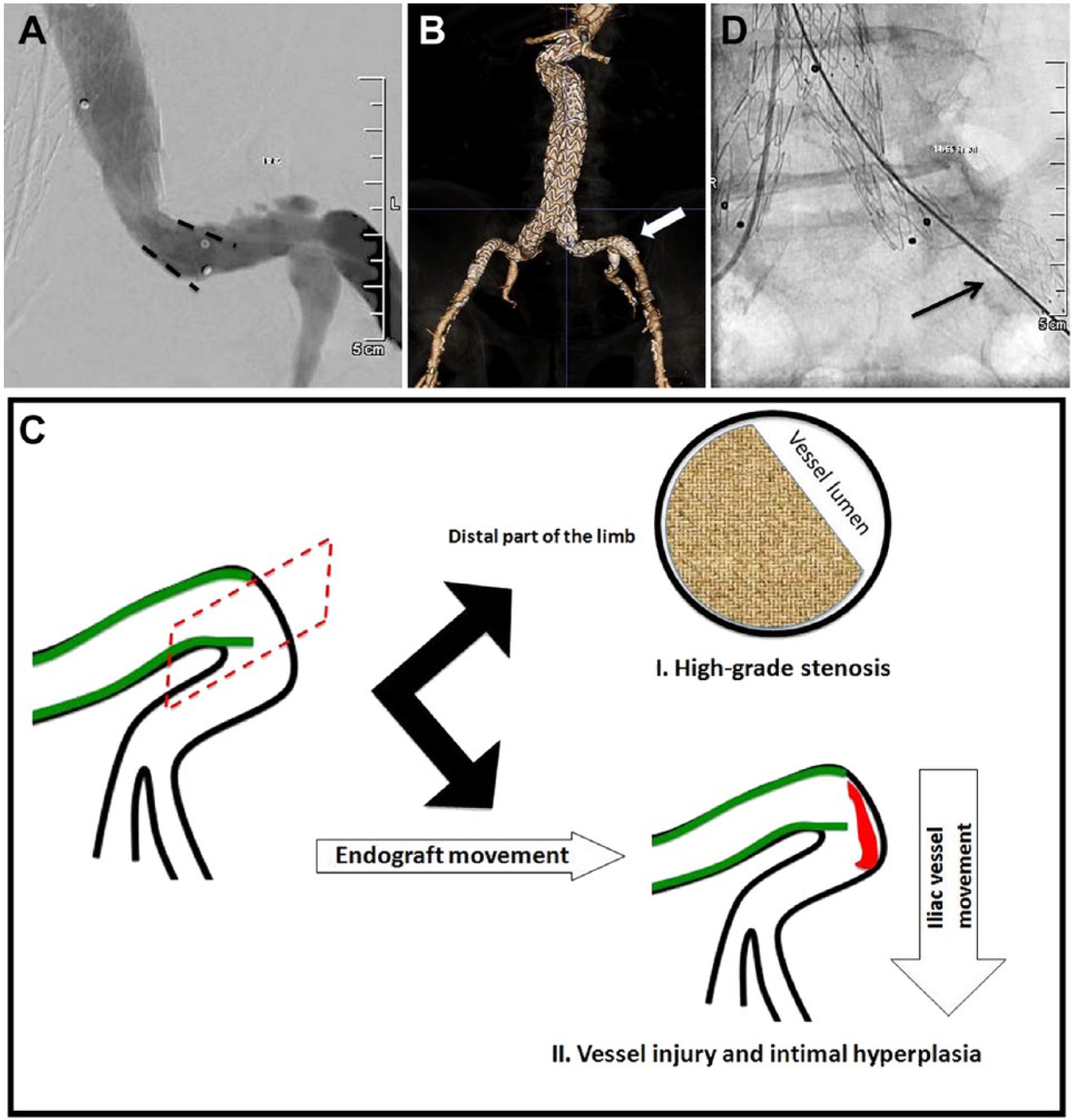
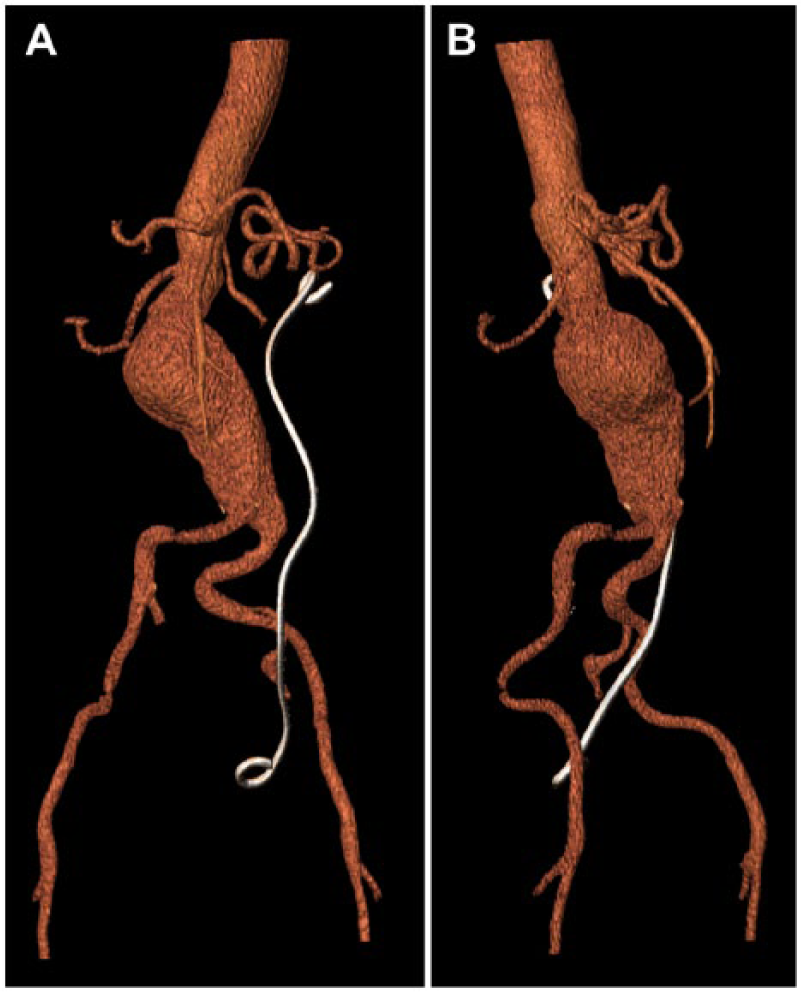
Suboptimal apposition of the iliac limb (arrow) in a tortuous artery (dotted lines) shown on angiography (A) and in a 3-dimensional reconstruction (B) of an abdominal aortic aneurysm treated endovascularly (arrow). (C) Possible mechanisms leading to limb occlusion involve either high grade stenosis due to reduction of the vessel lumen or vessel injury and intimal hyperplasia (red area) associated with the different directions of endograft and artery movement during the cardiac cycle. (D) Such suboptimal apposition may be addressed with placement of an additional self-expanding stent extending to the straight segment of the external iliac artery (arrow). The color version of this figure is available online at www.jevt.org .
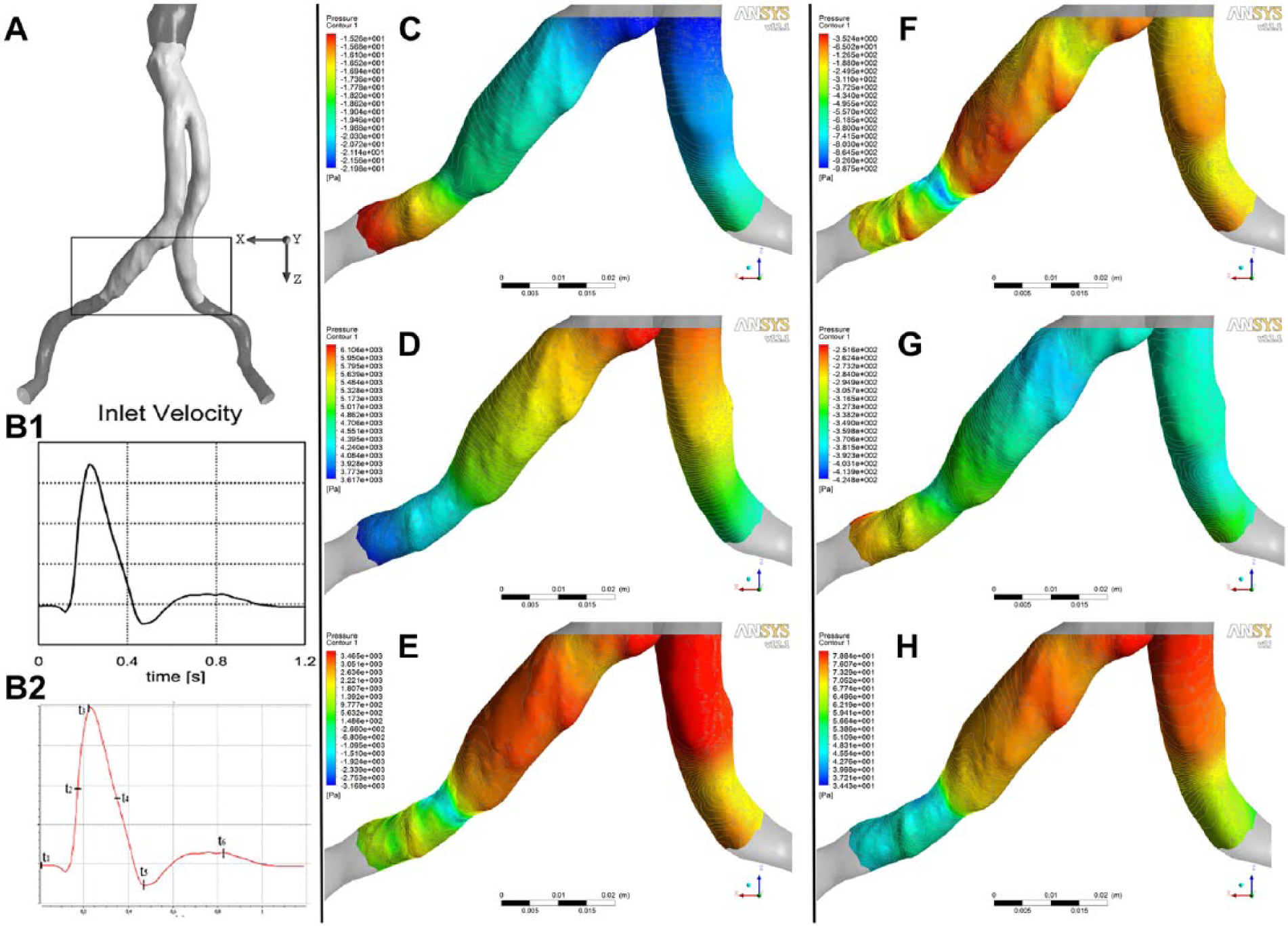
(A) Computational reconstruction of patient-specific endograft geometry to study the pressure distribution at the iliac limbs. The white segment represents the endograft while the gray upper and lower segments represent the inlet (aorta) and outlet conduits (iliac vessels), respectively. The studied iliac segments are depicted within the black frame. Note that the distal end of the right iliac limb is fixed in a stenosed area. (B1) The flow waveform used for the calculations in the endograft model. (B2) Six distinct phases are noted in each cardiac cycle: t1 depicts late diastole, t2 the accelerating phase, t3 the peak systolic phase, t4 late deceleration, t5 end-systole, and t6 the early diastolic phase. (C–H) The pressure distribution varies between the distal parts of the stenosed right and the normal left limb. The variation becomes more prominent in early and late diastole, as well as in the late deceleration phase, imposing difference stresses. The color version of this figure is available online at www.jevt.org .
Notably, the hemodynamic effect of excessive oversizing of iliac limb diameters with respect to the native vessel can be described by the same model. Indeed, Chen et al 28 showed that the stent/vessel size mismatch can induce endothelial flow disturbances and intramural wall stress concentrations that correlate with the extent of neointimal hyperplasia and stenosis at the distal end of the iliac limbs. The gradual development of these phenomena seem to coincide with the fact that a certain percentage of limb occlusions do not occur within the first days or weeks but can rather appear up to 12 months after EVAR. Indeed, van Zeggeren et al 12 report that 35% of the iliac limb occlusions in their series of 496 patients treated with the Endurant device took place between 2 and 12 months after EVAR, with another 10% after 12 months. Similarly, Bisdas et al 27 identified limb occlusion as the leading cause for reintervention in a series of 273 patients treated with the Endurant endograft in a median follow-up of 42 months; only half of the reinterventions were performed early (<1 year), while 15% of patients were subjected to late secondary procedures after 4 years.
Ongoing Post-EVAR Change in Iliac Geometry
Deployment and fixation of an endograft within an AAA cause conformational changes in the aortoiliac anatomy, not only in the angulation of the neck but also in the tortuosity and angulation of the iliac arteries.29 –31 Krämer et al 30 estimated an average angulation change in the right (incorporated) limb of 6.43°±9.56° and −0.43°±12.94° in the anteroposterior and lateral projections, respectively, over the first 24 months postoperatively. Accordingly, the contralateral (left) limb showed an average change of 1.38°±21.03° on anteroposterior projection and 11.71°±15.75° laterally. Coulston et al 31 have recently shown alteration of aortoiliac tortuosity as a direct consequence of EVAR. The degree of the consequent postinterventional reduction in aortoiliac tortuosity depended on the type of endograft. Moreover, the aortoiliac tortuosity was identified as a prognostic factor for iliac complications (ie, kinking and/or occlusion). The aforementioned geometrical changes in iliac geometry and the interaction with the implanted endograft limbs necessitate the comparison and improvement of the iliac limbs’ conformability and flexibility. Until recently, clinical reports were restricted to the performance of iliac limbs with respect to reintervention causes and rates as well as to their configuration during completion angiography. However, recent basic research highlighted the influence of stent designs on the flexibility of endograft limbs and depicted their role in the resistance to (1) sideways displacement forces, (2) maximal stresses on stents, and (3) maximal strains on the fabric of the endograft limbs. 32
Estimating Iliac Tortuosity
The prognostic role of iliac angulation and tortuosity in early and late post-EVAR iliac events should be thoroughly studied, since not only may they be responsible for complications formerly attributed to small EIA diameter, but they also suggest the need for primary stenting if the distal limb edge is placed onto a tortuous iliac landing zone.2,33 Moreover, their influence on preprocedural EVAR planning and endograft choice should gain further attention. At present, the endograft instructions for use determine the minimum iliac diameter and fixation length, yet none defines the appropriate iliac angulation and/or tortuosity.
The major impediment to this task remains the poor calculation method and interpretation of the tortuosity index. This is illustrated in the definition inconsistencies between the different studies and in the confusion caused by the interchangeable use of the terms “tortuosity” and “angulation” (Figure 5), the latter associated closely with kinking of the iliac limbs (Figure 6). Possible measurements of tortuosity in the literature include the distance factor, the number of inflection points, the angle change along segments, and various line integrals of local curvature values. However, none of them has been accepted universally.34,35 Notably, easier but equally accurate methods have been also proposed, that is, taking into account the shortest distance between the aortic bifurcation and the common femoral artery on axial computed tomography scans as a surrogate for the calculated tortuosity index). 36 According to Johnson and Dougherty, 37 a tortuosity calculation needs to be invariant with respect to the translation, rotation, or scaling of a vessel in order to be clinically meaningful. On the other hand, tortuosity should be sensitive to the morphology of the vessel. In this way, a vessel with extreme angulations and another that bends gradually yield different tortuosity indexes, thus avoiding misleading calculations. 33 Modern 3-dimensional software programs enable the extraction of the AAA centerline with minimum operator training required. 38 Therefore, an automated estimation of tortuosity is now more feasible than ever and can lead to delineation of its association with migration and thrombotic phenomena and successful prediction of graft-related complications.
Three-dimensional reconstruction of an aortic aneurysm. While the coronal plane (A) shows angulation of the right iliac artery, the sagittal plane (B) unveils significant tortuosity of the right iliac axis. The color version of this figure is available online at www.jevt.org .
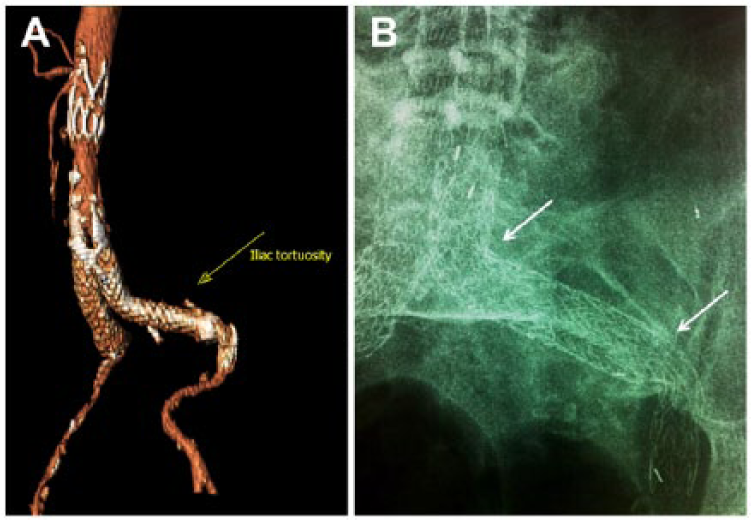
A case of abdominal aortic aneurysm treated with the Ovation endograft system. The presence of concomitant internal iliac artery aneurysm dictated the use of an iliac extension to the external iliac artery. While the tortuosity of the iliac limb is not excessive (A), the extension to the external iliac artery meets severe angulations (arrows) (B), which constitute a risk for limb thrombosis, irrespective of the external iliac artery diameter. The color version of this figure is available online at www.jevt.org .
In conclusion, it becomes apparent that limb occlusion will tend to become the primary cause for reintervention in the long term, so further research should focus on comparing spiral, circular, and Z-shaped stents of various amplitude and density in distribution.32,39 However, since the comparative studies (computational simulation or bench-testing) have been performed in rather plain geometries, ongoing research to compare mechanical properties in more complex geometries is awaited. 40
Footnotes
Acknowledgements
We thank Antonios Xenakis, MEng, MSc, for providing the images of pressure distribution at the iliac limbs and helping with interpretation of the experimental results.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.