
Abstract
Keywords
Endovascular aneurysm repair (EVAR) has become the treatment of choice for infrarenal abdominal aortic aneurysms (AAAs). Successful endovascular repair of AAAs depends on correct selection of patients based on their vascular anatomy, choice of the correct endoprosthesis, and familiarity with endovascular techniques and procedure-specific complications.
Endovascular aneurysm repair, however, is complicated by endoleaks in 20% to 25% of patients1,2; as many as 10% require reintervention due to type I endoleaks seen on 30-day surveillance imaging. 3 Traditionally, type I endo-leaks have required immediate attention to prevent aneurysm rupture. When a type I leak is observed during the completion angiogram, ancillary maneuvers (eg, balloon angioplasty, extension cuff deployment, or Palmaz stent implantation) may be used at the level of the leak to achieve the requisite seal. However, there are some cases in which an intraprocedurally identified type I endoleak have been observed. Kim et al 4 found a type I endoleak in 11.6% of their EVARs on completion angiography. After repeated balloon molding that diminished the endoleaks in 8 patients, the authors conservatively followed them and found that 7 endoleaks sealed within 2 weeks, whereas the eighth patient required transarterial coil embolization 1 week after EVAR. Bastos Gonçalves et al 5 recently reported their experience with type I endoleaks that spontaneously sealed during follow-up. Specifically, sealing was observed on the first post-EVAR computed tomography (CT) at 1 week in 8 of 15 patients and in another 6 patients within the following median 5-month follow-up. They conclude that a conservative approach for primary type Ia endoleaks may be justified in selected patients. 5 This approach, of course, should be taken with caution since the authors also revealed that fatal rupture occurred in 1 patient.
In the case described by Gandini et al 6 in this issue of the JEVT, a type I endoleak occurred 7 months after successful implantation of an Ovation Abdominal Stent-Graft System (TriVascular Inc, Santa Rosa, CA, USA). Interestingly, the patient presented symptoms (left inguinal pain), and CT imaging revealed a type Ia endoleak and a contained rupture of the left common iliac artery, mandating immediate repair. The authors also observed that the endoleak seemed to correlate with the presence of partial inward collapse of the proximal sealing ring. They treated the endoleak with sac embolization utilizing a transcaval approach after a proximal extension failed to seal the endoleak. 6
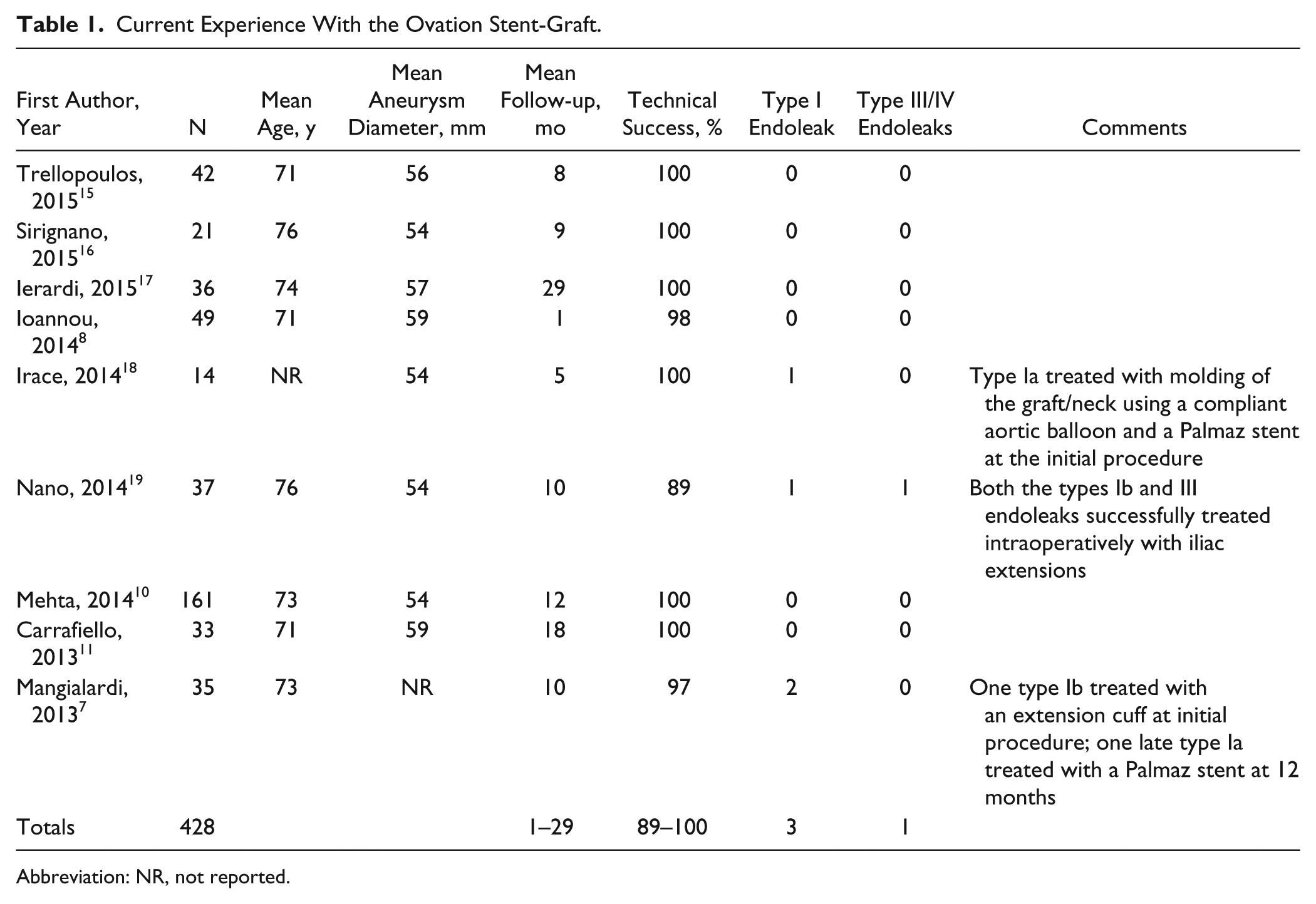
This is a very interesting article, and Gandini et al 6 should be commended on their overall management of this case. This article has two specific elements that deserve special comment. First, delayed type Ia endoleak with the Ovation stent-graft is very rare. Mangialardi et al 7 previously reported a delayed type Ia endoleak that they managed by deploying a Palmaz stent at 12 months (Table 1). Gandini et al 6 try to establish a connection between the possible structural change at the main graft O-ring and the development of the endoleak. The second notable component of this article is the authors’ use of a transcaval approach to treat this endoleak. We will discuss these two aspects in greater detail.
Current Experience With the Ovation Stent-Graft.
Abbreviation: NR, not reported.
Ovation Endograft Performance: Type I Endoleak
Stent-graft technology has evolved substantially over the past 20 years, yet most interventionists would agree that the ideal endograft is not among the currently available devices. The ability to accommodate to the aortic neck for seal and fixation, not only in straightforward cases but also in those presenting with short and angulated (often called “hostile”) necks, and to withstand aortic forces and prevent migration and endoleaks are the desirable advantages that newly developed systems aim to provide. In this regard, the Ovation endograft is a next-generation device that significantly improves on the limitations of earlier-generation models. Besides being ultra low profile (14-F delivery system), it offers a totally new perspective on the sealing-fixation philosophy. It was designed to overcome the limitations of currently available stent-grafts and deal with a broad range of aortoiliac characteristics, navigate through complex iliac and femoral accesses, and provide seal in complex proximal infrarenal aortic neck morphology.8 –11 The polymer-filled ring network conforms to the aortic neck, creating an uninterrupted concentric seal. Purportedly, this mechanism does not exert the kind of chronic outward force on the aorta that is seen with other stent-graft systems employing oversized self-expanding stents to achieve seal. It has been suggested that this radial force phenomenon exhausts the elastic recoil of the degenerating aortic wall, resulting in enlargement of the aneurysm neck with subsequent risk for type Ia endoleaks and/or device migration. 12 Moreover, the Ovation endograft seems to overcome limitations relevant to conical aortic necks since adequate sealing depends only on the first inflatable ring, provided that the neck portion at that point (13 mm below the lowest renal artery) does not exceed 30 mm. Diameter discrepancies along the aortic neck length do not compromise sealing, unlike other endografts. 13 This feature alone might increase EVAR eligibility by about 10%. 14
Experience with the use of the Ovation stent-graft is accumulating, with a number of publications reporting excellent technical success rates ranging between 97% and 100% for all7,8,10,11,15 –18 but one 19 report (Table 1). In the Ovation global pivotal study, Mehta et al 10 reported successful implantation in 100% of patients; 50% of subjects were treated percutaneously, without any access failures, type I or III endoleak, stent-graft migration, explant, or aneurysm rupture. Furthermore, at 1 year, there was no migration, type I or III endoleak, or conversion to open surgery. There was a 6% AAA-related secondary reintervention rate. 10 Similarly, Carrafiello et al 11 in a 3-center study, including initial results from our institution, reported a technical success rate of 100%; none of the patients required conversion to open surgery. Furthermore, at midterm follow-up, they found no aneurysm enlargement, rupture, fracture, migration, or type I, III, or IV endoleak. 11
From a total of 428 patients included in the previously published series,7,8,10,11,15-19 only 4 (0.9%) cases presented a type I endoleak,7,18,19 of which 2 (0.45%) where type Ia7,18 (Table 1). Of these 4 type I endoleaks, three were identified and managed during the initial EVAR procedure, whereas the fourth case 7 was discovered and treated at 12 months’ follow-up. All cases were successfully treated with molding of the graft/neck with a compliant aortic balloon, insertion of a Palmaz stent, or a limb extension (Table 1).
Initial success of any aortic stent-graft is dependent on proximal neck fixation, thus it is important to consider certain anatomical factors that predispose patients to both periprocedural and late type I endoleaks. Proximal neck angulation >45° to 60° and conical or very short aortic necks are strongly associated with proximal type I endo-leaks in some studies, whereas aortic neck diameter and distal attachment site diameter do not seem to play a role.20,21 Progressive aortic dilatation,22 –25 which may be exacerbated by oversizing and the radial force of self-expanding stents, can cause loss of fixation and seal. Supposedly, the Ovation polymer-filled O-rings should not contribute to neck dilatation in this fashion.
Gandini et al 6 observed that the proximal O-ring had “partially collapsed,” suggesting that the inward indentation of the ring most likely was the cause of the endoleak. A previous study performed at our institution revealed that the proximal O-rings often expand inward to a varying extent such that they may cause an inflow stenosis. 8 Although the current standard of 10% to 20% oversizing appears to be relatively safe 26 and is recommended in the Ovation’s planning instructions (15% to 20%), this practice may not be necessary with the Ovation device since by oversizing the graft we are cramming the inflatable rings, which are designed to expand to a specific diameter, into a smaller diameter aorta. Inevitably, if these rings cannot expand outward, they will expand inward toward the lumen, causing a stenosis. 8 Thus, sometimes the Ovation graft O-rings may not be perfect tubes mimicking the shape of the aortic neck but may have bends. We have seen this in a number of our cases, but it has not caused any sealing difficulties. The interesting aspect of the case presented by Gardini et al 6 is that this structural modification of the proximal rings was not present in the first follow-up CTs but occurred months later, even perhaps precipitating an endoleak.
Transcaval Embolization
While type I and type III endoleaks are usually treated with endograft-related procedures, type II endoleaks can be managed with transarterial embolization, direct puncture of the aneurysm sac, or transcaval embolization. The case presented by Gandini et al 6 was an aneurysm rupture due to type Ia endoleak. The authors attempted to treat the endoleak with the placement of a proximal cuff extension. This procedure was unsuccessful, possibly due to blood flow passing from above and external to the collapsed rings. In this scenario, the authors had three endovascular treatment options.
First, there is the transarterial embolization approach, which is the delivery of embolic agents through the superior mesenteric or internal iliac artery collaterals to the inferior mesenteric or lumbar arteries. Advancing the catheters to the aneurysm sac for intrasac embolization could be attempted; however, the procedure can be technically difficult and is plagued by high rates of recurrence (20% to 80%)27–29; in Gandini’s patient, who was treated as an emergency due to aneurysm rupture, it would be considered rather risky. Furthermore, bilateral embolization of the internal iliac arteries had been performed in the first operation, thus decreasing accessibility.
The second option would be the translumbar direct puncture of the aneurysm sac. This procedure has been shown to have better success rates in 70% to 90% of patients at 8 months.30,31 However, the patient would need to be transferred between the angiographic suite and the CT room and to change from a supine to prone position. A translumbar transcaval approach with CT guidance for right-side aneurysms and a transabdominal approach with ultrasonographic guidance have also been reported as alternatives to translumbar direct puncture of the aneurysm sac.32,33
The third option, the transcaval approach, which was the method used by Gandini et al, 6 requires no CT puncture guidance and is performed in the angiographic suite under fluoroscopic control. It is less time consuming, and the patient remains supine, which is suitable for a combined arterial transfemoral approach. Moreover, in the Gandini case, the patient had favorable anatomy due to the proximity of the sac to the inferior vena cava and adequate space between the aortic wall and the endograft for safe puncture.
Transcaval puncture has been proposed as a safe alternative to the translumbar approach for the treatment of type II endoleaks.34,35 Midula et al 36 proffered the use of a transseptal needle sheath system. This is a precurved 8-F profile set used for the puncture of the interatrial septum to gain left atrial access. It consists of an 18-G luminal stainless steel needle and a solid stainless steel stylet mounted on a precurved introducer set. The authors used the 50° angle.
Mansueto et al 34 suggested a dedicated set for transjungular intrahepatic systemic shunt, which requires a 10-F introducer sheath. Since there is no dedicated set for transcaval aneurysm sac puncture, Gandini et al 6 had to choose one of the two systems described previously, and they chose the second one, with an excellent final result. This is the first report to our knowledge of transcaval aneurysm sac puncture and embolization for a type I endoleak.
As any good article should, the report from Gandini and colleagues 6 raises questions: Should a type I endoleak in an Ovation stent-graft be aggressively treated or should conservative observation be initially attempted? If the endoleak persists, what is the next step? Hopefully, as experience accumulates and further studies are published, the answers to questions such as these will be provided.
Conclusion
A type I endoleak is a significant complication that causes increased morbidity and mortality. The O-rings incorporated in the Ovation stent-graft to seal the proximal neck seem to protect against type I endoleak, but if it occurs, its management may be challenging. Changes in graft structure should be carefully noted and followed since this may cause a loss in seal. Gandini et al 6 have utilized their experience with the transcaval approach in type II endoleaks to successfully adapt the technique to treat type I endoleaks as well. The transcaval embolization approach may serve as a helpful addition to our armamentarium and aid in the treatment of both early and late endoleaks. It is imperative that the interventionist be aware of the available tools for diagnosis and treatment of type I endoleaks in order to recognize and treat this complication expeditiously and in a controlled manner to avoid costly and potentially devastating complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.