
Abstract
Introduction
Endovascular interventions are the first-line option in the treatment of uncomplicated stenotic lesions in the femoropopliteal segment.1,2 Compared with stents or balloon dilation, mechanical atherectomy catheters decrease the plaque burden and barotrauma, while achieving similar patency rates with a reduced need for bailout stent placement compared with primary angioplasty.3–5 Although the immediate clinical success of peripheral interventions in general is very high, long-term patency continues to be undermined by restenosis.
Approximately 1.5 million patients undergo peripheral interventions for peripheral artery disease (PAD) in the United States each year, 2 and 90% of symptomatic PAD patients have femoral and popliteal artery disease, 6 so determining the most effective therapy for femoropopliteal lesions and reducing the incidence of restenosis are of vital importance. The impact of deep injury to the adventitial or medial layers created by excisional atherectomy has not been studied as regards restenosis. We sought to investigate the effect of atherectomy-induced adventitial or medial injury on the 1-year duplex-documented primary patency in patients with and without histopathologically confirmed adventitial or medial injury.
Methods
In a study approved by the local institutional review board, 116 consecutive patients (mean age 69.6 years; 56 men) with femoropopliteal stenoses treated with directional atherectomy at a single center between 2007 and 2010 were retrospectively analyzed. Patients who presented with critical limb ischemia, chronic total occlusion, iliac disease, or no runoff to the foot were excluded. All patients had claudication (Fontaine stages IIa/b) and TASC (TransAtlantic Inter-Society Consensus) A/B lesions in the superficial femoral or popliteal arteries.
Atherectomy Procedure and Histology
All the procedures were performed by experienced interventionists after obtaining patient informed consent for the procedure. After assessing lesion characteristics (severity, lesion length, and degree of calcification) on the diagnostic angiogram, directional atherectomy was performed using the SilverHawk Plaque Excision System (Covidien/Medtronic, Mansfield, MA, USA). If the lesion was angiographically concentric, the cutter was first placed facing laterally, using the femur as the reference. From this position the cutter was rotated clockwise in a complete circle using the torqueing device to position the cutter posteriorly, medially, and then anteriorly to make cuts in lateral, medial, posterior, anterior wall. The cutter was always returned to the lateral position facing the femur; the device was then clocked into the desired position to avoid repeated cuts in the same plane. If the lesion was eccentric, the cutter was directed toward the lesion and away from the angiographically normal vessel wall.
According to institutional protocol, atherectomy specimens were obtained at the time of the procedure, placed in formalin, and sent to the pathology department, where the specimens were fixed in paraffin, sectioned, and analyzed using hematoxylin and eosin stain. All pathologists were blinded to the patient’s symptoms and other imaging data.
Endpoint and Definitions
The primary clinical outcome was the occurrence of restenosis at 12 months. For the purposes of this study, adventitial or medial deep injury was defined as the presence of medial or adventitial tissue within the plaque sample. The patients underwent clinical follow-up and lower extremity ultrasound at 3, 6, and 12 months; restenosis was determined by a peak systolic velocity ratio <2.4.
Statistical Analysis
All patients were dichotomized by the presence or absence of adventitial or medial cuts as evaluated by histopathology; the groups were compared using a chi-square or Student t test for categorical and continuous variables, respectively. The null hypothesis that the proportion of restenosis at 1 year in patients with adventitial or medial injury will be equivalent to the proportion of restenosis in patients without adventitial cuts was evaluated using a chi-square test. Variables of interest in the current dataset were first explored through visualization and inspection for potential outliers and distributional assumption. Associations were evaluated using logistic regression analysis; the final model included age and injury as covariates. Outcomes of the regression analysis are presented as the odds ratio (OR) and 95% confidence interval (CI). All analyses were performed using SAS software (version 9.3; SAS Institute, Inc, Cary, NC, USA).
Results
Baseline demographic and clinical features were similar between the groups (Table 1). Adventitial or medial injury was identified in 62 (53%) patients. There were no significant differences in lesion length (58.7±12.8 vs 56.2±13.6 mm, p=0.40), vessel runoff (1.9±0.6 vs 2.0±0.6, p=0.37), or reference vessel diameter between patients with and without adventitial or medial injury, respectively. The 1-year restenosis rate was significantly higher (p<0.0001) in patients with adventitial or medial injury (97%, 60/62) as compared with those without (11%, 6/54).
Patient Demographics, Comorbidities, Selected Blood Values, and Lesion Characteristics.
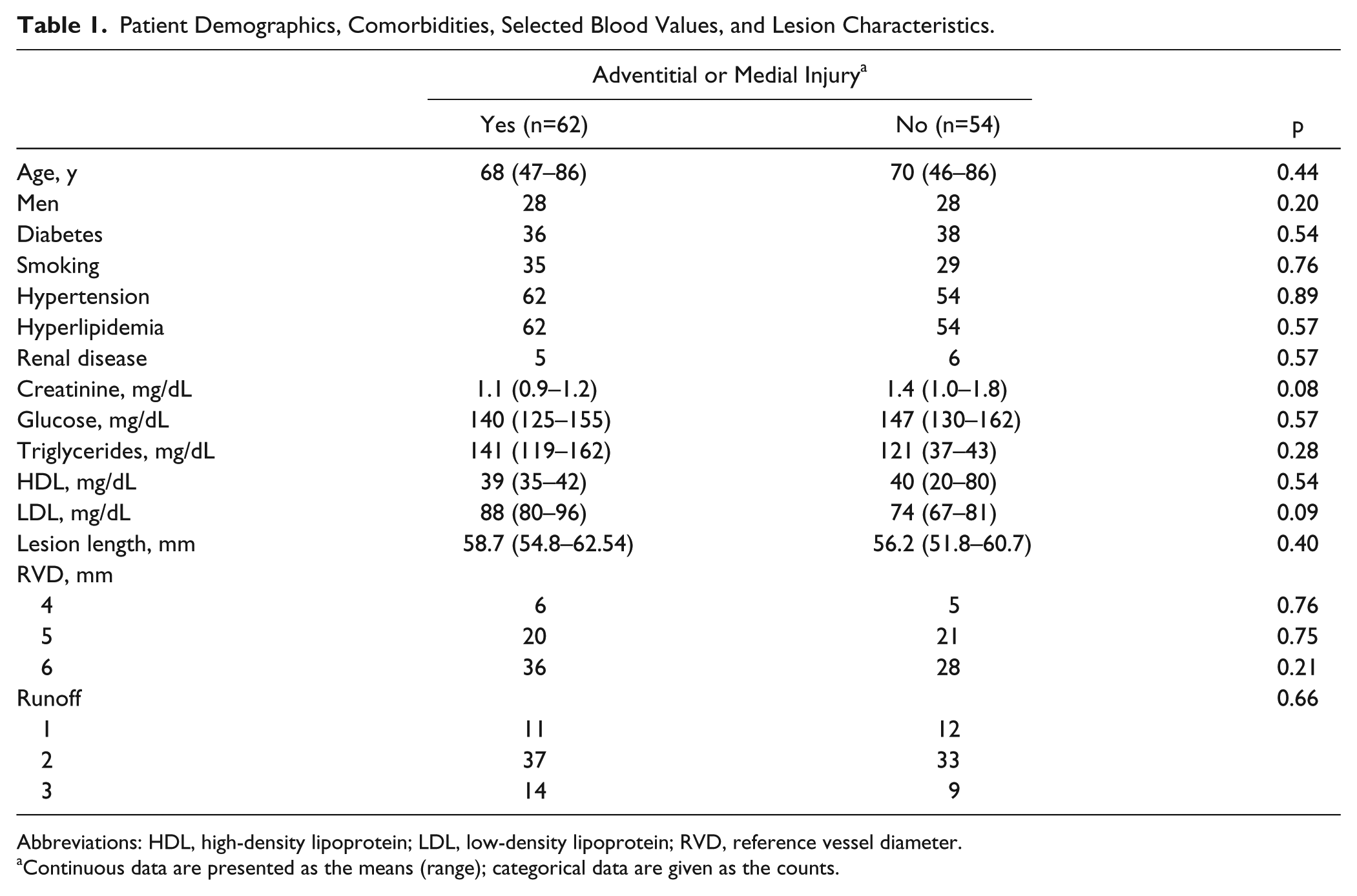
Abbreviations: HDL, high-density lipoprotein; LDL, low-density lipoprotein; RVD, reference vessel diameter.
Continuous data are presented as the means (range); categorical data are given as the counts.
In simple logistic regression analysis, adventitial or medial injury was strongly associated with restenosis (OR 228, 95% CI 43.97 to 999, p<0.0001). No covariates of interest or interaction terms were found to be significant on follow-up multivariate logistic regression (all p>0.05). The final model, which included age and injury as covariates, produced ORs of 270 (95% CI 46.89 to 999, p<0.0001) for injury and 1.04 (95% CI 0.96 to 1.12, p=0.33) for age.
Discussion
Excision of plaque has been shown to avoid the complications of traditional angioplasty and stenting, such as dissection, elastic recoil, and barotrauma, in the treatment of lower limb atherosclerotic lesions.3–5 For the SilverHawk system, reported patency rates have ranged from 54% to 84% in de novo lesions.3–5 It has been shown to have good procedure success as a standalone therapy or as an adjunct to angioplasty in short lesions; however, there is no difference in target lesion revascularization rates between patients treated with SilverHawk atherectomy vs balloon angioplasty.7,8 SilverHawk may facilitate optimal vessel expansion with low balloon pressures, preventing dissection and recoil and thus reducing the need for stents. 7 The reported bailout stent rates are 0% to 6% with atherectomy compared with 10% to 43% for balloon angioplasty alone. 8
The mechanism of SilverHawk restenosis remains poorly understood since it does not produce barotrauma, unlike its predecessor, the Simpson atherectomy catheter. However, the consequence of potential disruption of the internal and external elastic lamina during directional atherectomy is not known. It has been demonstrated in a porcine model that balloon injury in conjunction with disruption of the internal elastic lamina is associated with accelerated intimal hyperplasia vs overdistention without disruption of the internal elastic lamina. 9 This is consistent with our analysis of human peripheral restenotic plaques, which suggested that a breach in the structural integrity of the internal elastic lamina between the tunica media and the tunica intima is associated with increased neointimal proliferation, inflammation, and cellularity compared to de novo atherosclerosis. 10 This correlates with a biological response of cellular proliferation and repair resulting from deep injury leading to restenosis.
The role of deep balloon injury in restenosis has been studied in several animal models. The porcine model shows that postangioplasty overstretch causes proliferating adventitial myofibroblasts to migrate into the neointima 2 to 3 days after angioplasty and contributes to the mass of the restenotic lesion; after 14 days, the adventitial myofibroblasts proliferate, forming a fibrotic scar around the injury site. 11 In the canine aorta, balloon overstretch injury has been shown to produce a medial wall rupture similar to that seen in the porcine coronary artery system. 12 The adventitial or medial injury proliferation after injury is similar to the formation of neomedia containing smooth muscle cells and collagen fibers replacing the injured vessel wall, decreasing the luminal area and producing restenosis. 12
The traditional concepts of cell response to injury have changed, from abluminal to adluminal origin, implying an adventitial or medial role in response to injury.12–14 Deep injury during directional atherectomy may trigger restenosis by the disruption of internal and external elastic lamina integrity. Theoretically, there is no barotrama, no chronic irritation by a stent, and no stretch injury or spiral dissection. We propose that directional atherectomy causes deep tissue injury resulting in aggressive restenosis. This is the first study that shows a significant correlation between the presence of adventitial or medial injury and restenosis after peripheral atherectomy. Specifically, our results suggest that adventitial or medial injury disruption is the primary cause of restenosis in TASC A and B lesions treated with directional atherectomy. However, our study is limited by its single center, retrospective nature and the lack of core laboratory adjudication.
Conclusion
Our study suggests that adventitial or medial injury results in aggressive restenosis. Devising a structured and careful interventional approach by avoiding adventitial or medial injury may serve to reduce restenosis after directional atherectomy. While our study clearly demonstrates the relationship between adventitial or medial injury to restenosis, further studies are needed to evaluate the effect of both imaging modalities and/or concomitant drug-coated balloons in preventing restenosis after directional atherectomy.
Footnotes
Declaration of Conflicting Interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.