
Abstract
Keywords
Introduction
The transradial approach (TRA) is an accepted standard of care for coronary artery interventions and has significantly reduced access site bleeding and major vascular complications leading to associated reductions in mortality, morbidity, and hospital stay costs. 1 For many patients undergoing diagnostic or interventional procedures, the shorter postprocedural monitoring, early ambulation, and less discomfort make TRA an attractive alternative to the transfemoral approach. 2
Recent data suggest that TRA may also be safe and efficacious for the treatment of selected above-the-knee peripheral lesions, particularly with the introduction of newer delivery catheter and sheath technologies.3-5 Perceived increases in radiation exposure, prolonged procedure times, and prohibitive lesion complexity or distance from the access site remain potential barriers to TRA uptake, along with concerns regarding major vascular complications and stroke. Nonetheless, in a number of studies of patients presenting with acute coronary syndromes, the estimated rates of major vascular complications occurring with TRA (hand ischemia, compartment syndrome, major bleeding) remain strikingly low, ~1.7% of cases, with stroke rates varying from 0.1% to 0.4%.6-9 The aims of this study were to compare safety and outcomes between radial and femoral approaches for aortoiliac and femoropopliteal lesion subsets and to examine factors that may predict radial artery approach failure.
Methods
Study Design
A single-center retrospective study was conducted involving 188 patients (mean age 66.4±10.8 years; 116 men) with lower limb claudication (158, 84.0%) or critical limb ischemia (30, 16.0%) who underwent aortoiliac (117, 62.4%) or femoropopliteal (71, 37.6%) interventions on 210 lesions over a 3-year period (2013–2015). All patients provided written informed consent for the procedures. Baseline patient and lesion characteristics are given in Table 1.
Baseline Patient and Lesion Characteristics. a
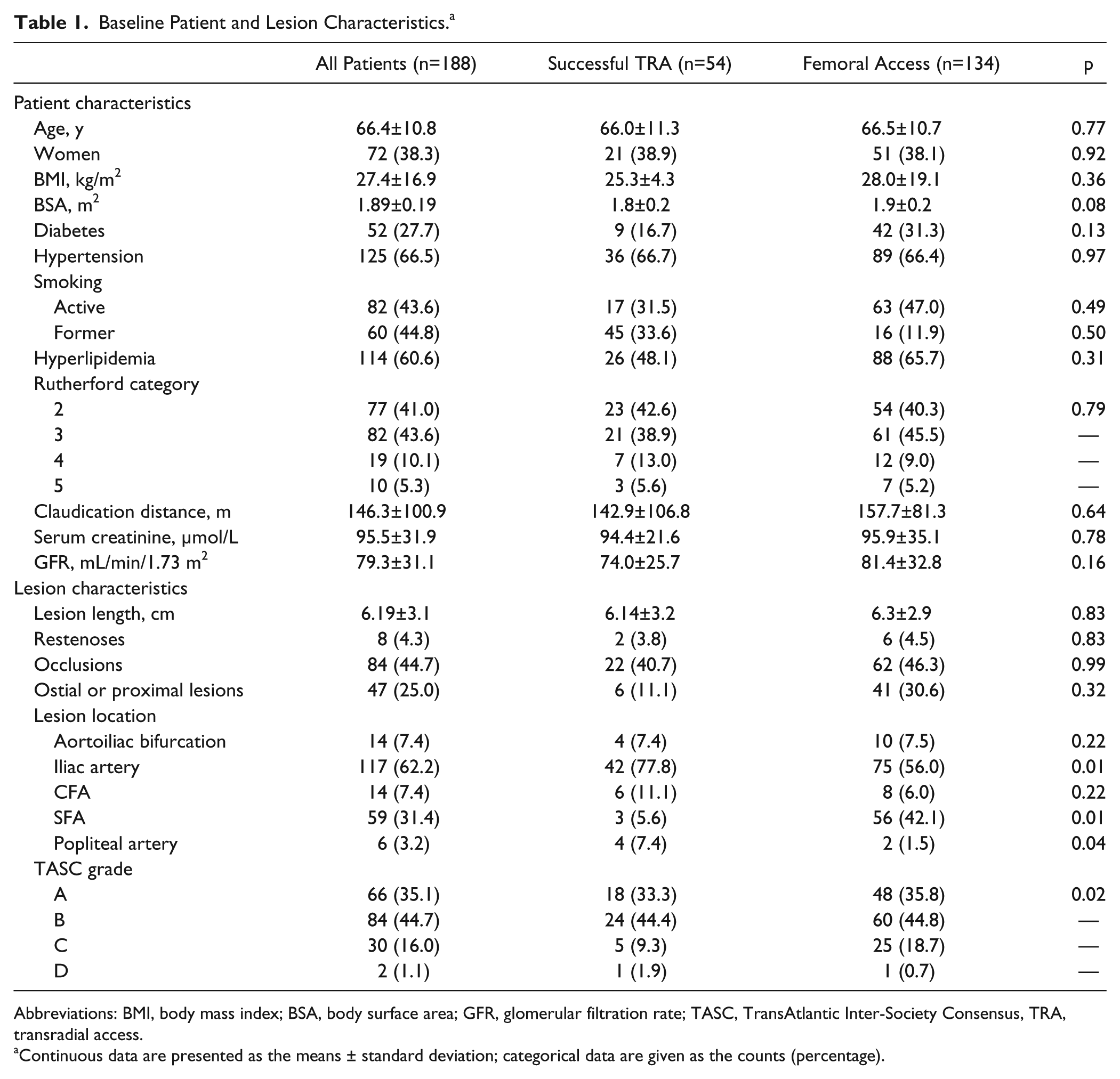
Abbreviations: BMI, body mass index; BSA, body surface area; GFR, glomerular filtration rate; TASC, TransAtlantic Inter-Society Consensus, TRA, transradial access.
Continuous data are presented as the means ± standard deviation; categorical data are given as the counts (percentage).
After angiography to characterize lesion severity,10,11 revascularization was ideally performed during the same procedure or at elective readmission, depending on the use of dual antiplatelet therapy and bed availability. Patients with more complex lesions [TransAtlantic Inter-Society Consensus (TASC) C or D with clear surgical contraindications] were discussed on a case-by-case basis in a multidisciplinary meeting among interventional radiologists, vascular surgeons, and interventional cardiologists. The choice of therapy (balloon angioplasty ± stent implantation) was determined by individual lesion characteristics and current guidelines.11-13
Suitability for TRA was determined on a case-by-case basis by operators who had performed >2500 transradial procedures, in accord with current operator proficiency recommendations. 1 TRA from the right radial artery was the preferred strategy when both approaches were equally suitable, but once a dedicated radial access support system for the left arm became available, left radial access became more feasible owing to operator comfort. Patients were excluded from TRA if they were known to have Raynaud’s disease, symptoms of upper limb claudication, absent pulses [in the setting of peripheral artery disease (PAD) and possible supra-aortic disease], or end-stage renal failure ± planned dialysis. Patency of the radial and ulnar arteries was assessed by palpation; in cases where the radial artery diameter was estimated to be small (<1 mm) or pulse pressure diminished, Doppler ultrasound was used. The Allen test was not routinely performed for examining collateral patency, as it has not been shown to improve transradial complication rates. 14
Interventions
All patients were pretreated with dual antiplatelet therapy [aspirin (100 mg/d) and clopidogrel (75 mg/d)] for at least 1 week before peripheral revascularization. Conscious sedation was achieved with weight-adjusted remifentanil unless contraindicated, whereby midazolam, diazepam, or ketamine was administered. Bolus unfractionated heparin (5000 units) was administered in all procedures to maintain an activated clotting time of 300 seconds.
For transfemoral access, the right and/or left femoral artery puncture site was identified using fluoroscopy, ultrasound, or anatomic landmarks, depending on operator preference. Cannulation was performed using a modified Seldinger technique. To treat infrainguinal lesions, antegrade wire insertion was guided by fluoroscopy, ultrasound, or both; a short 20-cm, curved, 4-F catheter (Bolia Mini-Cath; Terumo Corporation, Tokyo, Japan) was often used to navigate the wire to the superficial femoral artery (SFA). For retrograde procedures, iliac bifurcation crossover was performed using a hydrophilic wire, supported by a Judkins right or a right internal mammary catheter, where necessary. After wire placement, longer delivery sheaths were exchanged, where required (see Supplementary Table 1 for a listing of commonly used equipment for angioplasty/stenting; supplementary material available at http://jet.sagepub.com/content/by/supplemental-data ). Femoral artery puncture sites were closed using suture-mediated (ProGlide; Abbott Vascular, Redwood City, CA, USA) or collagen plug–based devices (AngioSeal or FemoSeal; St Jude Medical, St. Paul, MN, USA).
For the radial procedures, the patient’s right or left arm was supported using a dedicated radial access support system (CazaConfort Medical, La Teste de Buch, France) that attaches to any angiography table and reduces radiation scatter. The artery was punctured using the through-and-through technique15-18 in the distal third of the radial artery. A 10- or 16-cm dedicated hydrophilic radial sheath (Terumo Corporation) was inserted if diagnostic angiography was required. Vasodilators were routinely administered after sheath insertion to prevent arterial spasm (1 mg nicardipine hydrochloride and 1 mg glyceryl trinitrate). If arterial spasm did occur, intra-arterial injections of either glyceryl trinitrate or intravenous incremental doses of fentanyl (0.25–0.5 µg/kg) or propofol (0.1–0.15 mg/kg/min) were administered.
A 5-F or 6-F multipurpose catheter or coronary diagnostic catheter (3.5-F Judkins right, multipurpose, or 4.0-F Judkins left) was used to support wire passage to the descending aorta. Tortuosity at the subclavian bifurcation or aorta was usually overcome by asking the patient to perform a simple breath-hold maneuver. Accessing the descending aorta from the right TRA was performed in the anteroposterior or left anterior oblique 30°–40° projection, with gentle clockwise rotation of the catheter.
A catheter exchange over the wire was performed using the syringe injection/jet injection technique 19 to introduce a long (90–110 cm) hydrophilic sheath [Flexor or Shuttle (Cook Medical, Bloomington, IN, USA) or Destination (Terumo)]. The lesion was usually crossed directly or with the support of a 3.5-F Judkins right or multipurpose catheter to guide the direction of the wire, where necessary (Supplementary Table 1). For all radial procedures, and the majority of femoral interventions, a premounted radiopaque ruler board was used to guide balloon and stent deployment to avoid geographic lesion miss. Roadmap software was also used where necessary. No reentry or atherectomy devices were used for any of the chronic total occlusions (CTOs). Hemostasis of the radial artery puncture sites was obtained with an inflatable compression hemostasis band (TR-Band; Terumo Corporation).
Follow-up
Access sites for all patients were reviewed by clinical examination at hospital discharge and again at 4 to 6 weeks after the procedure. Where radial artery occlusion was suspected, patency was confirmed using duplex ultrasound, which was also used to investigate questionable femoral artery patency (bruit, palpable mass, diminished pulses, pain).
Definitions
Lesion characteristics were classified according to standard definitions recommended for peripheral endovascular revascularization trials.10,20 The degree of lesion calcification was classified using the Peripheral Academic Research Consortium criteria.10,21
FA failure was defined as the need to switch to the contralateral femoral artery for any reason to complete the procedure; TRA failure was confirmed if lesion crossing was not achieved and any form of alternative access was required to complete the procedure.
Major access site vascular complications included vessel perforation, occlusion, pseudoaneurysm, arterial dissection, compartment syndrome, retroperitoneal hematoma, hematoma >5 cm, need for blood transfusion, hemoglobin drop >3 g/dL, or any event that required a vascular intervention as defined by the Quality Improvement Guidelines for Vascular Access and Closure Device Use. 22 Stroke was defined as a new, persistent, neurological disability lasting >24 hours and confirmed on cerebral imaging. Length of stay <24 hours was considered 1 day.
The radiation exposure measures of fluoroscopy time, air kerma, and dose area product (DAP) were recorded automatically from individual catheter laboratory radiography systems [General Electric Medical Systems (Milwaukee, WI, USA) or Siemens (Erlangen, Germany)], as was the volume of iodinated contrast used.
Statistical Analysis
Demographic and clinical data were expressed as mean ± standard deviation or median (interquartile range) in the case of nonnormally distributed variables. Groups were compared using the chi-square, Student t, Fisher exact, or Mann-Whitney U test as appropriate. Univariate and multivariate logistic regression models were used to identify any independent predictors of radial artery access failure. The Hosmer-Lemeshow test were used to analyze goodness of fit of the model, and p<0.05 was considered the threshold of statistical significance. Analyses were conducted using SPSS software (version 23; IBM Corporation, Somers, NY, USA).
Results
The FA approach was used in 123 (65.4%) patients initially, and the radial approach was attempted in 65 (34.6%) patients. Details of the procedures are given in Table 2. Eleven (16.9%) of these access attempts failed compared to 9 (7.3%) failures among the 123 patients having primary FA (p=0.42). FA failure was due to chronic occlusions in 5 patients and challenging aortic bifurcation anatomy requiring further support in 4 patients. TRA failure was due to occlusive lesions requiring alternative equipment in 9 patients and to unexpected tortuosity of the aortic arch vessels in 2 patients. All crossovers from TRA were successfully treated via the FA. There were no cases of severe radial artery spasm that prompted conversion to FA.
Procedure Characteristics.
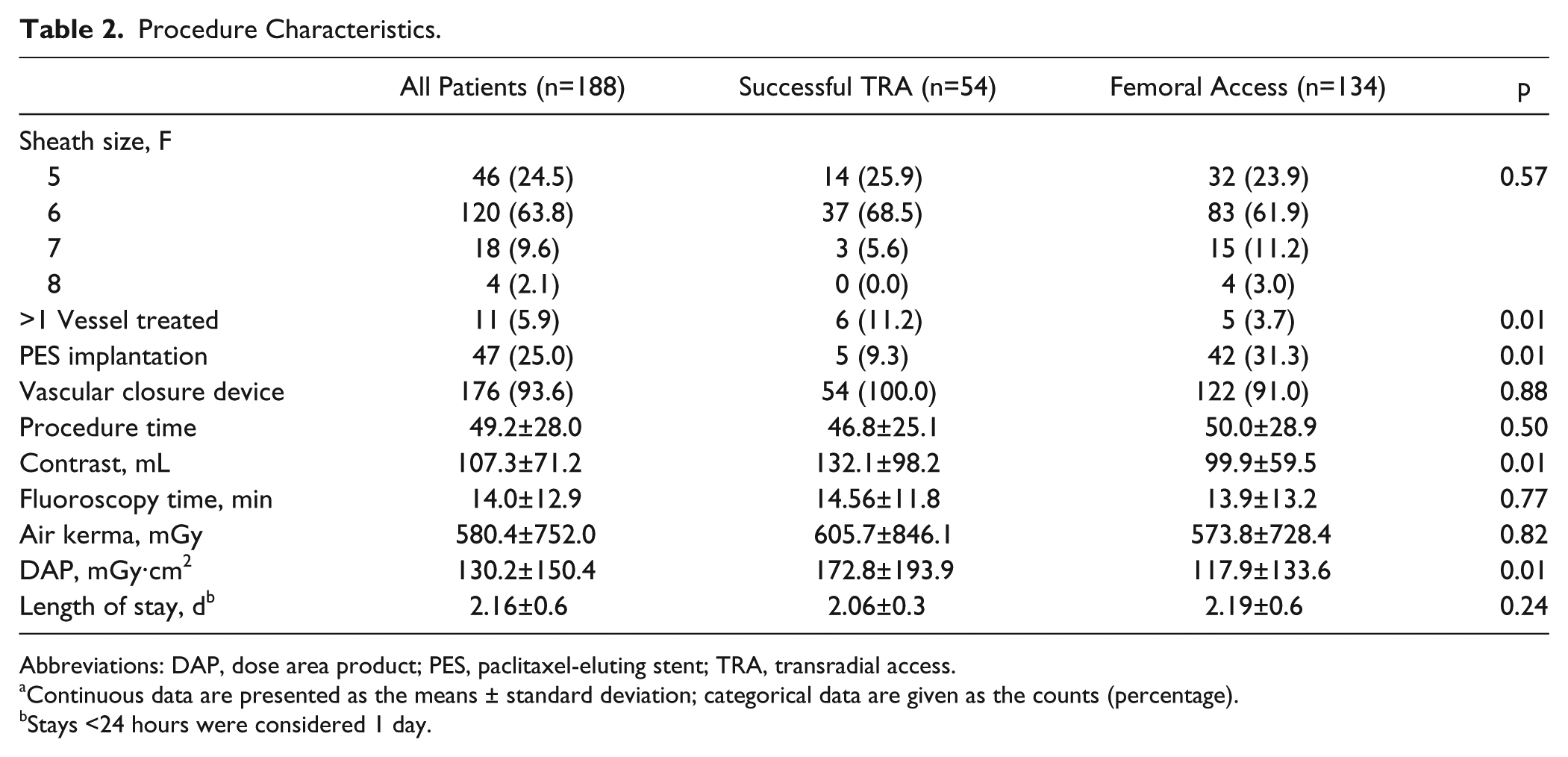
Abbreviations: DAP, dose area product; PES, paclitaxel-eluting stent; TRA, transradial access.
Continuous data are presented as the means ± standard deviation; categorical data are given as the counts (percentage).
Stays <24 hours were considered 1 day.
From the TRA intention-to-treat cohort, 53 (81.5%) patients had the approach from the right radial artery, with 44 (83.0%) successful. Twelve (18.5%) patients had attempted left radial artery access, with 10 (83.0%) successful. There were no differences in radial procedure success rates between the left and right sides (p=0.97). Importantly, the left radial artery approach was associated with less use of fluoroscopy (p=0.002) and thus lower radiation exposure (p=0.02 for air kerma and p=0.001 for DAP; Table 3).
Comparison of Radiation and Contrast Exposure for Successful Right and Left Transradial Approaches.
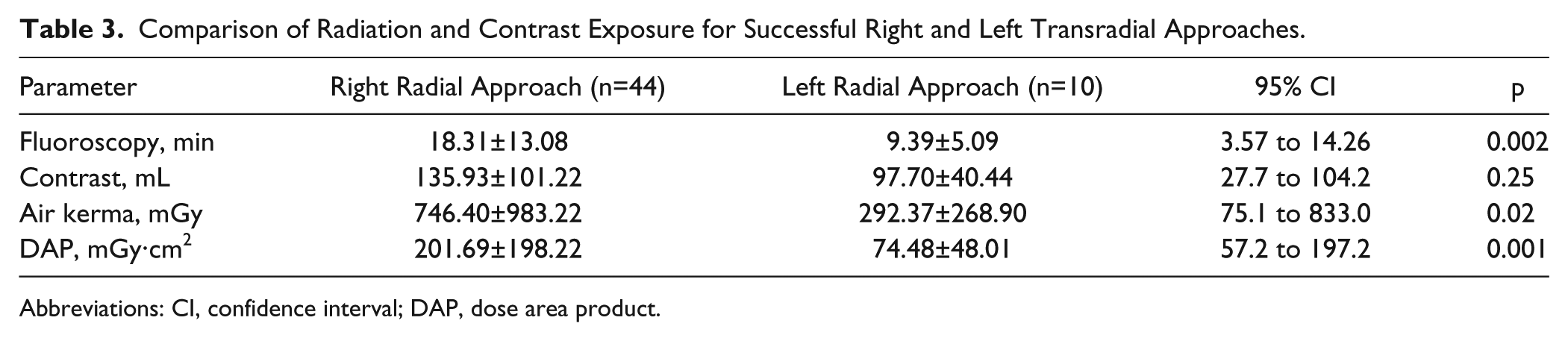
Abbreviations: CI, confidence interval; DAP, dose area product.
Of the 46 aortoiliac lesions treated successfully via the TRA, 38 (82.6%) had balloon angioplasty ± stent insertion with devices ≥7 mm in diameter. When analyzed by anatomic lesion subsets, there were no significant differences between TRA and FA in terms of radiation dose exposure (air kerma or DAP) for aortoiliac vs femoropopliteal lesions, which accounted for 24% (n=13) of successful TRA interventions (p=0.58 and p=0.39, respectively). Importantly, successfully treated TRA and all FA cases had no significant differences in lesion lengths, ostial or proximally located lesions, or CTOs (Table 1).
TRA Failure Analysis
In the TRA fail/crossover group, there were no significant differences between the composite of TASC lesion grades and TRA failure (p=0.12). Seven (63.6%) of 11 TRA failures were in CTOs, while CTOs accounted for 22 (40.7%) of 54 successful TRA cases (p=0.16). Similarly, degrees of lesion calcification (moderate/heavy vs mild/none) did not correlate with TRA failure (p=0.70). All attempted iliac bifurcation lesions were successfully treated using TRA, while the majority of failed TRA procedures occurred in iliac lesions located more distally [8/11 (72.7%) vs 42/54 (77.8%) successful TRAs, p=0.50]. Of the 4 SFA lesions treated via TRA, 1 was unsuccessful, whereas all 4 of the popliteal arteries attempted via TRA were successful.
For TRA failures converted to FA, contrast use was significantly higher (189.6±139.2 vs 102.0±61.7 mL, p=0.001) than TRA or FA, but fluoroscopy times (18.5±15.6 vs 13.7±12.7 minutes, p=0.23) and air kerma exposure (373.2±700.7 vs 590.1±754.7 mGy, p=0.42) were not.
In a multivariate logistic regression model looking at potential predictors of TRA failure (Table 4), none of the univariate factors retained significance (p=0.75 for the model).
Predictors of Transradial Access Failure From the Multivariate Model.
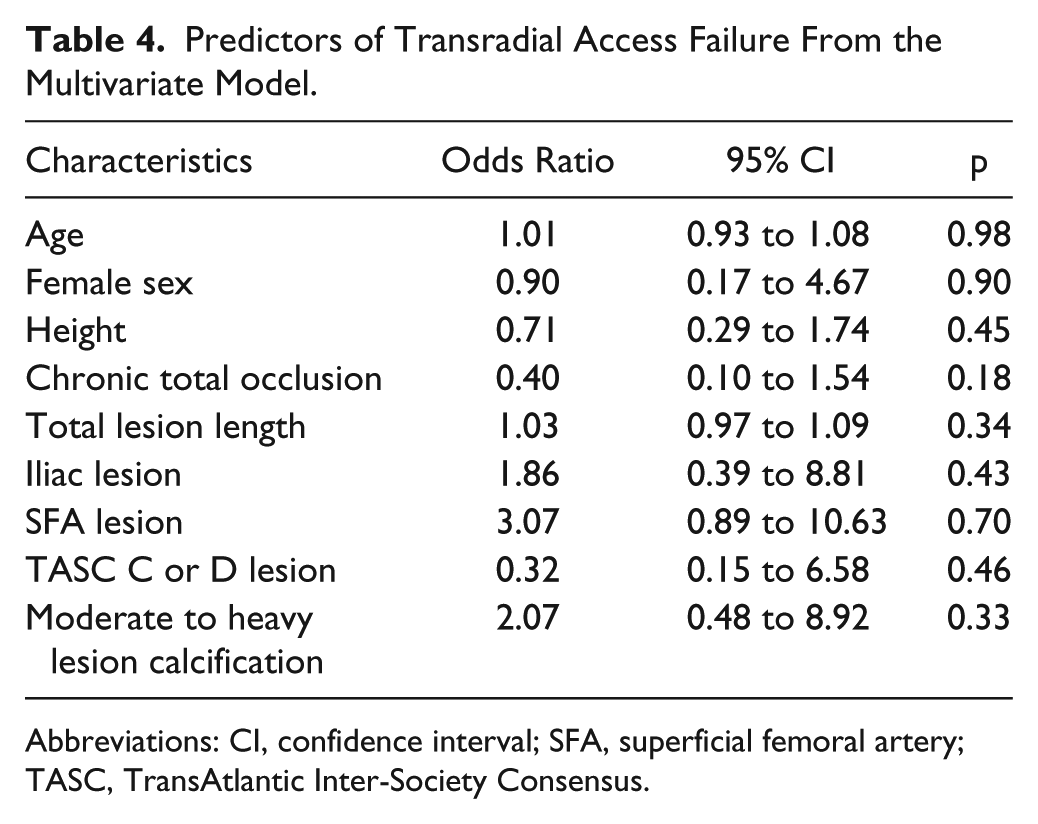
Abbreviations: CI, confidence interval; SFA, superficial femoral artery; TASC, TransAtlantic Inter-Society Consensus.
Complications
Access site complications diagnosed at hospital discharge or 6-week follow-up are presented in Table 5. For the major sequelae, there were no intraprocedural strokes, but 1 (0.7%) FA patient developed a hematoma >5 cm requiring surgical drainage (p=0.56). Two (3.7%) asymptomatic radial artery occlusions were detected (neither occurred in the TRA failure patients). In sum, access site complications occurred in 6.0% of the FA patients vs 3.7% of the TRA patients (p=0.12). Nonetheless, all vascular access complications occurring in the FA group required further intervention (percutaneous or surgical) compared to none in the TRA group (p<0.001). FA patients requiring access site reintervention had no significant increase in length of stay (2.91 vs 2.11, p=0.07).
Major Vascular and Access Site Complications for Peripheral Interventions Using the Transradial and Transfemoral Approaches. a
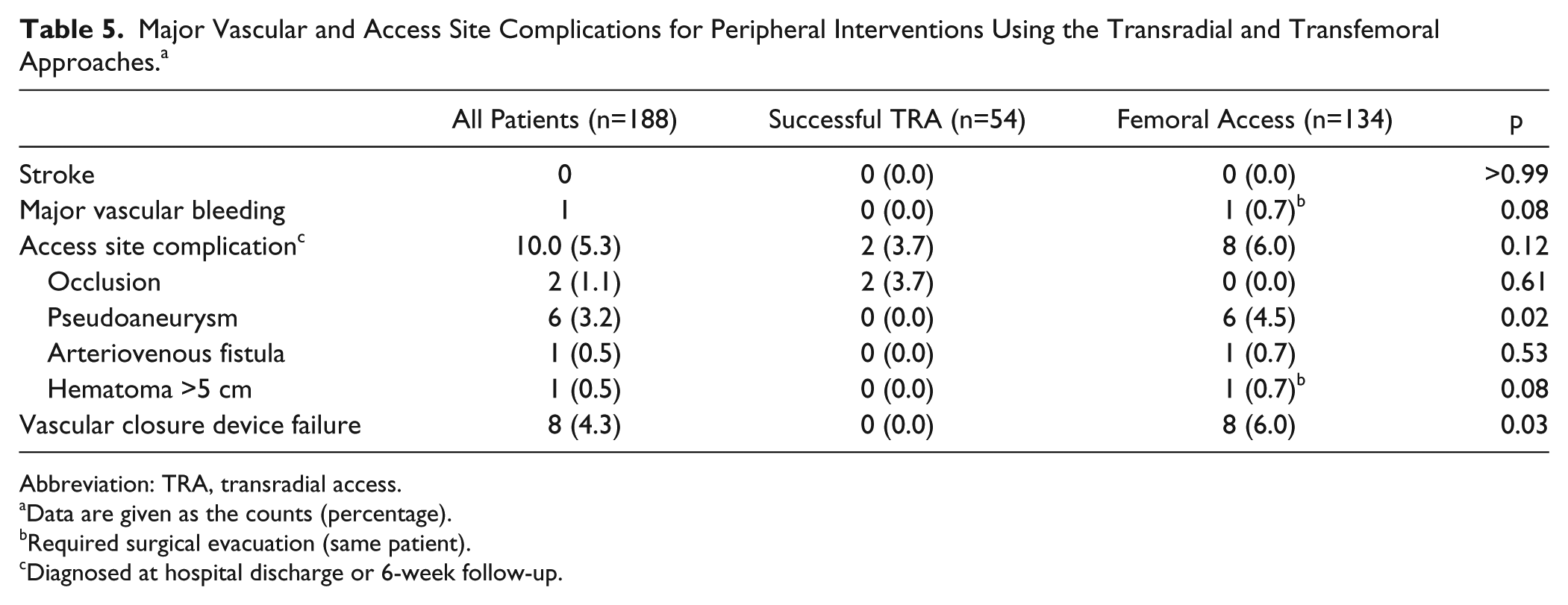
Abbreviation: TRA, transradial access.
Data are given as the counts (percentage).
Required surgical evacuation (same patient).
Diagnosed at hospital discharge or 6-week follow-up.
Discussion
In the present study, TRA was safe, with no strokes and a low complication rate compared to FA. Although the technical failure rate was higher for TRA, lesion complexity (length, presence of CTO, ostial or proximal lesions) was not associated with TRA failure, and there were no differences in radiation dose exposure for iliac and below-iliac artery lesion subsets treated by transradial or transfemoral approaches. In comparison to the right transradial approach, left transradial procedures are associated with shorter fluoroscopy times and lower radiation dose exposure but equal success rates. Notably, access site complications associated with FA require significantly higher rates of reinterventions.
This study extends findings from previous reports that TRA can be considered a safe and efficacious alternative to FA for the majority of above-the-knee lesions. Lorenzoni et al 4 studied 110 patients undergoing above-knee interventions primarily using the left radial artery (84, 76%) for TRA. Their overall treatment success rate was 91%, similar to results from this study. Asymptomatic radial artery occlusions (10.6% vs 3.7% in the current study) resulted in no adverse sequelae at 1-month follow-up and were likely due to the use of larger 8.5-F sheaths. However, using sheath sizes similar to the current study, the Italian Radial study reported a 2.7% rate of asymptomatic occlusions with no sequelae. 23 Considering that the average radial artery diameter ranges from 2.2 to 3.4 mm, 24 the findings from Lorenzoni et al 4 suggest that TRA using larger hydrophilic sheaths is feasible. There are also potential benefits for TRA in proximal iliac bifurcation or CTO lesions when an antegrade approach may reduce the risk of aortic dissections or for cases where the aortoiliac angle is unfavorable for crossover support. Furthermore, with TRA, the operator may treat bilateral lesions (eg, left iliac and right SFA lesions) during the same procedure while avoiding dual femoral punctures (Figure 1).
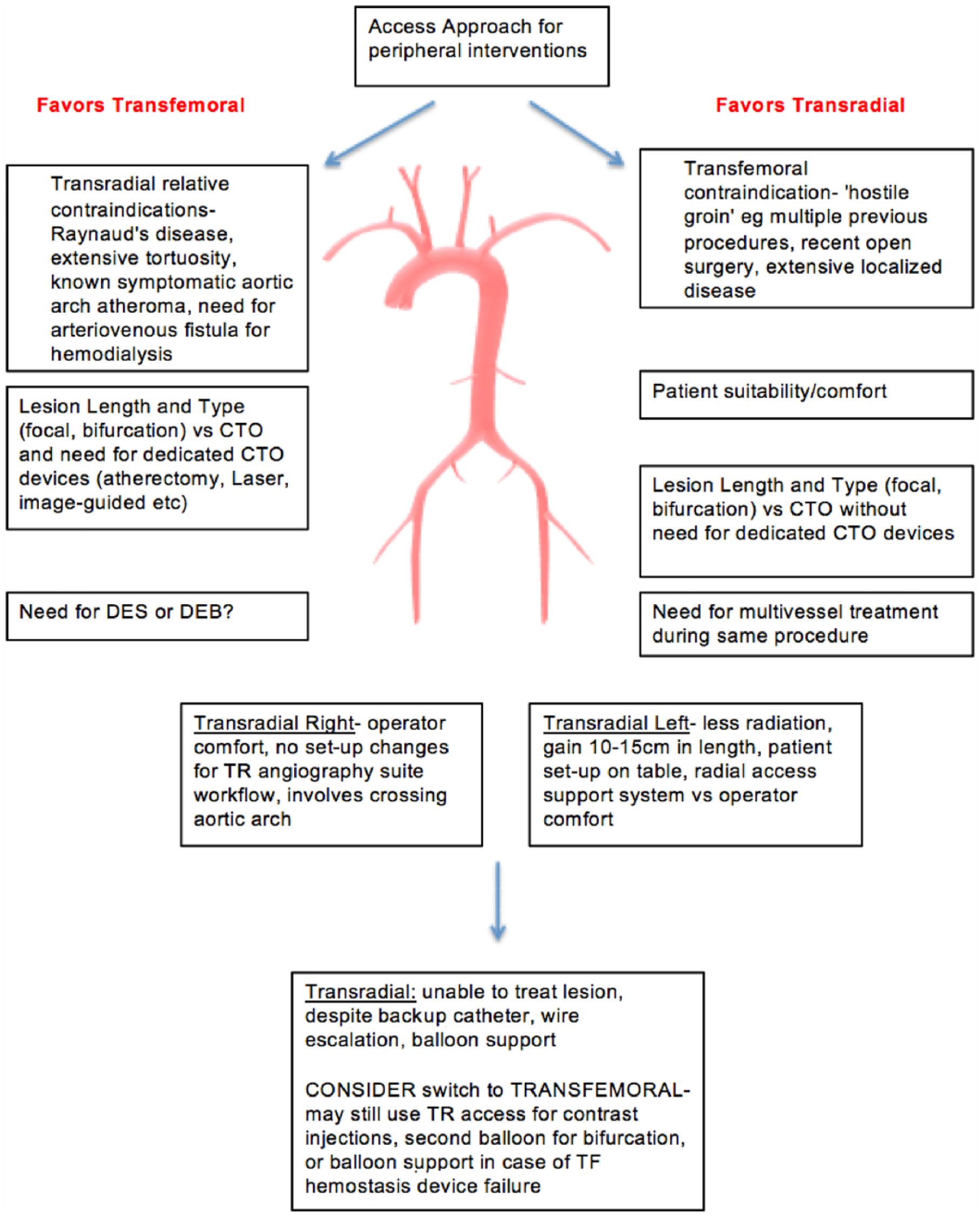
Algorithm for selecting the access route for peripheral interventions. CTO, chronic total occlusion; DEB, drug-eluting balloon; DES, drug-eluting stent; TF, transfemoral; TR, transradial; TRA, transradial approach.
Analyzing technical success achieved by the high-volume TRA operators in our center, there were no independent predictors of TRA failure. In the more heterogeneous population (n=149) from the Italian Radial study, 23 TASC D lesions, long lesions >30 cm, CTOs (length and anatomic location within the iliac artery not specified), as well as the use of guiding catheters instead of long sheaths, were all found to be independent predictors of TRA failure. Reassuringly, for the TRA failure group in the current study, fluoroscopy times and radiation exposure were not significantly higher than those treated successfully via TRA or FA, although contrast volume was increased. Increasing the use of roadmap programs, graded radiopaque marker boards or skin tape, and even CO2–based contrast alternatives may help to minimize excessive contrast use in these circumstances.
Stroke Risk
The stroke rate for this study was nil, similar to all but one of the published TRA peripheral intervention studies. In the exception, Coscas et al 5 reported 1 (4%) minor hemispheric stroke due a TRA procedure from the left radial artery in a small series of 22 patients. By comparison, stroke rates ranged from 0.1% to 0.5% for TRA (left or right) for large randomized controlled trials (RCTs) and registry studies for coronary interventions involving many thousands of patients.6,9
In order to prevent cerebrovascular complications during peripheral interventions, the practice adopted by many TRA centers, including ours, consists of (1) meticulous catheter preparation and deairing, particularly with smaller diameter sheaths (4-F to 5-F) that can tend to allow air entry during balloon or stent exchanges; (2) target ACT–guided (300 seconds) procedures to prevent catheter thrombus; (3) prevention or early treatment of arterial spasm to avoid excessive manipulation of catheters across the arch vessels; and for the same reason, (4) the use of hydrophilic catheters and sheaths. Operators should also consider avoiding TRA for known high stroke risk patients in whom significant aortic arch atheroma is suspected or documented while also selecting appropriate patients and optimal lesions for earlier stages in the learning curve for TRA.
Bleeding Complications
Major access site or procedural bleeding remains a key concern for peripheral endovascular interventions, often requiring percutaneous reinterventions that may be associated with adverse outcomes. There are no RCTs examining bleeding rates for TRA vs FA, so one must rely on data from this and other observational studies. Staniloae et al, 3 in a small observational study of 27 TRA vs 41 FA patients undergoing aortoiliac interventions, reported no transfusions for either group, but 7.3% had access site complications in their FA group. Similar to results from this series, the Italian Radial study reported no in-hospital major and 0.7% minor vascular bleeding episodes. 23 By contrast, in the largest study of its kind to date, Kimmelsteil et al 25 reported in-hospital outcomes of 23,934 patients undergoing above- or below-knee interventions via a femoral access, showing an 8.7% (2102 patients) rate of periprocedural blood or blood product transfusions. Given the associations between procedure-related transfusion and increased mortality,1,26-29 findings in such a large population warrant concern, justifying the need for RCT comparisons. While the authors did not specify the source of bleeding events (eg, access site vs other sites), minimizing bleeding risk should remain a key consideration when deciding on TRA or FA access options, particularly when accessing potentially diseased and calcified vessels.
Radiation Exposure
Previous reports examining cumulative radiation exposure suggest that procedural and fluoroscopy times may be increased with TRA. Given the potential increased risk of pathologies, such as cataracts, cerebral tumors, and lymphomas due to possible radiation exposure, much attention has been focused on methods to minimize unnecessary dosing, where possible. 30 Furthermore, the left radial artery compared with the right has been traditionally considered higher risk for dose exposure, mostly based on the assumption that procedures would take longer from that side, and that operators would have to lean over the patients, thus increasing radiation. Nonetheless, among the few peripheral intervention studies addressing radiation doses using TRA, Staniloae et al 3 reported fluoroscopy times between groups (TRA 30.4 vs FA 26.6 minutes, p=0.60) that were not significantly different, albeit longer than other studies, including ours. For the Italian Radial iliac intervention series, 23 average fluoroscopy time was 16 minutes and average procedure time was 64 minutes for 5 centers using equal numbers of left and right radial artery accesses.
For the current study, radiation doses were minimized by the use of strict radioprotective practices, including mandatory operator radioprotection certification, additive lead shields, dose minimization programs, and radial support boards that help prevent unnecessary exposure to body scatter from a left TRA. In addition, most of the above-knee procedures can be successfully completed using neutral C-arm projections, avoiding the steeper angulations that increase dose exposure. With these factors in mind, the left radial artery may still offer shorter procedure times and less radiation exposure for feasible peripheral lesions.
Limitations
This study is limited by its small population and retrospective design. Any significant findings may be prone to biases inherent for all observational studies, particularly given that the choice between TRA and FA was at the operator’s discretion based on individual case features, rather than a randomized process. Color duplex sonography was not routinely used by all operators for TRA or FA puncture guidance. Nonetheless, these findings remain largely consistent with other published TRA studies, both in the coronary and peripheral fields, and address key gaps in knowledge regarding lesion subsets treated by TRA peripheral intervention. Moreover, this study was conducted in a single center with high TRA volume where each operator had performed >2500 TRA procedures.
Conclusion
This study provides further evidence that transradial arterial access, in particular from the left radial artery, has comparative safety and efficacy to transfemoral access for peripheral interventions and is feasible for the majority of lesion subsets. Outstanding issues still remain regarding dedicated device lengths (in particular, short delivery systems for many current stents) and the need for appropriate RCT data.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Andrew K. Roy is supported by an unrestricted bursary provided by the Irish Cardiac Society Brian McGovern Travelling Fellowship fund.