
Abstract
Keywords
Introduction
During the past decade, endovascular aneurysm repair (EVAR) has gained wide acceptance as the preferred method to treat patients with suitable abdominal aortic aneurysms (AAA). 1 EVAR is associated with lower 30-day mortality and morbidity, faster discharge, and fewer complications than open repair, but reintervention rates are higher. 2 Long-term durability of EVAR depends on the maintenance of a successful seal between the stent-graft and the aneurysm neck. Gradual aortic neck dilatation (AND) may cause a loss of this seal, with subsequent endoleak, migration, and need for secondary intervention.
Diameter changes of the proximal neck after EVAR have been investigated in several studies, leading to diverging results. Diehm et al 3 reviewed the EUROSTAR registry and reported 24.9% of patients at 2 years and 35.1% at 4 years having a >15% increase in proximal neck diameter. Smaller retrospective studies, however, have demonstrated the absence of AND.4,5 The clinical significance of aortic neck expansion has also been debatable. The correlation of AND with migration and endoleak type I has been reported, although some studies did not show any relation of AND to unfavorable clinical outcome.6–8
In 2008, Diehm et al 9 published a review of the English literature on infrarenal AND after EVAR including 16 studies until 2007. Although a systematic methodology was not followed, the authors concluded that AND may raise serious concerns about long-term durability of stent-graft fixation in the proximal aortic area. They also reported a significant heterogeneity in measurement methods and definition of AND among studies, which may compromise comparability of the results.
The objective of the present article was to provide an updated, contemporary systematic literature review and summarize current evidence on AND after EVAR.
Methods
Eligibility Criteria
The objectives and methodology of the systematic review and analysis and the inclusion criteria for study enrollment were prespecified. Standard Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 10 were followed and documented in advance in a formal protocol. Studies considered for inclusion and full-text review fulfilled the following criteria: (1) reported AND after EVAR, (2) included at least 5 patients, and (3) provided data on AND quantification. Two reviewers (G.K. and A.K.) evaluated the eligibility of studies for inclusion in this review independently in an unblinded standardized manner. Disagreements between reviewers were arbitrated by discussion.
Search Strategy
An electronic search of the English-language literature was conducted from 1991 to September 2015 using MEDLINE and EMBASE databases to find studies relevant to AND after EVAR for AAA. Search terms included “aortic neck dilatation” or “proximal seal zone” or “neck expansion” and “EVAR” and “abdominal aneurysm.” Related articles suggested by the PubMed search engine and reviews on this subject were searched for additional relevant articles. Further articles were also identified via examination of the references cited in the initially identified reports. The following data were extracted from each study: publication year, country of origin, number of patients, age, gender, levels of aortic neck measurement, definition of AND, type of stent-graft, mean follow-up, and clinical impact of AND.
Quality Assessment
The quality of observational studies was assessed using the Newcastle-Ottawa Quality Assessment Scale (NOS) for case control studies or cohort studies (as applicable). 11 This tool evaluates 3 main methodological elements of cohort studies: selection methods (representativeness of the exposed cohort, selection of the nonexposed cohort, ascertainment of exposure, and demonstration that the outcome of interest was not present at the start of the study); comparability of cohorts on the basis of the design or analysis; and assessment of outcome (ascertainment of outcome, adequacy of follow-up). The scale uses a star system, with a maximum of 9 stars; studies achieving ≥6 stars were considered to be of higher quality.
Data Synthesis and Analysis
Means of outcome parameters were weighted and data were pooled after significant outcome heterogeneity was excluded. A meta-analysis was performed on the incidence of AND. The pooled proportion was calculated as the back transformation of the weighted mean of the transformed proportions using the random effects model proposed by DerSimonian and Laird. 12 Combined clinical events (endoleak type I, migration, reintervention) in patients with vs those without AND were calculated and reported as the odds ratio (OR) and 95% confidence interval (CI) to reflect the uncertainty of the point estimate of effects.
A significant clinical and methodological diversity of the selected studies was anticipated, so a random-effects model was used, and forest plots were created to visually assess interstudy heterogeneity. Furthermore, heterogeneity was assessed using the Cochran Q test (chi-square) and by measuring the inconsistency (I2). A funnel plot was constructed to visually assess publication bias.
The meta-analyses were performed using the Comprehensive Meta-Analysis software (version 2.0; Biostat, Englewood, NJ, USA) and Review Manager (version 5.3; Cochrane Information Management System; available at: http://ims.cochrane.org/revman). Pooled data analysis was performed using SPSS software (version 20; IBM Corp, Somers, NY, USA).
Results
The initial search identified 218 articles potentially suitable for inclusion in the review. After excluding articles whose titles had no relevance to the topic or subsequent publications on AND from the same institution, the full texts of 25 articles were retrieved and assessed for eligibility. The manual search of the reference list of the selected articles added another 2 citations; one was excluded because it did not provide detailed data for the measurement method. The final analysis included 26 articles3–8,13–32 published between 1998 and 2015 that included 9721 patients (median age 71.8 years; 9439 men). The study cohorts ranged from 27 to 6383 patients. Twelve of the 26 studies achieved a NOS score ≥6 (Table 1).
Summary of Studies Reporting Aortic Neck Dilatation After Endovascular Aneurysm Repair.
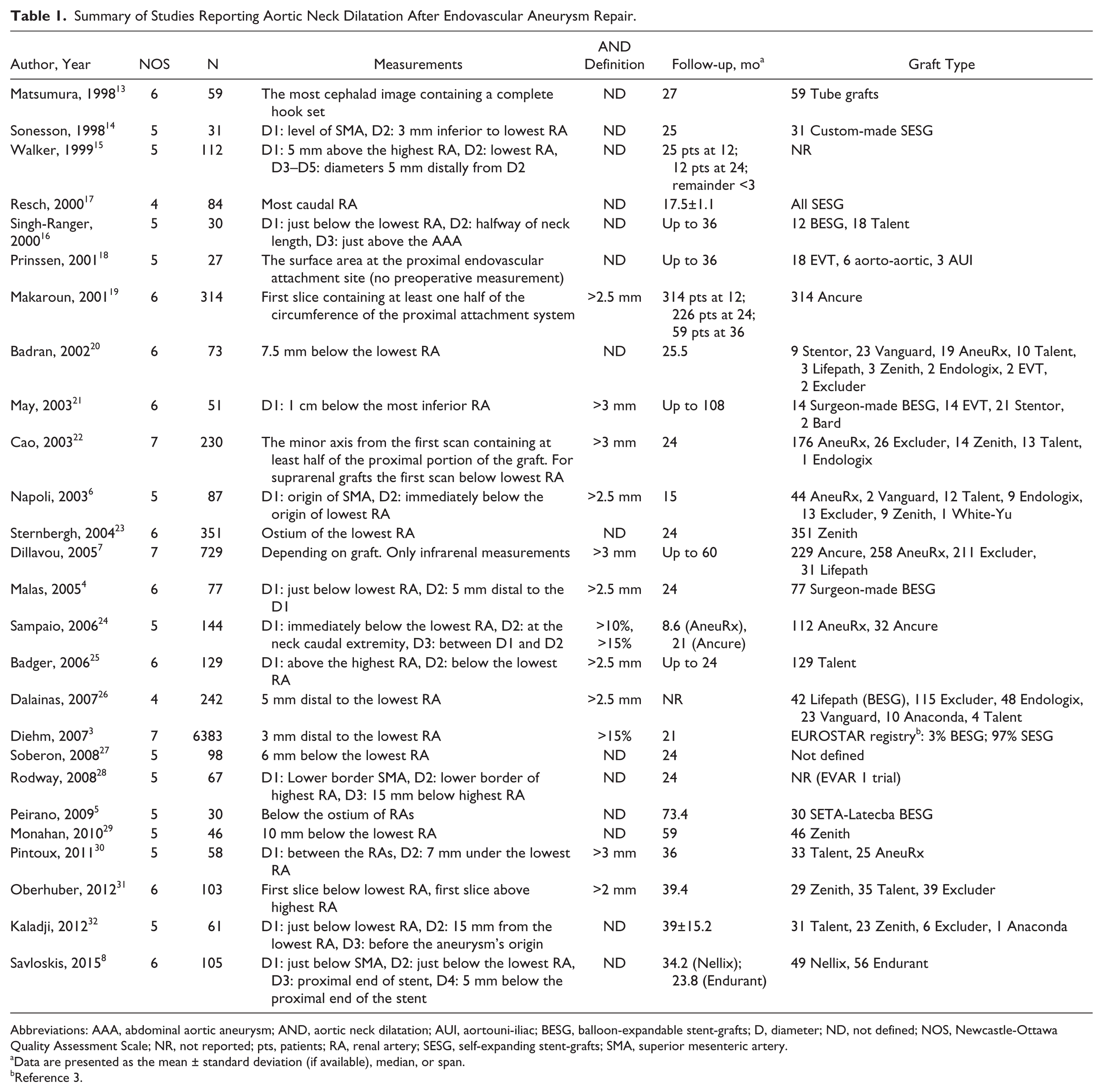
Abbreviations: AAA, abdominal aortic aneurysm; AND, aortic neck dilatation; AUI, aortouni-iliac; BESG, balloon-expandable stent-grafts; D, diameter; ND, not defined; NOS, Newcastle-Ottawa Quality Assessment Scale; NR, not reported; pts, patients; RA, renal artery; SESG, self-expanding stent-grafts; SMA, superior mesenteric artery.
Data are presented as the mean ± standard deviation (if available), median, or span.
Reference 3.
Methods of Measurement
The measurement protocol varied among studies. Infrarenal aortic diameters were measured at 1 level in 18 studies,3,5–7,13,14,17–23,25–27,29,31 at 2 levels in 4 studies,4,8,28,30 at 3 levels in 3 studies,15,16,24 while only 1 study 15 measured 4 different aortic levels. In 5 studies7,13,18,19,22 the level of measurement was defined according to the proximal stent-graft’s attachment site, leading to unreliable follow-up calculations, especially in patients with device migration. Differences were also noted in the definition of the infrarenal aortic neck. Some studies measured directly below the lowermost renal artery,4–6,8,15,23–25,28,31,32 while others were 3 mm,3,14 5 mm,4,8,15,26 6 mm, 27 7 mm, 30 7.5 mm, 20 10 mm,21,29 and 15 mm28,32 distal to the lowermost renal artery. Other measurement methods included halfway between the lowermost renal artery and the beginning of the aneurysm.16,24 In 17 studies5–8,13,16,18,19,21–23,25,26,29–32 follow-up images were compared with the first postoperative set of computed tomography (CT) images, while in 9 studies3,4,14,15,17,20,24,27,28 the comparison was made with the preoperative CT examination. Seven studies3–5,21,22,30,32 used a Kaplan-Meier analysis to calculate freedom from neck enlargement.
Suprarenal Segment
The suprarenal part of the aorta was investigated in 7 studies.6,8,14,15,25,28,31 Four studies6,8,14,28 measured the level of the SMA and the other 3 studies15,25,31 the region just above the highest renal artery. A significant increase in the diameter of the suprarenal region was found in 2 studies (154 patients). Rodway et al 28 reported a mean annual increase of 0.33 cm2, while Napoli et al 6 found a 13.8% yearly increase in cases with suprarenal AND (defined as a >2.5-mm increase). No significant changes in the suprarenal part of the aorta were reported in 4 studies8,14,15,31 (351 patients), while no adequate data were available in 1 study (Table 2). 25
Summary of the Main Results and the Clinical Impact of All Studies.
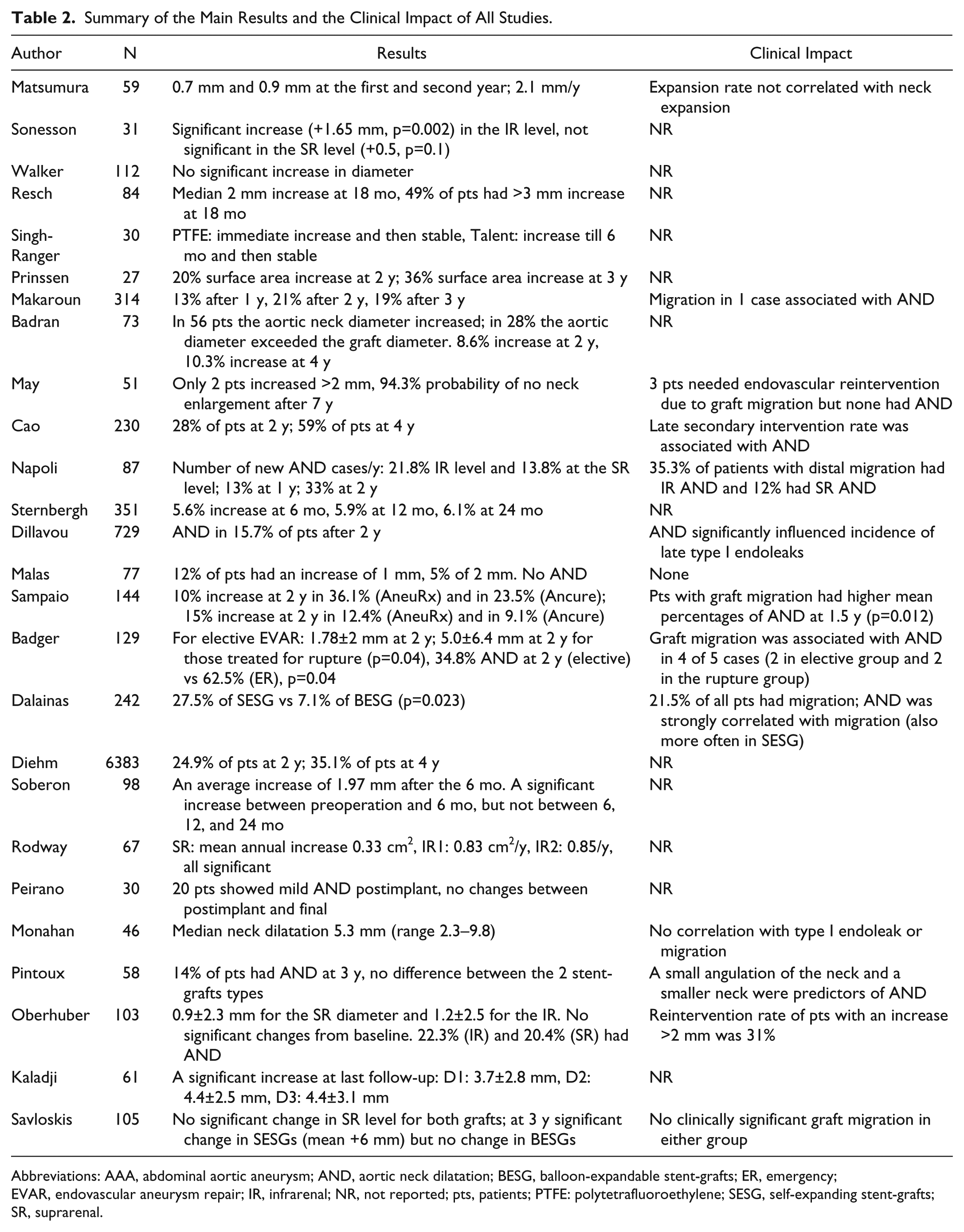
Abbreviations: AAA, abdominal aortic aneurysm; AND, aortic neck dilatation; BESG, balloon-expandable stent-grafts; ER, emergency; EVAR, endovascular aneurysm repair; IR, infrarenal; NR, not reported; pts, patients; PTFE: polytetrafluoroethylene; SESG, self-expanding stent-grafts; SR, suprarenal.
Definition of AND
Neck dilatation was clearly defined in 11 studies.3,4,6,7,19,21,22,25,26,30,31 Five studies4,6,19,25,26 (848 patients) defined AND as an increase in diameter >2.5 mm and reported a cumulative rate of 23.7% at 2 years of follow-up. Four studies7,21,22,30 (1078 patients) defined AND as an increase >3 mm and reported a cumulative rate of 14.4% at 2 years. In 1 study 31 AND was defined as a >2-mm increase and was reported in 22.3% of the patients at the infrarenal level and 20.4% of the patients at the suprarenal level during a median follow-up of 39.4 months. In the largest registry (6382 patients) 3 AND was defined as an increase in diameter >15% and was found in 24.9% of patients at 2 years and 35.1% of patients at 4 years.
Quantification and Clinical Impact of AND
Twelve studies3,4,6,7,19,21,22,24,25,26,30,31 (8550 patients) provided detailed data for the incidence of AND (Figure 1). Over a follow-up ranging from 15 months to 9 years, AND was evident in 24.6% of the patients (95% CI 18.6% to 31.8%).
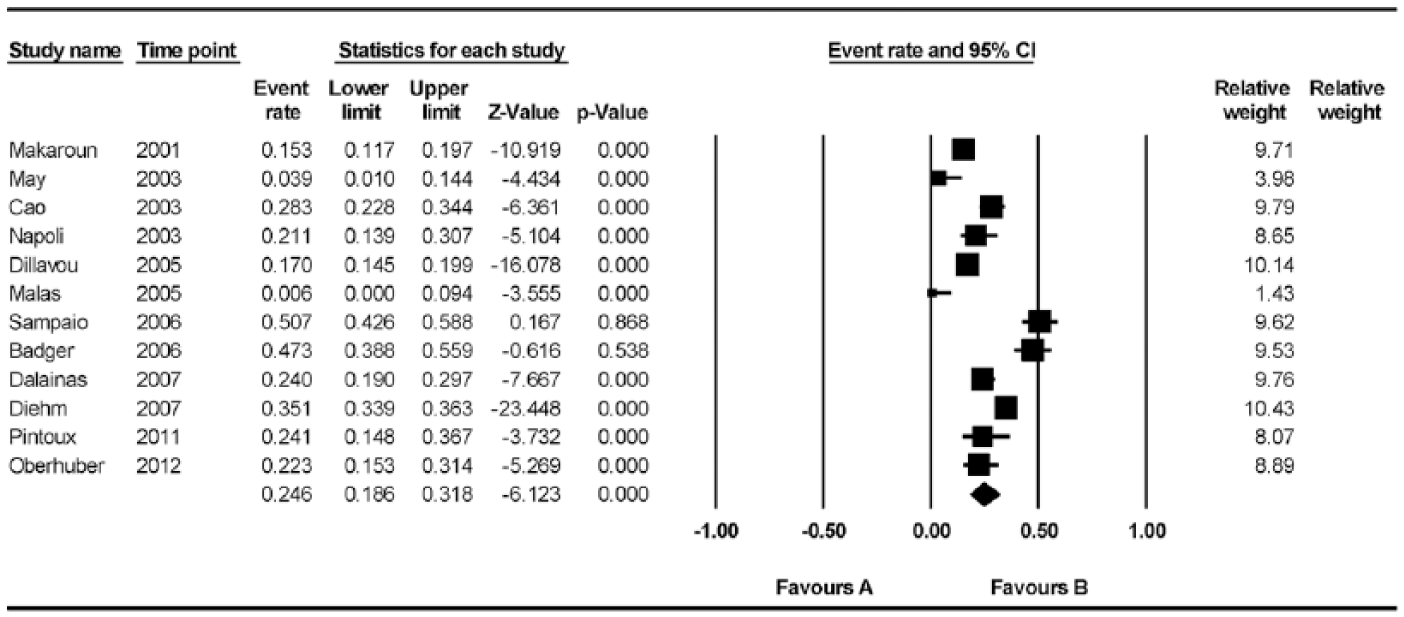
Pooled incidence of aortic neck dilatation. CI, confidence interval.
Seven studies6,7,19,21,22,26,31 (1759 patients) provided adequate data on clinical outcome for groups with and without AND. The incidence of combined clinical events (endoleak type I, migration, reintervention during follow-up) was 26% (88/339) in the AND group compared with 2% (29/1420) in the group without AND (OR 28.7, 95% CI 5.43 to 151.67, p<0.001; Figure 2). High heterogeneity among the studies was indicated (I2=82%), and no asymmetry in the funnel plot was found to indicate significant publication bias.
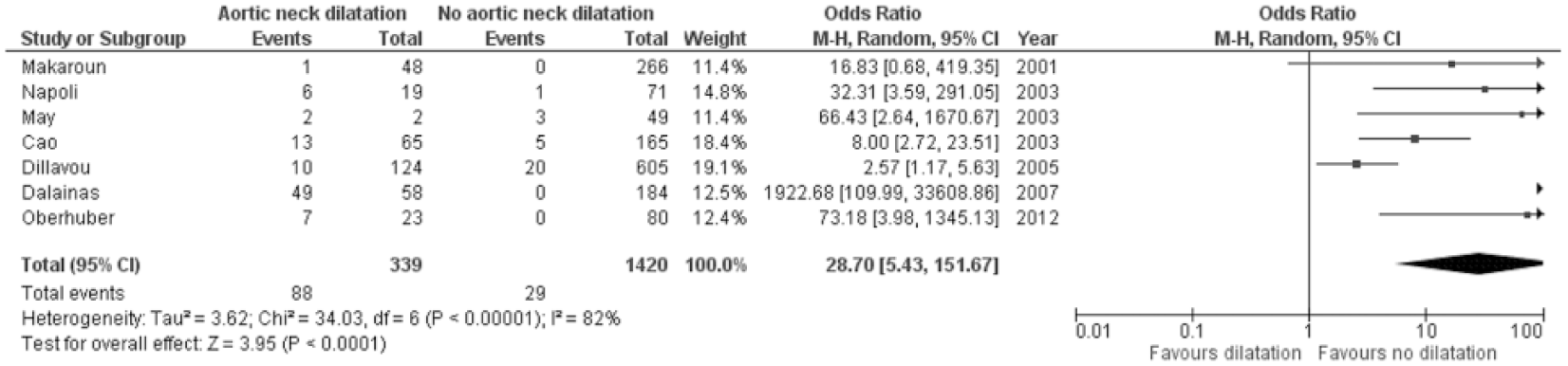
Differences in clinical outcome during follow-up between patients with and without aortic neck dilatation. CI, confidence interval; M-H, Mantel-Haenszel.
Predisposing Factors
Predictive factors that may affect AND were investigated in 11 studies.4,7,13,18–20,22,23,25,29,31 Four studies7,12,23,25 did not find any factor that may predispose to AND. The extent of AND was found to correlate with the percentage of graft oversizing in 3 small retrospective studies.18,20,29 In contrast, Sternbergh et al 23 found no correlation between AND and oversizing in a cohort of 351 Zenith endografts with a mean follow-up of 2 years. In an old study of 314 first-generation stent-grafts, 19 small proximal necks <19 mm had an 80% likelihood of dilating in 2 years; stent-graft oversizing was not an independent predictor of neck dilatation. These findings were partially confirmed in a later study 7 of 729 patients with various endografts, which found that a small neck size (<25 mm) was predictive of AND. Unfortunately, in the latter study, oversizing rates were not investigated.
Discussion
Durable EVAR relies on the maintenance of a persistent seal between the proximal edge of the stent-graft and the nondilated aortic wall. Despite the various definitions, AND was evident in nearly 25% of EVAR patients during follow-up. The causes of AND after EVAR have not been adequately studied. It is unclear whether it is a part of the continuing aneurysm disease process or the result of the stent-graft’s radial force. The fact that neck dilatation seems to occur after open repair supports the theory of vessel degeneration. Oberhuber et al 31 demonstrated similar increases in aneurysm neck diameters between AAA groups treated by EVAR or open repair, suggesting that AND may be caused by a natural progression of the disease. 1 Furthermore, the effect of endograft oversizing on AND has also been investigated, leading to diverging results. A few small studies showed a positive correlation between the percentage of oversizing and the degree of AND,18,20,29 though larger studies failed to prove this relation. 23
The suprarenal part of the aorta does not seem to dilate significantly over time as shown from 5 studies8,14,15,25,31 of the 7 studies investigating this region. This finding might be explained by the differences in stiffness and thickness between the suprarenal and infrarenal segments of the aorta, which may lead to the observed difference in aneurysm disease prevalence between those regions.33,34 The evolution of the diameter of the suprarenal aorta is specifically relevant to endografts with suprarenal fixation and fenestrated EVAR. The long-term influence of stent-graft fixation has been evaluated in only 1 study 30 of 58 patients and no correlation was found. In deployment of an endograft with suprarenal struts, fixation may be better but the sealing remains unchanged. Furthermore, AND following fenestrated EVAR has not been investigated adequately. Fenestrated EVAR has shown low rates of migration and type I endoleak, probably reflecting the absence of significant dilatation of the suprarenal part of the aorta. 35
The clinical impact of AND has been controversial. By pooling results of 7 studies,6,7,19,21,22,26,31 a higher event rate in patients with AND during follow-up was evident. This finding may have implications on long-term EVAR surveillance. Currently, EVAR surveillance relies on ultrasound imaging to identify changes in the aneurysm sac and the presence of endoleak. Our group has previously shown that a follow-up protocol comprising duplex ultrasonography and plain abdominal radiography gives a wide range of information covering EVAR-related risks with less radiation exposure and lower risk of renal dysfunction, 36 although aortic neck morphology is difficult to quantify with ultrasound. AND has not been directly associated to AAA rupture, though a negative clinical impact has been demonstrated. It would be interesting to identify patients at risk for AND in whom CT surveillance would be indicated.
Balloon-expandable stent-grafts have not been associated with AND.4,5 Comparative studies have also shown a strong correlation of AND with self-expanding but not with balloon-expandable endografts,3,26 which maintain their diameter after deployment and do not exert continuing radial force like self-expanding stents. Furthermore, they need less oversizing (<5%). Balloon-expandable stent-grafts are not commonly used in current EVAR practice. Recently, a novel device has been introduced using balloon-expandable stent-grafts along with polymer-filled endobags to achieve fixation and seal of the aneurysm. 37 Savloskis et al 8 compared this new stent-graft with a latest generation self-expanding endograft and found that patients treated with the balloon-expandable device showed no significant change in infrarenal aortic neck diameter whereas patients treated with the self-expanding device had a progressive 25% increase in neck diameter during a 3-year period. However, despite these interestingly promising results, current evidence on the value of balloon-expandable stent-grafts remains low, and larger, prospective, comparative studies are needed.
Patients at risk for significant AND during follow-up have not been well defined yet. There is generally a slight increase in diameter after self-expanding stent-grafts but thereafter some necks continue to grow and others do not. As seen in the present review, data on predisposing factors for AND are inadequate and cannot lead to any solid conclusion. Some necks seem to dilate more, but it is never uniform, and no long-term data exist despite the wide availability of EVAR stent-grafts for nearly 15 years now. By defining patients who are at higher risk for AND, we may also be able to change the initial therapeutic strategy and proceed with a more durable solution for those patients, such as a fenestrated stent-graft or even open repair.
Limitations
The results of our review and analysis should be interpreted in the context of its limitations. Most of the studies were retrospective, with some reporting a small number of patients. Nearly half of the studies were of poor methodological quality, which may bias the results. The vast majority of the endografts were old-generation models from the early EVAR years, and not enough data about the association of AND with specific devices were available.
Anatomical characteristics, such as the initial neck length, diameter, and the quality of the neck, have not been reported. The wide range of the year of publication and the variability in follow-up duration should also be acknowledged. Only 8 studies had a mean follow-up period >3 years, so data on the long-term clinical impact of AND are inadequate.
According to the Society for Vascular Surgery/American Association for Vascular Surgery (SVS/AAVS) reporting standards, 38 aortic neck changes should be referenced to those measurements taken from the first set of postoperative images, while a Kaplan-Meier analysis should be used to calculate freedom from neck enlargement. These requirements were clearly met by 4 studies only.21,22,26,30 Nine (34.6%) studies3,4,14,15,17,20,24,27,28 compared follow-up with preoperative data, thus not considering the effect of the stent-graft oversizing after EVAR.
Given the variability of measurement methods and the definition of AND, it is important to establish commonly accepted measuring standards. In our opinion, proximal aortic neck should be measured at 6 levels, 3 suprarenal and 3 infrarenal. Suprarenal measurements should include the levels just above the highest renal artery, just below the superior mesenteric artery, and just below the celiac trunk. Infrarenal measurements should include the levels just below the lowest renal artery and 2 points at 7 mm distally and at the end of the neck. With these measurements, the clinically relevant changes of the proximal aortic neck can be quantified. It is important that all measurements are compared to the first set of postoperative images, as recommended by the SVS/ISCVS reporting standards. 38 The definition of AND should be directly linked to clinical outcome, as estimation of absolute values of neck dilatation has not led to any definite clinical conclusion so far. Therefore, clinically significant AND should be defined as an increase in the proximal aortic diameter leading to loss of adequate seal and subsequent endoleak or migration.
Conclusion
AND seems to affect a considerable proportion of EVAR patients and was related to worse clinical outcomes, as indicated by increased rates of type I endoleak, migration, and reinterventions. Future studies should focus on a better understanding of the pathophysiology, predictors, and risk factors of AND. This could help to determine the group of patients that may warrant a different EVAR strategy and/or a closer post-EVAR surveillance strategy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.