
Abstract
Introduction
Minimally invasive endovenous ablation techniques have become an established treatment of great saphenous vein (GSV) insufficiency, which is a common medical condition in the Western world. Both endovenous laser ablation (EVLT) and radiofrequency ablation (RFA) have been proven to be effective and superior to surgery with regard to postprocedural pain, quality of life (QoL), and time to recovery.1-4 Thermal ablative modalities, however, carry the risk of damaging the surrounding tissues of the vein and thus necessitate tumescent anesthesia, which requires multiple punctures along the treated vein segment. This may prolong the procedure and adds to patient discomfort during treatment. Despite the use of tumescent anesthesia, there remained a subset of patients who have postoperative pain, which can last for several weeks.5,6 To overcome these drawbacks, new endovenous techniques were developed, such as ultrasound-guided foam sclerotherapy, 7 the VenaSeal Sapheon Closure System,8,9 and mechanochemical endovenous ablation (MOCA). MOCA combines mechanical damage to the endothelium caused by a rotating wire with simultaneous catheter-guided infusion of a liquid sclerosant that irreversibly damages the cellular membranes of the endothelium, causing fibrosis of the vein. The exact mechanism is still not known; however, recent experimental research showed that various sclerosants induced apoptosis in the vein wall rather than having an effect restricted to the endothelium. Incomplete loss of endothelial cells and penetration of the sclerosant effect into the media suggest that medial damage is crucial to the success of sclerotherapy and may explain why it is less effective in larger veins. 10
With more than 40,000 MOCA procedures performed with the ClariVein device (Vascular Insights, Quincy, MA, USA), the complications have been minimal; deep vein thrombosis occurs in <0.5% of cases, and no nerve or skin injury has been reported.11-16 MOCA proved to be as effective as RFA in the short term and was associated with lower postprocedural pain and faster recovery compared with RFA, most likely owing to the avoidance of heat-related complications.17-19 Short-term results include immediate closure rates >96%13,15 and early closure rates ranging from 97% at 9 months to 88% at 1 year.13-15,19 The aim of this study was to evaluate the 3-year midterm results of MOCA in patients with GSV insufficiency.
Methods
Study Design
Between December 2010 and December 2011, 85 consecutive patients (median age 51.4 years; 56 women) referred for varicose vein treatment in 104 limbs owing to symptomatic primary GSV insufficiency were enrolled in a prospective registry approved by the Medical Ethics committee of Nijmegen (CMO 2011/091) and the local institutional review board of each hospital. Patient characteristics are shown in Table 1. The design of the study and early results were published previously 13 and can be found on ClinicalTrials.gov (identifier NCT01459263). Briefly, patients were included after signing informed consent. Inclusion criteria included age >18 years, C2 to C5 varicose veins, GSV diameter of 3 to 12 mm, and primary GSV insufficiency determined by duplex ultrasound examination. It was decided not to include C6 disease as this would induce severe bias related to QoL scores because of the presence of an ulcer. Other exclusion criteria were comorbid small saphenous vein (SSV), anterior accessory great saphenous vein (AAGSV), or posterior accessory saphenous vein incompetence; pregnancy and lactation; use of anticoagulants; coagulation disorders; previous surgical treatment of the target varicose vein; previous deep venous thrombosis; severe renal or liver insufficiency; and allergy to polidocanol.
Baseline Patient Characteristics (per Treated Limb) and Details for the 102 Successful Procedures. a
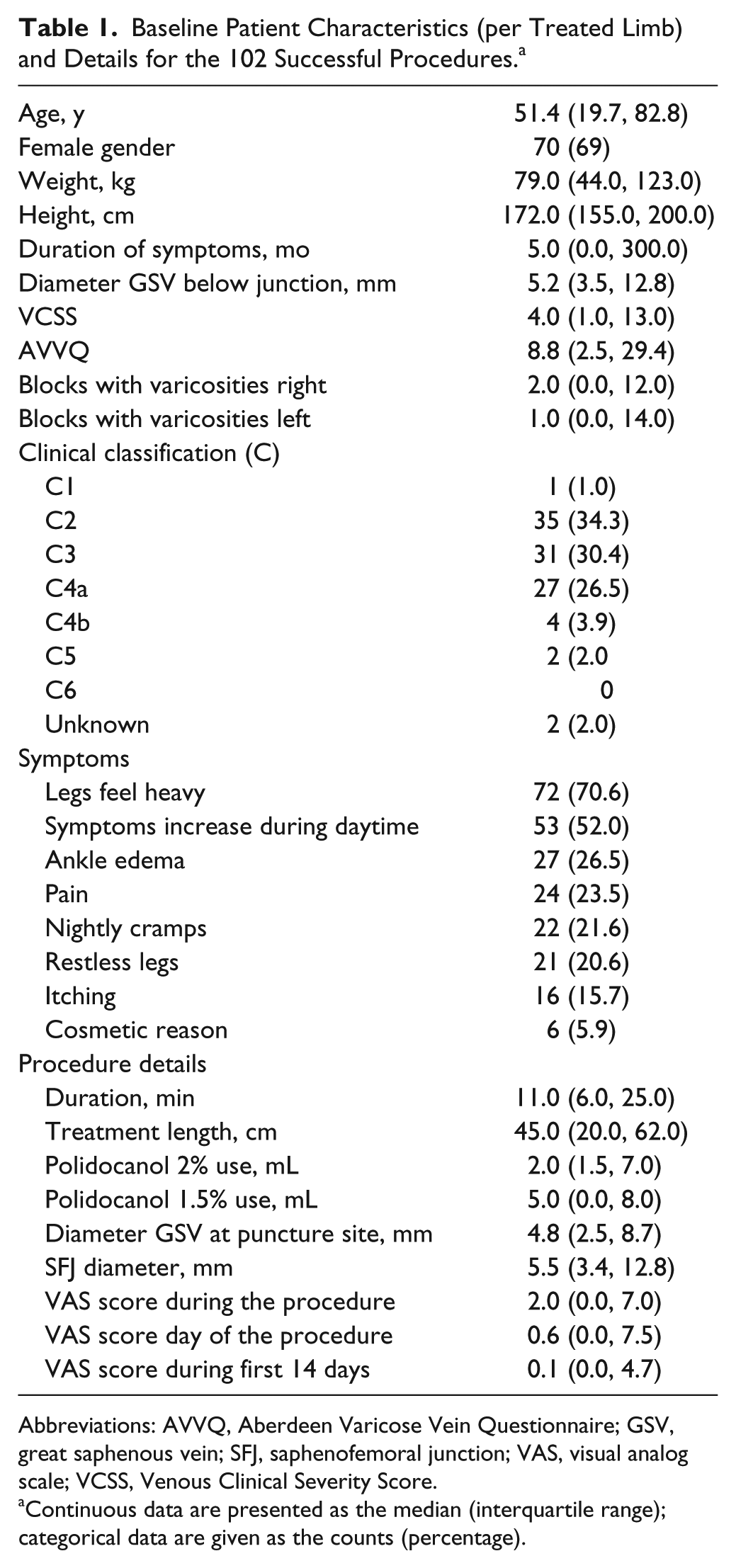
Abbreviations: AVVQ, Aberdeen Varicose Vein Questionnaire; GSV, great saphenous vein; SFJ, saphenofemoral junction; VAS, visual analog scale; VCSS, Venous Clinical Severity Score.
Continuous data are presented as the median (interquartile range); categorical data are given as the counts (percentage).
Baseline Assessment
Primary GSV insufficiency was diagnosed in all patients with duplex ultrasound examination performed by certified vascular practitioners. Reflux was defined as retrograde flow ≥0.5 seconds after calf compression measured in a standing position. Preprocedural physical examination was performed by a vascular surgeon. The CEAP (clinical, etiologic, anatomic, and pathophysiologic) classification 20 and Venous Clinical Severity Score (VCSS) 21 were determined.
In order to observe the general and disease-specific QoL, patients were asked to complete the Dutch versions of the RAND Short Form 36-Item Health Survey (RAND-SF36) 22 and the Aberdeen Varicose Vein Questionnaire (AVVQ). 23 The RAND-SF36 covers health status in multiple dimensions: physical functioning, social functioning, role limitations due to physical health problems and emotional problems, general mental health, vitality, bodily pain, and general health perception. It also includes a single item that provides an indication of perceived changes in health. A high score indicates good health status.
Treatment
MOCA was performed on an outpatient basis with the ClariVein device by a specialized team consisting of a vascular surgeon and a certified vascular practitioner. Bilateral treatments were scheduled at least 6 weeks apart. Detailed descriptions of the ClariVein device and treatment have been published. 16 In short, an introducer wire and sheath were inserted into the GSV under ultrasound guidance, then the ClariVein catheter was inserted and the tip of the stainless steel wire was placed below the saphenofemoral junction (SFJ). By connecting the motorized handle unit, the distal end of the dispersion wire was unsheathed to expose the dispersion tip, which was positioned ~2 cm distal to the SFJ. The wire was activated for 2 to 3 seconds to induce vasospasm, then the activated catheter was slowly withdrawn at a speed of ~7 s/cm while polidocanol (Aethoxysklerol; Kreussler Pharma, Wiesbaden, Germany) was continuously injected. The proximal 10 cm was treated with 2% polidocanol (mean 2 mL) and the remaining vein with 1.5% polidocanol (mean 5 mL). During the procedure no sedation or antibiotics were given. Duplex was performed to confirm occlusion of the treated vein. No additional phlebectomies or sclerotherapy were performed during or up to 4 weeks after the initial procedure with the ClariVein device.
After the procedure, a compression thigh stocking (30–40 mm Hg) was worn continuously for 24 hours and during daytime for the following 2 weeks. Patients were asked to scale pain during the procedure using the 100-mm visual analog scale (VAS) from 0 mm (no pain) to 100 mm (worst imaginable pain). Patients were allowed to perform their daily activities immediately. No standard analgesics were prescribed.
Follow-up
Patients were asked to keep a log of the level of experienced pain on the VAS during the first 14 days following treatment and to note the day of return to normal activities and work, if applicable, and the amount of analgesics used. Postprocedural complications were recorded. After 4 weeks and annually to 3 years, patients were seen at the outpatient clinic to document anatomic and clinical success. Duplex examination, VCSS, RAND-SF36, and AVVQ were completed at all above mentioned time points.
Outcomes
The primary outcome measures were clinical success (defined as an improvement in VCSS ≥1) and anatomic success (defined as occlusion of the treated vein). Failure was the presence of flow and reflux in a recanalized segment with a length ≥10 cm. Complete recanalization referred to blood flow in the entire treated segment of the vein, while partial recanalization indicated an open segment >10 cm. Secondary outcome measures included postprocedural pain (VAS), complications, general and disease-specific QoL (RAND-SF36 and AVVQ), and time to return to daily activities and work.
Statistical Analysis
Continuous variables are presented in means ± standard deviation, if distributed normally, or as median with interquartile range (IQR; 25th, 75th percentiles), if appropriate, and as frequencies and percentages in case of categorical variables. A repeated-measures analysis of variance was used to evaluate postoperative pain and post hoc Bonferroni correction to evaluate differences in the AVVQ, RAND-SF36, and VCSS scores before and at different follow-up visits. All tests were 2-sided; differences achieving p<0.05 were statistically significant. Statistical analyses were performed with SPSS software (version 21.0; IBM Corporation, Somers, NY, USA).
Results
Technical success (99%) was achieved in all but 1 male patient in whom technical problems with the device arose; leakage of sclerosant through the catheter device prompted conversion to RFA (the primary method of choice in our center) and both legs were treated in 1 session. The median procedure time in the remaining 102 procedures/limbs was 11 minutes (IQR 6, 25), during which a median 45-cm vein segment (IQR 20, 62) was treated. The periprocedural pain score (VAS) was 2 (IQR 0, 7) and overall pain reported on the day of the procedure was 0.6 (IQR 0, 7.5). Information about analgesic use (mostly paracetamol or ibuprofen) was available in 75 patients; the median number of days that analgesics were used was 0 (IQR 0.0, 1.0). Procedural characteristics are summarized in Table 1.
The mean VAS score in the first 2 weeks was 0.1 (IQR 0, 4.7). Daily activities were resumed after a median of 1 day (IQR 0, 22) and work after 1 day (IQR 0, 15) post procedure. There were no major complications. Hyperpigmentation occurred in 5%, hematomas/bruising in 11.2%, prolonged pain of >1 week in 6.1%, induration in 14.3%, and superficial thrombophlebitis in 2% of the 102 treated legs.
Follow-up
After a median follow-up of 36 months (IQR 12.5, 46.3), 14 patients (16 limbs) were lost to follow-up. Reasons for loss were due to patient request (n=10), conversion to other treatment modality for persisting complaints (n=1), no further contact with patient (n=2), and 1 death (2 limbs) as a result of an intracranial hemorrhage at 13 months. This patient did not use anticoagulants at the time of varicose vein treatment but started acenocoumarol 11 months later because of de novo atrial fibrillation; he died 2 months later.
Additional Treatments
During follow-up, 14 additional treatments and 4 reinterventions for varicose veins were performed. The additional treatments, performed on other varicose vein segments than those treated with MOCA, consisted of additional sclerotherapy (n=4), phlebectomy (n=1), foam therapy (n=3), VNUS (n=2), and MOCA (n=4). Reinterventions for recanalized GSVs were performed by RFA after 6 months (n=1), 28 months (n=2), and 29 months (n=1).
Anatomic Success
At 4 weeks, partial recanalization was seen in 3 proximal GSVs, which all progressed to complete failure after 36 months. No reinterventions were performed in these patients during follow-up. At 6 months, 5 more recanalizations had occurred (2 complete and 3 partial). The 3 partial recanalizations included a patient with proximal recanalization remaining as such at 2 years, a second patient with proximal and mid GSV recanalization remaining as such at 2 years, and a third patient with proximal recanalization at 6 months that progressed to proximal and distal recanalization at 2 years. In the latter, a high ligation of the SFJ was performed.
At 1-year follow-up, 3 new recanalizations were encountered; all were partial (proximal and distal remaining the same at 2 years, proximal remaining the same at 2 years, and proximal progressing to proximal and mid GSV at 2 years, respectively). No reinterventions were performed in these patients. At 36 months, 4 more vein segments had recanalized [3 complete and 1 partial (proximal and distal)]. No reinterventions were performed in these patients. In total, recanalization was seen in 15 (14.7%) of 102 treated vein segments; 1 reintervention was performed in these 15 recanalizations. Anatomic success after MOCA was 91.8% after 12 months, 89.5% after 24 months, and 86.5% after 36 months of follow-up, as presented in Figure 1.
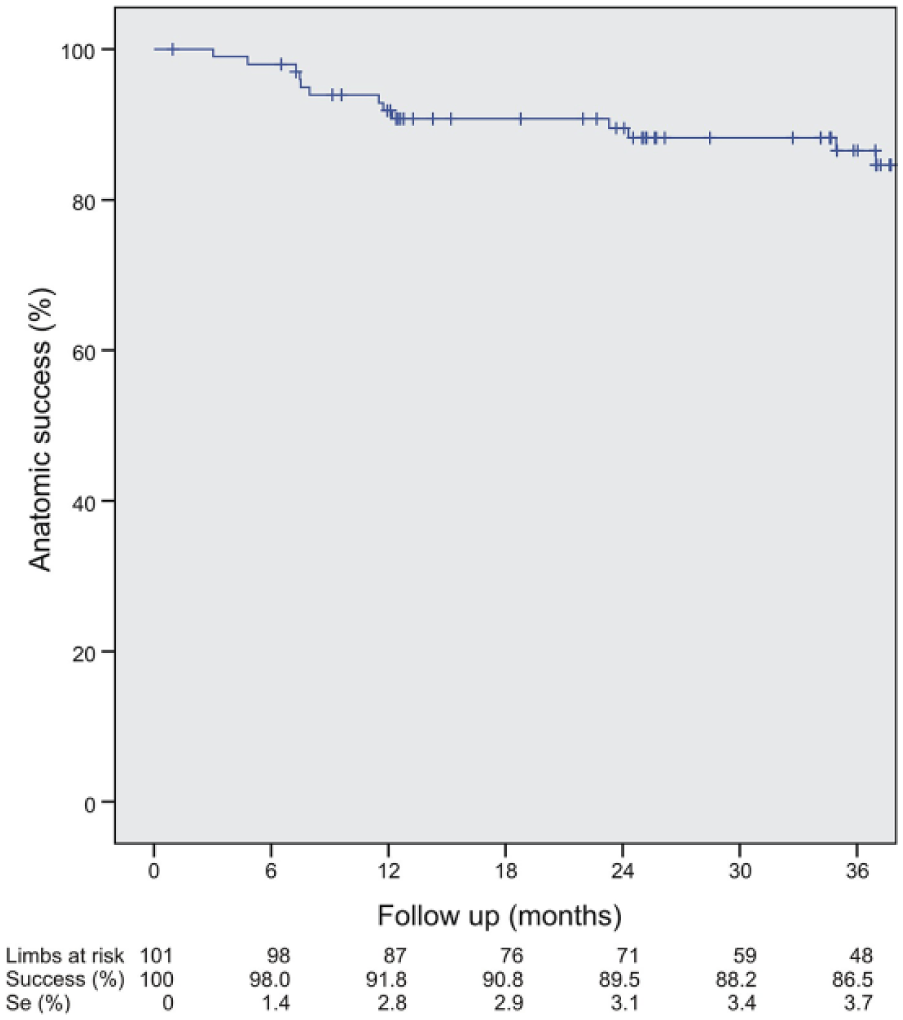
Survival curve for anatomic success during follow-up. Se, standard error.
Clinical Success
Median VCSS scores during follow-up are shown in Table 2. After 36 months, clinical success was achieved in 83.1% of treatments. A significant improvement of VCSS was seen at all time intervals compared to the median preprocedural VCSS of 4.0 (IQR 1, 13). After 12 months, the VCSS significantly (p=0.003) deteriorated from 1.2±1.4 to 1.8±1.5 at 36 months (Table 3). With regard to the VCSS in the 15 anatomic failures, there was also an improvement compared to baseline at all time intervals, with the lowest value at 6 months and slight deterioration thereafter.
VCSS, AVVQ, Blocks per Treated Leg, and RAND-SF36 Domains During Follow-Up. a
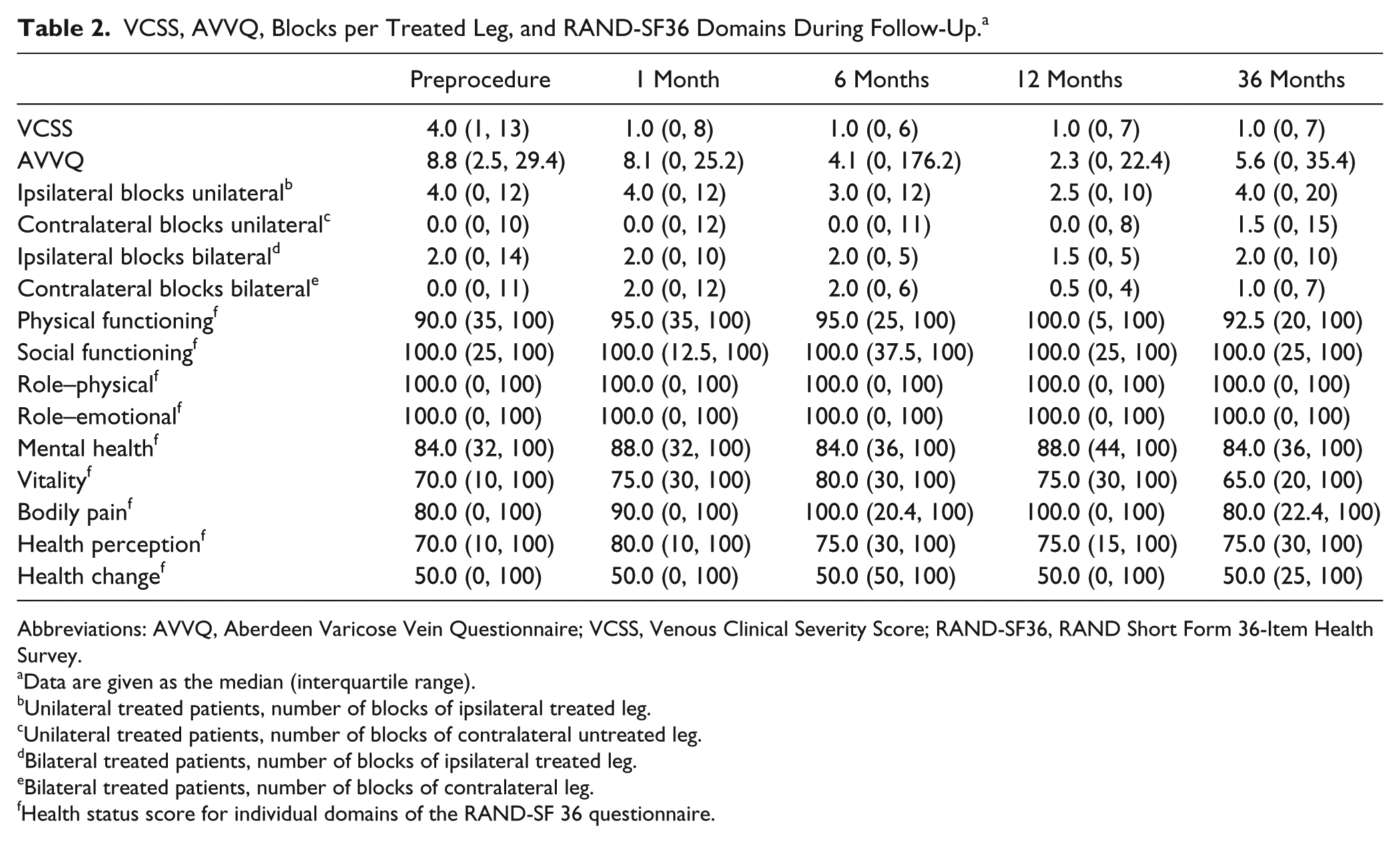
Abbreviations: AVVQ, Aberdeen Varicose Vein Questionnaire; VCSS, Venous Clinical Severity Score; RAND-SF36, RAND Short Form 36-Item Health Survey.
Data are given as the median (interquartile range).
Unilateral treated patients, number of blocks of ipsilateral treated leg.
Unilateral treated patients, number of blocks of contralateral untreated leg.
Bilateral treated patients, number of blocks of ipsilateral treated leg.
Bilateral treated patients, number of blocks of contralateral leg.
Health status score for individual domains of the RAND-SF 36 questionnaire.
Analysis of Variance of VCSS, AVVQ, and Blocks per Treated Leg at Different Time Points in Follow-up.
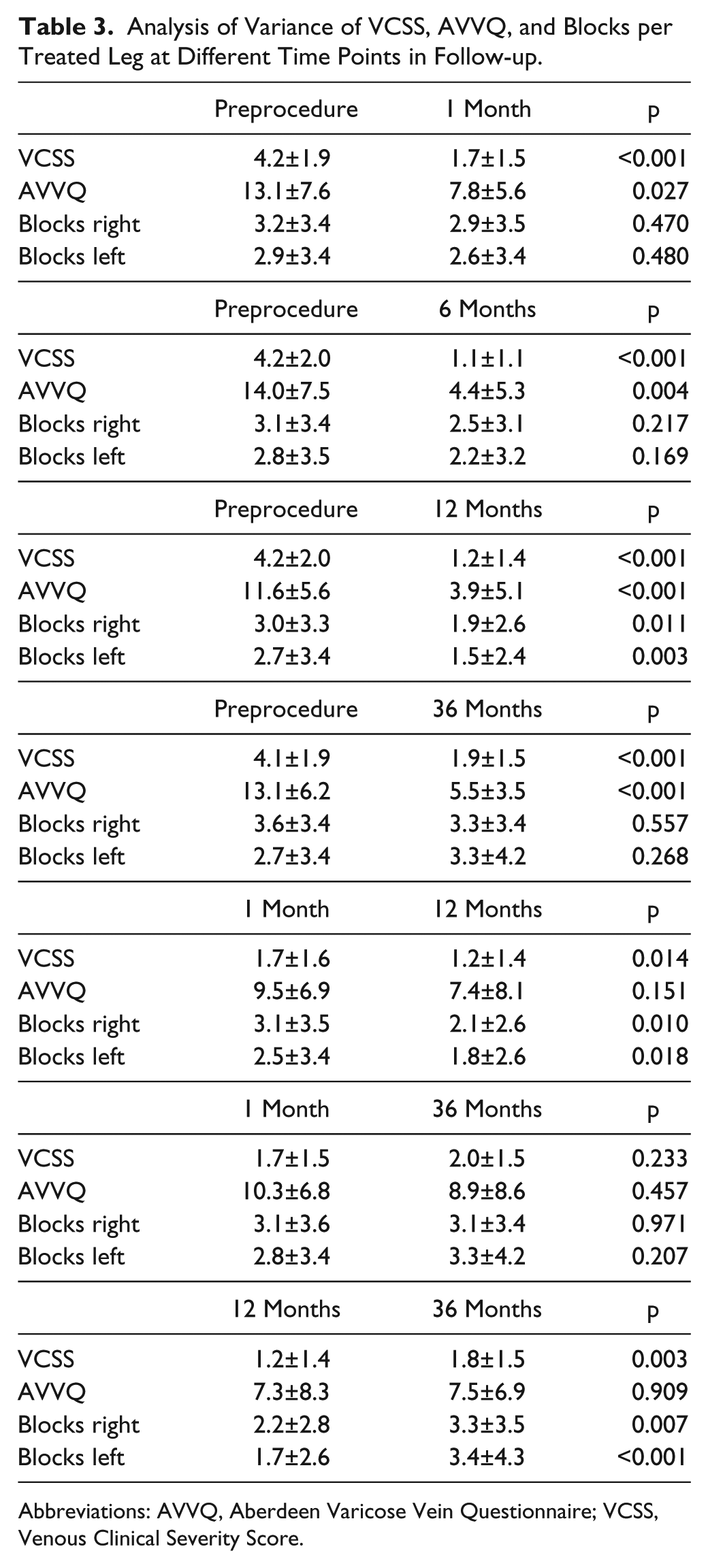
Abbreviations: AVVQ, Aberdeen Varicose Vein Questionnaire; VCSS, Venous Clinical Severity Score.
Patient Health Status
The disease-specific AVVQ score during follow-up is presented in Table 2. Preprocedurally, the median AVVQ score was 8.8 (IQR 2.5, 29.4). At all time intervals, the AVVQ score showed significant improvement compared with baseline (Table 3). The amount of varicose veins drawn on each leg in the AVVQ questionnaire was measured in blocks (Table 1). After 12 months, a significant decrease in the number of blocks was seen for both legs compared to the mean preoperative number of blocks of 3.0±3.3 right (p=0.011) and 2.7±3.4 left (p=0.003) and also compared to 1-month follow-up (p=0.010 right and p=0.018 left; Table 3). However, this improvement in blocks disappeared after 36 months, and the difference compared with baseline was no longer significant at that time point. Compared to 12 months, there was a significant increase in blocks drawn after 36 months for both legs (p=0.007 right and p<0.001 left; Table 3), suggesting an increase in varicose veins, not only in the treated leg. Thus, recurrences appeared to arise between 12 and 36 months, correlating with clinical deterioration.
Assessment of the general health status with the RAND-SF36 questionnaire showed an improvement in almost all domains at 1-year follow-up compared with baseline. However, at 36 months, scores were diminished compared to the other time intervals (Table 2). After 12 months, data on wearing stockings were available for 82 patients; 4 (5%) patients were wearing them (2 most days and the other 2 intermittently). After 36 months in 83 patients, 5 (6%) patients were still using them (2 most days and the others intermittently).
Discussion
This study shows that MOCA is effective in the treatment of GSV insufficiency, not only in early follow-up as published in the literature13-15,19 but also at 36 months, although anatomic and clinical failures do occur. The VAS scores during the procedure and thereafter were low; a quick return to daily activities was achieved with no serious complications, 17 as reported by others.16-19
As regards the patient-reported health status, the disease-specific AVVQ scores showed significant improvement after 36 months, as did all domains of the RAND-SF36, reflecting general health status. However, between 12 and 36 months, a significant deterioration was observed in clinical score (VCSS). This clinical deterioration is also supported by an increase in mean AVVQ score, representing worsening of the disease-specific health status after 1 year, and by the increased number of varicose veins drawn in the AVVQ on each leg after 1 year. Furthermore, a worsening in health status on all domains of the RAND-SF36 was seen at the latest time interval, with significant deterioration in the domains of social functioning and vitality. This worsening, however, does not reflect only the known recurrent nature of varicose veins but might also reflect progression in comorbidities not specifically associated with varicose vein disease.
It was our assumption that using 2% instead of 1.5% sclerosant in the proximal 10 cm of the GSV would reduce the number of proximal recanalizations. Nevertheless, recanalization was seen in 15% of treated vein segments, of which only a third occurred after 1 year and so are unlikely to account for the worsening in observed clinical scores and disease-specific and general QoL after that time. A possible explanation might be the recurrent nature of varicose veins after a mean of 36 months, which is a well-known phenomenon.24,25 A recent study clarified that the majority (77%) of recurrences after endothermal venous ablation occurred in association with perforating veins. New AAGSV and SSV insufficiency were responsible for 40% of those patients who developed recurrent venous disease. 24 The impact of (recurrent) varicose veins on general QoL may account for the diminished RAND-SF36 scores.
Remarkably, even patients with an anatomic failure showed improvement of their clinical scores after 36 months compared to baseline, and only 4 reinterventions for GSV recanalization were performed. Potentially, the polidocanol injected during MOCA may have caused obliteration of side branches that could have contributed to the clinical state. This is supported by the fact that adjuvant treatment of side branches was performed in only 5 patients, which is remarkably low. Still, varicose veins recurred, as reflected by the deterioration in QoL scores.
In the literature no studies with comparable follow-up of MOCA have been published to date. When looking at thermal endovenous ablation techniques (EVLT and RFA) for which long-term results have been published, comparable anatomic success rates of ~80% at 2 to 3 years have been described.26-28
With regard to other endovenous nonthermal techniques to exclude varicose veins, ultrasound guided-foam sclerotherapy was one of the first developed but has not proven as effective as endovenous thermal techniques, with success rates of only 67% to 73% at 1 year.7,29 In addition, there is a rare but well documented risk of stroke. 30 The VenaSeal Sapheon Closure System is another new nonthermal technique that comprises the endovenous delivery of cyanoacrylate tissue adhesive to the vein, causing fibrosis. Short-term results show that cyanoacrylate embolization (CAE) is noninferior to RFA at 3 months after treatment with closure rates of 99% for CAE and 96% for RFA.8,9 Longer term results have to be awaited to compare this technique with MOCA.
Limitations
The results of the present study are affected by the chosen definitions of success. Although the definition used is in accord with previous landmark trials, 4 heterogeneity in the definition among studies is a major problem in comparing results and emphasizes the need for standardization of outcome measures. Furthermore, follow-up was not completed for every patient, and questionnaires were not always complete.
Conclusion
MOCA is effective in the treatment of GSV insufficiency, with an anatomic success of 86% and clinical success of 83% at midterm follow-up of 36 months. The clinical results, however, seem to drop between 1 and 3 years, potentially related to the recurrent nature of varicose veins.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Michel M. P. J. Reijnen and Jean-Paul de Vries have received research grants from Vascular Insights.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.