
Abstract
Keywords
Introduction
Currently, the endovascular-first approach tends to be the preferred method when treating symptomatic femoropopliteal (FP) occlusive disease. Historically, balloon angioplasty was the standard endovascular therapy in the FP segment; however, unacceptably high rates of restenosis, except for treatment of relatively short lesions, have limited its usefulness. 1 Bare metal stents (BMS) improved on these results but were still associated with clinically significant and difficult to treat restenosis patterns. More recently, drug-based technologies using the antiproliferative agent paclitaxel have been developed to reduce restenosis rates and improve clinical durability.2–4 The first drug-coated peripheral device approved for use in the United States was a drug-eluting stent (DES) delivering paclitaxel in a nonpolymer base; the outcomes with this device have shown reduced rates of restenosis and reintervention at 5 years compared to balloon angioplasty and BMS. 2 The second wave of drug-delivery devices were drug-coated balloons (DCBs), which also have demonstrated improved results compared to bare balloon angioplasty.3,4
Although it appears that the use of drug elution has changed the endovascular treatment paradigm in the FP segment, there is still a paucity of real-world data for DES and DCB in complex TASC (TransAtlantic Inter-Society Consensus) C and D lesions. For example, the mean lesion length in the level-1 randomized safety and efficacy trial of the paclitaxel-coated DES for treating FP disease was 5.5 cm, with a stented length of 6.6 cm.1,5 An early registry from Germany supported the use of DES in slightly more complex lesions with a mean length of 10 cm. 6 More recently, a 1-year post-market surveillance study from Japan with a mean lesion length of 14.7 cm also demonstrated the effectiveness of paclitaxel-coated DES. 7
Diffuse FP arterial disease (>20 cm) is a common entity, and treatment of these lesions with DES warrants formal clinical evaluation in an effort to better understand their durability and clinical effectiveness in a real-world setting. Unfortunately, this population is typically underrepresented in the device approval trial cohorts. This study investigated the 1- and 2-year restenosis rates as well as the need for clinically-driven target lesion reintervention (TLR) in patients with diffuse de novo FP atherosclerotic lesions or FP in-stent restenosis (ISR) treated using the Zilver PTX, a self-expanding tubular nitinol stent with a polymer-free paclitaxel coating (3 μg/mm2 dose density). 1
Methods
Study Design and Patient Population
This was a single-center, retrospective analysis to appraise in detail the outcomes after intervention utilizing the Zilver PTX (Cook Medical, Bloomington, IN, USA) in long, complex de novo and ISR lesions in the FP segment. Patients were eligible for Zilver PTX treatment if they were diagnosed with symptomatic (Rutherford category 2–6) occlusive disease in the superficial femoral artery (SFA; ostial disease not excluded) and/or first 2 segments of the popliteal artery. Data collection began with the device release in the United States and continued for 1 year (December 2012 to December 2013). The study was approved by the OhioHealth Institutional Review Board.
Demographic and baseline data were recorded, including age, sex, date of diagnosis, Rutherford class, comorbidities, risk factors, and smoking history. Prespecified patient subsets for comparison included a short lesion (SL) group (≤20 cm) vs a full DES jacket (FDJ) group with lesions >20 cm long. Recorded procedure data included date of DES implantation, location, lesion length, stent diameter, presence of total occlusion, ISR treatment, and stent characteristics. Lesion lengths were measured using a standard fluoroscope measuring tape in centimeters.
In the enrollment period, 89 consecutive patients (mean age 68.7±9.8 years; 86 men) with atherosclerotic FP occlusive disease underwent Zilver PTX placement. Demographics and lesion characteristics are shown in Table 1. A third of the patients (30, 34%) had critical limb ischemia (CLI; Rutherford category 4–6). More than half of the patients (54, 61%) had chronic total occlusion (CTO). The mean lesion length for the complete study cohort was 24.2±11.3 cm (median 24.0, range 4–48). Forty-one (46%) patients were assigned to the SL group (mean lesion length 13.9±5.6 cm) and 48 (54%) to the FDJ group (mean lesion length 33.0±6.5 cm).
Demographic, Clinical, and Lesion Characteristics. a
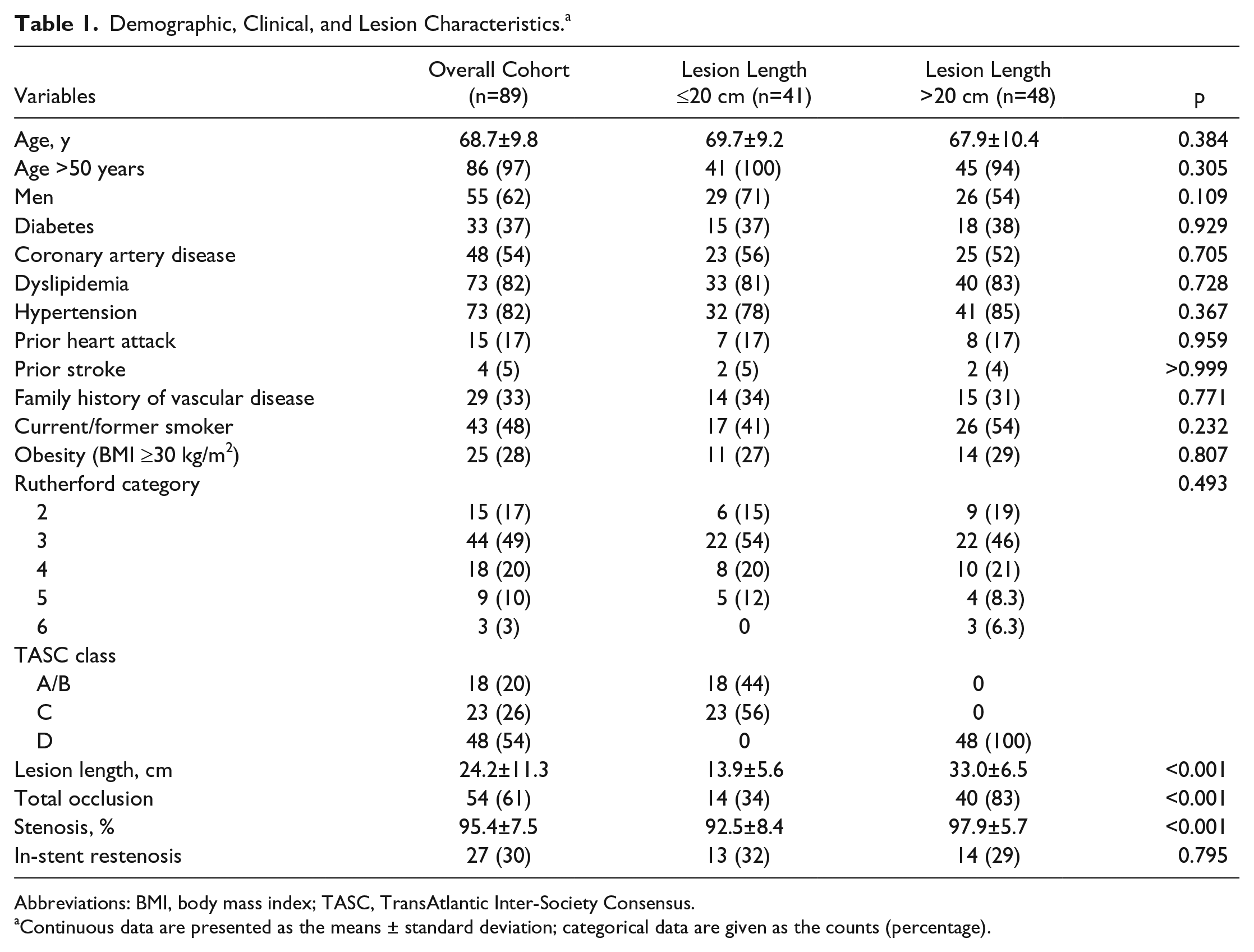
Abbreviations: BMI, body mass index; TASC, TransAtlantic Inter-Society Consensus.
Continuous data are presented as the means ± standard deviation; categorical data are given as the counts (percentage).
Procedure
All patients received aspirin (81 mg) and a clopidogrel loading dose (at least 300 mg) prior to the procedure. If the patient was already using daily clopidogrel the 75-mg daily dose was administered prior to the procedure.
Anticoagulation was achieved with heparin utilizing a goal activated clotting time of >250 seconds. Treatment of inflow and outflow disease outside the FP segment was performed at the treating physician’s discretion either before or after DES implantation. Patients being treated for FP ISR prior to DES implantation had angioplasty alone, atherectomy with or without angioplasty, or thrombectomy in addition to balloon dilation. The method of treating ISR before DES implantation was at the interventionist’s discretion.
The FP target lesions were crossed using conventional wire and catheter techniques, followed by predilation with a balloon one size smaller than the reference vessel diameter to allow for stent placement. The stent(s) were postdilated with balloons sized in a 1:1 ratio with the normal vessel diameter.
The dual antiplatelet therapy used in the previous Zilver PTX studies (clopidogrel and aspirin) was recommended for at least 60 days after the procedure, followed by lifelong aspirin therapy.
Endpoints and Statistical Analysis
Two primary endpoints were assessed at 12 and 24 months (±30 days). First, restenosis >50% was defined by a peak systolic velocity ratio (PSVR) >2.5 calculated from duplex ultrasound scans performed by registered vascular sonographers. The need for clinically driven TLR was the second efficacy endpoint. The safety endpoint was major amputation above the ankle.
Demographic and clinical characteristics and outcomes of interest were described using frequencies and percentages for categorical or dichotomous variables and means ± standard deviations and/or medians (range) for continuous variables. Differences between demographic and clinical characteristics and outcomes by lesion length were examined using chi-square or Fisher exact tests for categorical variables and 2-sample t tests or Wilcoxon rank sum tests for continuous variables. Kaplan-Meier survival curves were calculated for time to reintervention by lesion length with and without patients treated for ISR; the groups were compared using the log-rank test. Multivariable regression was used to compare odds of reintervention by lesion length while controlling for procedure variables; results are presented as the odds ratio and 95% confidence interval (CI). Statistical significance was set at p<0.05. Statistical analyses were performed using SAS Enterprise Guide software (version 7.1; SAS Institute Inc, Cary, NC, USA).
Results
Group Comparison
There was no significant difference in demographic or clinical characteristics between patients in the FDJ and SL groups (Table 1). A greater proportion of patients in the FDJ group had a total occlusion (83%) vs the SL (34%) group (p<0.001). The proportions of de novo lesions and ISR lesions were similar between the groups. Half of the patients in the ISR subgroup had CTOs, and the proportions did not differ between the groups. Prior to DES placement in the ISR subgroup, atherectomy was completed in 7 and mechanical thrombolysis in 2. The remainder underwent plain balloon angioplasty followed by DES implantation.
Early Outcomes
Procedure details are summarized in Table 2. Technical success (residual stenosis <30%) was achieved in all patients. In an effort to avoid long stent overlap, 9 (10%) patients had a BMS (no more than 4 cm in length) placed along with the DES due to limited stent lengths originally available. The average procedure time was significantly longer for the FDJ group compared to the SL patients (88.0±43.9 vs 63.8±31.8 minutes, p=0.004). However, contrast use was similar between the groups (p=0.205). Two-thirds of the patients in both groups were treated as outpatients. On discharge, all patients were placed on dual antiplatelet therapy; 68 (76%) patients were on statin therapy and 39 (44%) on angiotensin inhibition.
Procedure Details. a
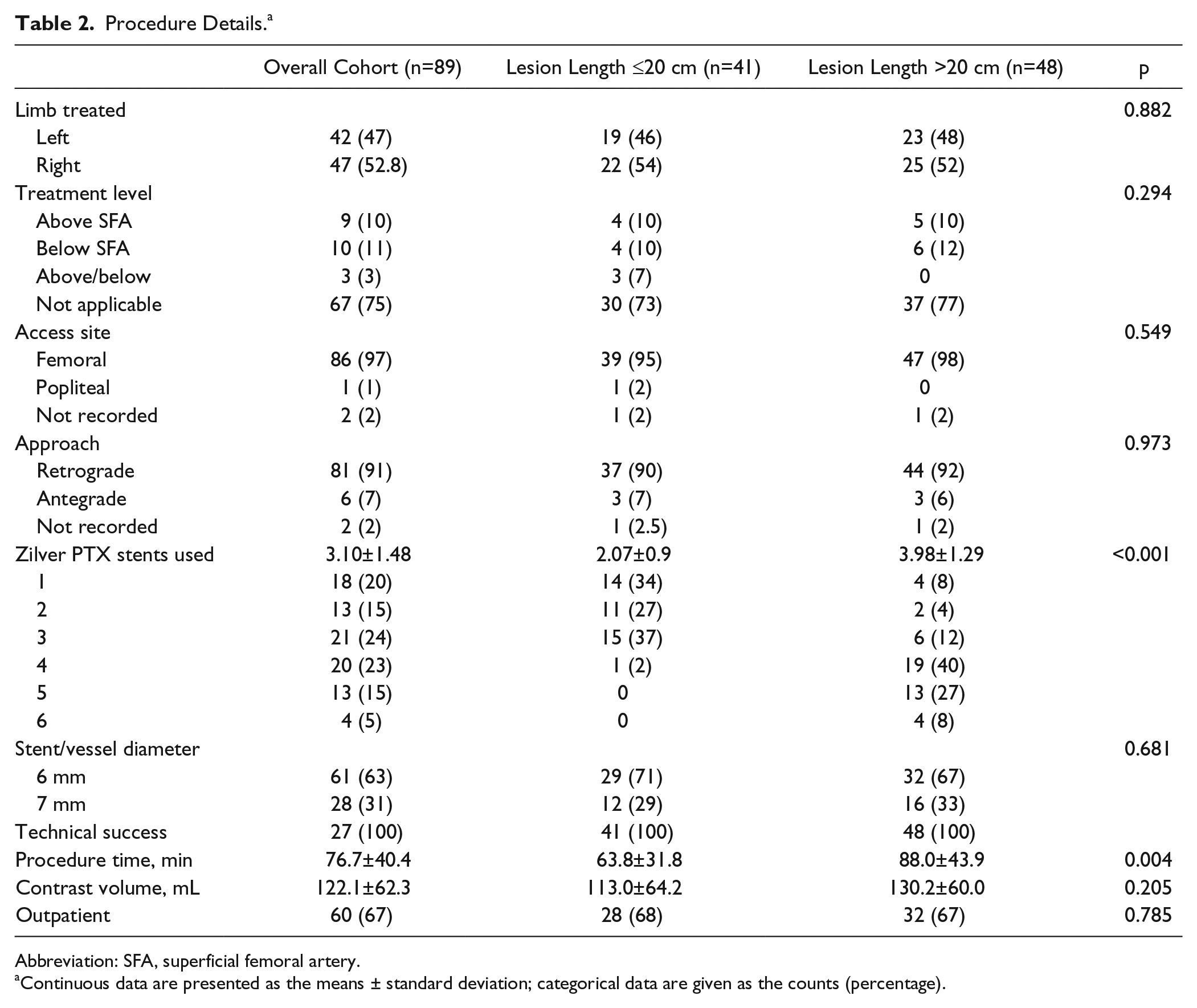
Abbreviation: SFA, superficial femoral artery.
Continuous data are presented as the means ± standard deviation; categorical data are given as the counts (percentage).
Outcomes in Follow-up
Restenosis and reintervention data are summarized in Table 3. Clinical follow-up was available for 72 (81%) patients. Twelve (13%) patients died during the 2-year observation period of causes unrelated to the procedure; 5 patients were lost to follow-up. Duplex ultrasound scans were available at 1 year in 69 (78%) patients. Three patients had angiography alone, so patency evaluation was available in 72 (81%). Restenosis occurred in 21/69 (30%) at 1 year and in 22/46 (48%) 2 years. The SL group at 1-year follow-up demonstrated a lower incidence of restenosis compared to the FDJ (19% vs 40%, p=0.050) and was associated with a statistically significant lower rate of reintervention (2% vs 21%, p=0.009).
Patency and Clinical Follow-up Data. a
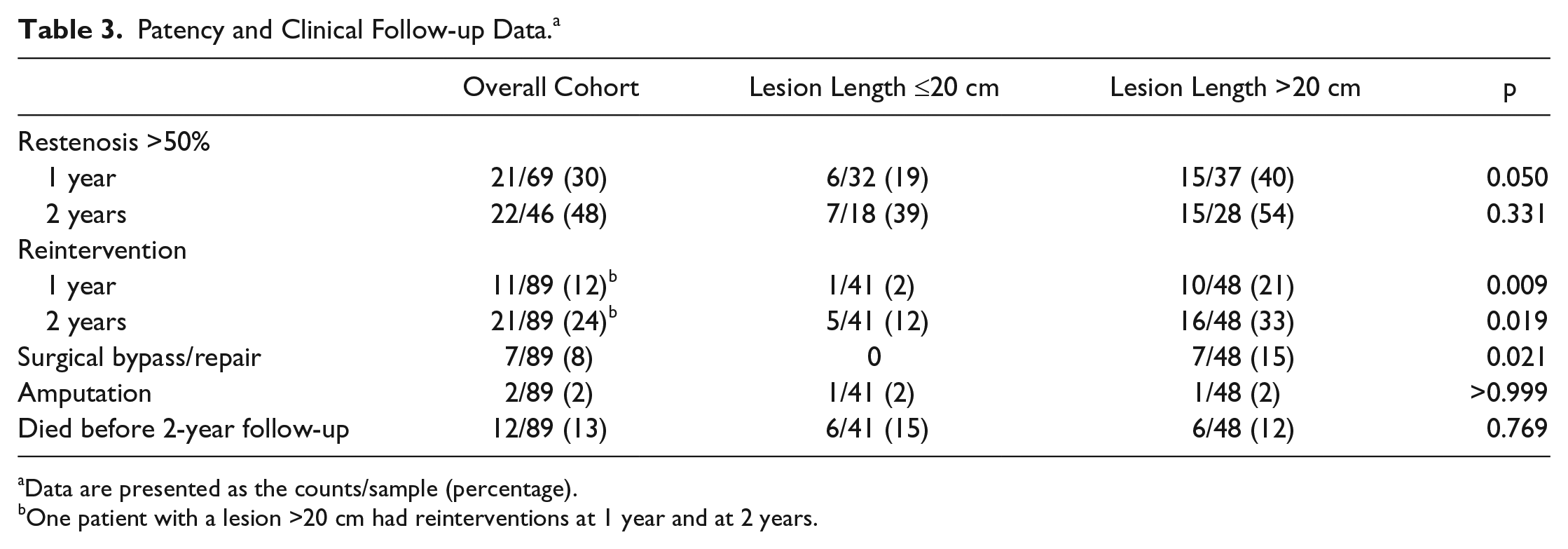
Data are presented as the counts/sample (percentage).
One patient with a lesion >20 cm had reinterventions at 1 year and at 2 years.
At 2 years, restenosis rates had increased for both groups to 39% and 54%, respectively. The need for TLR continued to be significantly lower in the SL compared to the FDJ (12% vs 33%, respectively; p=0.019). Figure 1A displays the time until reintervention by lesion length, with a lower probability of patency in the FDJ group, as the curves separate at around 5 months (log-rank p=0.016). The reinterventions involved 7 (8%, p=0.021) FDJ patients who underwent surgical bypass/repair and 2 (2%) major amputations in CLI patients, one from each group. Neither amputation was related to the procedure. Multivariable analysis demonstrated that patients in the FDJ group had greater odds of reintervention than patients in the SL group after controlling for the need for a BMS (OR 3.60, 95% CI 1.19 to 10.95, p=0.024).
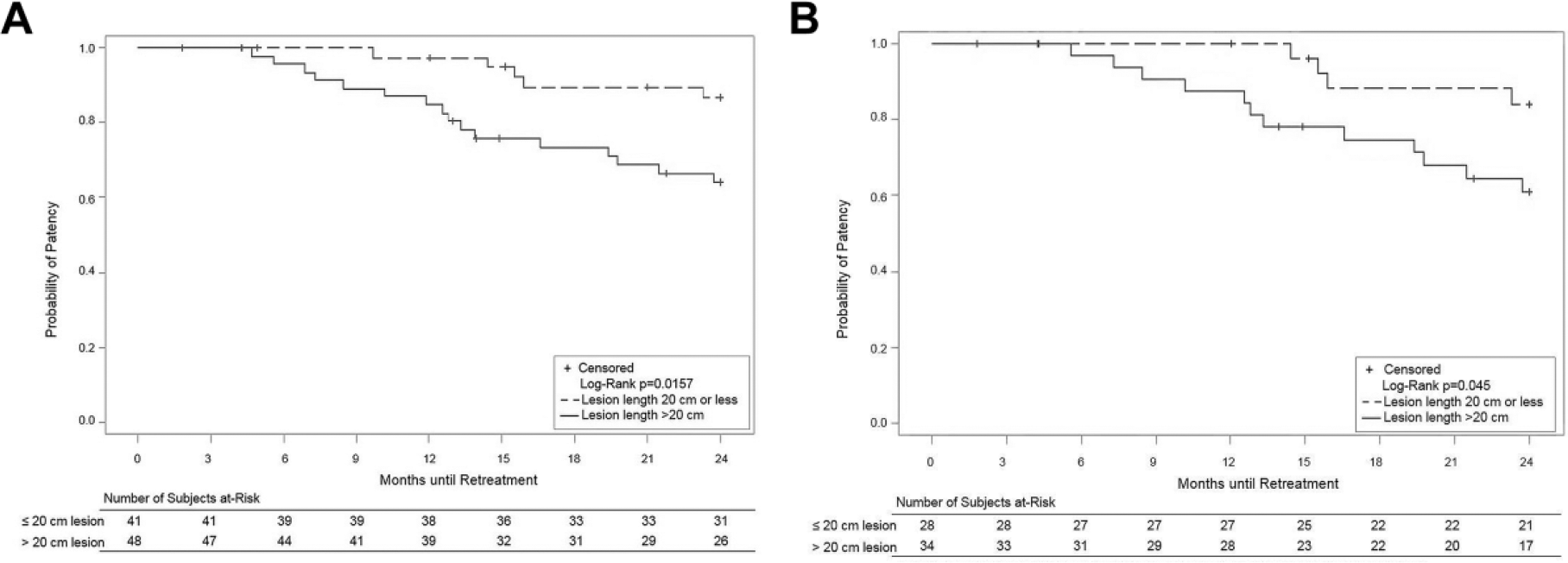
Kaplan-Meier curves of clinically driven target lesion revascularization (A) for all patients and (B) excluding patients with in-stent restenosis. The standard error did not exceed 10% at any time point to 2 years.
Of the 27 patients with ISR, 13 were in the SL group and 14 in the FDJ group. Five patients had already undergone at least 1 procedure for ISR prior to treatment with the DES; more specifically, 3 patients had 3 procedures for ISR between their index procedure with BMS and treatment with DES. TLR at 24 months was higher in the non-ISR patients in the SL group (14% vs 8%). However, in the FDJ subset, restenosis rates were greater in the ISR group (67% vs 47% in the non-ISR FDJ patients), ultimately both being equally high. Figure 1B displays the time until reintervention by lesion length in the non-ISR group. The similarity in the curves demonstrates that ISR did not play a role in the probability of restenosis in either lesion length cohort. Restenosis and reintervention rates were also not different between patients treated with a BMS or not.
Discussion
To date, there are very limited data on the treatment of FP lesions >20 cm long and even less on lesions >30 cm. Given the fact that the SFA is the longest artery in the body and is subject to constant torsion and compression, it is logical that the longer the extent of atherosclerotic disease, the higher the likelihood of restenosis and reintervention.
The 1- and 2-year results of this single-center experience shed further light on the durability and efficacy of DES for the treatment of truly complex FP disease. The long-term safety and effectiveness of the Zilver PTX stent has been clearly demonstrated in lesions <10 cm; in fact, this DES technology has reported the longest-term patency of any of the endovascular technologies in a core laboratory–adjudicated randomized trial. 2 However, it remains unclear if creating a “full metal jacket” with DES is a reasonable approach, both from durability and safety standpoints. The lesions treated in our study were longer and more complex than previously reported studies or registries evaluating Zilver PTX. The mean lesion length in this analysis was >24 cm (>30 cm in the long lesion group), with high rates of CTOs and TASC C/D lesions. The patient population itself was also complex, with multiple risk factors including high rates of diabetes, dyslipidemia, coronary artery disease, and tobacco abuse.
When specifically comparing the SL cohort with an average lesion length of 13.9 cm with the largest Zilver PTX datasets, such as the randomized trial 1 (6.5 cm), the European registry 6 (10.0 cm), the Japanese postmarket single-arm surveillance study 7 (14.7 cm), and the Zephyr study 8 (17 cm), our 12-month patency results (81.2%) are very similar (86.2%, 84.8%, 84.4%, and 83.3%, respectively). There are similar results for freedom from reintervention at 12 months (97.6% vs 83.7%, 94.7%, 91.0%, and 78.0%, respectively) and for those that reported at 24 months (87.8% vs 90.5% 1 and 83.6% 7 ).
More than a third of the FDJ patients treated with a mean lesion length of 33 cm had restenosis at 1 year; the rate increased to 54% at 24 months, suggesting perhaps if the treated segment develops restenosis, it would likely happen within the first year with less progression thereafter, similar to that observed in the randomized trial. 2 Obviously, further long-term surveillance is warranted. Despite the high rate of restenosis by duplex ultrasound, the 2-year freedom from TLR rate was ~80%. In another moderately long-lesion Zilver PTX dataset, Bosiers et al 9 reported primary patency rates of 77.6% (PSVR <2.5) and 85.4% freedom from TLR in their long lesions with an average length of 22.6± 4.4 cm. These rates compare very favorably to the low freedom from TLR rates seen in BMS trials that evaluated long segment disease.10,11 However, though DES is certainly delaying restenosis, especially for these long lesions, it appears to not be fully preventing it in the long term. The lowered need for revascularization may also be in part due to a lower restenosis plaque burden pattern that was recently reported. 12
The use of a “full drug jacket,” particularly with treatment lengths averaging over 30 cm, could be considered an endovascular form of bypass. This comparison is being addressed in the European-initiated ZILVERPASS study, 13 which is randomizing patients 1:1 to Zilver PTX or surgical bypass for TASC C and D lesions. With contemporary primary patency rates of ~78% at 12 months for surgical bypass, comparing the FDJ with surgical bypass could shed some light on the durability of these treatment modalities, potentially paving the way for a preferred method.
The clinical impact of restenosis after FP stenting is not benign, 14 as demonstrated by Tosaka at el. 15 In their retrospective study, restenosis after FP stenting was classified based on 3 angiographic patterns: focal lesions defined as ≤50 mm (class I), diffuse lesions >50 mm in length (class II), and complete in-stent occlusion (class III). After treatment with balloon angioplasty, class III ISR was associated with increased risks of recurrent ISR (84.8%), recurrent occlusion (64.6%), and surgical revascularization at 2 years. 15
Nearly equal but small numbers of patients in each group were treated for ISR (13 in the SL group and 14 in the FDJ group). Interestingly, the ISR group and non-ISR groups appeared similar in the SL subset. In fact, TLR rates at 24 months were higher in the non-ISR patients than in the SL group. However, in the FDJ subset, restenosis rates were greater in the ISR group. These data support the notion that regardless of ISR, the longer lesions tend toward higher rates of restenosis yet, in our opinion, have acceptable TLR rates. In addition, having ISR prior to DES implantation did not reduce the probability of patency when comparing the Kaplan-Meier estimates. These findings again suggest that DES is an acceptable treatment option for ISR irrespective of lesion length, with shorter lesions maintaining greater patency over time. Finally, the use of DES in ISR appears safe, as we had no amputations in the ISR group, with little effect on patency.
There was little need for conversion to surgical revascularization due to stent occlusion, which occurred only in the FDJ group. The 2 major amputations were not attributed to the index procedure; both patients had CLI and wound deterioration despite successful FP recanalization. Finally, there were no major complications leading to acute limb ischemia, further demonstrating the safety of using DES in long complex lesions that require several stents.
Whether longer term antiplatelet therapy would improve results is an important question. Patients in this study were on an antiplatelet regimen specified in the randomized trial; however, since that time there has been a case report of thrombus and exposed Zilver PTX struts at 6 months. 16 Further data are needed to address this issue.
Limitations
Limitations of this analysis include its retrospective nature, single-center site, and incomplete follow-up. No data were collected on stent fracture nor were radiograms performed to formally track fractures. Also, any potential role of stent fracture pertaining to patency was not addressed; however, in general the rate of stent fracture in the Zilver PTX experience worldwide is <2%, which was also reflected in the 5-year data from the randomized trial. 2 Finally, because of the limited length of currently available stents, a greater number of stents with more regions of stent overlap were needed to treat the long lesion cohort, perhaps influencing the patency and restenosis rates.
Conclusion
Although there were similar patency and TLR rates in our short lesion group compared to similar studies, our higher rates of restenosis and greater need for reintervention in the “full drug jacket” group reinforces the need for continued research and refinement of our endovascular methods in very long, complex lesions. However, despite having patency rates <50% at 24 months in the full drug jacket group, the 67% freedom from reintervention ultimately illustrates that the use of Zilver PTX in lesions >20 cm is both feasible and a clinically effective treatment for these patients with lifestyle-limiting peripheral artery disease. Head-to-head trials of drug-based endovascular technology are needed in complex FP disease.
Footnotes
Authors’ Note
Preliminary data from this study were presented at the International Symposium on Endovascular Therapy 2017 (February 4–8, 2017; Miami, FL, USA) and the Amputation Prevention Symposium 2017 (August 8–11, 2017; Chicago, IL, USA).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: John A. Phillips is a consultant to Cook Medical. Gary M. Ansel is a consultant to and receives royalties from Cook Medical.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.