
Abstract
Introduction
Thoracic aortic mural thrombus (TAMT) that develops without concomitant atherosclerotic occlusive or aneurysmal disease is a relatively uncommon pathological finding with potentially devastating complications.1,2 In the literature, the incidence in the general population has been reported to be 0.45%, with 17% of the cases involving distal embolization. Six percent of the embolization cases were severe enough to be lethal. 3 The origin of TAMT has been most commonly attributed to hypercoagulable states, trauma, smoking, use of steroids, drug abuse, primary endothelial disorders, iatrogenic causes, and history of vasculitis.1–6
Although TAMT is an uncommon pathological entity with a difficult differential diagnosis, it remains a significant source of noncardiogenic emboli (stroke, end-organ damage, acute limb ischemia).1,4 The treatment strategy for this disease remains controversial and is determined by the location and extent of the thrombus, presence of complications, patient comorbidities, and the physician’s preferences. 7 Options include anticoagulant therapy, aspiration thrombectomy, surgical thrombectomy, or endovascular repair using covered stent deployment. 7
The presented technique involves a unique application of the AngioVac System (AngioDynamics, Latham, NY, USA), a dedicated device for venous thrombus removal, 8 to aspirate TAMT from the ascending aorta. The AngioVac System has been approved by the US Food and Drug Administration “to remove fresh, soft thrombi or emboli during extracorporeal bypass for up to 6 hours.” 9 It has been suggested as an effective treatment modality for aspirating large volumes of acute and subacute thrombus in larger veins, such as the inferior vena cava and iliac veins. 8
Technique
The technique is demonstrated in a 66-year-old woman with brain metastases from a non–small cell adenocarcinoma with a primary origin in the lungs. She was referred to our institution following a staging computed tomography angiography (CTA) scan that revealed a free-floating TAMT in the ascending aorta 17 mm from the sinotubular junction and 42 mm from the innominate artery (outer curvature), which had no signs of calcification (Figure 1A and B).
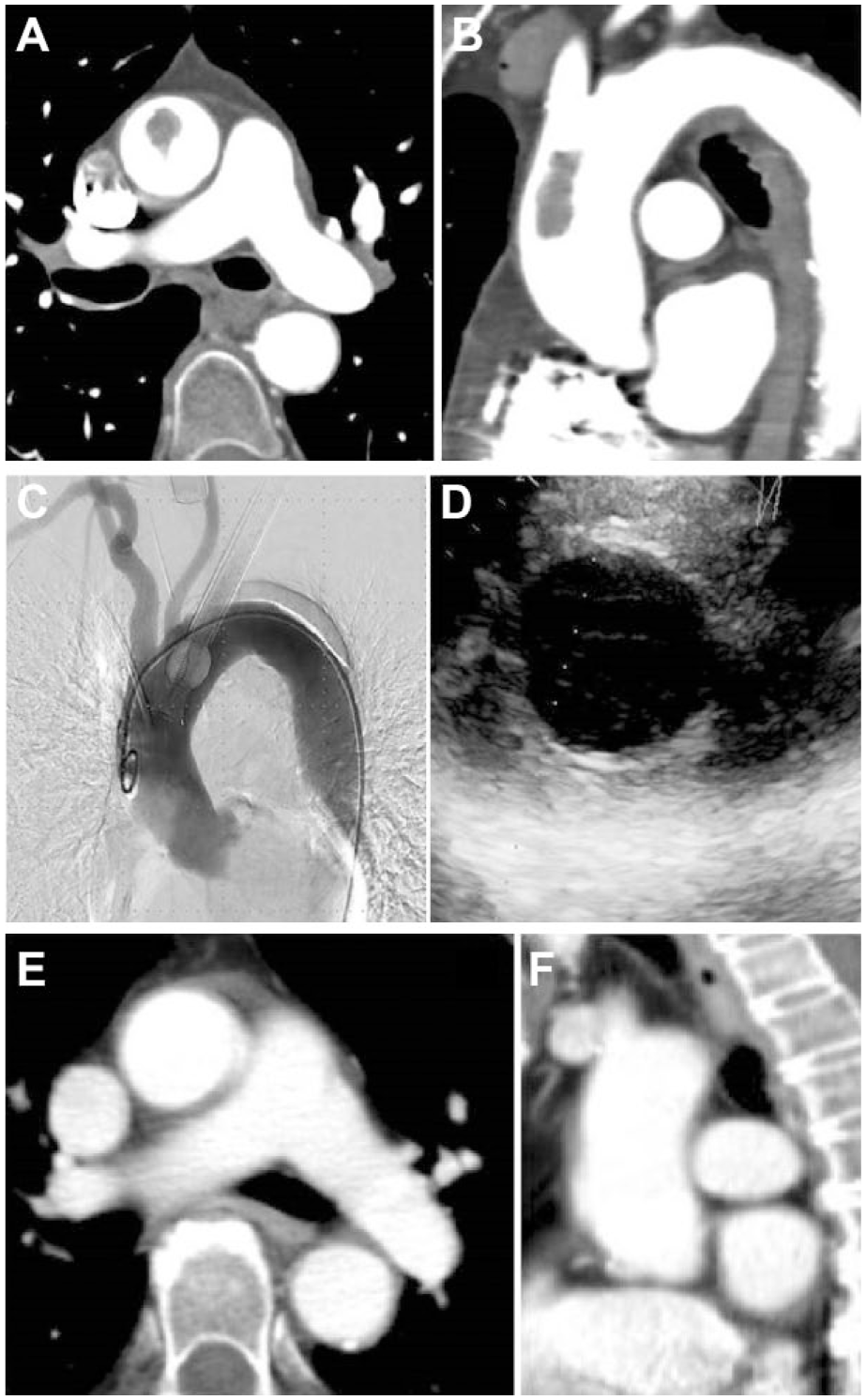
Computed tomography angiography (CTA) in the (A) axial and (B) sagittal planes documented a free-floating thoracic aortic mural thrombus in the ascending aorta. (C) The AngioVac was inserted over the sheath through the conduit and exact advancement of the suction was guided by transesophageal echocardiography (D). A pigtail catheter was advanced in the ascending aorta only after thrombus aspiration to acquire the final angiogram. (E) Axial and (F) sagittal CTA scans revealed no signs of any free-floating mural thrombus in the ascending aorta.
The patient had recently undergone resection of the brain metastases and was currently in planning for chemotherapy and potential resection of the primary tumor. She was considered an unsuitable candidate for open aortic surgery under cardiopulmonary bypass and cardiac arrest. An endovascular approach (stent-graft) was considered but any wire manipulation at the area of the ascending aorta would most likely dislocate the thrombus and cause stroke. Conservative treatment with anticoagulation only was discussed with the patient but was considered also high risk because of the very small stalk of the thrombus, making the risk of embolism very high. Because of the free-floating nature of the TAMT it was decided to use the AngioVac device.
Inasmuch as the 22-F AngioVac System was constructed for use in the venous system, a technique had to be devised for arterial use. In venous procedures, there are 2 access points required, one aspiration access for the AngioVac cannula and one for the reinfusion cannula. The access points may include any combination of the femoral vein and/or internal jugular vein. In this case, it was decided that the arterial access point would be the proximal left subclavian artery (LSA), which was chosen because it provided the right angle to advance the AngioVac cannula without wire manipulation in the ascending aorta. It would require suturing of a 10-mm conduit in a side-to-end fashion for device access. The other access would be the right femoral vein.
An extracorporeal bypass circuit would be created consisting of an outflow line, a centrifugal pump, a filter, and an inflow line. The AngioVac cannula has a balloon-activated tip that prevents clogging of the cannula and facilitates the removal of fresh, soft thrombi or emboli from the venous system into the filter. The carotid arteries would be exposed without any arteriotomy and clamped (<1 minute) during the aspiration maneuver to avoid cerebral embolization. Any debris would flow into the LSA or the distal aorta since the carotid flow would be temporarily interrupted.
The procedure was performed with the patient under general anesthesia in a hybrid room; simultaneous transesophageal echocardiogram (TEE) monitoring was initiated. Intravenous unfractionated heparin was administered with a targeted activated clotting time >250 seconds throughout the procedure. To facilitate the advancement of the AngioVac cannula close to the thrombus without prior wire manipulation, a 26-F sheath was first advanced into the aortic arch with a super-stiff wire placed in the descending aorta. Thus, the sheath was inserted over a wire with an orientation toward the descending aorta, and once the dilator and the wire were removed the sheath resumed an orientation toward the ascending aorta.
The AngioVac was inserted over the sheath and the 22-F reinfusion cannula was inserted into the right femoral vein. Exact advancement of the AngioVac cannula was guided by TEE (Figure 1C and D). The centrifugal pump was activated, which created a one-way flow that provided suction at the tip of the AngioVac cannula in the aorta and retransfusion into the vein system. After a single pass, the TAMT was aspirated successfully without any hemodynamic changes identified by TEE or the intraoperative angiogram. After removal of the 26-F sheath, local dissection and rupture of the LSA was successfully managed with covered stents. A final visceral angiogram was also performed with no pathological findings. The endovascular part of the procedure lasted 40 minutes. The patient had an uneventful postoperative course without any clinical neurological findings.
In the postoperative CTA, the ascending aorta was free of any TAMT (Figure 1E and F), and the CT scan of the head did not reveal any strokes. The patient was on aspirin and a therapeutic dose of low-molecular-weight heparin for 1 week and only aspirin thereafter; no oral anticoagulant was administered after consultation with the oncologists. The patient had further treatment of the lung cancer, and at 8-month follow-up, no residual or recurrent thrombus was present on the CTA.
Discussion
The rarity of TAMT and the difficulty in its diagnosis have hindered any determination of its natural history or optimal treatment. The presence of TAMT remains a controversial treatment dilemma, with no clear preference for surgical, endovascular, or solely medical treatment. 2 However, it seems that recent reports tend to favor invasive treatment. Fayad et al 6 presented a systematic review of the 98 articles comprising 200 patients, comparing surgical treatment to conservative medical treatment. They demonstrated that open repair was superior to medical treatment in terms of persistence of aortic thrombus (5.7% vs 26.4%, p<0.001), recurrence of peripheral artery embolization (9.1% vs 25.7%, p<0.003), complications (17% vs 27%, p<0.07), and major limb amputation (2% vs 9%, p<0.004). In another more recent systematic review, Meyermann et al 1 included 32 studies showing that patients with TAMT treated medically were more likely to present persistent thrombus compared with open or endovascular aortic repair. They also suggested that endovascular therapy may be a useful first-line option for TAMT because of the reports of positive outcomes in select literature; however, further study of this treatment option is required.
Recent studies2,10 highlighted the potential role of thrombus mobility in the selection process of interventional rather than conservative treatment. Endovascular repair of TAMT is most commonly performed by covering the respective aortic segment with a stent-graft. 10 While this is feasible and fairly uncomplicated in the descending thoracic aorta, stent-grafting of the thrombus in the ascending aorta or the aortic arch 11 is much more complicated and requires more wire and device manipulation than standard thoracic endovascular aortic repair. Therefore, open surgical techniques have been preferred for the aortic arch and the ascending aorta when invasive therapy was deemed necessary. 12
In a recent systematic review of the literature, Jabaar and Jenkins 13 suggested that vacuum-assisted thrombectomy using the AngioVac System is a minimally invasive alternative to surgical thrombectomy for managing chronic venous thromboembolism. The use of this device in iliocaval thrombosis appeared to be safe and effective compared to other anatomical locations. 13 No retroperitoneal bleeding, caval injury, or procedure-related mortality was noted.
The AngioVac System has been also used in the abdominal aorta in a patient with symptomatic aortic thrombus complicated by mesenteric ischemia arising from paravisceral aortic thrombus involving the celiac artery and superior mesenteric artery. 14 This patient was also treated with over-the-wire thrombectomy and stenting to successfully restore blood flow within the superior mesenteric artery. However, no technique has been presented until now describing the use of AngioVac in the aortic arch.
The advantage of the AngioVac device with the current off-label technique is that no manipulation close to the thrombus was necessary prior to the aspiration maneuver. The potential risk of thrombus dislodgement during aspiration is high, so protective measures against cerebral embolism should be taken whenever possible. In our institution, the technique has been successfully used in 2 further cases, one for thrombus aspiration in the ascending aorta, again using a transaxillary approach, and in one case for thrombus aspiration from the right atrium.
Disadvantages of the technique are the 22-F profile of the device, which requires a 26-F sheath to safely advance it, and the stiffness of the device, which hampers its more frequent use in such cases. The potential high cost of the procedure is another potential limitation.
Conclusion
The use of the AngioVac System seems to be a feasible technique for aspiration of thrombus from the ascending aorta. Expanding this therapeutic option for patients unsuitable for open or endovascular repair may be proven efficient in the near future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Nikolaos Tsilimparis and Tilo Kölbel are proctors for Cook Medical. Tilo Kölbel received research and travel grants from and has intellectual property with Cook Medical.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.