
Abstract

Keywords
Feasibility of thoracic endovascular aortic repair (TEVAR) for type B aortic dissection (TBAD) continues to be a subject of debate. Current guidelines recommend optimal medical therapy for acute TBAD with continued imaging surveillance. 1 TEVAR is reserved for patients who present with complications. 1 However, 50% of patients who are initially treated with optimal medical therapy alone develop aneurysmal degeneration of the weakened aortic wall during follow-up. 2
The study of Menichini et al 3 in the October 2018 issue of the JEVT presents 2 patients with aneurysmal dilatation of the thoracic false lumen following TBAD. Both patients were treated with TEVAR, patient 1 in the chronic phase and patient 2 in the subacute phase. Early follow-up results were satisfactory, but at 14-month follow-up a stent-graft–induced new entry tear (SINE) with aneurysmal dilatation was observed at the distal end of the stent-graft in patient 1. The dissected aorta in patient 2 remained stable. With the caveat of the simplistic modeling approach of this analysis, which considered the aorta as a linear elastic material and disregarded the prestress, computational analysis showed higher stress, torsional strain, and wall displacement in patient 1 compared with patient 2. The region of high stress and displacement corresponded well with the location of SINE. The authors conclude that tortuosity, curvature, and thoracic aortic length have a strong influence on local stress distributions and risk of SINE. We agree that patient-specific anatomical features can impose challenges for successful endovascular repair of TBAD and would like to comment on planning TEVAR in such cases.
In TBAD, timing has important implications for the biomechanical properties of the intimal flap. 4 In the acute phase (within 2 weeks from onset of dissection), the intimal flap is still thin and highly mobile. Covering the proximal entry tear with a stent-graft in this phase induces positive aortic remodeling by reducing perfusion of the false lumen, approximating the intima to its original position, and opening the true lumen. This way, TEVAR in the acute phase has been shown to improve survival compared to optimal medical therapy alone.5,6 Following the acute phase, the intimal flap becomes thicker and less mobile (Figure 1). 4 After 8 to 12 weeks, TBAD is classified as chronic. TEVAR in the chronic phase is more challenging as the thickened intimal flap does not approximate to the aortic wall as it would in the acute phase. 7 Furthermore, complete thrombosis of the false lumen is less likely to occur due to formation of persistent distal intimal tears that accommodate perfusion of the false lumen after TEVAR. 7 Consequently, aortic remodeling is limited. 8
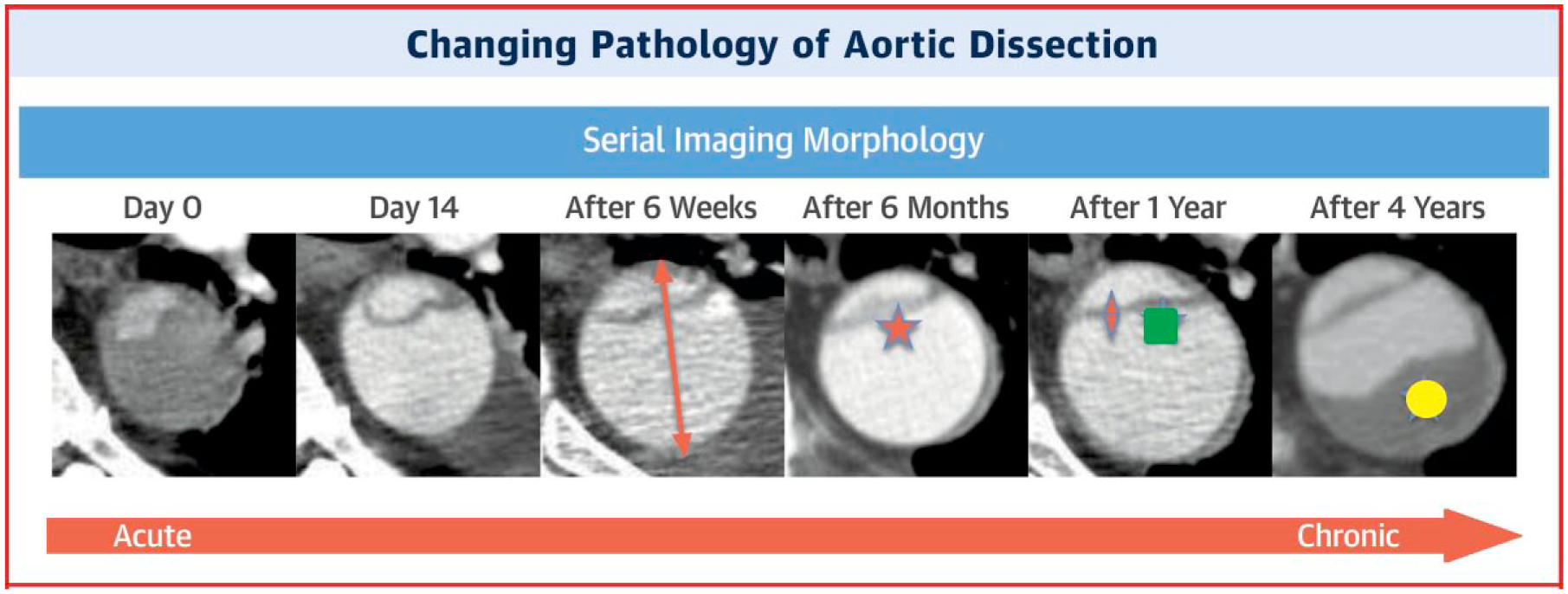
Changing morphology over time of an individual patient’s type B dissection captured by good quality computed tomography images at the same aortic level. Please note the (1) marked early increase in aortic diameter (orange arrow); (2) intimal thickening over time (orange star); (3) decreased flap motion over time (orange diamond); (4) flap straightening over time (green square); and (5) increased false lumen thrombosis over time (yellow circle). Reprinted with permission from Peterss et al. 4
Another challenging factor when performing TEVAR for TBAD is the tortuosity of the dissected aorta. Tortuosity increases wall stresses due to the spring-back forces in the stent-graft, 3 reduces stability in the landing zones, 9 and increases hemodynamic displacement forces that can cause stent-graft migration.10,11 To secure stability, the stent-graft needs to be sized correctly. The proximal and distal landing zone lengths should be at least 2 cm to accommodate safe deployment. If the landing zones are angulated, longer lengths should be considered to provide a larger area of healthy aortic wall for secure fixation.9,12 Oversizing of the stent-graft diameter aids fixation in the landing zones, yet excessive oversizing (>20%) needs to be avoided as this is known to induce disadvantageous stress distributions (Figure 2) 9 and is associated with SINE. 13 When planning for TEVAR, stent-graft diameter is often selected based on the total aortic diameter (true lumen + false lumen). This approach is correct if the true lumen opens completely after stent-graft deployment. In the chronic phase, however, the thick intimal flap and false lumen thrombosis (Figure 3) can restrict expansion of the true lumen. The radial force that resides in the partially unfolded stent-graft increases the risk of SINE. Therefore, it is suggested to avoid significant oversizing when planning TEVAR for chronic TBAD.1,7–9
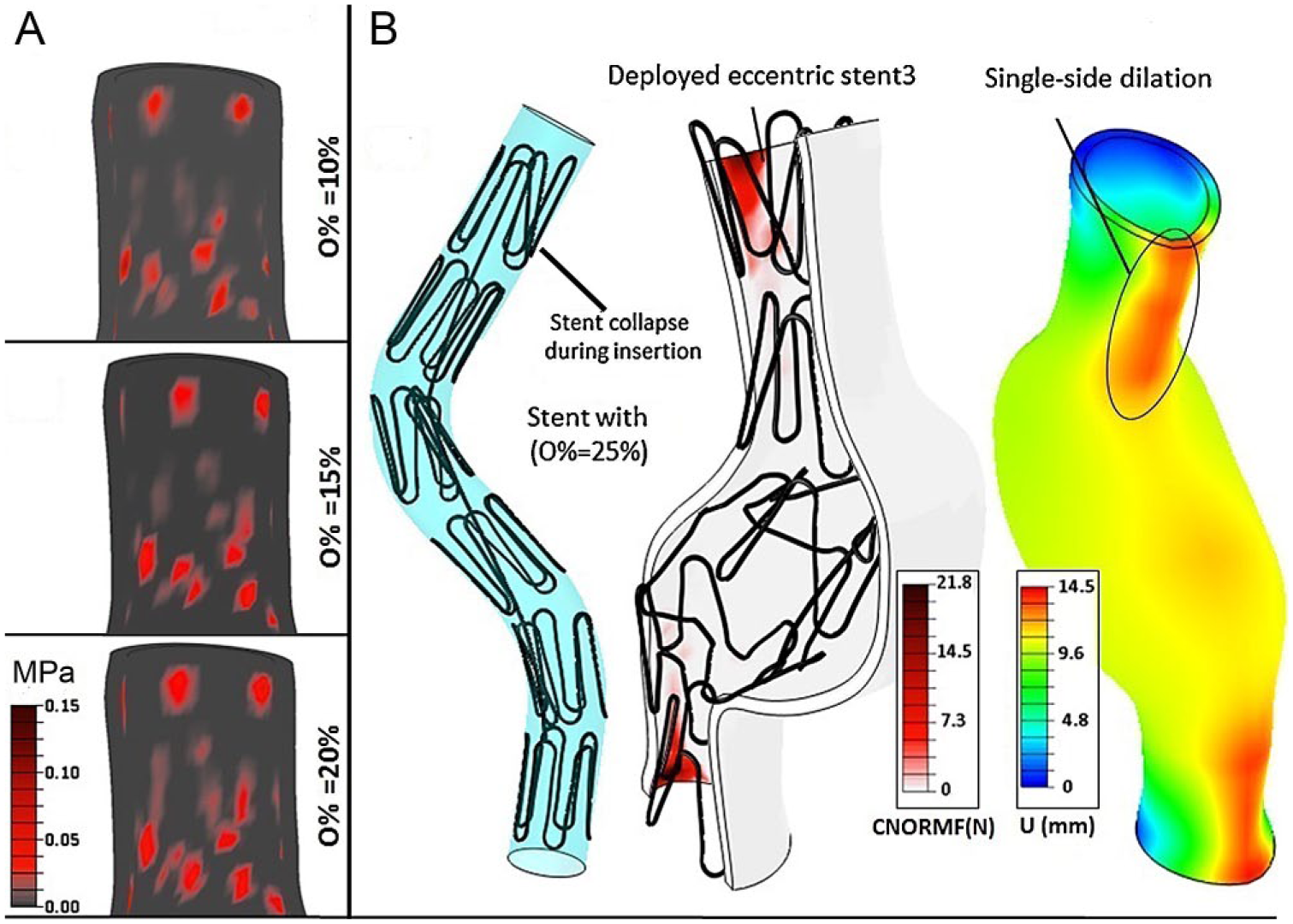
(A) Contact stresses in the proximal landing zone for different percentages of oversizing (O%). (B) Excessive oversizing (O%=25%) with stent-graft collapse and increased dilatation (U) in the landing zones. Reprinted with permission from Altnji et al. 9

Thickened dissection flap with false lumen thrombosis in a patient with a chronic type B dissection. Reprinted with permission from Kasirajan et al. 7
Preferably, all patients who will develop postdissection aneurysmal dilatation should be treated in the acute phase. However, it would be harmful to subject patients who may never develop aneurysmal dilatation to the risks of TEVAR-related complications such as retrograde dissection, stroke, and spinal cord ischemia. The challenge therefore remains selecting those patients who will develop aneurysmal dilatation from those who will not. At this point, no guidelines are available to aid early patient selection. Future research may fill this void, using 4-dimensional flow magnetic resonance imaging and patient-specific computational modeling to identify hemodynamic characteristics that can predict the risk of aneurysmal dilatation following uncomplicated TBAD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.