
Abstract
Keywords
Introduction
Up to 20% of patients with critical limb ischemia (CLI) are considered poor candidates for endovascular revascularization because of extensive noncrossable occlusions in the below-the-knee (BTK) or below-the-ankle (BTA) vessels. Percutaneous venous arterialization could be an alternative technique for limb salvage in these patients with no-option CLI. 1 However, up to 20% of these procedures can fail because of the inability to create the arteriovenous (AV) communication. 2 The Limflow system (Limflow SA, Paris, France) is a dedicated device that can help overcome this challenge, but it significantly increases the overall procedure cost and is not always available. 3 Herein is described the venous arterialization simplified technique (VAST) using a low-profile balloon catheter and a snare to facilitate AV fistula (AVF) creation during venous arterialization.
Technique
Under local anesthesia with sedation, tibial or pedal vessel recanalization is first attempted in a standard fashion. If conventional wire/catheter maneuvers fail, the VAST maneuver can be considered. The 0.014-inch guidewire (Command ES; Abbott Vascular, Redwood City, CA, USA) is left in place at the level of the noncrossable lesion, and a 2.5- to 3×40-mm, low-profile balloon catheter (Armada; Abbott Vascular) is advanced over it. Venous access is achieved by ultrasound-guided puncture of a tibial or BTA vein, and a 4-F sheath (Cook Medical, Bloomington, IN, USA) is inserted from the ankle in a proximal direction. A 5-mm GooseNeck snare (Covidien/Medtronic, Minneapolis, MN, USA) is advanced through the sheath, up to and parallel with the arterial balloon catheter. Once the 2 elements are aligned, the image intensifier is adjusted to acquire the best projection angle to view the snare loop (fully open) and the inflated balloon overlapping. To verify the position of the artery with regard to the vein (using the radiopaque markers of the balloon and the snare as landmarks), an angiogram is performed in an orthogonal view with respect to the former projection. The final position adopted by both vessels decides which of the following techniques is applicable. The first technique is employed if the vein is positioned anterior to the artery, while the second technique is followed when the vein is located posterior to the artery. Following additional infiltration of local anesthetic, and with an entry needle angle almost perpendicular to the skin surface, a 22-G micropuncture needle (Arrow International Inc., Reading, PA, USA) is advanced percutaneously (under fluoroscopy) through both vessels in line with the image intensifier.
VAST 1 (Vein Anterior to Artery)
The needle is inserted pointing to the snare loop and passing through both walls of the vein, including the snare loop. At this point, the snare is tightened to confirm needle traversal. Once the needle has exited the vein, it is further advanced until it reaches the artery and punctures the balloon catheter. A 0.018-inch guidewire (Command; Abbott Vascular) is advanced through the needle and placed inside the punctured balloon catheter. The balloon catheter is completely withdrawn while maintaining the guidewire entrapped inside so that the wire from the venous access can be externalized through the femoral artery sheath. After establishing this femorotibial AV through-and-through wire, a 4-F support catheter (Terumo, Tokyo, Japan) is advanced over the wire antegradely up to the vein. Finally, a second 0.014-inch guidewire (Command; Abbott Vascular) is introduced into the catheter and advanced until it is clearly positioned within the venous lumen. Vessel access is confirmed by gentle injection of contrast. Once the AVF has been created, both the first guidewire and the venous sheath are withdrawn; the AV anastomosis is dilated (Figures 1 and 2).
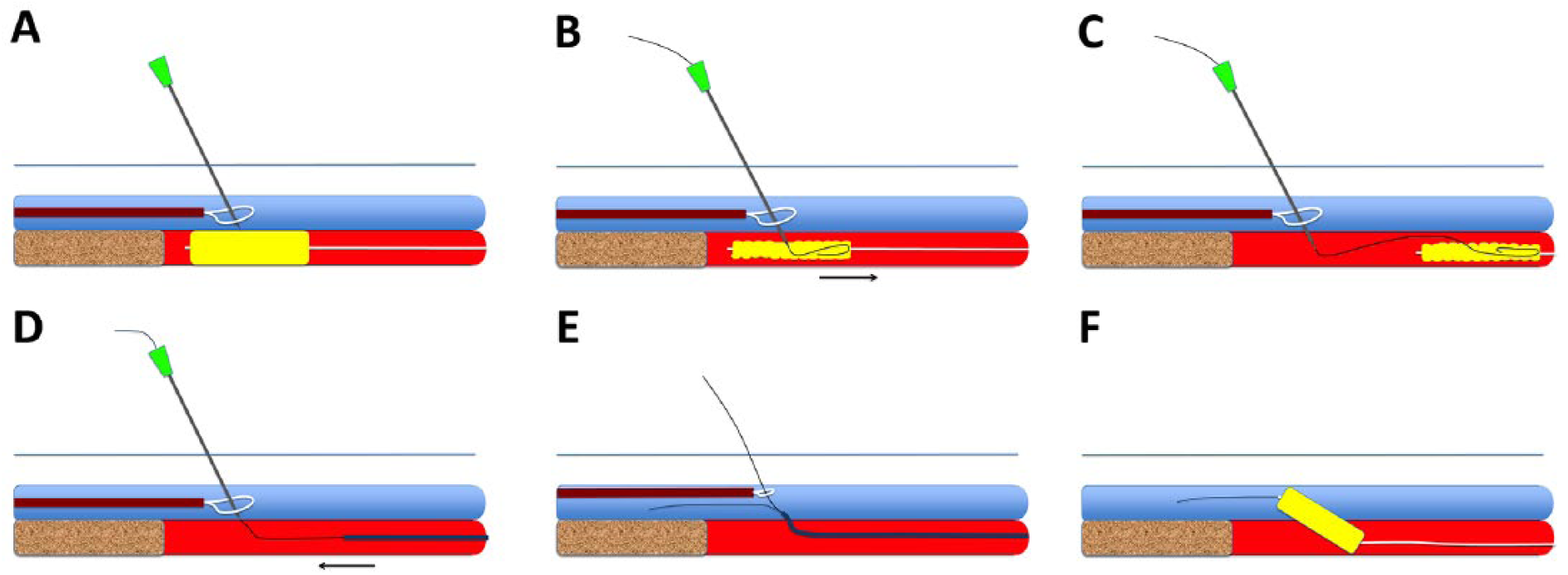
Diagram of the venous arterialization simplified technique 1 (the vein is positioned anterior to the artery). (A) The needle is inserted, passing through both walls of the vein and the snare loop. (B) The needle reaches the artery and punctures the balloon catheter. A 0.018-inch guidewire is advanced and placed inside the punctured balloon. (C) The balloon catheter is withdrawn, maintaining the guidewire’s position so that it can be externalized through the femoral sheath. (D) A support catheter is advanced antegradely. (E) A second 0.014-inch guidewire is advanced until it is clearly positioned within the venous lumen. (F) Angioplasty of the arteriovenous communication.
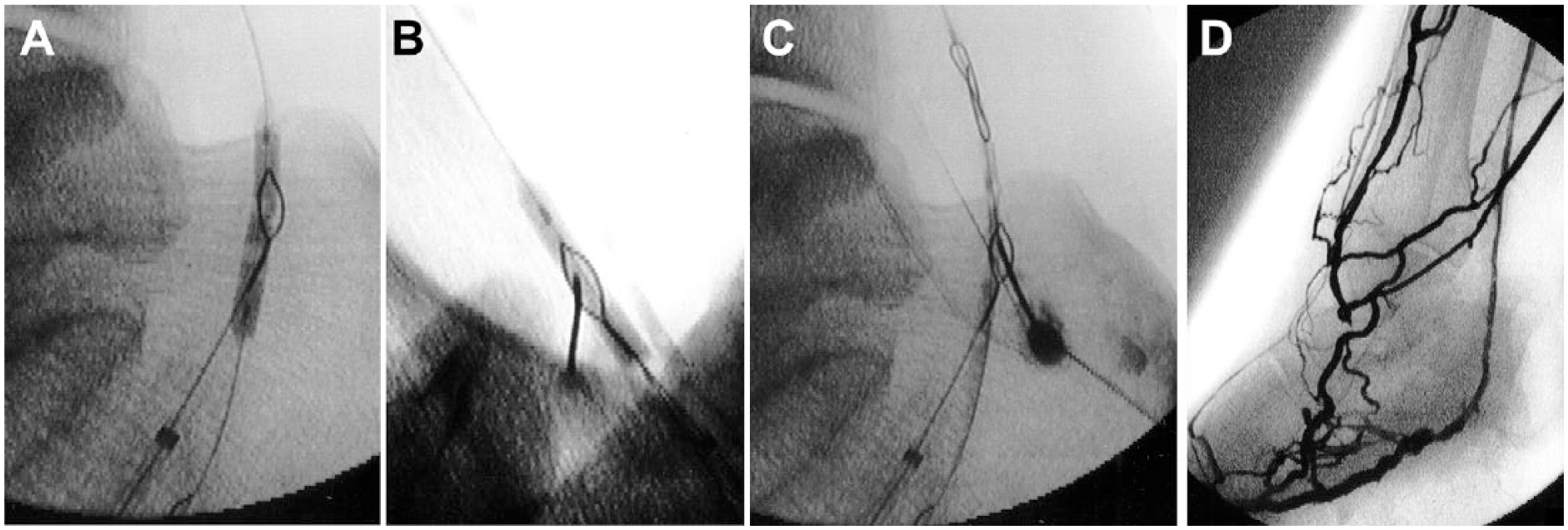
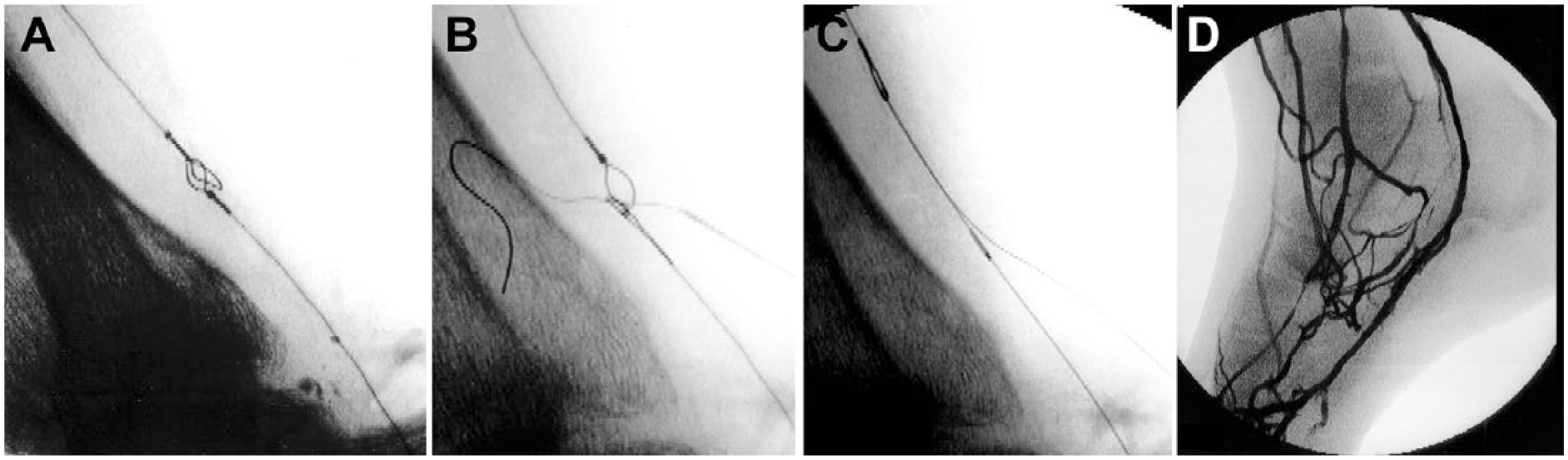
Intraoperative fluoroscopy images of the venous arterialization simplified technique 1. (A) A fluoroscopic projection is obtained that overlaps the snare and the inflated balloon. (B) A 22-G needle is advanced percutaneously in plane with the image intensifier through both vessels. (C) The balloon catheter is withdrawn while maintaining the guidewire entrapped inside it. (D) Angiogram of the venous arterialization.
VAST 2 (Artery Anterior to Vein)
The needle is inserted pointing to the balloon (as a landmark of the arterial position) and passing through both walls of the balloon. Once the needle has exited the artery, it is further advanced pointing to the center of the snare loop until it completely pierces the vein passing through the snare loop. The loop is tightened to confirm needle traversal, and a 0.018-inch Glidewire (Terumo) is advanced. The needle is withdrawn and the snare closed and retrieved so that the wire is grasped and externalized through the venous access. The pierced balloon catheter is gently retrieved, and a 4-F support catheter is introduced in the venous sheath and advanced over the wire from the vein into the artery. Finally, a second 0.014-inch guidewire (Command; Abbott Vascular) is introduced into the catheter and advanced until it is clearly positioned within the arterial lumen. Vessel access is also confirmed by gentle injection of contrast. The first guidewire and the arterial balloon catheter are then completely retrieved, and the AV anastomosis is dilated through the 4-F venous sheath (Figures 3 and 4).
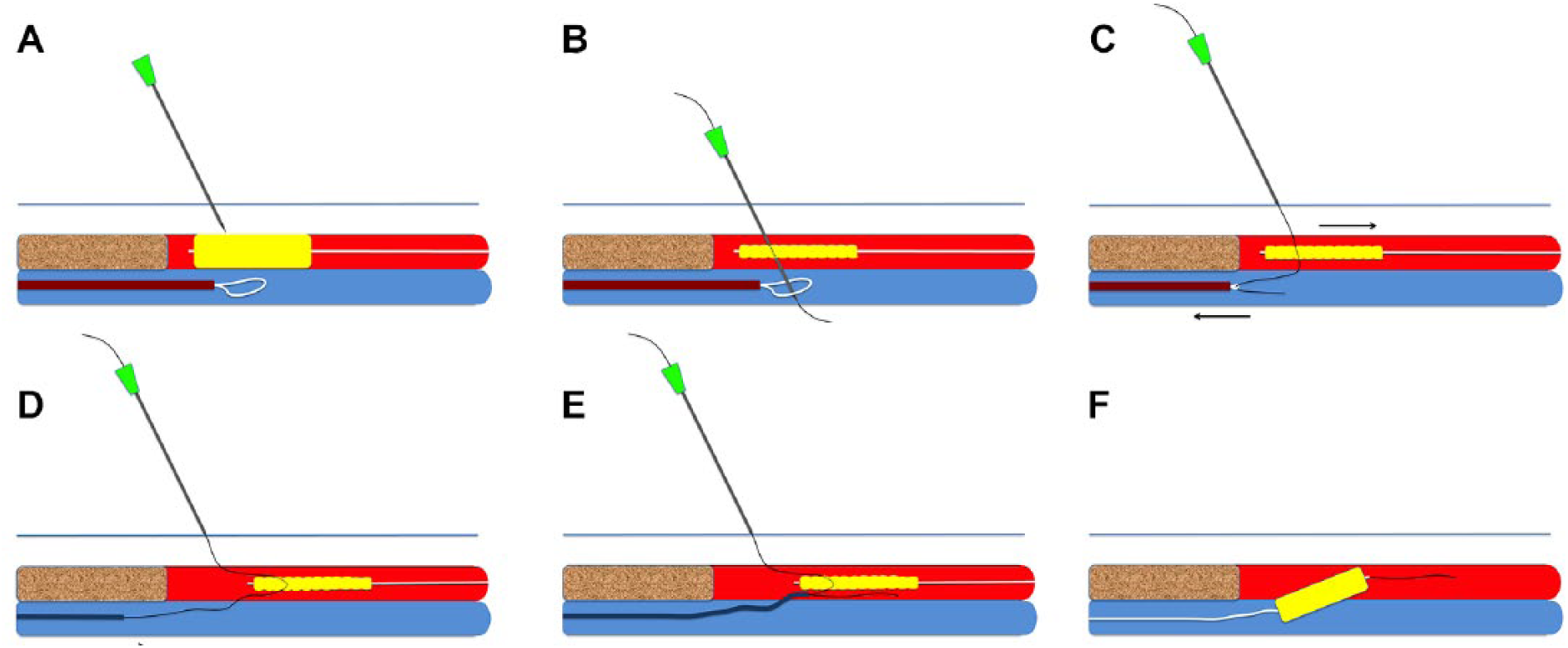
Diagram of the venous arterialization simplified technique 2 (the vein is positioned posterior to the artery). (A) The needle is inserted pointing to the arterial balloon catheter. (B) The needle is further advanced, crossing through the balloon catheter and finally piercing the vein while crossing through the snare loop. (C) The needle is withdrawn; the snare is closed and retrieved through the venous sheath. (D) A support catheter is advanced over the wire from the vein into the artery. (E) A second 0.014-inch guidewire is advanced until it is clearly positioned within the venous lumen. (F) Angioplasty of the arteriovenous communication.
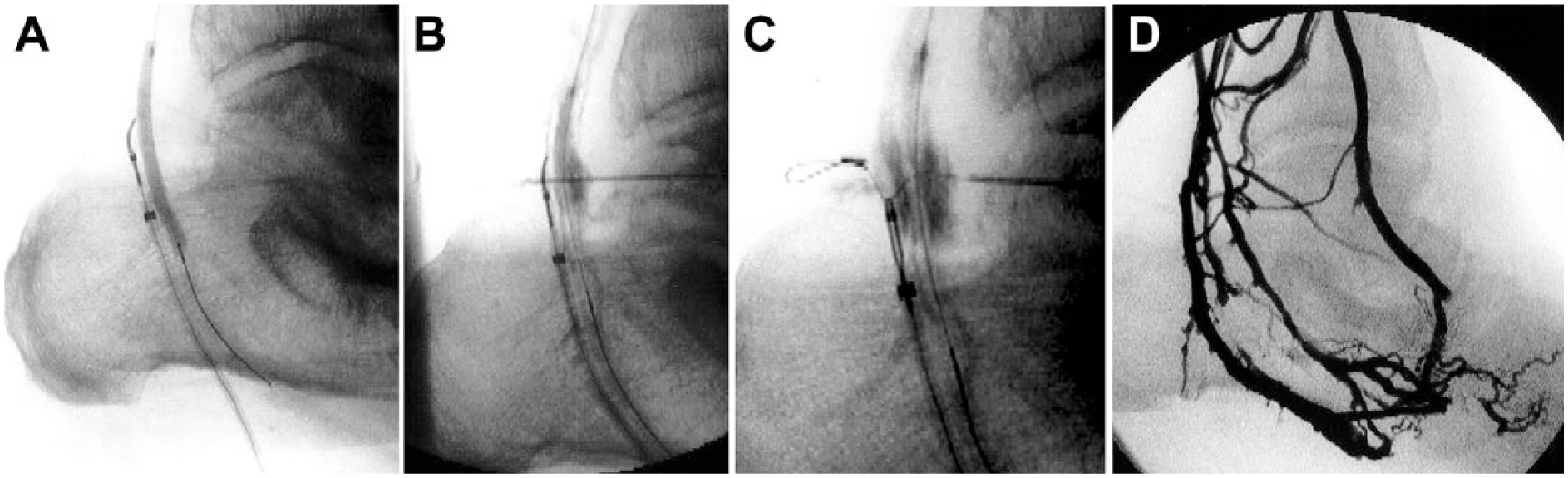
Intraoperative fluoroscopic images of the venous arterialization simplified technique 2. (A) The venous snare loop is positioned posterior to the arterial balloon catheter in the lateral projection. (B) A 22-G needle is advanced percutaneously, crossing through both the balloon catheter and the snare loop. (C) A Glidewire is advanced and the snare loop closed and retrieved. (D) Angiogram of the venous arterialization.
Once the AVF is established, the percutaneous venous arterialization procedure is completed following the method previously reported by Gandini et al. 2 To confirm adequate venous runoff of the AVF, 2 mL of contrast medium are injected through the balloon catheter. If necessary, balloon angioplasty of the lateral plantar vein and the deep venous arch is performed with a long 4×150-mm balloon catheter (Armada 14; Abbott Vascular). Once the procedure is completed, hemostasis at the distal puncture sites is achieved by 5 to 10 minutes of manual compression.
Clinical Experience
To October 2018, 5 diabetic patients (median age 72 years; 4 men) with high risk of amputation based on the Society for Vascular Surgery WIfI classification 4 were treated with the described maneuvers. All patients presented with occlusion of the tibial vessels and poor/absent foot arteries. They were selected for this strategy when the standard arterial recanalization procedure had been unsuccessfully attempted several times (average of 15 minutes of fluoroscopy). The AVF was created uneventfully in all cases (4 distal posterior tibial–plantar and 1 pedal arteries). In 1 case, however, the entire venous arterialization procedure could not be completed due to inability to cross a remaining distal valve combined with severe intraoperative deterioration of the patient’s condition. Mean fluoroscopy time was ~70 minutes.
No major complications were observed, and a completion duplex ultrasound assessment before hospital discharge routinely performed in all patients showed no evidence of vessel wall injury or leakage at the AV crossover point. All the revascularized subjects underwent debridement or minor amputation of one or more toes and were discharged on anticoagulation and single antiplatelet therapy for at least 3 to 6 months. One subject had impaired lower limb perfusion 4 weeks after revascularization. Arterial balloon angioplasty and coil embolization of the venous return to the heart to redirect blood distally was performed, with dramatic improvement of the foot perfusion.
Three of the 4 successfully treated patients achieved complete wound healing and resolution of rest pain (with patent AVF) over an average of 20±4 weeks. The remaining patient (admitted with extensive heel gangrene and osteomyelitis) underwent BTK amputation 5 weeks after the procedure due to progressive sepsis despite a patent AVF and the presence of emerging granulation tissue. No patients died during the mean 6-month follow-up.
Discussion
If a chronically occluded BTK/BTA artery cannot be recanalized or in the presence of a “desert foot,” percutaneous venous arterialization has proven to be a bailout strategy for limb salvage. The first description of a totally percutaneous venous arterialization was reported by Kum et al. 3 The authors designed a dedicated device based on an ultrasound-guided puncture to establish the AV communication. Despite an outstanding 100% technical success rate, the high cost and limited availability of the Limflow system has prohibited its widespread use. The reimbursement is related not only to the device itself but also includes the crossover stent, the extension covered stents, and the antegrade valvulotome. The main advantage of the described homemade device compared with the Limflow system is its universal availability, since almost all of the required materials (22-G needle, 0.014/0.018-inch guidewires, 4-F support catheter, and a 0.014-inch balloon catheter) are already on the table in a standard BTK recanalization procedure. The extra cost of our procedure is mainly related to the snare kit, the distal venous access, and occasionally, the balloon catheter for the venous segment if needed.
The distal venous access was usually achieved under ultrasound-guided puncture. However, the anatomic disposition of the tibial vessels around the ankle (double veins with the arteries lying in between) may allow direct puncture of the vein using arterial wall calcification or an arterial guidewire as a landmark. Moreover, the snare cost can also be minimized by using a homemade snare with a looped 0.014-inch guidewire. 5 In our early experience, the cases were performed with 2 operators, but the technique could easily be accomplished by a single operator assisted by the scrub nurse.
Two essential aspects seem to improve results in venous arterialization: a more distal location of the AVF and disruption of the valves in the vein distal to the site of the anastomosis.6,7 In our maneuver (as in the method described by Gandini et al 2 ), a more distal anastomosis in the vein reduces the chance of encountering valves that might obstruct blood flow (the last valve is generally located halfway to the foot 8 ). Therefore, the need to use stents to sort out valve destruction can be overlooked. In case of flow-limiting residual valve–related stenosis, focal 3.5×10-mm cutting balloon angioplasty (Boston Scientific Corporation, Marlborough, MA, USA) could be performed.
The increased profile and stiffness of the ultrasound-emitting arterial catheter with an embedded hollow crossing needle of the 7-F Limflow system may be a downside when dealing with small diameter, tortuous, or calcified vessels, especially in BTA arteries. In fact, in Kum’s study, 3 the AV communications were usually performed in the upper calf; no BTA AVFs were reported (4 posterior tibial, 2 anterior tibial, and 1 popliteal).
Although our technique has not been tested in an upper calf tibial vessel, it seems reasonable to assume that following AVF creation with the snare and balloon maneuver in such a proximal location, the antegrade valvulotome and the crossover/extension stents of the Limflow system would be of help to ensure valve destruction and to complete the arterialization procedure.
Gandini et al 2 recently described an inexpensive technique for percutaneous venous arterialization by pointing the tip of a guidewire opposite to the arterial wall calcification. The maneuver is based on the anatomic disposition of the double vein neighboring the plantar arteries. However, in their “blind technique,” up to 20% of the procedures could not be accomplished due to unsuccessful venous entry. Inability to locate the vein and adequately steer the catheter and the wire toward it may be the potential reasons behind the failures. Heavily calcified arteries can also be challenging to perforate (even from inside to outside). With our maneuver, the needle penetration power is substantially increased compared with the above-described methods. If needed, the buddy needle technique 9 may be helpful to facilitate puncture of heavily calcified tibial vessels by fixing the artery with complementary needles. Both techniques may be used together if needed.
Among the 3 principles of venous arterialization (crossing, valve destruction distally, and maintaining flow to achieve limb salvage), the novelty of our method lies in the AVF formation stage, since the other 2 principles were accomplished according to the formerly reported percutaneous venous arterialization methods.2,3 The reasoning behind the snare and balloon maneuver is that it gives guidance and allows the operator to precisely control the level of the AVF by adjusting the location of both elements (mimicking the gun-sight approach technique in transjugular intrahepatic transcaval portosystemic shunt 10 ) and therefore enhancing the chance of successful access. In our early experience, once the operator gets familiar with the technique, the access is generally achieved on a “getting it right the first time” basis. Alternatively, using the same principles as the dual bull’s-eye technique, 11 the arterial angioplasty balloon could be replaced in both VAST 1 and VAST 2 by a second snare loop (Figure 5).
Intraoperative fluoroscopic images of the “double snare” venous arterialization simplified technique in a case with the vein positioned posterior to the artery. (A) The snares are aligned and the best fluoroscopic projection is obtained such that both snares overlap. (B) Once the needle has crossed through both snares, a guidewire is advanced; the venous snare loop is closed and retrieved. (C) The arterial snare loop is gently retrieved and a support catheter introduced through the venous sheath into the artery, gaining the arteriovenous communication. (D) Angiogram of the venous arterialization.
The possibility of embolization of balloon material during balloon puncture has been weighed. Given the low profile of the 22-G needle, the chances of encountering such a complication should not be different from the chances observed when a sharp calcified plaque punctures an angioplasty balloon during inflation.
The described maneuvers are quite simple and reproducible, and the time taken to create the AV communication does not seem to be longer than other previously described techniques. The technique can be easily learned by operators (with previous experience in retrograde tibial vessel punctures) who would be deemed proficient to perform it after practice on a basic plastic tube model and with an assistant for the first “live” procedure.
Obvious slight increases in screening time and radiation dose are observed due to the manipulation of the needle/wire under fluoroscopy control. The operators should take care to avoid as much radiation as possible by using short exposure times and appropriate shielding.
Conclusion
The described maneuvers may be a useful option for creating a percutaneous AVF during a venous arterialization procedure in no-option CLI patients. Larger series with follow-up examinations are required to confirm the safety and effectiveness of this technique.
Footnotes
Acknowledgements
The authors thank Luis M. Palena (Policlinico Abano Terme, Italy) and Marc Sirvent (Hospital Germans Trias i Pujol, Spain) for their inspiring support in the development of the technique.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.