
Abstract
Keywords
Introduction
Type II endoleak (EII) is the most commonly occurring endoleak; nearly one-fourth of patients will develop an EII after endovascular aneurysm repair (EVAR). 1 The risk factors that are consistently associated with EII include age, smoking, patent inferior mesenteric artery (IMA), maximum aneurysm diameter, and number of patent lumbar arteries (LAs). 2 Moreover, a persistent EII with sac enlargement can lead to new type I or III endoleak and EVAR-related morbidity, with potential risk of rupture. 3 Treatment of an EII includes embolization of the IMA or lumbar arteries with coils or glue, direct translumbar injection of the aneurysm sac, transcaval embolization, or laparoscopic ligation of the IMA and lumbar arteries. 4 However, these interventions are not always successful, and some sacs continue to expand despite repeated reinterventions. 5 Thus, effective treatment of EIIs remains challenging.
Since sealing EIIs can be technically difficult, several preventive methods have been implemented to reduce the incidence of this complication. Preoperative coil embolization of side branches has been an effective option to reduce EIIs and increase shrinkage of the aneurysm sac.6,7 Moreover, intraoperative sac embolization during EVAR has been performed to decrease the EII and reintervention rates,8,9 but no systematic review has investigated this topic. Hence, this analysis sought to determine if these embolization techniques are safe and more effective in preventing EIIs as compared with no embolization.
Materials and Methods
Search Strategy and Selection Criteria
In accord with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, 10 MEDLINE and EMBASE were searched on December 31, 2018, using relevant terms (embolization, type II endoleak or type 2 endoleak, endovascular, and aneurysm) to identify randomized trials and comparative observational studies reporting preoperative embolization of side branches (IMA and LAs) or intraoperative aneurysm sac embolization during EVAR.
After removing duplicate studies, the authors independently reviewed the titles and abstracts of the remaining articles to determine eligibility. Abstracts, case reports, case series, commentaries, technical notes, and reviews were eliminated, as were articles without full text, not in English, and not on EII. Full-text versions of the remaining articles were reviewed for the outcomes of interest: EII rate, reintervention rate for EII, types I and III endoleaks, and complication rates. The reference lists of the included papers were searched manually to identify additional publications. For duplicate data, the most recent or most comprehensive paper was included. The authors independently undertook quality scoring of included studies using the Newcastle-Ottawa score. 11
Selected Studies
The search identified 898 articles of potential interest (Figure 1); another 6 were found in a search of reference lists. After eliminating ineligible/irrelevant articles, 125 full-text articles were reviewed; 17 studies12 –28 published between 2002 and 2018 encompassing 2084 patients were ultimately selected for inclusion in the meta-analysis.
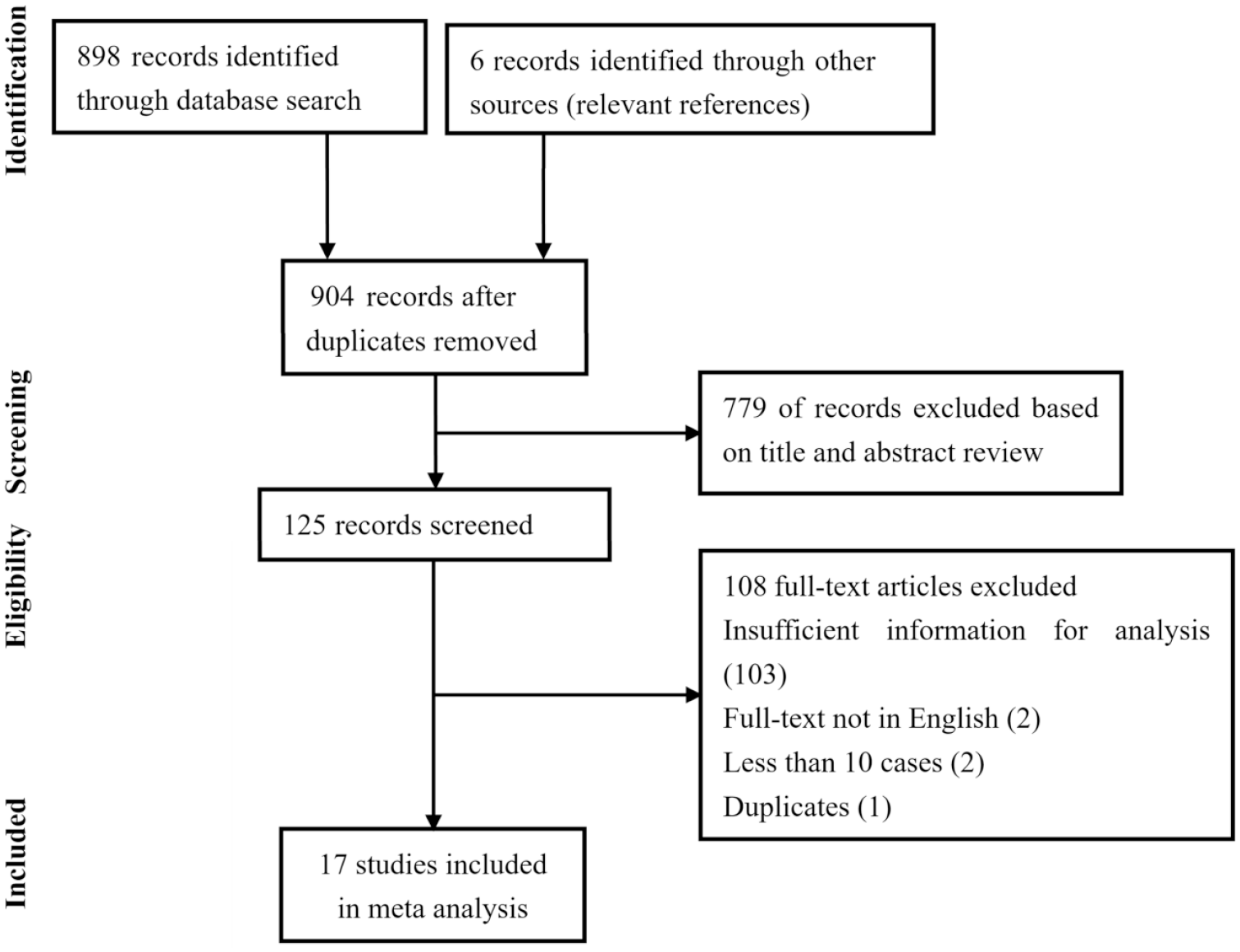
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow chart for the review.
Data Extraction
Using a predefined data extraction form, the authors independently extracted the following data from text, tables, and/or figures (wherever possible): first author, publication date, study design, patient population and subgroup sizes, EII rate, criteria for embolization, embolic materials, procedure time, fluoroscopy time, contrast use, technical success, surveillance mode, any complication related to the embolization procedure, incidence of types I/III endoleaks, reintervention criteria, reintervention rate, and follow-up duration. If the articles used for data collection did not present the relevant outcomes in absolute numbers or percentages, the authors of these articles were contacted to obtain these data. Any discrepancies were resolved by discussion between the authors.
Statistical Analysis
Heterogeneity was assessed using the I 2 statistic, with cutoff values of 25%, 50%, and 75% representing low, moderate, and high heterogeneity, respectively. If no heterogeneity was found, a fixed effects model based on the Mantel-Haenszel estimator was used. Otherwise, a random effects model based on the DerSimonian-Laird estimator was employed. Outcomes were expressed as the odds ratios (ORs) with the 95% confidence intervals and are presented as forest plots. Publication bias was assessed by applying the Horbold-Egger’s test. A sensitivity analysis was performed comparing routine embolization with selected use in high-risk patients. A 2-sided p<0.05 was considered statistically significant. Statistical analysis was performed using Review Manager (version 5.1.20; The Cochrane Collaboration; http://community.cochrane.org/help/tools-and-software/revman-5 )
Results
Characteristics of the included studies comparing sac or branch embolization to no embolization are shown in Table 1. Only 1 randomized trial 16 was among the 17 studies in the analysis. The size of the studies varied between 24 and 404 participants, and the follow-up duration ranged from 1 to 44 months. Seven studies12–18 provided data on 897 EVAR patients with abdominal aortic aneurysm (AAA) undergoing intraoperative aneurysm sac embolization vs no embolization. Ten studies19 –28 provided relevant outcome data for 1187 subjects with AAA who underwent pre-EVAR embolization of side branches or no embolization; among these, 5 studies19–23 provided outcomes for embolization of the IMA and LAs; the other 5 studies24–28 reported outcomes for IMA embolization only. All studies showed high quality (Table 2); however, most lacked points for comparability. No evidence of publication bias was found.
Characteristics of the Included Studies.
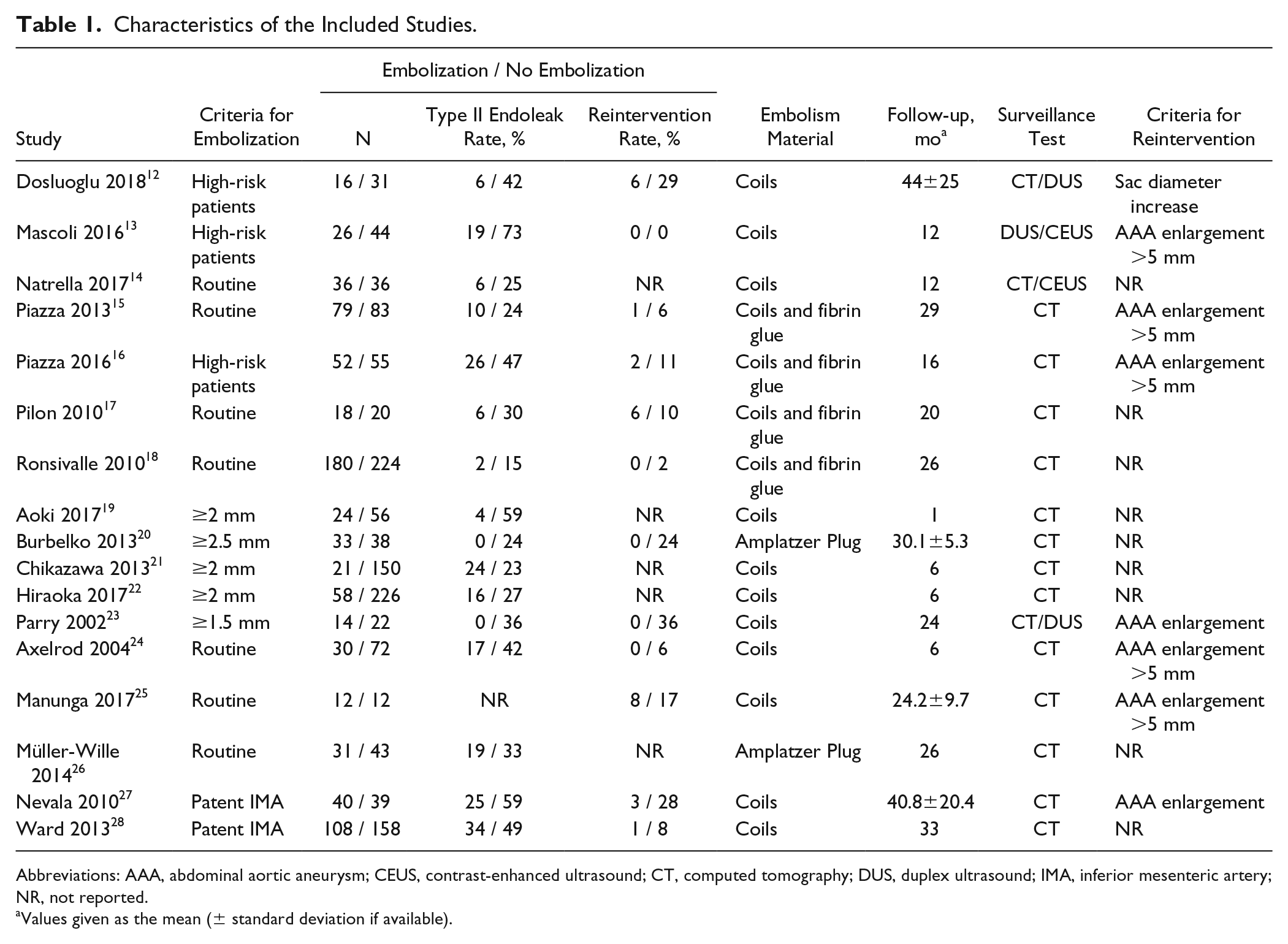
Abbreviations: AAA, abdominal aortic aneurysm; CEUS, contrast-enhanced ultrasound; CT, computed tomography; DUS, duplex ultrasound; IMA, inferior mesenteric artery; NR, not reported.
Values given as the mean (± standard deviation if available).
The Quality Assessment of Included Studies Based on the Newcastle-Ottawa Scale.
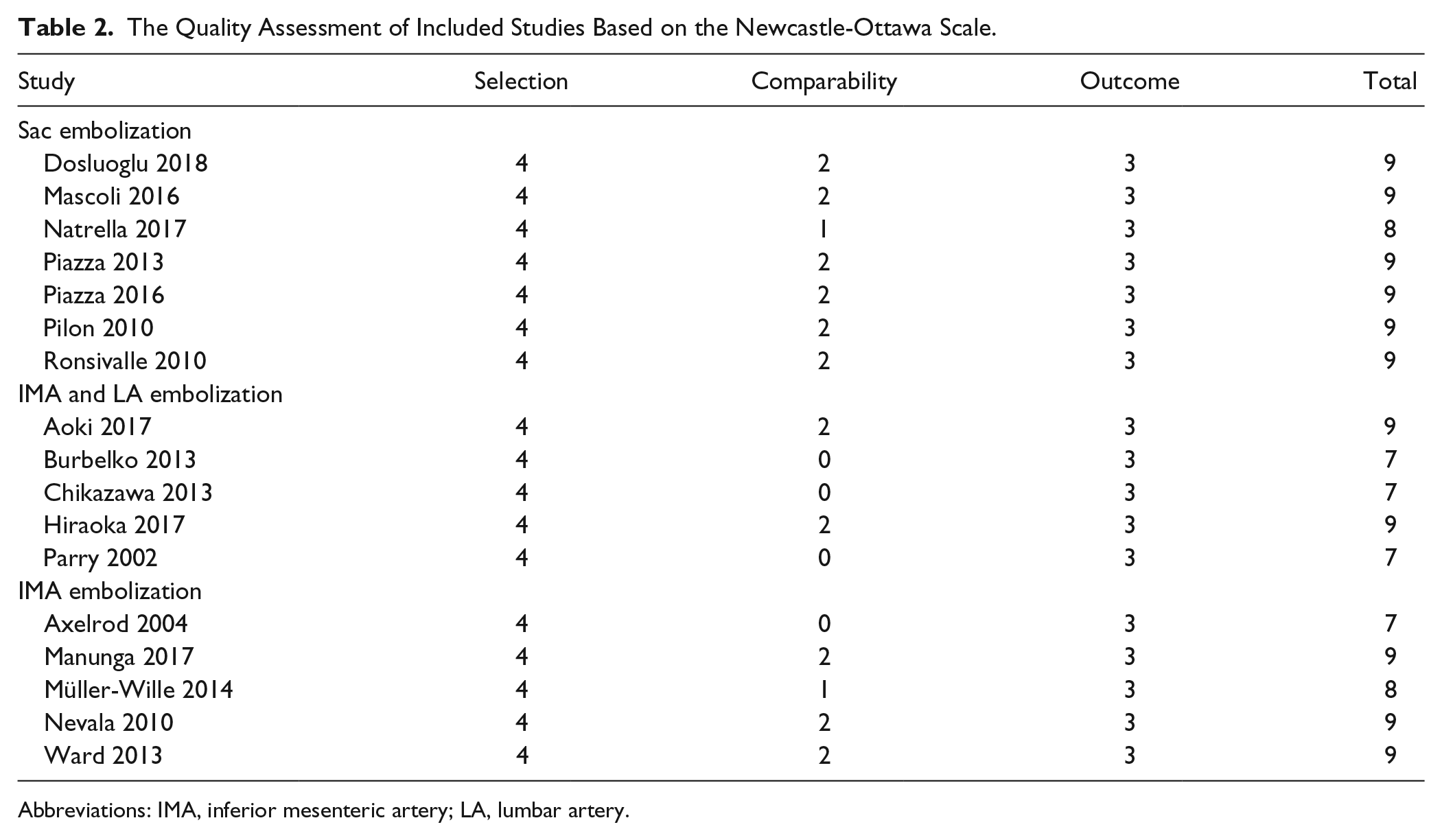
Abbreviations: IMA, inferior mesenteric artery; LA, lumbar artery.
Sac Embolization
Of 6 studies12–17 reporting technical success for the sac embolization technique, the success rate was 99% (224/226). Meta-analysis of all 7 articles12–18 reporting on sac embolization showed a significantly lower EII rate than the no embolization group (OR 0.21, 95% CI 0.13 to 0.34, p<0.001; Figure 2A). Heterogeneity of the studies was low (I 2 =13%). Six studies,12,13,15–18 which included 825 procedures, reported the reintervention rate for EII, which was significantly lower in the sac embolization group as well (OR 0.15, 95% CI 0.07 to 0.33; p<0.001; Figure 2B), with no heterogeneity (I 2 =0%). Three studies12,14,18 reported the types I/III endoleak rates; no significant difference was found (OR 0.57, 95% CI 0.23 to 1.37, p=0.21; Figure 3A), nor was there any heterogeneity among the studies (I 2 =0%). Furthermore, no significant difference was found in the incidence of complications between the groups in 6 studies12–17 reporting this outcome (OR 1.22, 95% CI 0.32 to 4.70, p=0.77; I 2 =0%; Figure 3B).
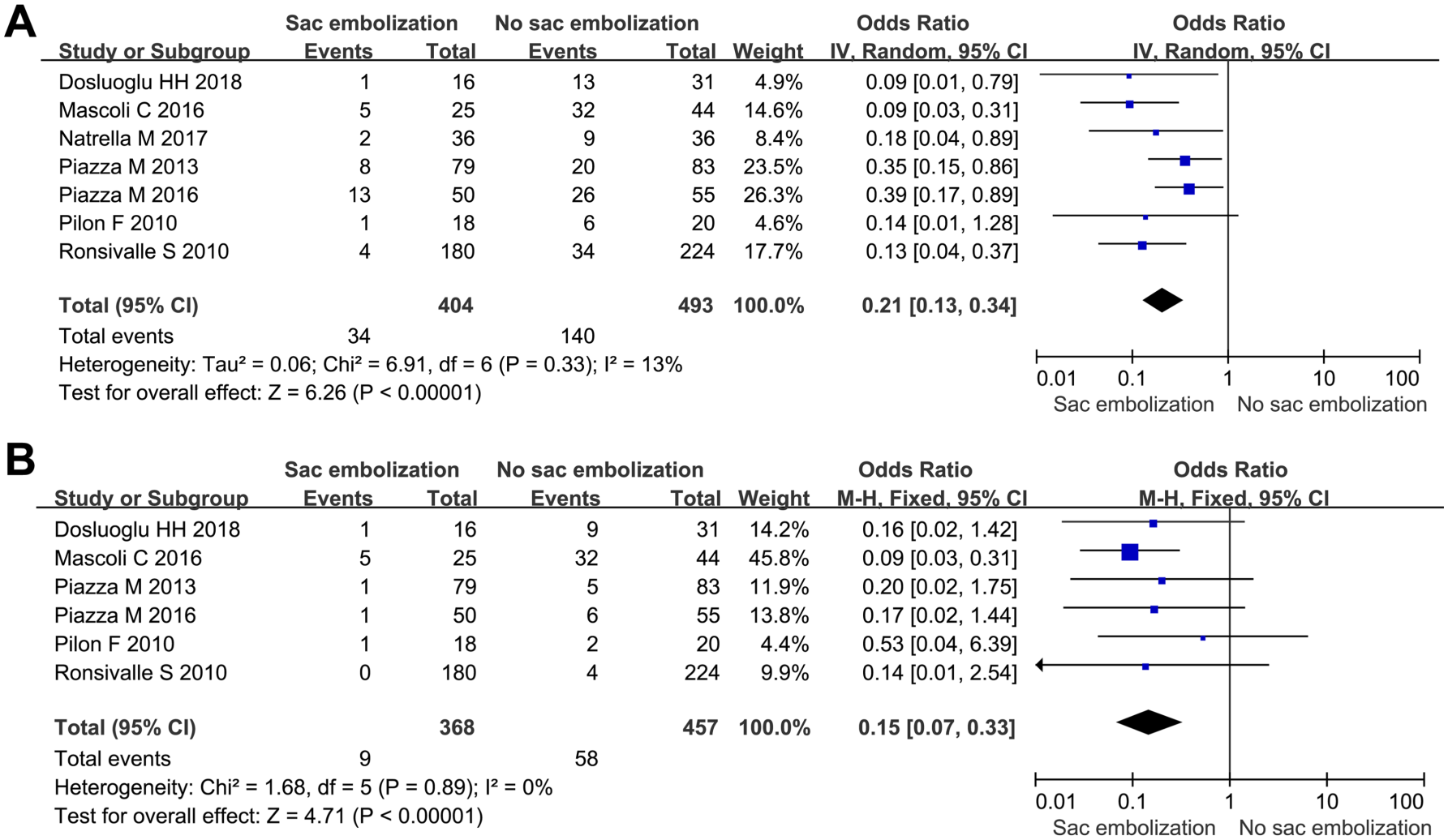
Forest plots comparing the type II endoleak rates between groups with (A) sac embolization vs no embolization and (B) the reintervention rate for type II endoleak. CI, confidence interval; IV, inverse variance; M-H, Mantel-Haenszel.
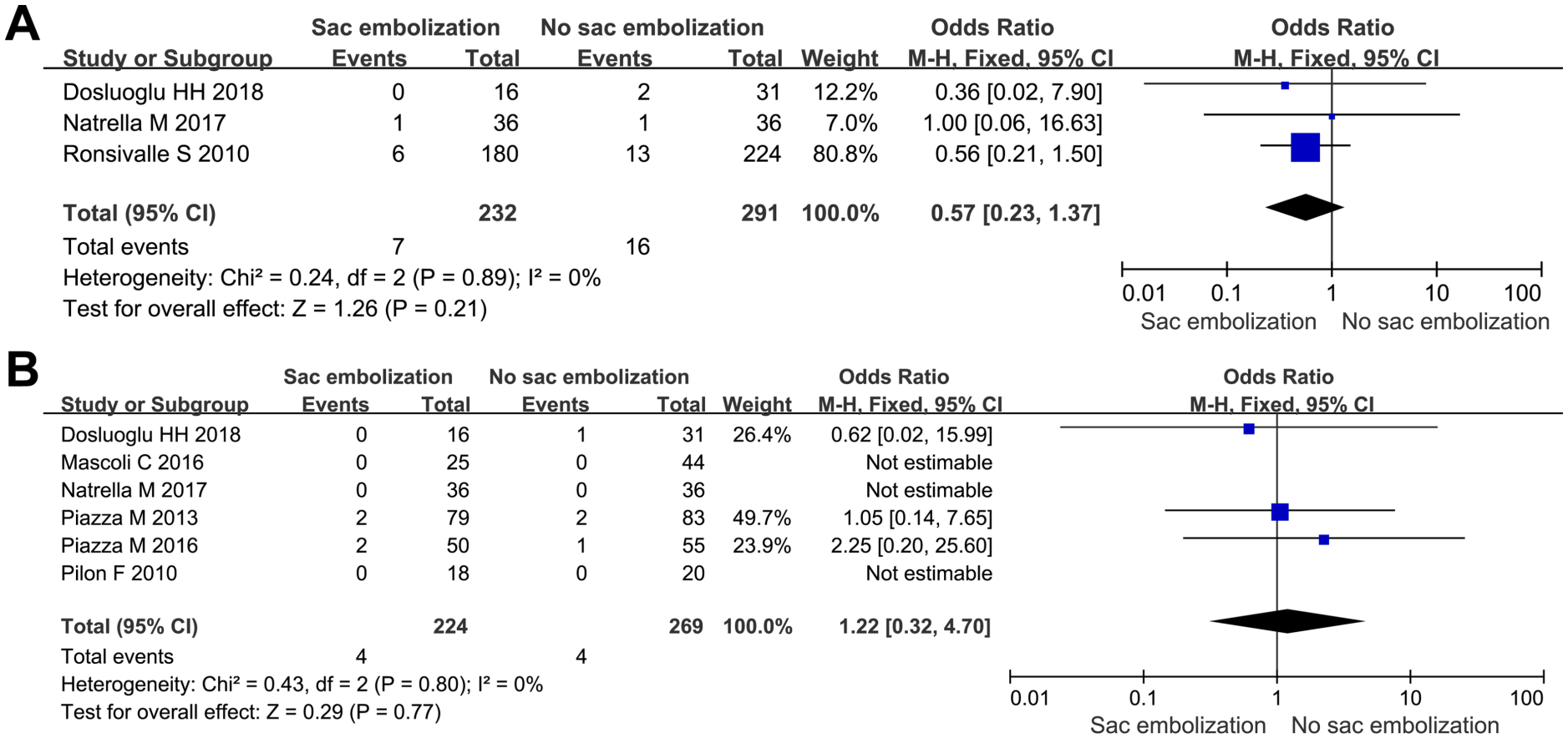
Forest plots comparing (A) the types I/III endoleak rates and (B) complication rates between groups with sac embolization vs no embolization. CI, confidence interval; M-H, Mantel-Haenszel.
A sensitivity analysis that included only studies that applied sac embolization in patients at high anatomical risk for EIIs resulted in a reduced incidence of EII (OR 0.18, 95% CI 0.06 to 0.54, p<0.001) and reintervention for EII (OR 0.12, 95% CI 0.05 to 0.31, p<0.001).
Side Branch Embolization
Among the 5 studies24–28 reporting outcomes for IMA embolization, the technical success was 99% (221/223) vs 94% (149/159) in the 5 studies19–23 involving embolization of both the IMA and LAs.
The pooled analysis of the 9 studies19–24,26–28 reporting the EII rate after side branch embolization found a lower incidence of EII with preoperative branch embolization (OR 0.35, 95% CI 0.21 to 0.60, p<0.001; Figure 4A). Moreover, subgroup analysis based on target arteries showed that embolization of the IMA and LAs (OR 0.21, 95% CI 0.06 to 0.77, p=0.02) or of only the IMA (OR 0.43, 95% CI 0.29 to 0.63, p<0.001) had lower EII rates than patients without embolization.
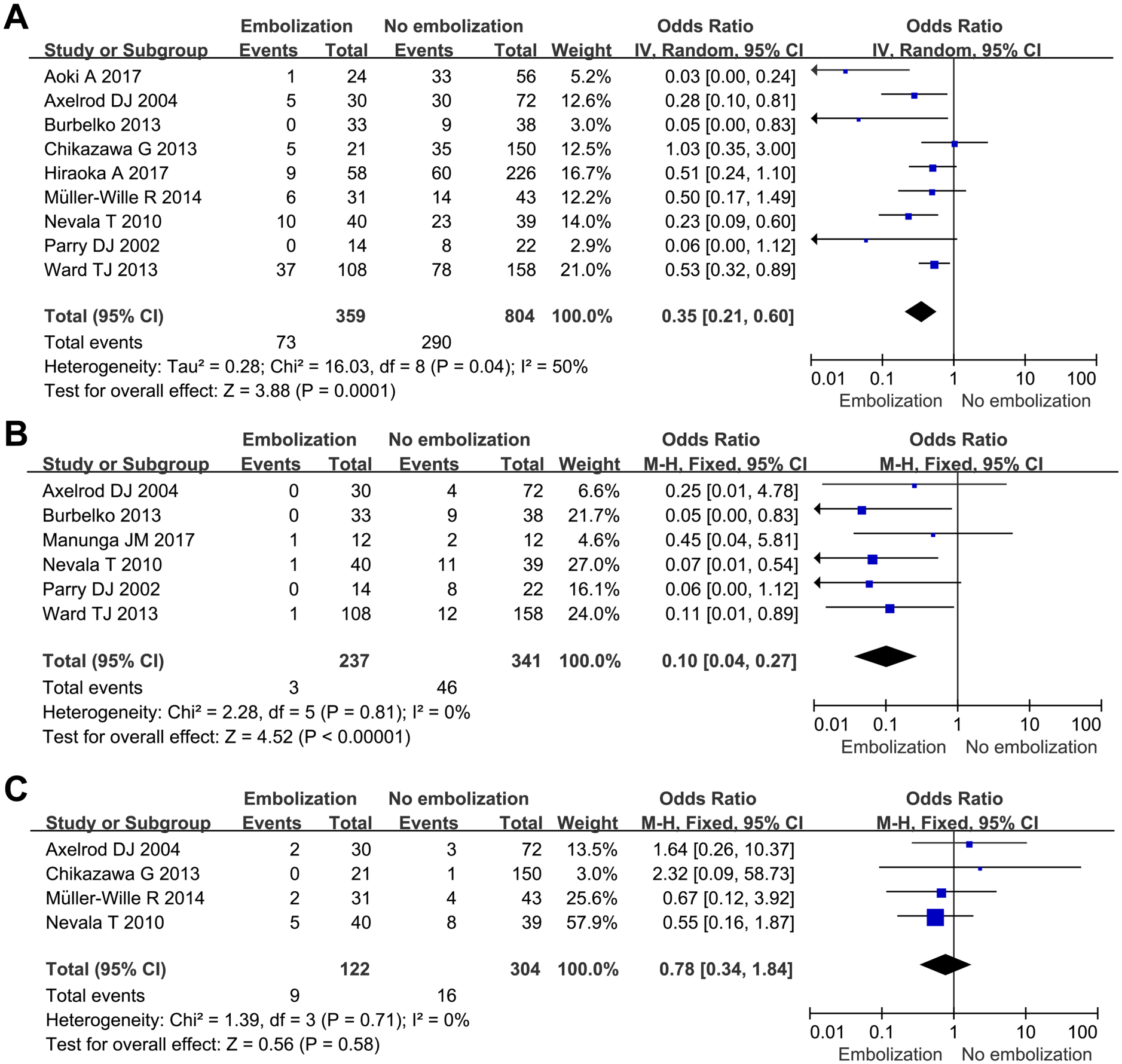
Forest plots comparing the type II endoleak rates between groups with (A) side branch embolization vs no embolization, (B) the reintervention rate for type II endoleak, and (C) the incidence of types I/III endoleak. CI, confidence interval; IV, inverse variance; M-H, Mantel-Haenszel.
Six studies20,23–25,27,28 assessed the reintervention rate for EII, which was found to be significantly lower in the side branch embolization group (OR 0.10, 95% CI 0.04 to 0.27, p<0.001; I 2 =0%; Figure 4B). Four studies21,24,27,28 reported the types I/III endoleak rates, with no significant difference between the groups (OR 0.78, 95% CI 0.34 to 1.84, p=0.58; I 2 =0%; Figure 4C). Although 719,20,22,24–28 studies mentioned complications, only one reported a single procedure-related sequela, a fatal case of colon ischemia.
Discussion
Although EIIs are associated with low secondary reintervention rates, endovascular techniques, such as transarterial or translumbar embolization, are not always effective for persistent EIIs, and an optimal management strategy has not been established.29,30 Thus, EII prevention is vital to improve the outcomes of EVAR.
In the sac embolization technique, a 5-F catheter is advanced around the iliac limb into the sac after deployment of the stent-graft main body; coils and/or fibrin glue are then introduced through the catheter. 13 This analysis demonstrated that sac embolization is effective in preventing the development of EII and is associated with a decrease in reinterventions. Moreover, the sac embolization group in our study showed a similar incidence of complications vs the no embolization group, and there was no complication-related mortality. Additionally, the technical success rate was high. Thus, sac embolization is safe and effective in preventing EII-related complications during short- and midterm follow-up after EVAR. Nevertheless, this approach has not gained wide acceptance owing to concerns over increased procedure time, radiation dose, contrast volume, and cost. However, 2 studies have concluded that sac embolization would not prolong the procedure or increase radiation exposure or contrast use.12,16
Three12,13,16 of 7 studies on sac embolization applied the technique in patients with a high anatomical risk for EIIs, whereas nonselective sac embolization was reported in 4 studies.14,15,17,18 Definitions of high-risk patients were based on morphological details, 31 which varied in these studies. Piazza et al 16 conducted a randomized trial that defined high risk for EIIs as patent IMA (≥3 mm) or 3 pairs of patent LAs. Dosluoglu et al 12 identified high risk for EIIs as 4 or more patent LAs, patent IMA (≥3 mm), and a flow lumen diameter ≥30 mm. Mascoli et al 13 defined high risk for EIIs as 6 efferent patent vessels and/or a ≤40% thrombus volume of the total AAA volume. Of these 3 studies, only one compared the clinical outcomes in low- and high-risk patients who underwent sac embolization and high-risk patients who did not. 12 The results suggested that EII and reintervention rates were lower in low-risk patients than in high-risk patients who underwent sac embolization and high-risk patients who did not, thus, sac embolization seemed unnecessary in low-risk patients. However, further cost-effectiveness studies are needed to quantify the effect of different strategies on long-term outcomes.
After EVAR, many potential communications exist between the IMA and superior mesenteric artery via the marginal artery of Drummond or the arc of Riolan or between LAs and the iliac artery. 32 When these connections fail to thrombose and propagate, EIIs develop. This is the theoretical basis of side branch embolization for preventing EII. Aoki et al 19 found that the endoleak area of the IMA tends to be larger than for LAs in many patients. Thus, the IMA is an important contributor to EII. A systematic review investigating the mid- to long-term clinical outcomes of preoperative IMA embolization found it to be a protective measure against the development of EII and secondary interventions; the technique may also potentially lead to rapid aneurysm sac regression. 25 Hiraoka et al 22 stated that even if the IMA and LAs are embolized, 2 residual LAs (inflow and outflow) could take form because of sac enlargement owing to an EII. Our results showed that embolization of the IMA and LAs or embolization of only the IMA produced a significantly lower EII rate compared with no embolization. Additionally, the average success rate of preoperative IMA embolization only matched the success rate in trials that reported embolization of both the IMA and LAs. Considering the safety aspect, Ward et al 28 reported that a single patient succumbed to mesenteric ischemia as a result of an inability to form collateral vessels to the left colon after IMA embolization. These studies revealed that side branch embolization can be generally performed safely with high technical success; however, severe colon ischemia should be closely monitored.
Comparing the technical aspects of these 2 procedures, preoperative side branch embolization in 2 studies19,20 took 18 to 25 minutes with a mean 15 minutes of fluoroscopy, whereas sac embolization12–17 added a mean 7 to 18 minutes to the EVAR procedure and a mean 2 minutes of additional fluoroscopy.
Based on the current evidence, both sac embolization and side branch embolization are efficient and generally safe. Unfortunately, there is still no study directly comparing the clinical outcomes of these 2 procedures, though sac embolization seems to be easier to implement, saving the patient from an additional embolization session.
Limitations
First, the included studies varied in the criteria for a preventive procedure, the criteria for reintervention, and the follow-up duration. However, subgroup analyses attempted to mitigate the impact of these characteristics. Second, no previous study has concentrated on the direct comparison of sac embolization to side branch embolization, and an algorithm is lacking for the prevention of EII. Third, with the exception of one randomized trial, the studies were of open-label design, which might introduce bias. However, after assessing the methodological quality of the included studies, most of them exhibited low or medium risk of bias.
Conclusion
Sac embolization and side branch embolization are effective for preventing EIIs. Moreover, these techniques are generally safe and rarely cause postoperative morbidity, though side branch embolization requires a separate procedure. Based on the current body of evidence, sac embolization should be considered in high-risk patients because it is safe and effective in preventing EIIs. However, a randomized trial is needed to directly compare sac embolization with side branch embolization.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.