
Abstract
Keywords
Introduction
The use of endovascular therapy (EVT) for peripheral artery disease (PAD) has expanded rapidly because of the less invasive nature of the procedure compared with bypass surgery and continued improvements in interventional devices. 1 However, technical success is not always satisfactory in cases of infrainguinal chronic total occlusion (CTO), which remains a challenging lesion. 2 If antegrade transluminal or subintimal CTO crossing fails conventionally, reentry devices are often deployed; however, these devices fail to reach the distal true lumen in up to 35% of cases. 3
TruePath (Boston Scientific Corporation, Marlborough, MA, USA) is a unique device that facilitates antegrade crossing using a diamond-coated distal tip rotating at 13,000 rpm on a 0.018-inch guidewire with adjustable torque that permits distal tip adjustment up to 15°. The device is also equipped with an audiovisual feedback alarm that indicates high resistance at the device tip, which helps the operator avoid nonplaque areas and guides the tip to the distal true lumen.
The ReOpen study 4 reported that the TruePath device was safe and effective for facilitating crossing of CTOs resistant to conventional guidewire maneuvers. Banerjee et al 5 found that the successful lesion crossing rate was significantly lower using a primary wire catheter approach compared to a primary crossing device approach. Furthermore, several previous comparative studies were limited by operator experience and small samples sizes, so results may not necessarily reflect those in daily clinical practice.4,6,7
The application of intravascular ultrasound (IVUS) for EVT evaluation is also growing. 8 A previous report evaluating intraluminal wire crossing of CTOs with IVUS assessment found that the proportion of plaque crossings (relative to total route distance) may affect primary patency. 9 Therefore, this study employed IVUS to fully assess the crossing pathway of an established transluminal crossing device used for primary antegrade recanalization of infrainguinal CTOs.
Materials and Methods
Study Design
A prospective, multicenter, observational study was begun in July 2017 in 14 hospitals in Japan to enroll symptomatic patients with an infrainguinal CTO assigned to primary treatment with the TruePath reentry device with IVUS examination of the crossing pathway following recanalization. Patients with symptoms of PAD were screened using noninvasive tests to detect limb ischemia and the presence of CTOs. Inclusion criteria were (1) age >20 years, (2) infrainguinal PAD (Rutherford category 2–5) with CTO (in-stent included), (3) ABI <0.9 or lower limb ischemia confirmed by other modalities if >0.9, (4) eligibility for EVT after a trial of exercise and/or drug therapy, (5) agreement to participate in clinical follow-up at 6 and 12 months after the procedure, and (6) signed informed consent. Exclusion criteria were (1) age <20 years, (2) pregnancy, (3) bleeding diathesis or coagulation disorder, (4) acute arterial occlusion or occlusion attributable to nonatherosclerotic or inflammatory diseases, (5) life expectancy <1 year, and (6) severe dementia that precluded informed consent.
The study was conducted in accordance with the principles of the Declaration of Helsinki, and the study protocol was approved by the ethics committee at each participating hospital. The study was registered with the University Hospital Medical Information Network (UMIN) Clinical Trial Registry (no. UMIN000026977) according to the guidelines of the International Committee of Medical Journal Editors. Written informed consent was obtained from every patient.
Procedure
A 5- or 6-F guiding sheath was inserted into the common femoral artery via a contralateral or ipsilateral antegrade approach at the operator’s discretion. Five thousand units of heparin were injected through the sheath; the activated clotting time was thereafter maintained at >200 seconds. The choice of microcatheter was at the operator’s discretion, as was the guidance method for the primary use of the reentry device during antegrade recanalization (fluoroscopy alone, IVUS, and/or duplex ultrasonography). If the feedback alarm of the reentry device was activated, the operator recorded the vessel location using plain fluoroscopy to perform IVUS assessments after recanalization. If it was not possible to cross the CTO using the reentry device, a conventional guidewire (antegrade), a retrograde approach via the tibial or popliteal artery, or the Outback reentry catheter (Cordis Corporation, Santa Clara, CA, USA) was used.
If antegrade guidewire navigation was successful, IVUS images were recorded by auto or manual pullback at a constant speed of 10 mm/s through the target segment to analyze the guidewire crossing route. IVUS images were acquired using commercially available consoles and a phased-array 20-MHz transducer (Eagle Eye Platinum; Volcano Corp, Rancho Cordova, CA, USA) or 30-MHz (Opticross 18; Boston Scientific Corporation) or 40-MHz [Opticross or AltaView (Terumo, Tokyo, Japan)] imaging catheters. If the IVUS catheter did not cross the lesion, a 2-mm-diameter balloon was inflated in the vessel prior to IVUS recording.
Conventional balloon dilation was then performed with an appropriately sized angioplasty balloon. For cases with optimal dilation [no major (≥grade D) flow-limiting dissection or residual stenosis <50%], a drug-coated balloon (IN.PACT Admiral; Medtronic, Santa Rosa, CA, USA) was used starting in January 2018 when this device first became available in Japan. No directional or rotational atherectomy devices were used as they are unavailable in Japan.
If a suboptimal result was obtained (≥grade D flow-limiting dissection or residual stenosis ≥50%), a stent approximately 1 mm larger than the vessel diameter was implanted. The stenting strategy (spot or full-covered stenting) and the choice of bare nitinol stent [S.M.A.R.T (Cordis Corporation, a Cardinal Health company, Santa Clara, CA, USA); Innova (Boston Scientific Corporation); or LifeStent (Bard Peripheral Vascular, Tempe, AZ, USA)], drug-eluting stent (Zilver PTX; Cook Medical, Bloomington, IN, USA), or covered stent (Viabahn; Gore Medical, Flagstaff, AZ, USA) was at the operator’s discretion. After stenting, routine postdilation was performed to achieve better stent expansion and apposition. At the end of the endovascular procedure, additional IVUS images were captured to evaluate the final outcome and stent apposition.
Dual antiplatelet therapy (DAPT) was prescribed for at least 1 month after procedures involving conventional balloon angioplasty, bare stent implantation, or DCB angioplasty. Patients receiving a drug-eluting stent were advised to continue DAPT for at least 2 months based on the package insert instructions.
IVUS Analysis
All IVUS images were reviewed, and a quantitative IVUS analysis was performed by an independent experienced investigator blinded to the clinical and angiographic information. The IVUS parameters measured or calculated were the crossing route of CTOs (intraplaque, subintimal, or intramedial); proximal, distal, and minimum external elastic membrane (EEM) areas; the presence of superficial calcification; maximum calcification arc; the presence of calcified nodules; minimum and maximum lumen areas; stent eccentricity; and stent edge dissection. The proportion of the total CTO route within the plaque was calculated based on the number of IVUS frames showing the guidewire and IVUS transducer along the intraplaque route divided by the total number of IVUS frames showing the entire CTO route. Subintimal and intramedial routes were calculated in the same manner.
Definitions and Outcomes
The severity of calcification was assessed according to the Peripheral Arterial Calcium Scoring System (PACSS). 10 The angiographic morphology of CTOs (tapered/nontapered) at entry point and exit point was decided based on criteria from a previous study. 11 The IVUS parameters were measured according to a previous consensus. 12 Stent symmetry index was defined as the ratio of the minimum to maximum stent diameters. The wire passage route in CTOs was classified according to IVUS findings as intraplaque (inside the plaque), subintimal (between the plaque and tunica media), or intramedial (between the tunica media and adventitia). 13 Stent edge dissection was defined as a dissection <5 mm proximal or distal to the stent margin.
The outcome measures were complete success, assisted success, procedure- and device-related complications, and successful antegrade crossing route with IVUS assessment. Complete success was defined as the TruePath reentry device reaching the distal true lumen. Assisted success was defined as initial reentry device usage followed by conventional wire usage to reach the distal true lumen. Procedure- and device-related complications included puncture site events (pseudoaneurysm, arteriovenous fistula, and hematoma), clinical wire perforation (any perforation requiring treatment), dissection, and any prolonged hospitalization.
Patient Population
Between July 2017 and September 2018, 143 symptomatic patients (mean age 75±9 years; 101 men) with a CTO in 146 limbs were enrolled prospectively in this multicenter observational study. The baseline characteristics of the study population and the CTOs are summarized in Tables 1 and 2, respectively. One-third of the target limbs (52, 35%) had critical limb ischemia, and 15 (10%) had infrapopliteal lesions. The mean CTO length was 11.0±7.8 cm (range 1.5–30) by quantitative vascular analysis. The vast majority of the lesions (130, 89%) were de novo CTOs; 8 (5%) were in-stent occlusions. Seven (5%) limbs had a history of failed revascularization. The majority of lesions (92, 63%) had a proximal-end tapered stump. Severe calcification (PACSS grade 4) was observed in 35 (24%) lesions.
Characteristics of the 143 Patients and 146 Lesions in the Study. a
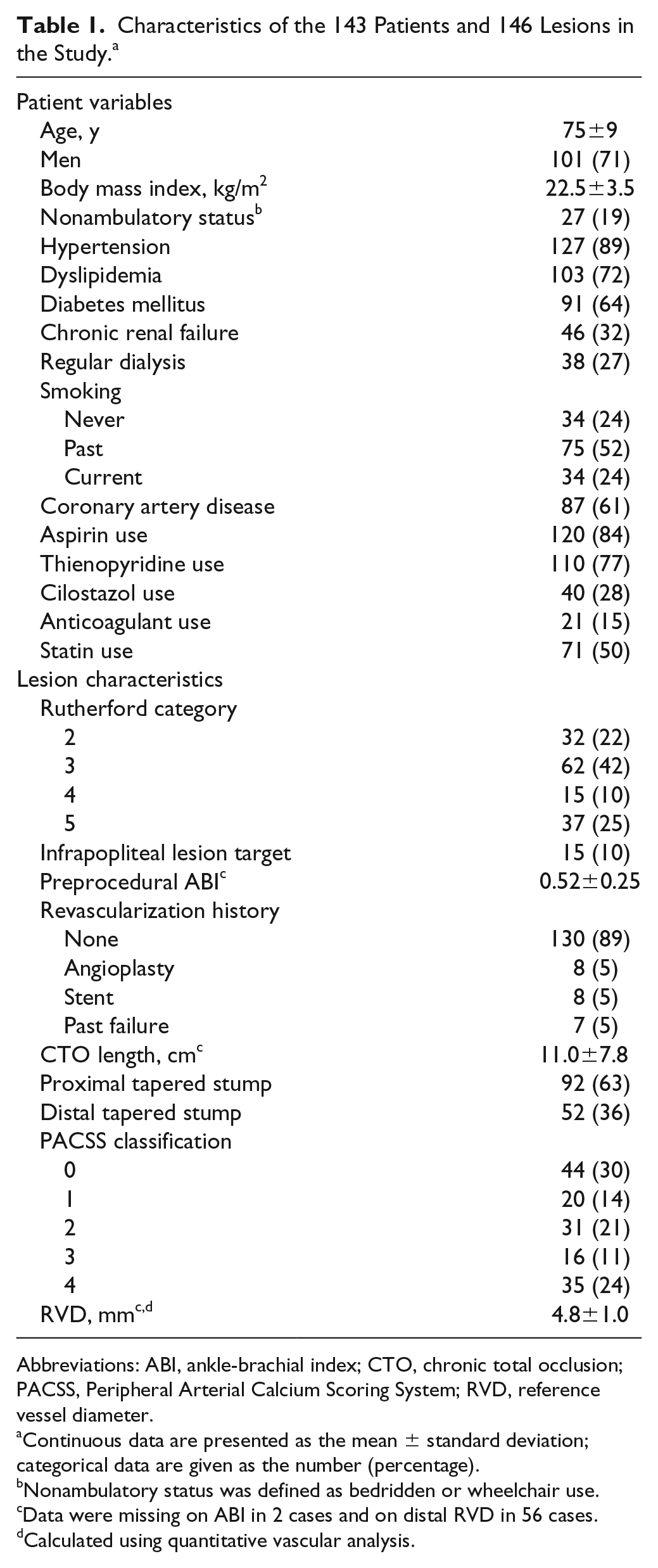
Abbreviations: ABI, ankle-brachial index; CTO, chronic total occlusion; PACSS, Peripheral Arterial Calcium Scoring System; RVD, reference vessel diameter.
Continuous data are presented as the mean ± standard deviation; categorical data are given as the number (percentage).
Nonambulatory status was defined as bedridden or wheelchair use.
Data were missing on ABI in 2 cases and on distal RVD in 56 cases.
Calculated using quantitative vascular analysis.
Details of the 146 Procedures Using the TruePath Reentry Device for Primary CTO Recanalization. a
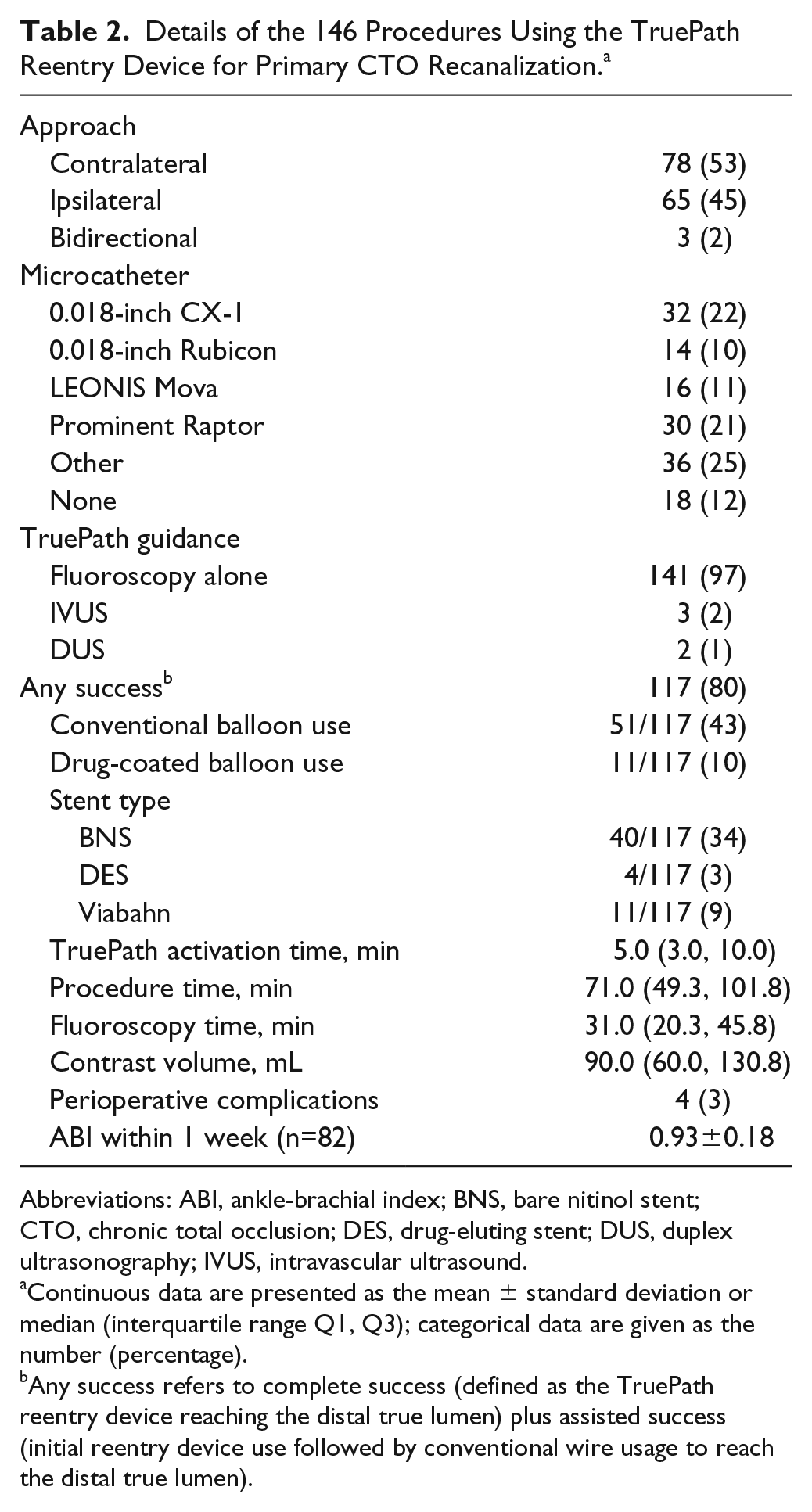
Abbreviations: ABI, ankle-brachial index; BNS, bare nitinol stent; CTO, chronic total occlusion; DES, drug-eluting stent; DUS, duplex ultrasonography; IVUS, intravascular ultrasound.
Continuous data are presented as the mean ± standard deviation or median (interquartile range Q1, Q3); categorical data are given as the number (percentage).
Any success refers to complete success (defined as the TruePath reentry device reaching the distal true lumen) plus assisted success (initial reentry device use followed by conventional wire usage to reach the distal true lumen).
Statistical Analysis
Continuous variables are presented as mean ± standard deviation, and discrete variables are presented as number (percentage) unless otherwise indicated. The 95% confidence interval (CI) for proportions was calculated using the Clopper-Pearson exact method. Risks of not achieving complete success (vs failure plus assisted success) and not achieving any success (vs failure) were calculated using binomial logistic regression models and expressed as the odds ratio (OR) with 95% CI. Sensitivity analyses for failure and assisted success individually vs complete success were conducted using multinomial logistic regression. The probability of complete success at a specific CTO length was assessed using the penalized cubic regression spline model with a logit link function. The threshold of statistical significance was a 2-tailed p<0.05. All statistical analyses were performed using R (version 3.1.0; R Development Core Team, Vienna, Austria).
Results
Complete success was achieved in 82 (56.2%) lesions (95% CI 47.7% to 64.4%), while any success (complete plus assisted) was documented in 117 (80.1%) lesions (95% CI 72.7% to 86.3%). Details of the EVT procedure are given in Table 2. EVT was performed mainly under fluoroscopic guidance using a microcatheter-supported TruePath reentry device. Stent implantation was required in 45 (38%) of the 117 successful cases; conventional balloons were used in 51 (43%) lesions and DCBs in 11 (10%). Four (3%) perioperative device-related complications were observed, including 2 puncture-site pseudoaneurysms, 1 distal embolization, and 1 wire perforation requiring treatment.
IVUS Findings in Successful Cases
Table 3 displays the proportional lengths of intraplaque, subintimal, and intramedial crossing (% of total) according to frame-by-frame IVUS assessment in successful cases. In completely successful cases, 95.3%±13.2% of the total crossing route was intraplaque compared with only 3.6%±10.2% subintimal and 1.2%±5.8% intramedial. Similarly, in cases with any success (complete plus assisted), 94.8%±14.4% of the route was intraplaque compared to only 4.2%±11.2% subintimal and 1.0%±5.4% intramedial. In 79.4% of cases achieving any success, the route was entirely intraplaque (95% CI 70.3% to 86.8%), and the route was entirely intraplaque in 80.6% of completely successful cases (95% CI 69.5% to 88.9%).
Proportion of Crossing Routes With IVUS Assessment. a
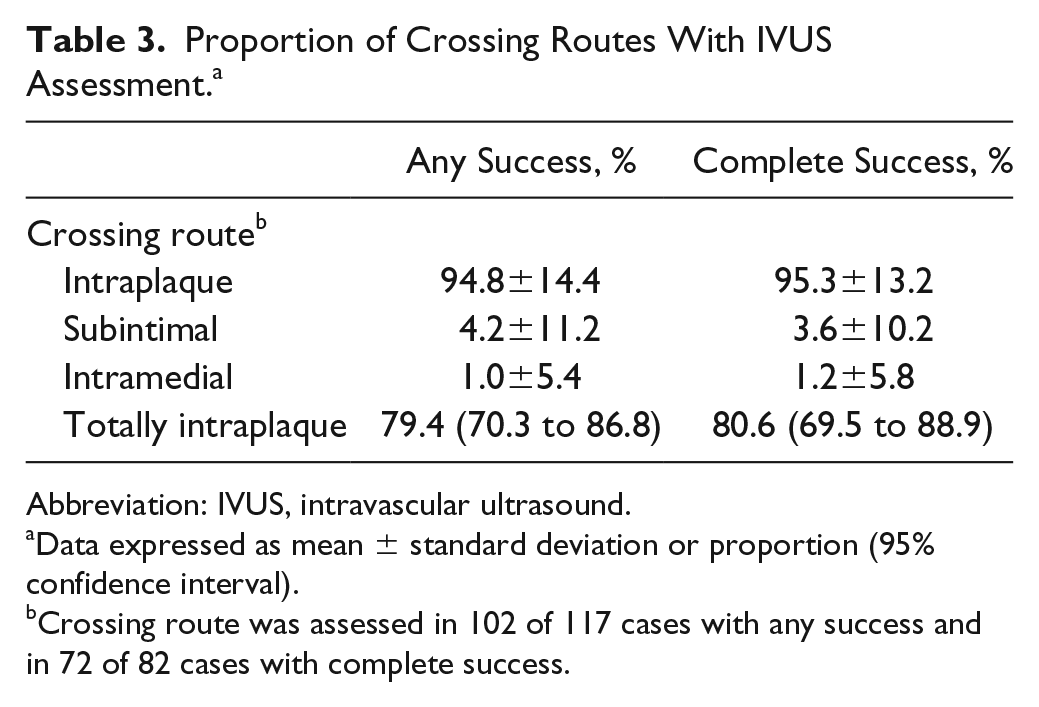
Abbreviation: IVUS, intravascular ultrasound.
Data expressed as mean ± standard deviation or proportion (95% confidence interval).
Crossing route was assessed in 102 of 117 cases with any success and in 72 of 82 cases with complete success.
In the 117 cases with successful antegrade crossing, superficial calcification was found in 46 (45%) cases, the mean maximum calcification angle was 222.0°±120.1°, and calcified nodules were present in 20 (20%) of 97 cases (Table 4). No stent edge dissection was detected. The TruePath reentry device crossed the CTO without feedback alarm activation in nearly half of the cases. The alarm rang mainly in subintimal locations.
IVUS Findings in the Successful Antegrade Crossings. a
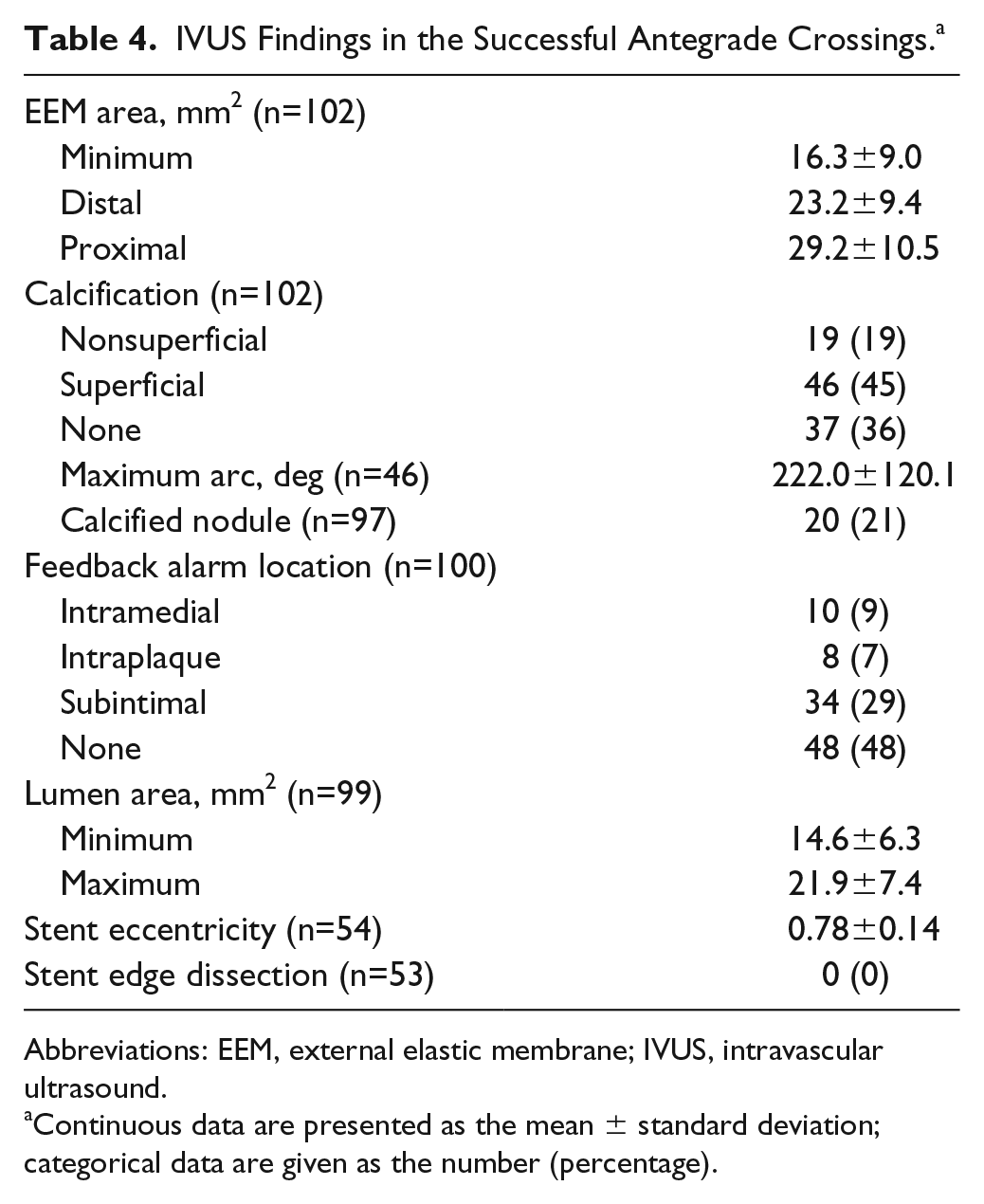
Abbreviations: EEM, external elastic membrane; IVUS, intravascular ultrasound.
Continuous data are presented as the mean ± standard deviation; categorical data are given as the number (percentage).
Association of Baseline Characteristics With Procedural Success (Table 5)
A long CTO lesion was a risk factor for not achieving complete success (OR 1.74, 95% CI 1.13 to 2.68 per 10-mm increase in occlusion length, p=0.012). In addition, a history of failed revascularization was a risk factor for not achieving any success (OR 6.08, 95% CI 1.28 to 28.9, p=0.023).
Associations of Baseline Characteristics With Procedural Success. a
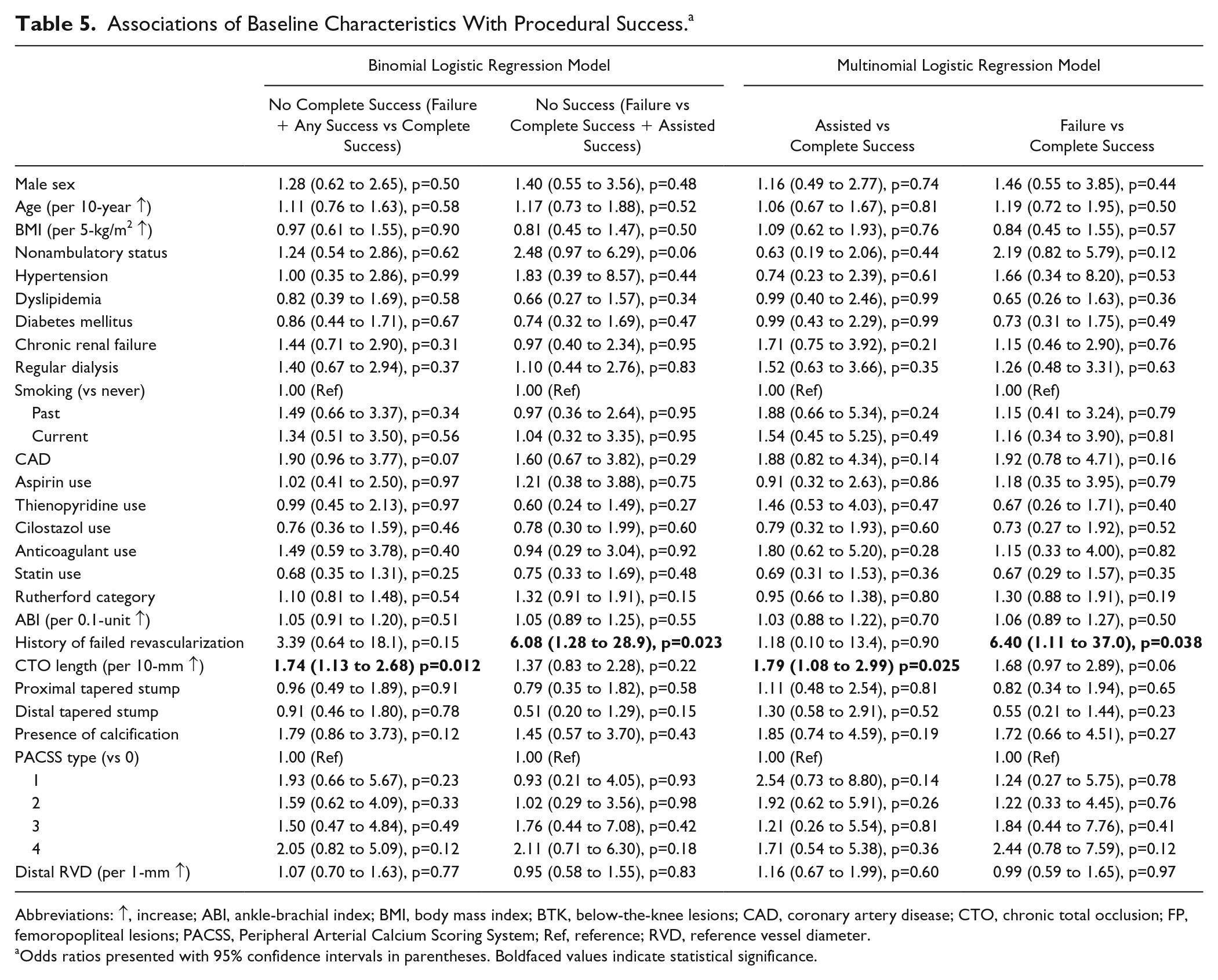
Abbreviations: ↑, increase; ABI, ankle-brachial index; BMI, body mass index; BTK, below-the-knee lesions; CAD, coronary artery disease; CTO, chronic total occlusion; FP, femoropopliteal lesions; PACSS, Peripheral Arterial Calcium Scoring System; Ref, reference; RVD, reference vessel diameter.
Odds ratios presented with 95% confidence intervals in parentheses. Boldfaced values indicate statistical significance.
For CTO length, a sensitivity analysis using the multinomial logistic regression model yielded an OR of 1.79 (95% CI 1.08 to 2.99, p=0.025) for assisted success vs complete success and an OR of 1.68 (95% CI 0.97 to 2.89, p=0.063) for failure vs complete success. For a history of failed revascularization, the corresponding values were OR 1.18 (95% 0.10 to 13.4, p=0.90) and OR 6.40 (95% CI 1.11 to 37.0, p=0.038). The spline model indicated that the proportion of complete success was almost linearly related to CTO length (Figure 1). Figure 2 illustrates the proportion of any success in subgroups with and without a history of failed revascularization.
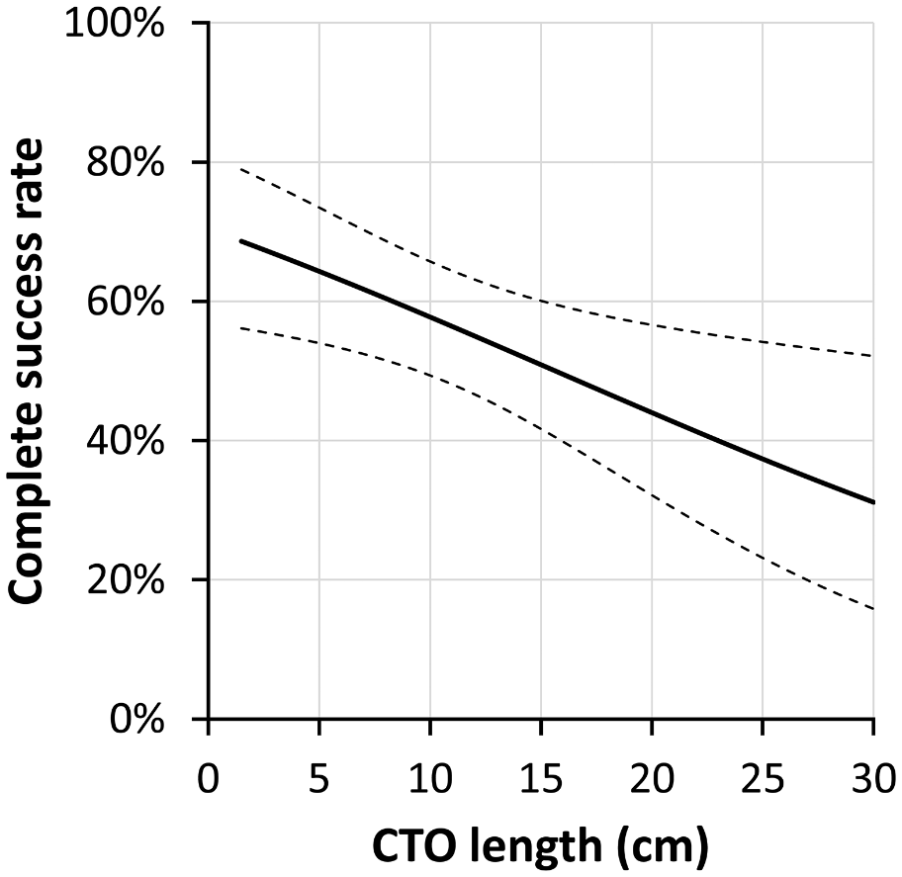
Association of chronic total occlusion (CTO) length and complete success rate. The bold solid line and thin dotted lines represent the probability of complete success at a specific CTO length and associated 95% confidence interval, respectively.
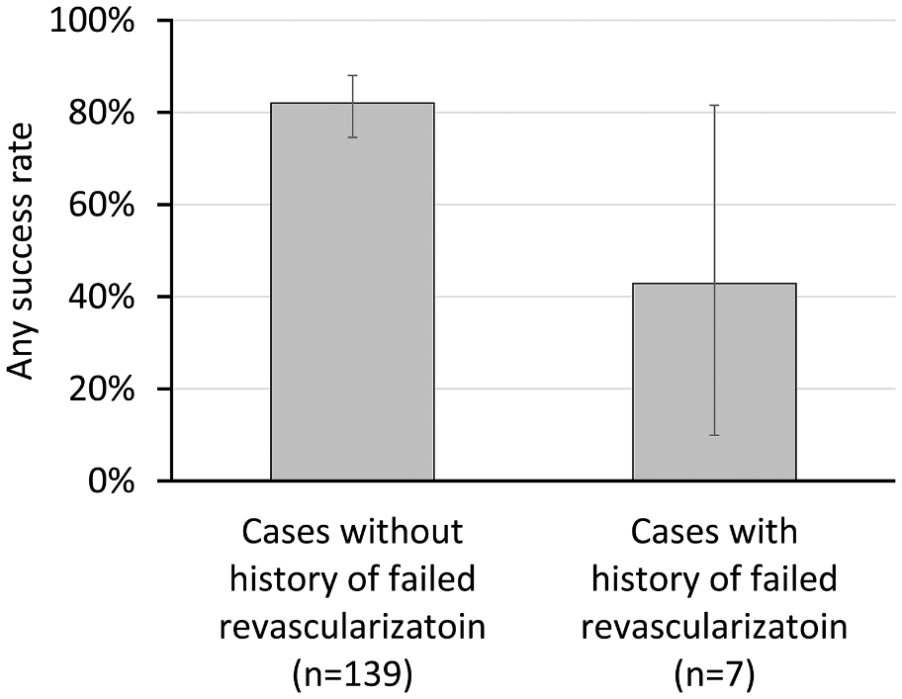
Comparison of the rate of any success in patients with vs without a history of failed revascularization. Error bars represent 95% confidence intervals.
Discussion
In this study, the majority of cases (89%) were intermediate-length de novo lesions, which reflects the routine clinical situation better than a previous study assessing the efficacy of secondary reentry device use, in which only 55% of cases were de novo lesions. 4 Although the TruePath reentry device proved relatively successful in recanalizing infrainguinal CTOs, the primary reentry device approach appears limited in some situations, such as especially long CTOs and patients with previous revascularization failure. For long femoropopliteal CTOs (mean lesion length 246±42 mm), a 0.035-inch looped subintimal wire was reported to achieve an antegrade success rate of 74% to 90%. 13 In the current study, the target CTO length was shorter, indicating the need for subintimal wire use. In addition, the route was almost entirely intraplaque in successful (complete or complete plus assisted) cases using the antegrade approach according to frame-by-frame IVUS assessment. In a study of cases with long occlusive length (mean of 177 mm), however, the intraplaque route accounted for only 73% of the total distance. 9
Nonetheless, even in cases with longer CTO length, the reentry device achieved a predominantly intraplaque route. One possible explanation is the inclusion of an alarm system, which rang mainly in subintimal locations according to IVUS assessment. A retrospective analysis from the XLPAD registry reported that a primary crossing device approach to CTOs provides significantly higher technical success with lower reintervention and amputation rates. 5 The proportion of total distance within the plaque may affect the final CTO patency. 9 Specifically, a primary crossing device approach with a high proportion of intraplaque crossing may improve patency and reduce the risk of reintervention. However, the aforementioned report was from a retrospective registry, 5 so additional follow-up of the present study cohort is required to verify whether the primary reentry device approach for CTOs improves patency, freedom from reintervention, and amputation rates.
In nearly half of the successful antegrade crossing cases, no alarm was activated, suggesting that the operator should subsequently proceed without changing the shape of the guidewire tip until or unless the alarm is activated. On the other hand, the distal tip of the reentry device is not tapered, so it may easily follow a previous wire route and be guided away from the intraplaque region. Therefore, a long CTO lesion and history of failed revascularization might be risk factors for not achieving complete or any success.
From previous registry data, initial simple guidewire use was a significantly less expensive procedure than initial use of the crossing device (p<0.001). 5 Although an experienced operator does not really need the reentry device for intermediate-length de novo CTOs, a reentry device might be valued by a less experienced operator from the viewpoint of getting decent results. In addition, the reentry device would not work well in adverse lesions (long CTOs and history of failed revascularization). However, this study had a single-arm design that did not compare primary reentry device use with an initial guidewire strategy for CTOs. A randomized controlled trial (RCT) would be needed to prove the advantage of primary reentry device use over the guidewire alone.
Although IVUS may contribute to EVT success, 8 it is not necessarily covered by medical insurance. In addition, high success rates have been reported only in some institutions, with more variable results in others.4,6,7 Therefore, it is difficult to apply these earlier findings to daily clinical practice. In the current prospective multicenter study, over 90% of the total route was intraplaque in successful crossing cases using the reentry device and IVUS. Therefore, the use of the TruePath reentry device for CTOs without IVUS may make more aggressive vessel preparation possible. Additional studies are required to assess the benefits of IVUS and to identify the remedial procedures needed if the reentry device is used without IVUS.
Limitations
First, this was a single-arm observational study, not an RCT comparing an initial reentry device strategy to an initial simple guidewire. Second, the mean CTO length was relatively short (11 cm), so selection bias may have influenced the results. Third, the accuracy of route proportion estimates may be affected by the manual pullback used for IVUS examination. Also, it was difficult to exactly match the location of the alarm activation with the same IVUS frame. Fourth, assessments of angiographic morphology (proximal and distal CTO type), PACSS grade, and IVUS findings were not evaluated by independent core laboratory review. Fifth, although the investigators perform EVT routinely as part of their daily practice, institutional differences in operator experience and procedures were not included in the analysis because it was limited in sample size. Finally, a cost-effectiveness analysis of the reentry device was not performed because of the relatively small number of cases and the single-arm study design. Therefore, further investigations, including RCTs, are needed to confirm the utility of the TruePath reentry device compared to conventional guidewire recanalization for CTOs.
Conclusion
The intraplaque route was the primary pathway taken by the TruePath reentry device as it crossed infrainguinal CTOs. Crossing rates were acceptable, with few device-related complications. However, CTO length and a history of revascularization failure decreased success, suggesting that the TruePath crossing device is most appropriate for intermediate-length de novo lesions.
Footnotes
Acknowledgements
The authors would like to acknowledge the study investigators and the catheterization laboratory medical staff. The authors also thank Enago ( www.enago.jp ) for the English language review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.