
Abstract
Keywords
Introduction
Advanced peripheral artery disease manifesting as chronic limb-threatening ischemia (CLTI) remains a challenging clinical problem, with 20% mortality and a 30% rate of major amputation at 1 year.1,2 With the increase in the endovascular first approach, alternative forms of access have been developed to expand the options for the delivery of peripheral devices. Described in 1990 by Iyer and colleagues, 3 retrograde tibial access is a revascularization option in selected patients. Since that time there have been several case reports and single-center series describing this technique.4–8 A prospective, nonrandomized, multicenter study reported outcomes only to 30 days. 9 Because the early success by pioneers and centers of excellence may not be replicated in real-world practice, this study analyzed the real-world use and outcomes of retrograde pedal access for peripheral vascular interventions (PVI) in patients with CLTI enrolled in a multicenter national quality improvement registry.
Materials and Methods
Study Design
This was a retrospective cohort study of prospectively collected data from the Vascular Quality Initiative (VQI) PVI Registry. The VQI is an Agency for Health Research and Quality–designated Patient Safety Organization that registers perioperative and 1-year follow-up data on vascular procedures to improve the quality of patient care across a spectrum of vascular procedures. Participants in the VQI PVI registry include vascular surgeons (53%), cardiologists (20%), interventional radiologists (17%), general surgeons (5%), and other (5%) specialists. Further information about the registry has been previously published. 10
The VQI PVI database was queried for all patients undergoing elective or urgent retrograde pedal access for PVI for CLTI, defined as ischemic rest pain or tissue loss, from October 2016 to September 2017. Infrainguinal interventions on the common femoral, superficial femoral, popliteal, tibial, and peroneal arteries were included. Interventions on the aorta and iliac arteries were excluded. Only percutaneous procedures were included with exclusion of concomitant bypass or femoral endarterectomy procedures. The study protocol followed the guidelines in the Declaration of Helsinki and was reviewed by the Institutional Review Board at the University of Vermont Medical Center, which deemed it to be exempt from patient consent.
Patient Samples and Propensity Score Matching
In the VQI database, there were 453 CLTI patients who underwent a PVI by retrograde pedal access in 458 limbs. Of these, 206 (45%) had follow-up data recorded, but 47 were missing data on amputation, for a total of 159 limbs. In the pedal access group, the approach was retrograde femoral (40%), antegrade femoral (26%), retrograde to antegrade femoral (22%), and pedal only (11%). Crossover from one approach to another occurred in 2 patients (one from a combined contralateral retrograde femoral and ipsilateral pedal to contralateral retrograde femoral and a second from ipsilateral pedal to contralateral retrograde femoral).
A comparator group of 1972 patients (mean age 69±12 years; 1129 men) having a contralateral retrograde femoral access was established based on the following variables: age, male gender, race, body mass index (BMI), presence of congestive heart failure (CHF), dialysis dependence, prior bypass, prior major or minor amputation, urgent operation, tissue loss as indication for the procedure, arterial segment treated, and living status. Characteristics of the 2 access cohorts are presented in Table 1.
Characteristics of Patients Treated by Retrograde Pedal and Contralateral Retrograde Femoral Access. a
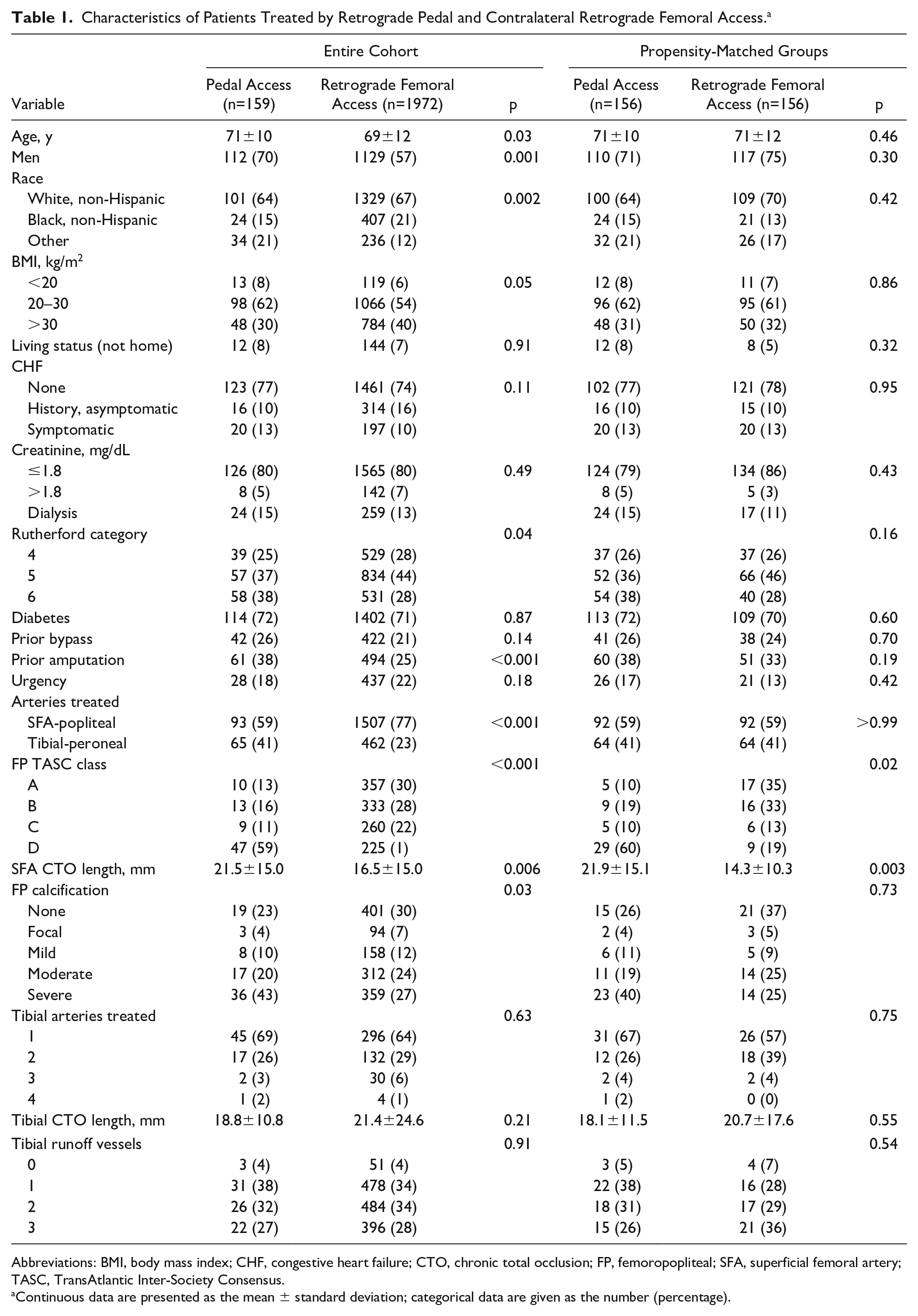
Abbreviations: BMI, body mass index; CHF, congestive heart failure; CTO, chronic total occlusion; FP, femoropopliteal; SFA, superficial femoral artery; TASC, TransAtlantic Inter-Society Consensus.
Continuous data are presented as the mean ± standard deviation; categorical data are given as the number (percentage).
Propensity scores were built through a binary logistic regression using the following baseline covariates: age, sex, race, BMI, living status, creatinine, urgency, indication, arteries treated, and prior history of CHF, bypass, and/or amputation. A 1:1 nearest neighbor matching was performed without replacement based on a greedy matching algorithm with a caliper range of 0.25, resulting in 156 matched patients (Table 1).
Outcomes
The main outcome was major adverse limb events (MALE), defined as major amputation or reintervention at 30 days and at 1-year follow-up. Secondary outcomes included (1) amputation-free survival (AFS), defined as absence of above-the-ankle amputation of the index limb or death from any cause at 30 days and 1 year and (2) in-hospital major adverse cardiac events (MACE) defined as any postoperative myocardial infarction or postoperative death. In addition, technical success and access site complications (hematoma, access site occlusion, and target vessel thrombosis) were compared between matched groups.
Statistical Analysis
Statistical methods to compare the variables of interest between the matched groups were the McNemar chi-square test for categorical variables and a paired t test for continuous variables. Survival was estimated using the Kaplan-Meier method (differences between groups were analyzed with the log-rank test) and Cox proportional hazards regression modeling stratified by matched sets to generate hazard ratios (HR) and 95% confidence intervals (CI). The threshold of statistical significance was p<0.05. All analyses were conducted using SAS statistical software (version 9.4; SAS Institute, Inc, Cary, NC, USA).
Results
Patients treated via pedal access in the unmatched cohort were older (71 vs 69 years, p=0.03) and were more likely to have had a prior minor or major amputation (38% vs 25%, p<0.001) or to have treatment of the tibial-peroneal vessels (41% vs 23%, p<0.001) than patients in the retrograde femoral access group (Table 1). The only significant differences between the propensity-matched groups were the length of chronic total occlusions in the superficial femoral artery and the TransAtlantic Inter-Society Consensus class, which were not included in the propensity matching (Table 1).
In the matched cohorts, the anterior tibial (89, 57%) was the most common artery used for access compared to the tibial peroneal trunk (25, 16%), posterior tibial (48, 31%), and peroneal arteries (17, 11%). Ultrasound guidance was utilized in 143 (92%) of the pedal access procedures, fluoroscopy in 7 (4%), and no imaging guidance in 6 (4%) cases (Table 2). The types of tibial interventions were balloon angioplasty (89% vs 99%), stent (11% vs 7%), and atherectomy (33% vs 23%) for pedal access vs retrograde femoral access procedures, respectively.
Procedure Characteristics in the 156 Matched Pairs.
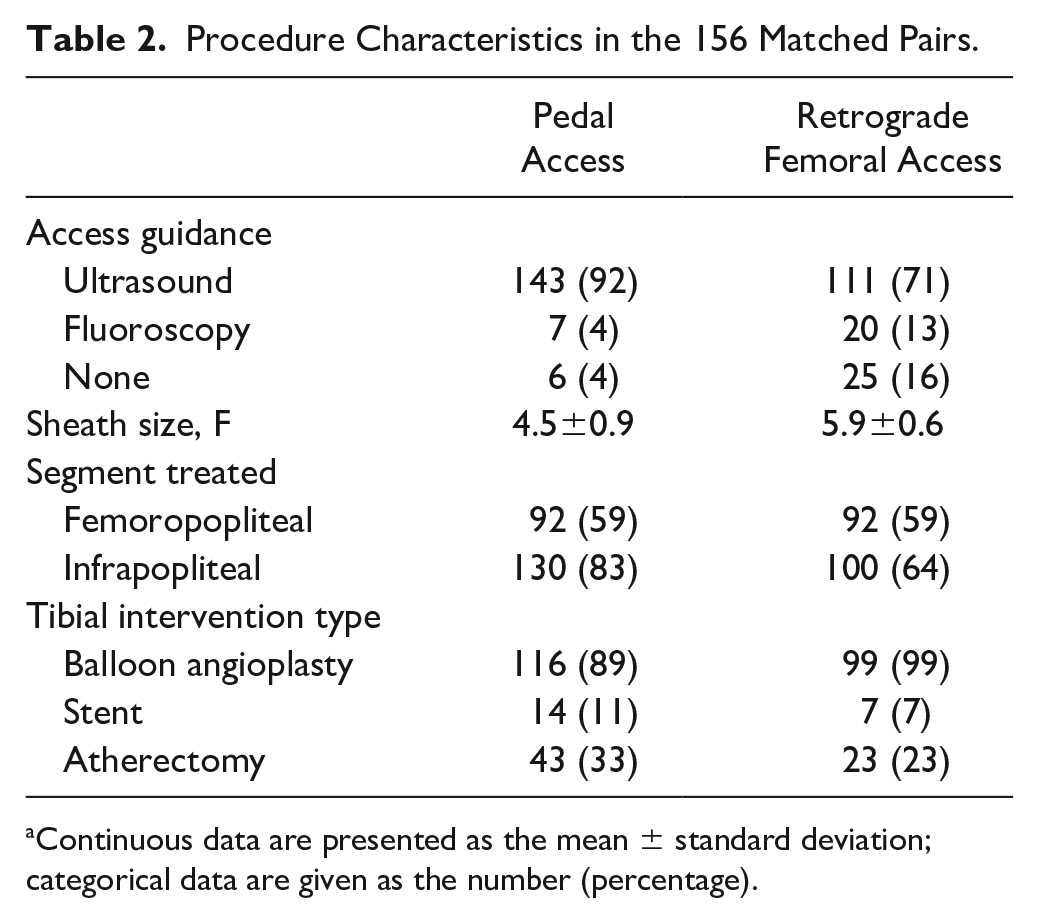
Continuous data are presented as the mean ± standard deviation; categorical data are given as the number (percentage).
Technical failure was not significantly different at 7% for femoral access and 13% for pedal access (p=0.07) in the matched groups. For patients without diabetes (14 pairs), technical failure was the same (n=1) for retrograde femoral and pedal access. For those with diabetes (80 pairs), the technical failure rates were significantly lower for retrograde femoral access (5%, 4/80) vs 19% (15/80) for pedal access (p=0.008).
Complications were rare and included access site hematoma (1% vs 3%, p=0.32) and target artery thrombosis (0 vs 1%) for the retrograde femoral vs pedal access groups, respectively. MALE occurred in 2 (1%) patients at 30 days in the retrograde femoral group vs 8 (5%) in the pedal access group (log-rank p=0.06; HR 4.00, 95% CI 0.85 to 18.84).
The rates of MALE at 1 year were 24% in the retrograde femoral group and 38% in the pedal access group (HR 1.95, 95% CI 1.15 to 3.30). Kaplan-Meier estimates for freedom from MALE at 1 year for the retrograde femoral and pedal access groups were 76% (95% CI 68% to 83%) and 62% (95% CI 52% to 70%), respectively (log-rank p=0.01; Figure 1A). AFS at 1 year was 86% in the retrograde pedal group and 83% in the pedal access group (HR 1.32, 95% CI 0.73 to 2.39). Kaplan-Meier estimates for AFS at 1 year for retrograde femoral and pedal access were 86% (95% CI 80% to 91%) and 83% (95% CI 76% to 88%), respectively (log-rank p=0.37; Figure 1B). Analysis of the propensity score–matched cohort revealed similar major amputation rates of 10% (16/156) for retrograde femoral access and 13% (21/156) for pedal access (HR 1.58, 95% CI 0.77 to 3.26, p=0.21) at a median follow-up of 10.8 months. Kaplan-Meier estimates for freedom from major amputation at 1 year for retrograde femoral and pedal access were 88% (95% CI 81% to 93%) and 85% (95% CI 77% to 90%), respectively (Figure 1C).
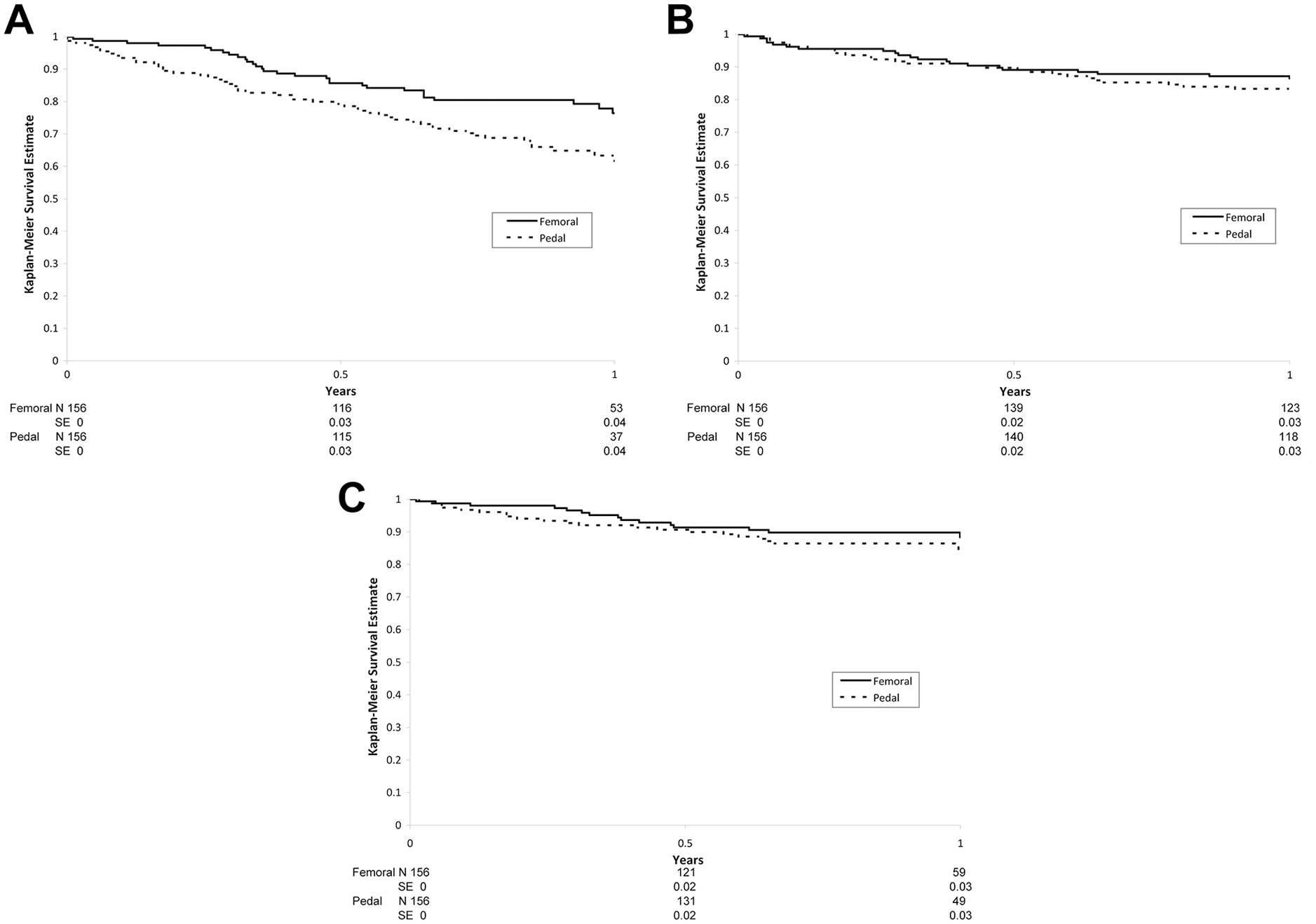
Kaplan-Meier analyses of (A) freedom from major adverse limb events, (B) amputation-free survival, and (C) freedom from major amputation after retrograde femoral vs pedal access.
In-hospital MACE rates were similar between the pedal access (9, 6%) and the retrograde femoral (8, 5%) groups (p=0.81). In the propensity-matched groups, the raw reintervention rates at 1 year were 21% for pedal access and 11% for retrograde femoral access (p=0.02).
The mean total length of stay (LOS) was similar between groups at 3.2 vs 2.6 days in pedal and retrograde femoral groups, respectively (p=0.34). The mean postoperative LOS was similar at 1.9 vs 1.5 days in the pedal and retrograde femoral groups (p=0.38).
Discussion
Patients with CLTI who are not candidates for a surgical bypass or are unable to be revascularized through a traditional percutaneous approach may benefit from alternative access routes such as retrograde pedal access. Bazan et al 11 describe some advantages of utilizing a pedal approach, including easier crossability, decreased likelihood of entering collateral vessels due to their caudal angle, and improved pushability through the smaller-diameter tibial vessels. The approach may also have a safety advantage in the patients with prior bifurcated aortic grafts, hostile groin, or morbid obesity. 11 Additionally, pedal access has been successfully used as a bailout procedure after complications from a traditional femoral approach in an SFA intervention. 12
El-Sayed et al 13 performed a retrospective study of patients with tibial vessel disease who had failed antegrade revascularization. They achieved successful revascularization in 67% of the patients, with an 88% limb salvage rate at 1 year. In addition to the efficacy of the approach, they reported a 5% 30-day MACE rate and 5% 30-day MALE, which was similar in our study. In another single-center retrospective study, Kaushal et al 14 reported a 63% technical success rate and a 79% limb salvage rate with short-term follow-up of only 5 months. Other authors in single-center studies have similarly supported the safety and effectiveness of this approach.15–19
Our study determined that a pedal approach is a safe alternative to a contralateral retrograde femoral approach, with no significant difference in technical failure or access site complications, specifically hematoma or target vessel occlusion or thrombosis. Despite patients undergoing pedal access being older and having a greater proportion of tibial-peroneal disease, there was no difference in major amputation rates in the unmatched analysis or in the propensity-matched groups. The pedal access group had a higher rate of MALE at 30 days and 1 year but comparable AFS to the retrograde femoral group. This was due to a reintervention rate in the pedal access group at 1 year nearly twice that in the femoral access group.
Limitations
Although the VQI database is a prospectively maintained database with claims-based auditing of procedure capture, there is no independent third party group responsible for auditing all data, and follow-up data were not available for all patients. Additional study with registry matched to Medicare claims is planned to address this limitation. Despite these shortcomings, the VQI provides the best available granular data on real world practice across a variety of specialties.
Conclusion
In this multicenter registry analysis, retrograde pedal access in patients with CLTI appears safe and effective in comparison to traditional contralateral retrograde femoral access, with similar technical success, early complications, and major amputations within 1 year. There was a higher reintervention rate in the pedal access group but no difference in AFS, suggesting a tradeoff between limb salvage and repeat interventions.
Footnotes
Authors’ Note
This study was presented at Society for Vascular Surgery–Vascular Annual Meeting (June 14, 2019; National Harbor, MD, USA).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.