
Abstract
Keywords
Introduction
The use of endovascular techniques has increased over the last decade and is expected to increase even further in years to come. There are many beneficial effects of such techniques, but the need for fluoroscopic guidance is not harmless. The exposure to ionizing radiation is often underestimated but has well-described consequences for patients and the operating room (OR) staff.1,2 Studies have shown that complicated interventions with long exposure times, such as endovascular aneurysm repair (EVAR), are associated with increased levels of circulating markers of DNA damage as well as a higher risk of developing future malignancies.1,3 Thus, it is crucial to develop techniques to reduce radiation exposure to patients and the operating staff. Fusion imaging is one such method whereby the preoperative computed tomography angiography (CTA) 3-dimensional (3D) data are dynamically superimposed on the intraoperative 2D fluoroscopic images, reducing radiation exposure during EVAR.4–6
Fusion imaging requires accurate alignment of the CTA volumes with the intraoperative position of the patient on the operating table.5,7 This process, known as image registration, was initially done using the skeleton and vascular calcifications obtained from cone beam computed tomography (CBCT, 3D-3D registration) performed at the beginning of the procedure. However, performing a CBCT at the beginning of the procedure can at times be logistically challenging and is associated with significant radiation exposure. More recent systems have shown the feasibility of using 2 single-frame 2D intraoperative fluoroscopy images in perpendicular projections to align the skeleton volume of the patient on the operating table with the CTA volume (2D-3D registration). Unfortunately, most of the first-generation angiographic fusion systems accommodate only 3D-3D registration and are not prepared to use 2D-3D registration. The update usually requires an upgrade of the hardware and/or software of the angiographic system or the reliance on third-party applications, both associated with considerable costs.
The present study sought to validate a new 2D-3D single-frame fusion registration method in a system prepared only for 3D-3D registration and explore how this registration affects the radiation exposure compared with traditional 3D-3D registration.
Materials and Methods
Study Design and Patient Sample
The electronic medical records of a university medical center were reviewed for 94 patients (median age 70 years; 85 men) who underwent EVAR with 2D-3D fusion imaging guidance between May 2013 and February 2017. Only patients with registration in the abdomen were included. The procedures were performed in a hybrid suite equipped with an Artis zee imaging system (Siemens Healthineers, Forchheim, Germany) installed in 2009. Data for 95 patients (median age 70 years; 81 men) in the 3D-3D registration control group were retrieved from a previous study 5 and corresponded to the period immediately preceding the introduction of the 2D-3D method. The clinical characteristics of the 189 patients and subgroups in the study are reported in Table 1. All patients gave their consent to participate in the study, which was approved by the Lund University ethics review board (EPN Dnr 2016/035) and followed the Declaration of Helsinki.
Clinical Characteristics of the Patients in the Study. a
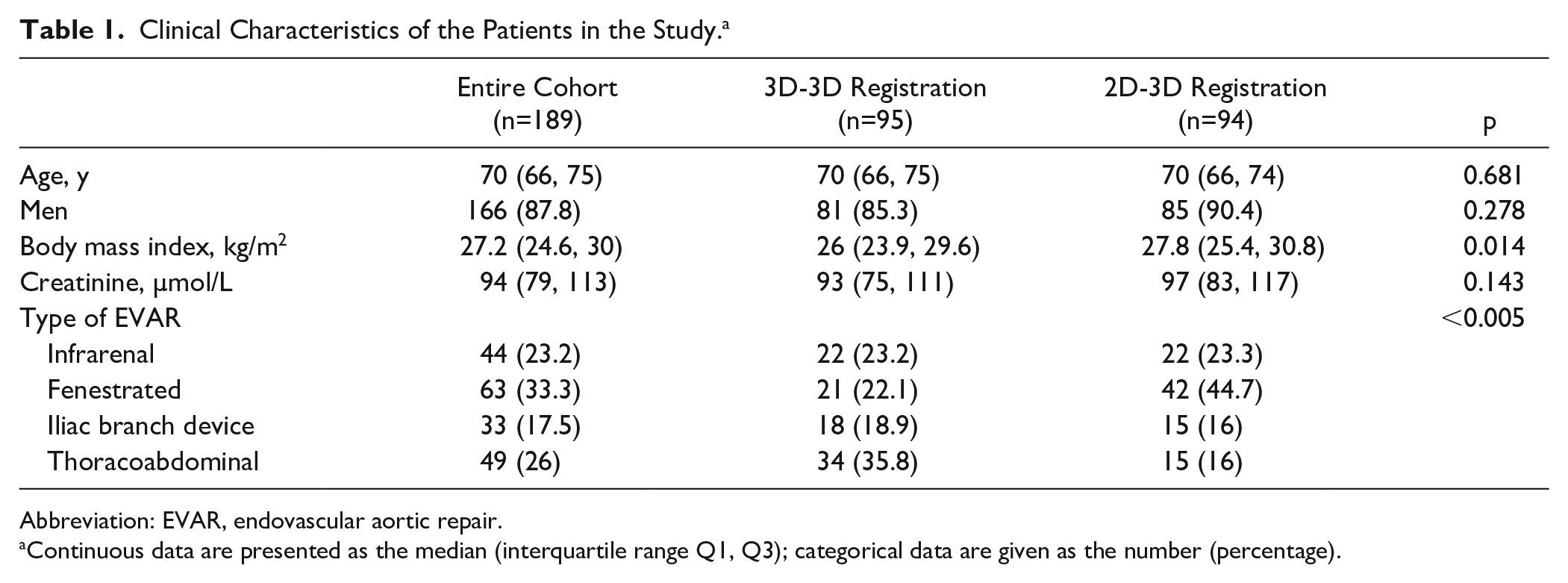
Abbreviation: EVAR, endovascular aortic repair.
Continuous data are presented as the median (interquartile range Q1, Q3); categorical data are given as the number (percentage).
Fusion Registration
The use of 3D-3D fusion registration has been described previously. 5 In summary, after sterile draping of the patient and immediately before vascular access, a 5-second CBCT scan focusing on the lumbar vertebral bodies and upper pelvis was done. This CBCT was automatically registered with the preoperative CTA using the 3D-3D registration tool that focuses on bone structures and aortic calcifications. Manual adjustments were performed whenever necessary.
In the new 2D-3D registration protocol, instead of performing the initial CBCT with the patient on the operating table, the dataset from a previously acquired offline CBCT of the empty operating table was uploaded into the intraoperative dataset (Figure 1A). This CBCT was then registered with the preoperative CTA using the system’s 3D-3D manual application (Figure 1B). In this way, instead of aligning the bone volumes of the CBCT and the CTA, the volume of the patient’s body on the CTA was made to lie on the operating table. Any rotational differences between the patient position on the operating table and the preoperative CTA were adjusted at this stage using the spinal processes on the CTA and on fluoroscopy as references.
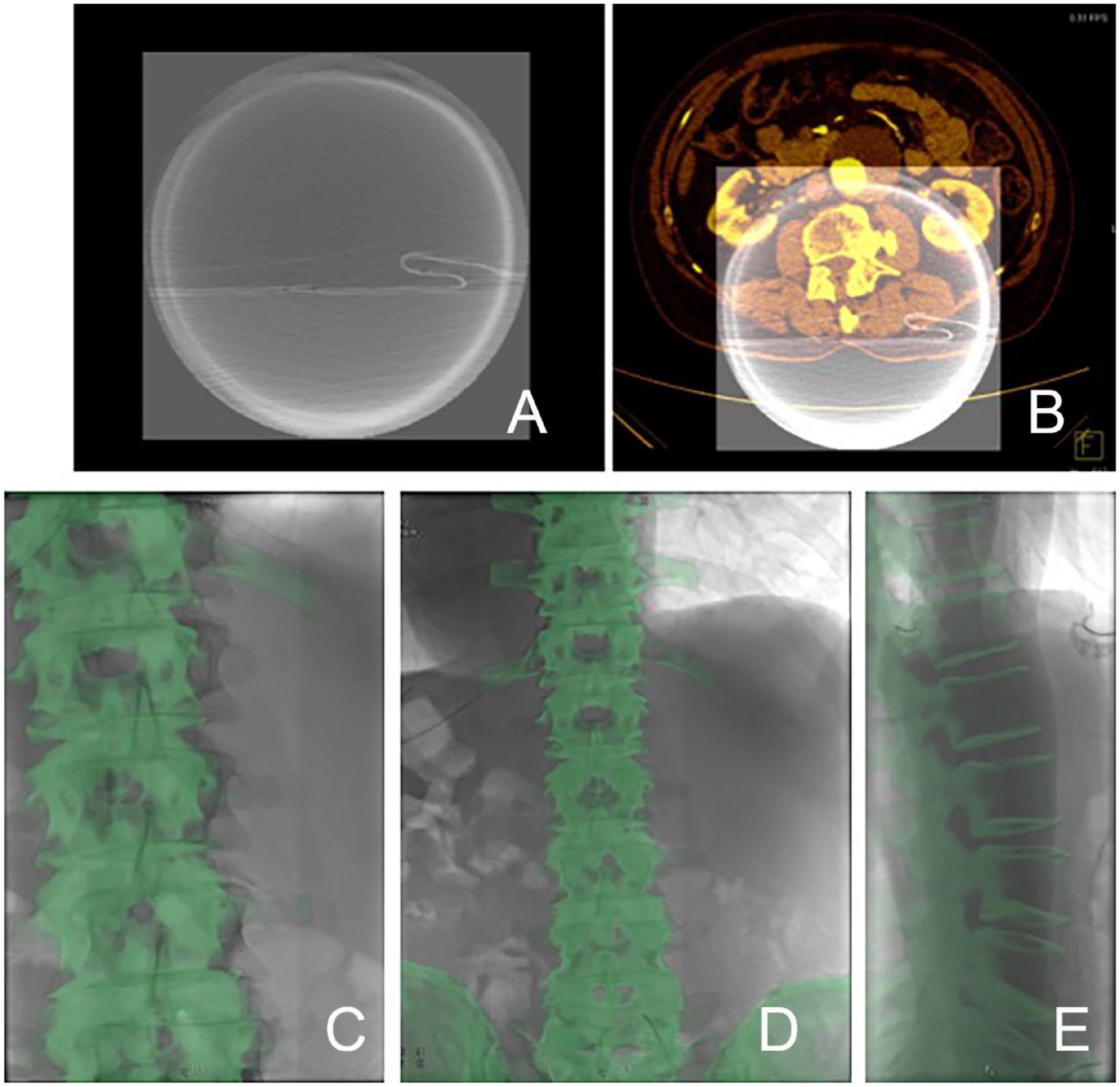
(A) Offline axial image of the cone beam computed tomography (CBCT) of the empty operating table. (B) Superimposition of the preoperative CT angiography on the empty CBCT. (C) Initial overlay of the skeleton from the CT angiogram (green) with intraoperative fluoroscopy in the anteroposterior projection. (D) Same as C but after correction of the misalignment. (E) Same as C but in a lateral projection.
Next, the patient’s vertebral bodies from T12 to L5 and pelvis from the preoperative CTA were overlaid on 2 intraoperative single-frame 2D fluoroscopy images (projections >60° apart, Figure 1C-E) using the manual alignment tool. In summary, this new method replaces the need for an initial CBCT of the patient by using a previously saved offline CBCT of the empty operating table. Moreover, the alignment of the table’s CBCT with the CTA is done only roughly instead of carefully as is the case in 3D-3D registration. These steps are faster in the new method than with the 3D-3D registration, but time is then required to align the 2D fluoroscopy with the CTA. However, this step is relatively fast.
Adjustment and Accuracy of Registration
After the 2D-3D or 3D-3D registration was done, digital subtraction angiography (DSA) was performed in an orthogonal projection to the aorta and one renal artery. This DSA was performed with the aortic stent-graft or a large hydrophilic dilator in place to simulate intraoperative distortion of the aorta by the stent-graft. Any misalignment of the renal artery origins between the CTA and DSA were corrected manually in 1-mm increments. The amount of correction was used as a measure of the total accuracy of the 2D-3D registration. The degree of correction was not registered in the 3D-3D control group; literature data were used instead as a reference.
Definitions and Statistical Analysis
Dose area product (DAP) of the registration process was assumed as the cumulative dose until the bone structures were aligned. The distribution of included variables was assessed using Kolmogorov-Smirnov analysis in combination with histograms. All variables were non-normally distributed and are presented as the median and interquartile range (IQR; Q1, Q3). Two-group comparisons were performed with the Mann-Whitney U or chi-square test; Spearman’s rho test was used for correlation analysis. Differences were considered statistically significant at p<0.05. SPSS software (version 23; IBM Corporation, Armonk, NY, USA) was used for statistical analysis; graphs were created using GraphPad Prism software (version 7.0; GraphPad, La Jolla, CA, USA).
Results
The patients who underwent the modified 2D-3D registration process had a significantly higher body mass index (BMI) compared with the 3D-3D group [27.8 vs 26 kg/m2, respectively; p=0.014]. No significant differences in gender, creatinine levels, or age were detected between the groups. On the contrary, the proportion of patients who underwent fenestrated EVAR was higher in the 2D-3D fusion imaging group (44.7% vs 22.1%), while thoracoabdominal repairs were more common in the 3D-3D registration group compared to the 2D-3D group (35.8% vs 16%).
Comparing the radiation exposure for the 2 registration processes disclosed a dramatically reduced median DAP for the 2D-3D group [1.12 Gy∙cm2 (IQR 0.41, 2.14)] vs the 3D-3D group [43.4 Gy∙cm2 (IQR 37.1, 49.0), p<0.001; Figure 2]. Finally, the 2D-3D registration measured in 73 of 94 patients had an accuracy of 4.0 mm (IQR 3.0, 5.0) after bone matching and before final correction with DSA (78% within 5 mm).
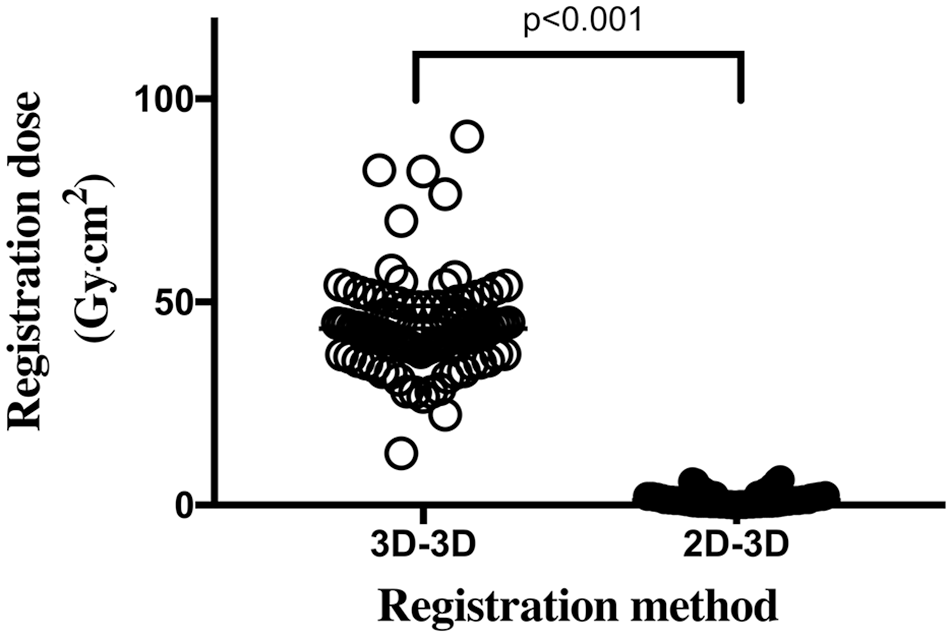
Plot of the dose area product used for the registration of fusion imaging. A 5-second cone beam computed tomography image was used in 3D-3D registration while single-frame fluoroscopy images were used for 2D-3D registration.
Discussion
The present study demonstrated the feasibility and accuracy of a new method to perform 2D-3D registration of fusion imaging on an angiography system originally prepared exclusively for 3D-3D registration. By applying this novel protocol for imaging fusion, the levels of radiation exposure were dramatically reduced without affecting the accuracy of fusion imaging.
According to a previous study by Schulz et al, 8 the accuracy of 3D-3D fusion registration was within 5 mm of the DSA in 68% of the cases. This is in line with the findings in the present study where new 2D-3D registration of the bone structures led to a <5-mm discrepancy of the aorta at the renovisceral segment in 78% of the cases. This is very good, especially taking into consideration that the angiography used for the final adjustment in our study was done with a large-bore device already within the aorta, which has been previously shown to lead to a 6-mm displacement of the origins of the renal arteries. 9 It also underlines the need for confirmation of the registration with a DSA independent of the method used.
Interest in the stochastic effects from exposure to ionizing radiation has increased in recent years. The 15-year follow-up of the EVAR 1 trial found a higher risk of future malignancies in patients who underwent EVAR compared with those who had open repair. 1 Even though repeated exposures from the follow-up CT scans are certainly major contributors to the radiation dose, the importance of all intraoperative measures reducing the DAP should not be ignored. The new 2D-3D protocol for registering fusion images used in this study reduced the radiation exposure during registration by almost 40-fold (median DAP of 43.4 vs 1.12 Gy∙cm2) compared with the traditional 3D-3D registration process. 5 This occurred even though the 2D-3D group had significantly higher BMIs, which automatically increases the exposure by the angiographic system.
The initial CBCT for the registration of fusion imaging makes up between 27% to 46% of the total radiation dose of the procedure depending on its complexity. 5 The omission of this exposure would therefore be significant, especially in less complex procedures such as infrarenal EVAR. Moreover, such intraoperative radiation reduction may also have an impact on the OR staff who are subjected to scatter radiation during the procedure and who have been shown to have more malignancies than staff members not performing fluoroscopically-guided procedures. 2 However, even if a CBCT is associated with significant radiation exposure, 10 it does not necessarily affect the staff because they can be outside the room during exposure. On the contrary, the acquisition of the 2 projections in fluoroscopy requires the proximity of the surgeon to the machine in order to adjust the table position. The levels of exposure are, nevertheless, minimal and negligible compared to the ones associated with the rest of the procedure. The replacement of the patient CBCT with an offline CBCT of the empty operating table obviates the need to interact with the patient, which can potentially make the workflow in the OR more effective. It also avoids the risks of changing the patient position if the CBCT was done before sterile draping.
The registration process of the 2D fluoroscopy images to the 3D volume from the CTA is equivalent to the verification step in the 3D-3D registration. The time required is negligible compared to the total procedure time and saves time by omitting the initial CBCT. However, when adapting a method to a system not prepared for it, the user-friendliness is naturally decreased compared to the methods currently available for 2D-3D registration in modern angiographic systems. However, this shortcoming is easily overcome for those already using the 3D-3D fusion imaging tools, though some staff training may be required.
Limitations
The lack of information on the magnitude of the adjustment after the 3D-3D registrations did not allow a direct comparison. For this reason, only procedures involving the renovisceral segment were included since this is the best studied segment to allow comparison with the literature.5,8,9,11 Furthermore, the study was done solely with old Siemens angiographic equipment, but similar adaptations should be possible with other manufacturers’ imaging systems. It should also be taken into account that by allowing a new technique to be incorporated into an older system, the utility of the older system can be prolonged while still having access to state-of-the-art imaging. However, the workflow is not streamlined and many extra steps are required compared to the newer versions of the software, making it less user-friendly.
Conclusion
A new registration protocol based on 2 single-frame images avoiding an initial intraoperative CBCT can be used for fusion imaging in a system originally designed for 3D-3D registration. This 2D-3D registration is accurate and leads to a significant reduction in radiation exposure.
Footnotes
Acknowledgements
We are grateful to Martin Von Roden, Siemens Healthineers, for his dedicated work in developing the method and to the staff at the Vascular Center, SUS Malmö, Sweden, especially Helen Billberg and Anas Alzahrani.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Nuno V. Dias is a consultant for Siemens Healthineers.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Swedish Heart and Lung Foundation, Skånes University Hospital funding, ALF, Swedish Society for Medical Research, Hulda Almroth Foundation, and Emil and Wera Cornell Foundation.