
Abstract
Keywords
Introduction
Over the past 10 years, fenestrated endovascular aneurysm repair (fEVAR) has become an important treatment option for complex aortic aneurysm. In 2004, the Advanta V12 balloon-expandable stent-graft (Getinge, Gothenburg, Sweden) started a new era in endovascular repair. For the first time it was possible to seal between a fenestration and its target vessel (TV), even if there was a distance between the fenestration in the main body and the TV. Today, there are 3 other balloon-expandable covered stents that have also been used as bridging stent-grafts (BSGs) in fEVAR procedures: the BeGraft (BeG; Bentley InnoMed, Hechingen, Germany), introduced in 2013, the LifeStream (BD/Bard, Tempe, AZ, USA), introduced in 2014, and the balloon-expandable Viabahn VBX (Gore Medical, Flagstaff, AZ, USA), introduced in 2018. Favorable outcomes with 99% TV patency after 1 year have been reported for the second-generation BeG stent-grafts in fEVAR, 1 and a recent in vitro study has confirmed their superior properties compared with the first-generation BeG. 2 Recently, the first positive results were also published about the Viabahn VBX used in fEVAR and branched EVAR (bEVAR). 3 Nonetheless, the need for reinterventions during follow-up in 8% to 26% of the patients1,4 remains the main problem after f/bEVAR. Most of the reinterventions are required for TV problems such as type III endoleaks, stenosis, and occlusion.4,5
Geometrical changes in the TV after f/bEVAR have been reported,6–8 and it has been hypothesized that those anatomical changes may predispose to TV-related complications.6,7 In a previous study assessing the immediate changes of the TV anatomy after fEVAR using 3 different types of BSGs and 2 types of main devices, 7 no significant differences among the different materials were found. Since most of TV-related complications occur during the midterm after fEVAR, 4 the aim of this study was to evaluate the anatomical TV changes after fEVAR during further follow-up of 2 different types of main body stent-grafts and 2 different types of BSGs.
Materials and Methods
Study Design
This retrospective, single-center study included 56 patients (mean age 71±7 years; 49 men) who underwent fEVAR in our center between June 2010 and July 2016 and who had at least 2 postoperative computed tomography angiography (CTA) scans. The study was approved by our local ethics committee. The patient characteristics are summarized in Table 1.
The Characteristics of the 56 Patients in the Study. a
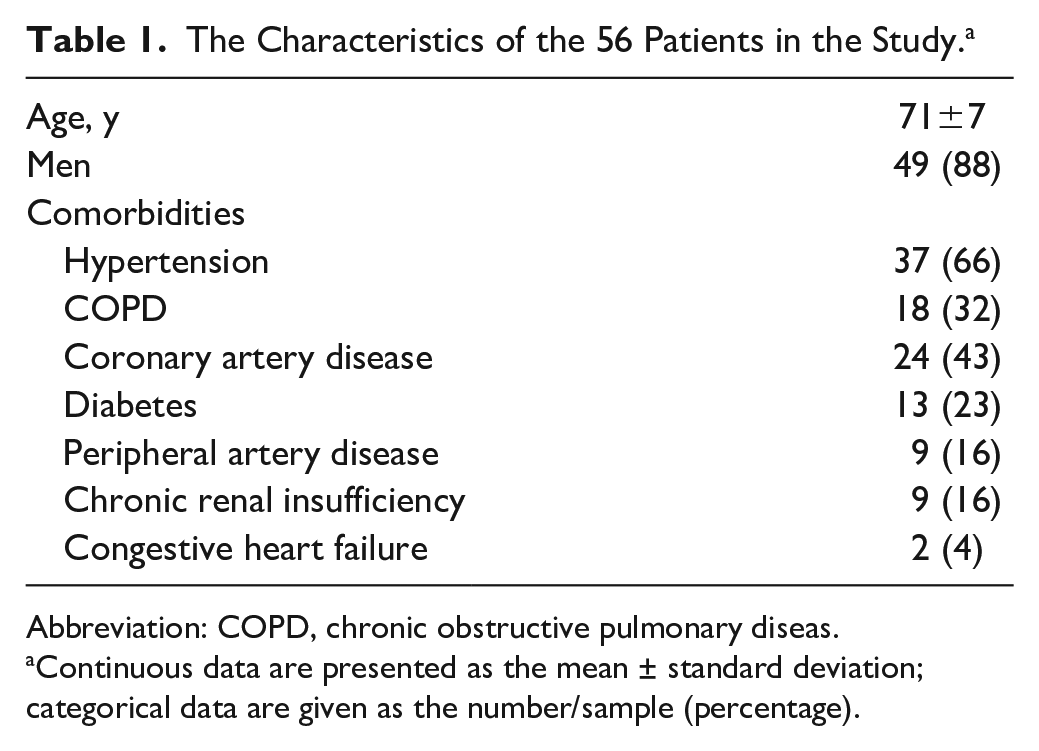
Abbreviation: COPD, chronic obstructive pulmonary diseas.
Continuous data are presented as the mean ± standard deviation; categorical data are given as the number/sample (percentage).
The patients received custom-made Zenith (Cook Australia Pty Ltd, Brisbane, Australia; n=22) or Anaconda (Terumo Aortic, Inchinnan, Scotland, UK; n=34) stent-grafts; 6 had both branches and fenestrations. Two types of balloon-expandable stent-grafts were used as BSGs: the Advanta V12 and the BeG stent-grafts. Before 2013, the V12 was used exclusively. After the BeG came to market in 2013, both the first and subsequently second-generation BeGs were employed. The choice between the BSGs was made according to the preference of the operating surgeon, but the second-generation BeG was used preferentially due to its favorable properties. 2
For purposes of this analysis only the TVs and BSGs of fenestrations were included in the measurements. Nine TVs having >1 BSG implanted during the primary procedure were excluded because no clear differentiation of anatomical changes of each stent-graft would be possible. In the same way, 3 TVs that had to be restented before the second CTA scan were excluded, leaving 140 TVs bridged by 74 V12s and 66 BeGs for analysis (Figure 1).
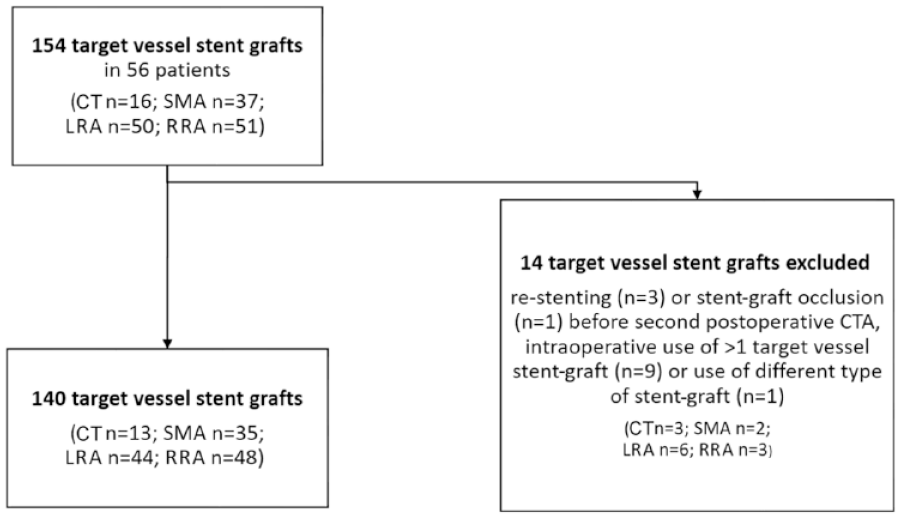
Number of target vessels included for analysis. CT, celiac trunk; LRA, left renal artery; RRA, right renal artery; SMA; superior mesenteric artery.
Imaging and Measurements
All CTA scans were electrographically gated, triphasic, high-resolution scans acquired during inspiration. The first CTA was the postoperative control before discharge. The first follow-up CTA after discharge was scheduled at 3 to 6 months after implantation; further scans were scheduled depending on the result. Routinely, the examination interval was extended to yearly in an uneventful course. In patients with chronic renal insufficiency, the CTAs were replaced by unenhanced CT scans supplemented by contrast-enhanced ultrasound in order to reduce the exposure to nephrotoxic contrast agent.
To evaluate the changes in TV geometry, the preoperative CTA scan as well as the first, the second, and if available, the most recent CTA scans were analyzed retrospectively using the OsiriX MD software (release 2.6; Pixmeo SARL, Geneva, Switzerland). The measurements were performed by 2 observers in consensus. Each TV was analyzed separately on each CTA scan. The measurements were performed in similar fashion to a previously published work on early changes in TV anatomy after fEVAR. 6 Briefly, 2 angles were measured to evaluate the anatomical response of the TV to the BSGs. The first angle was the ostial TV deviation. After normalizing the view mode by the second lumbar vertebral body (Supplementary Figure 1; available in the online version of the article), the angle at the TV origin was measured in 2 views [sagittal and axial views for the celiac trunk and the superior mesenteric artery (SMA), coronary and axial views for the renal arteries]. The measurement of the ostial TV deviation is shown in Figure 2A.
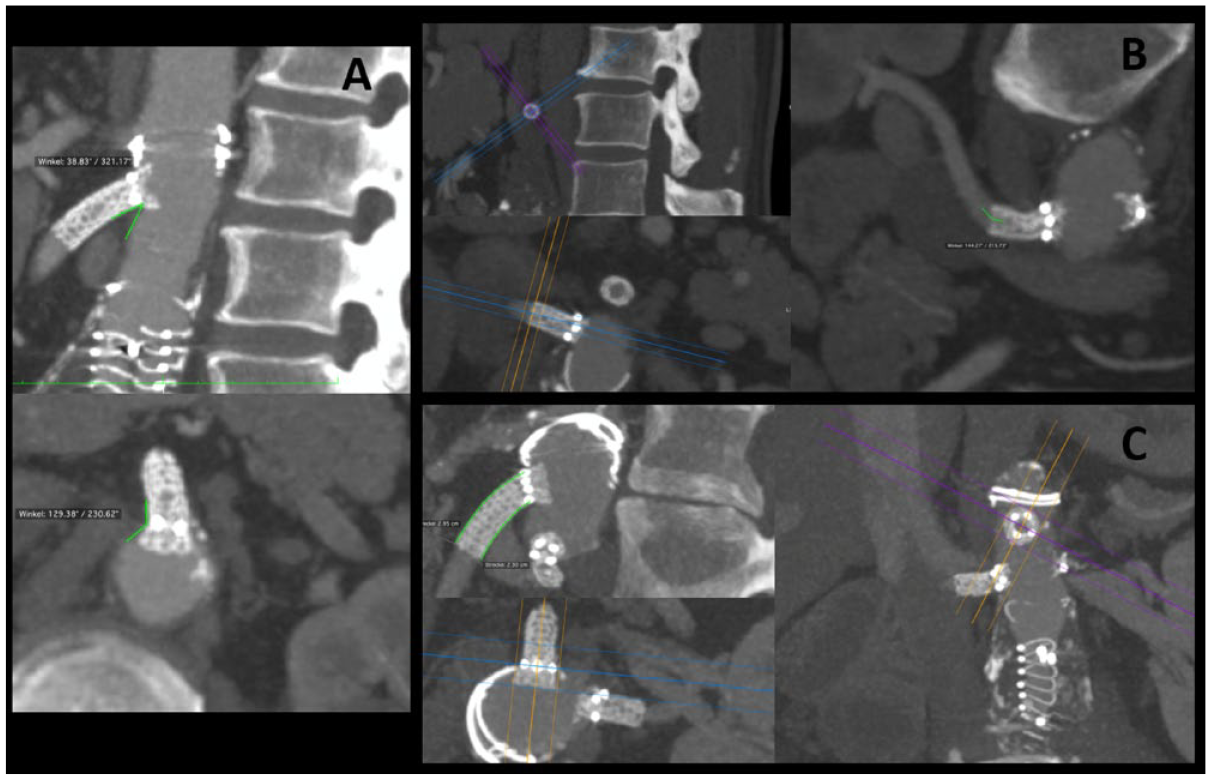
The 3 measurements of target vessel and bridging stent-graft (BSG) geometry. (A) The ostial TV deviation for the superior mesenteric artery. (B) The anatomical vessel shift distal to the BSG in the right renal artery. (C) Lengths of the inner and outer curves of the BSG.
The second angle was the anatomical TV shift distal to the BSG. As described before, 6 2 of the 3 axes in the 3-dimensional view mode were adjusted parallel to the longitudinal and the vertical direction of the BSG. The maximum angle distal to the BSG was determined by rotation around its longitudinal axis and measured (Figure 2B). The difference of this value from 180°, that is, the vessel shift, was calculated.
In order to assess the conformability of the BSG, the lengths of its outer curve (L1) and its inner curve (L2) were measured in this same view. In addition to measuring the individual lengths L1 and L2, the L1/L2 ratio was calculated (Figure 2C).
Statistical Analysis
Continuous variables are expressed as mean ± standard deviation. The data were analyzed using a multivariable linear mixed effects model to investigate the effect of age, type of main device, target vessel, type of BSG [V12 vs BeG (including both generations)], sex, time since implantation (repeated factor), complication, renal insufficiency, and diabetes on the ostial TV deviation, the TV shift distal to the BSG, and the BSG L1/L2 ratio.
Variables achieving p≤0.3 in the univariable analysis were entered into the multivariable model using a backward selection process if the interaction reached p<0.05, the threshold of statistical significance. Overall survival was analyzed using the Kaplan-Meier method. Statistical analyses were performed using SAS software (version 9.4; SAS Institute Inc, Cary, NC, USA).
Results
The CTA evaluation produced 393 measurements (38 celiac trunks, 102 SMAs, 121 left renal arteries, and 132 right renal arteries) for analysis. There were no statistically significant associations of the ostial TV deviation with any of the analyzed parameters over time (Table 2) in either the univariable or the multivariable analysis. However, the vessel shift distal to the BSG was significantly associated with the type of TV in the univariable (p<0.001) and multivariable analyses (p<0.001). Analyzing the different TVs separately in the univariable model (Figure 3), the mean vessel shift was 16.0° in the SMA, 25.0° in the celiac trunk (p=0.005 vs the SMA), 22.5° in the left renal artery (p=0.003 vs the SMA), and 24.5° in the right renal artery (p<0.001 vs the SMA).
Results of the Uni- and Multivariable Analyses for the Main Outcomes.
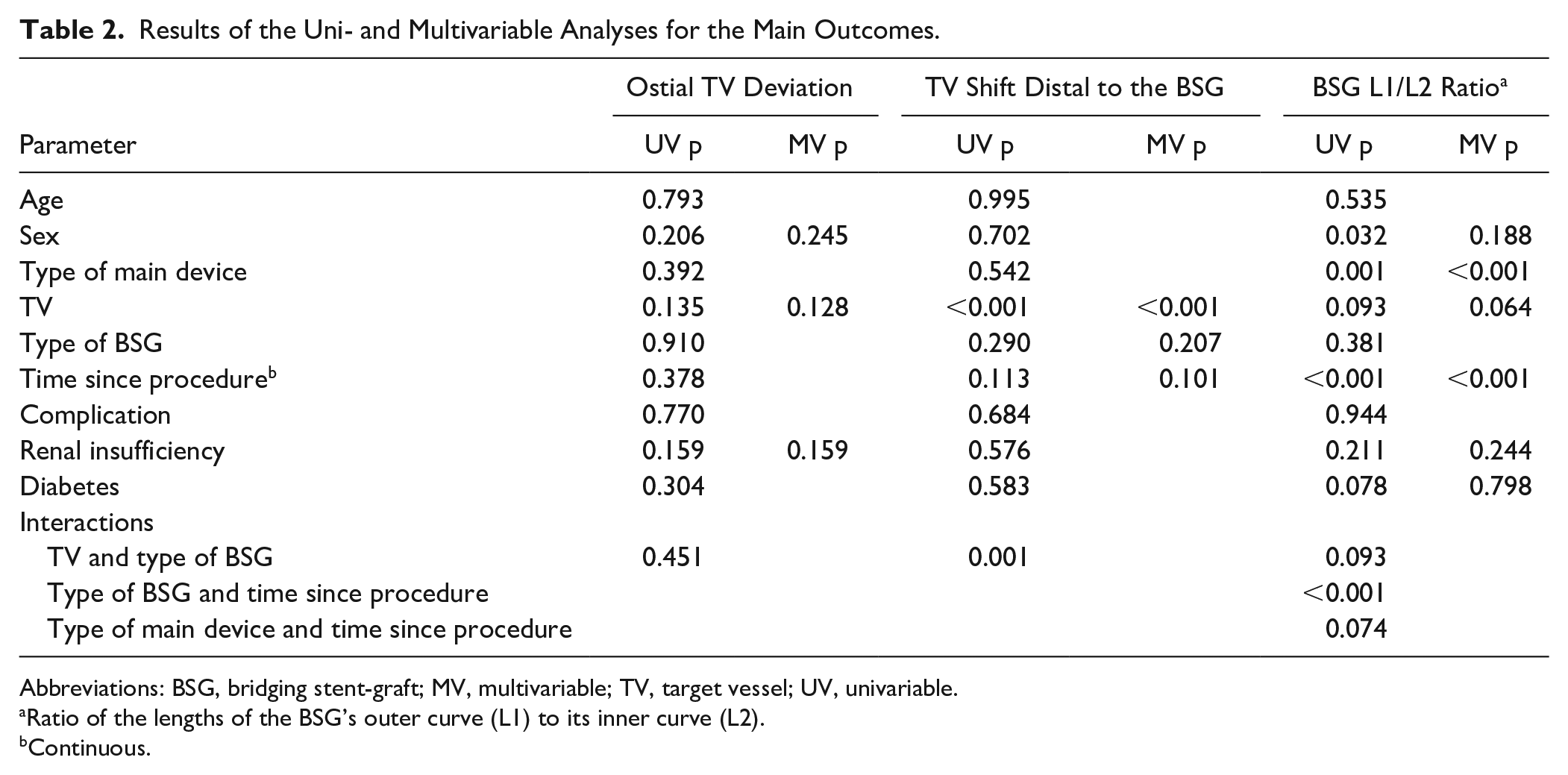
Abbreviations: BSG, bridging stent-graft; MV, multivariable; TV, target vessel; UV, univariable.
Ratio of the lengths of the BSG’s outer curve (L1) to its inner curve (L2).
Continuous.
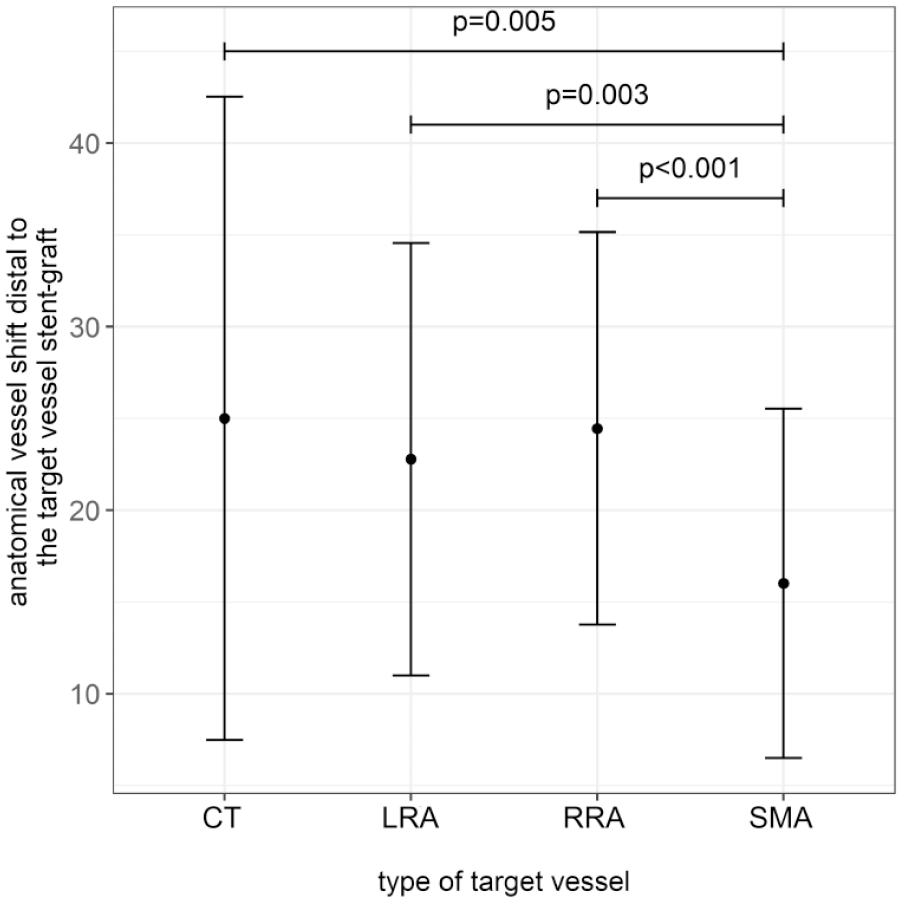
Anatomical vessel shift distal to the bridging stent-graft over time. The mean vessel shift was 16.0° in the superior mesenteric artery (SMA), 25.0° in the celiac trunk (CT; p=0.005 vs the SMA), 22.5° in the left renal artery (LRA; p=0.003 vs the SMA), and 24.5° in the right renal artery (RRA; p<0.001 vs the SMA).
Furthermore, the univariable analysis showed a significant association of the vessel shift distal to the BSG with the interaction of the type of TV and the type of BSG (p=0.001). In the celiac trunk, greater vessel shifts were observed after implantation of BeGs vs V12s. In all other TVs, there were greater vessel shifts after implantation of V12s vs BeGs. However, this interaction between the TV and the type of BSG did not show a statistically significant association in the backward selection process and was therefore not included in the multivariable model. Neither were the differences between the 2 types of BSGs statistically significant (Figure 4) for the TVs separately (celiac trunk: padj=0.141; SMA: padj=0.383; left renal artery: padj=0.236; right renal artery: padj=0.369). There was no significant association of the vessel shift distal to the BSG with any of the other parameters.
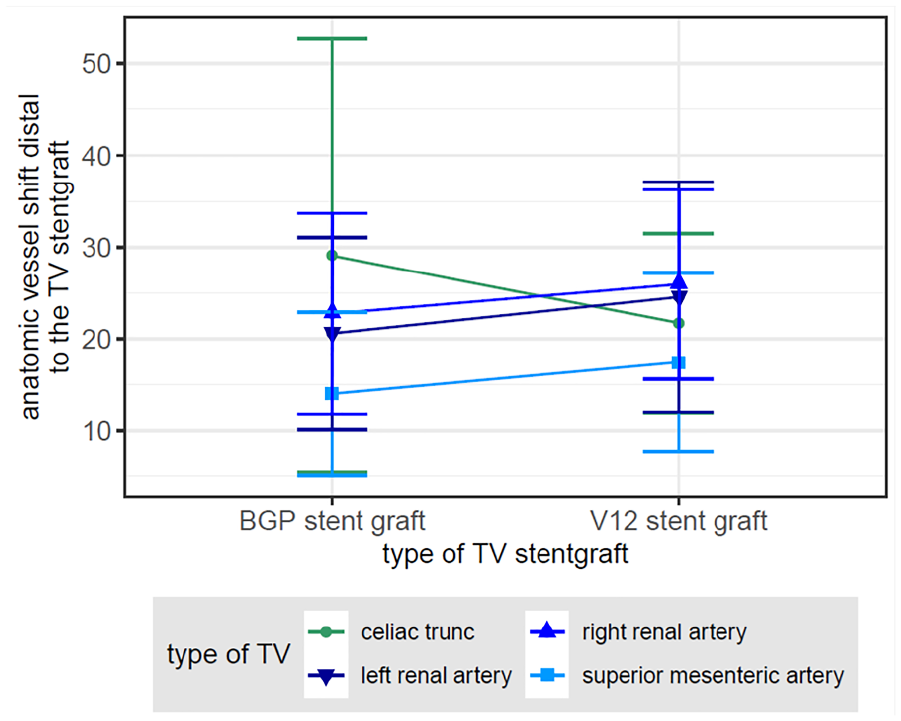
Anatomical vessel shift distal to the bridging stent-graft (BSG): Interaction between the type of target vessel (TV) and BSG. There was a significant association in the univariable analysis (p=0.001) for the celiac trunk, which had greater vessel shifts after BeG implantation vs the V12; all other TVs had greater vessel shifts after V12 implantation.
BSG Curve Lengths
The BSG L1/L2 ratio was significantly associated with the type of main device (Table 2) and was larger (p<0.001) in the Zenith devices compared to the Anaconda (Figure 5). The separate analysis of the outer (L1) and inner (L2) curve lengths showed that the mean L1 was greater in Zenith models: the difference was 0.31 cm for the right renal artery, 0.08 cm for the left renal artery, 0.17 cm for the SMA, and 0.59 cm for the celiac trunk. The mean L2 was 0.16 cm smaller in the Zenith than the Anaconda independent of the type of TV while adjusting for the other variables in a multivariable model. This effect was statistically significant (p<0.001 for both curves and both analyses).
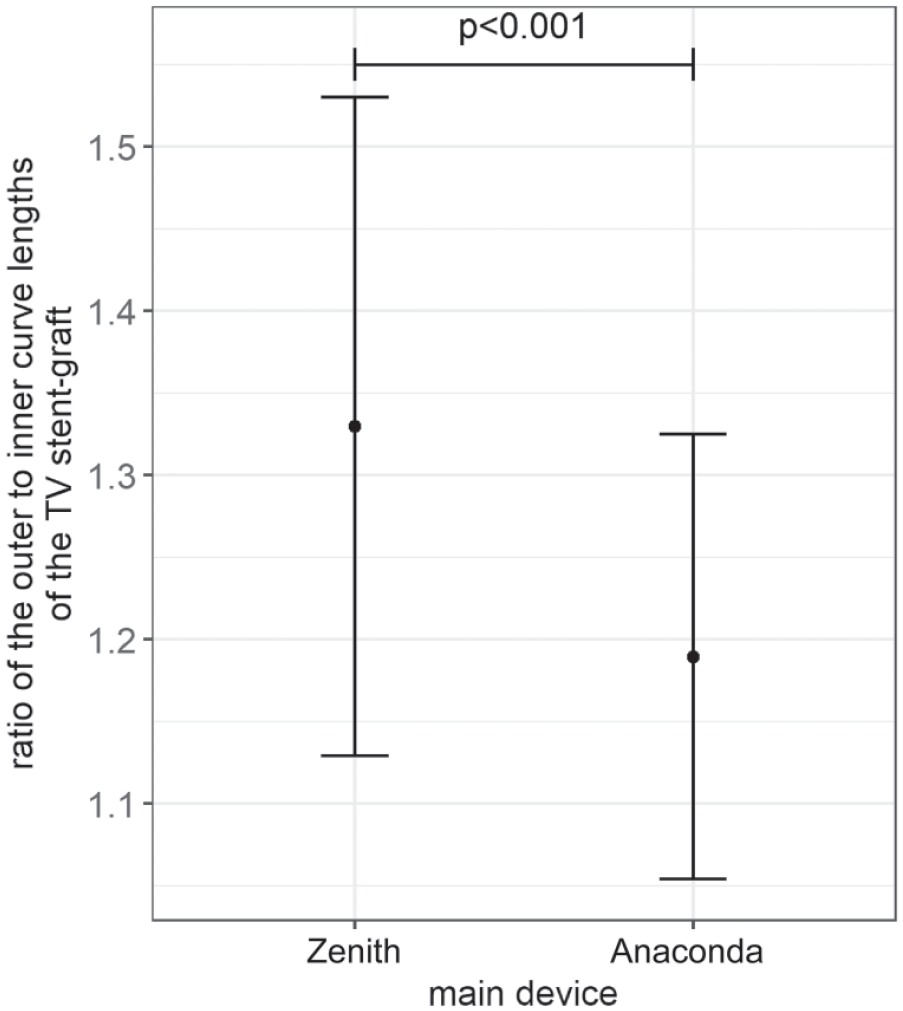
The ratio of the outer to inner curve lengths of the bridging stent-grafts was significantly larger in the Zenith than in the Anaconda (p<0.001).
Further, there was a statistically significant association between the type of TV and the L1 (p<0.001). Compared to the right renal artery, the mean L1 was 0.11 cm shorter in the celiac trunk, 0.09 cm shorter in the left renal artery, and 0.08 cm longer in the SMA. There was no significant association between the BSG L1/L2 ratio and the type of BSD (univariable p=0.381). The separate analysis did not show a statistically significant association of the type of BSG with L1 (univariable p=0.213) or L2 (univariable p=0.871). The interaction of the type of TV and the type of BSG showed a significant association with L1 only in the univariable analysis (p=0.015) but not in the backward selection method.
Moreover, the BSG L1/L2 ratio changed significantly with increasing time (p<0.001; Figure 6). In the individual analysis of L1 and L2, the L1 increased by a mean of 0.022 cm per year (p<0.001), whereas the L2 decreased by a mean of 0.019 cm per year (p<0.001).
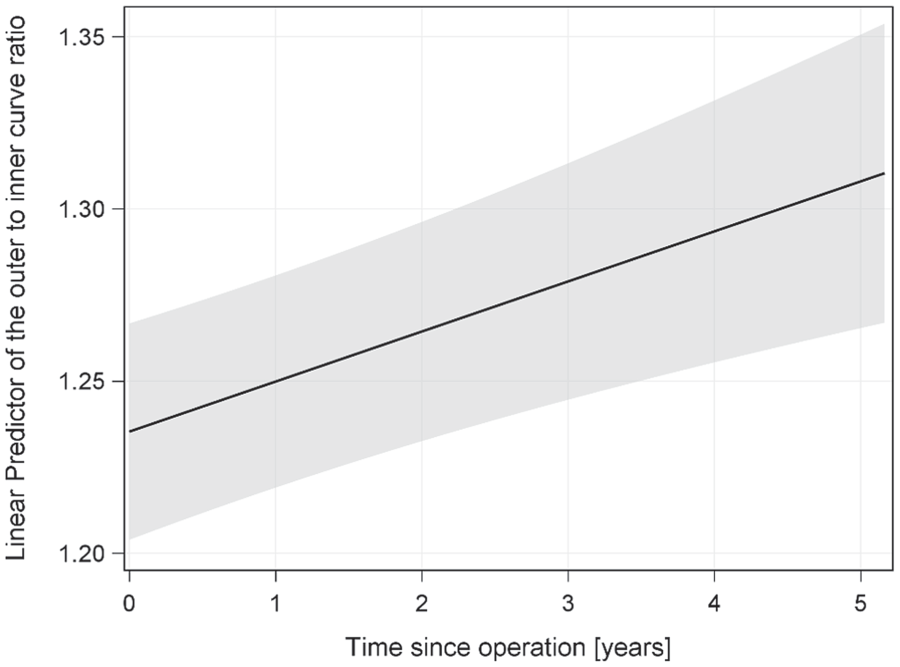
Effect of time since operation on the bridging stent-graft’s outer to inner curve length ratio.
Follow-up
At a median 24 months (range 2–61), the estimated overall survival rate was 79%. Two TV occlusions were observed during follow-up, both in a renal artery treated with a BeG. Furthermore, there were 11 TV reinterventions (6 BeGs and 5 V12s): 5 for endoleaks, 4 for stenosis, and one for impending dislocation of the BSG. However, as regards possible risk factors for BSG-associated complications, only the L1 had a statistically significant association (univariable p=0.013, multivariable p=0.033; Table 3). The mean L1 was 0.17 cm shorter in patients without vs with complications.
Results of the Uni- and Multivariable Analyses of the Inner and Outer BSG Curve Lengths.
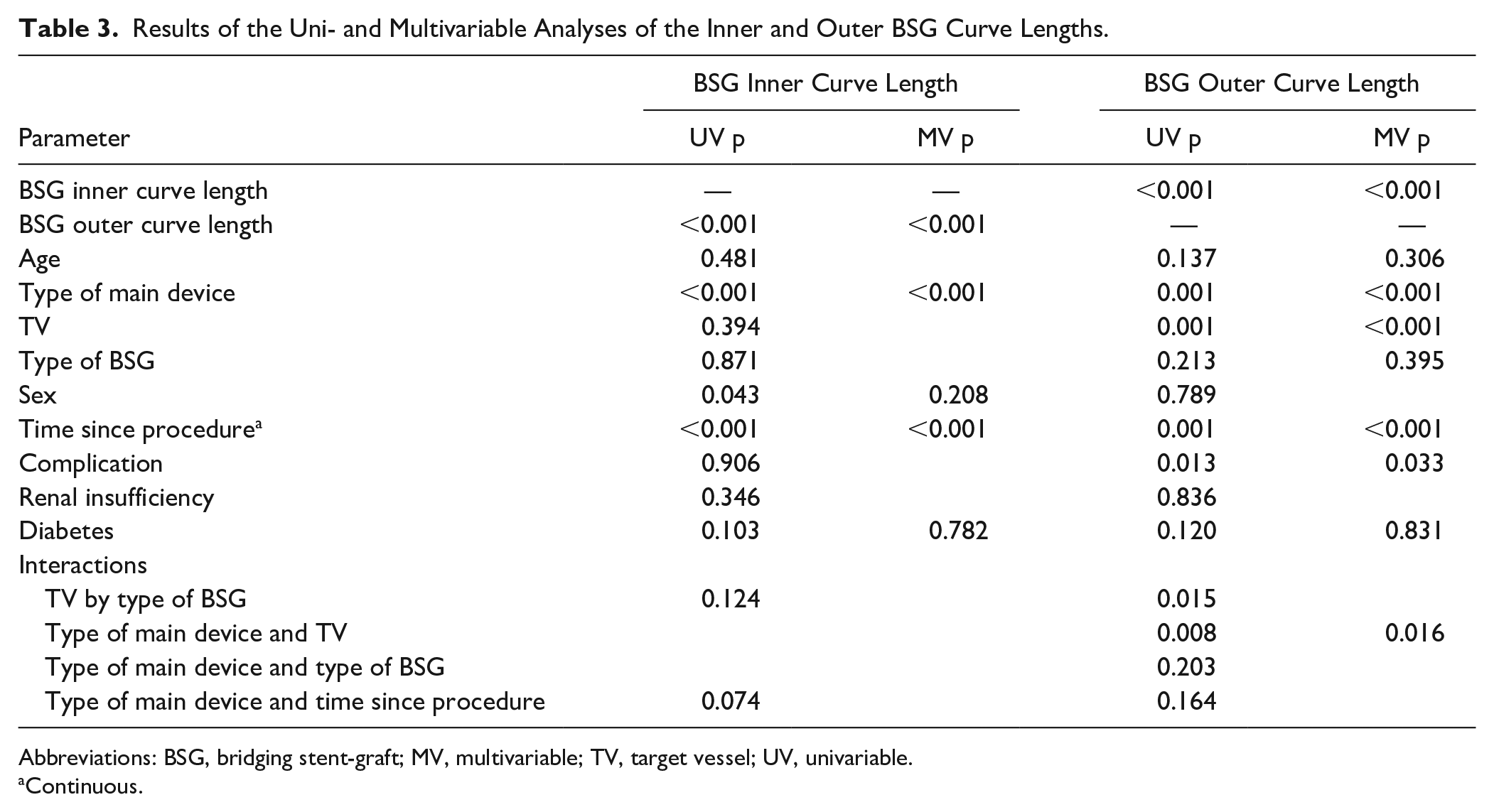
Abbreviations: BSG, bridging stent-graft; MV, multivariable; TV, target vessel; UV, univariable.
Continuous.
Discussion
The technique of fEVAR for complex thoracoabdominal aortic aneurysms has evolved significantly over the past years. One of the key improvements was the introduction of BSGs leading to higher TV patency rates, 9 which are currently reported as 92% to 99% in mid- to long-term follow-up.10–13 However, most of the reinterventions following fEVAR are still for TV-associated complications4,5 and may be related to anatomical changes induced by the operation.6,7
Indeed, significant anatomical changes of the renovisceral arteries can be observed immediately after fEVAR.7,8 In a study analyzing the ostial deviations of renal arteries after fEVAR, most of the changes were observed in the early phase between the pre- and postoperative CTA scans, without further changes thereafter. 8 This is in accord with the present results that showed no significant changes of the deviation of the TV at the aortic origin over a median 2 years.
However, other geometrical changes of the TV and the BSGs were observed during the study period. For instance, the BSG L1/L2 ratio increased significantly over time, which demonstrates an adaptation of the BSGs to the TV anatomy. Despite their distinct degrees of stiffness no significant difference between the V12 and the BeG was found in this regard.
Nonetheless, the findings of the present study suggest that the distinction between the two BSGs may be of importance depending on which artery is treated. In the celiac trunk, which has a straighter anatomy at its aortic origin than the other TVs, the vessel shift distal to the BSG was significantly smaller after V12 implantation vs the BeG. This relationship was reversed in all other TVs. Thus, the BeG seems to conform better to the original anatomy of the SMA and renal arteries. Although the clinical impact of this finding cannot be derived from the present study, it seems to correspond to the reported recently favorable early outcomes of the second-generation BeGs used as renal artery BSGs. 1
Moreover, the present study showed also a significant impact of the type of main device on the geometrical changes of the BSGs after fEVAR with larger L1/L2 ratios in the Zenith stent-graft vs the Anaconda. The most probable explanation is the greater stiffness of the Zenith owing to its Z-stent design compared to the ring stent and unsupported main body design of the Anaconda. In the latter, it seems that part of the adaptation of the endovascular components to the patient anatomy is transferred to the main body, whereas more adaptation occurs at the level of the BSGs when using the Zenith device. However, as found in a prior study on early anatomical TV changes after fEVAR, 7 the type of main device was not associated with the anatomical vessel shift distal to the BSG.
Regarding the possible association between anatomical/geometrical changes and TV-related complications, the present study did not show clear results. An increase of the BSG L1, possibly due to the continuous pulsatile strain on the outer curve of the vessel wall, was observed in TVs with complications vs in those without. However, no significant association of TV complications with any of the other measurements was detected. As reported earlier, this observation suggests that, although larger geometrical TV changes after f/bEVAR can lead to adverse TV events, 6 the renal arteries are able to adapt to a certain degree of anatomical change without sequelae. 8
In the authors’ opinion, the small to moderate anatomical changes of the aorta and its branches that are induced by complex endovascular aortic repairs can most likely be tolerated without increasing the risk for TV-associated complications during midterm follow-up. However, aside from the herein examined geometrical changes to the TV, other factors, such as the patient’s individual anatomy 14 and the hemodynamic impact of stent-graft implantation on target organ function, 15 also need to be considered. Further studies investigating all these aspects and including long-term data are required before a recommendation can be made regarding the preferential use of a specific combination of endovascular materials during f/bEVAR.
Limitations
The main limitations of this study are the retrospective study design and the limited patient number given the length of the study period. The latter is due to the fact that only patients with a complete follow-up were included in the study. Although the lack of intra- and interobserver variability assessment represents a drawback, measurement by 2 observers in consensus still allows for sufficient validity of the results in the authors’ opinion.
Conclusion
Regarding anatomical changes during midterm follow-up after fEVAR, the present study found no difference between the 2 most commonly used types of BSGs. Both the V12 and the BeG stent-grafts adapt to the TV anatomy over time. Furthermore, no clear relationship of the anatomical changes with TV-related complications was found, suggesting that small to moderate changes of the TV anatomy can be tolerated. The type of main device also influences the TV anatomy due to different degrees of stiffness/conformability.
Supplemental Material
19-0540_supplemental_material – Supplemental material for Changes in Target Vessel Anatomy Following Fenestrated Endovascular Aneurysm Repair: Midterm Results
Supplemental material, 19-0540_supplemental_material for Changes in Target Vessel Anatomy Following Fenestrated Endovascular Aneurysm Repair: Midterm Results by Paula R. Keschenau, Christina Sattler, Tanja Berger, Drosos Kotelis, Michael J. Jacobs and Johannes Kalder in Journal of Endovascular Therapy
Footnotes
Authors’ Note
Preliminary results to this work were presented at the 33rd German Society of Vascular Surgery Annual Meeting (September 28, 2017; Frankfurt, Germany).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Johannes Kalder is a proctor for Cook Medical and Terumo Aortic and a consultant for Bentley Innomed.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.