
Abstract
Despite recent guideline updates on peripheral artery disease (PAD) and critical limb ischemia (CLI) treatment, the optimal treatment for CLI is still being debated. As a result, care is inconsistent, with many CLI patients undergoing an amputation prior to what many consider to be mandatory: consultation with an interdisciplinary specialty care team and a comprehensive imaging assessment. More importantly, quality imaging is critical in CLI patients with below-the-knee disease. Therefore, the CLI Global Society has put forth an interdisciplinary expert recommendation for superselective digital subtraction angiography (DSA) that includes the ankle and foot in properly indicated CLI patients to optimize limb salvage. A recommended imaging algorithm for CLI patients is included.
Keywords
Critical Limb Ischemia Global Society
The Critical Limb Ischemia (CLI) Global Society’s mission is to eliminate ischemic rest pain, promote wound healing, and prevent amputations and death due to CLI. The CLI Global Society ( www.cligobalsociety.org ) is the only professional membership-based medical society focused on advanced peripheral artery disease (PAD) and CLI and advocacy for prevention of amputation. Members are committed to raise public, patient, and health professional awareness of CLI treatments through scientific study, research, and proliferation of peer-reviewed publications to advance the field. These initiatives dovetail with the work of other medical societies around the world, such as the Global Vascular Guidelines Group on Critical Limb-Threatening Ischemia organized by the European Society for Vascular Surgery (ESVS), the Society for Vascular Surgery (SVS), and the World Federation of Vascular Societies (WFVS); the International Working Group on the Diabetic Foot; as well as other guidelines by the SVS, the American Podiatric Medical Association, the ESVS, the European Society of Cardiology, the Society for Cardiovascular Angiography and Interventions, the American College of Cardiology (ACC), and the American Heart Association (AHA).
CLI Prevalence, Prognosis, and Variability of Care
The global prevalence of PAD increased by 23.5% from 2000 to 2010 (164 to 202 million people), indicating a global pandemic of PAD.1,2 These percentages likely underestimate the true burden of disease since they are derived from community-based studies that define PAD on the basis of reduced ankle-brachial index (ABI). 3 CLI, also known as chronic limb-threatening ischemia (CLTI), is the end-stage of PAD,3–8 resulting in impaired tissue perfusion that threatens the limb. The clinical manifestations of CLI are broad, ranging from rest pain to severe ischemic ulceration or tissue gangrene of the extremities.4–8 Although CLI is widely believed to be a growing global health care problem, reliable epidemiological data are extremely limited, especially since many estimates are being extrapolated from the incidence and prevalence of intermittent claudication, amputation, and diabetes mellitus. 3 Most PAD patients remain asymptomatic, but it is estimated that up to 10% will progress to or present initially with CLI, although that percentage seems to vary widely. 3 Recent analyses estimate the prevalence and annual incidence of CLI ranging from 0.32% to 1.59% and 0.26% to 0.35%, respectively.9–11
CLI is highly prevalent in older patients with diabetes and/or chronic kidney disease 12 and is associated with high risk of amputation and mortality.9,13–15 The consequences of amputation are dire.9,14,15 For example, following an initial lower extremity amputation due to CLI, 27% of the patients will have one or more re-amputation(s) within 1 year, 16 35% will require proximal extension of the initial amputation site, 17 and 55% of those with PAD will require contralateral limb amputation within 2 to 3 years. 18 Mortality after nontraumatic amputation is also very high, with 1-year rates of 9% to 33%16,17,19,20 rising to 26% to 82% at 5 years.16,19–21
Despite the fact that rates of amputation in the general PAD population are declining, an estimated 150,000 amputations due to CLI occur annually in the United States,2,22 and primary amputation continues to be first-line therapy for CLI at some institutions, with an average rate of ~20%.9,13–15,23 Surprisingly, of the patients who undergo primary amputation, 73% do not have diagnostic angiography 23 and 54% receive no revascularization attempts prior to the amputation. 24 This trend is also seen in Europe; researchers there have noted that 37% of the amputated CLI patients had not undergone angiography or revascularization during their index hospital stay or in the 2 years prior. 25 Thus, the contemporary management of patients with CLI is still highly variable.9,14,15,24
Diagnosis, Treatment Urgency, and Limb Salvage in CLI Patients
Briefly, CLI is diagnosed as a condition characterized by chronic (≥2 weeks) ischemic rest pain, nonhealing wounds/ulcers, or gangrene in one or both legs attributable to objectively proven PAD.4–8 PAD is objectively determined by clinical history, physical examination, ABI, toe-brachial index (TBI), transcutaneous oxygen pressure, or skin perfusion pressure.4–8 Supplementary parameters, such as absolute ankle and toe pressures and pulse volume recordings, may also be used to determine significant PAD.4,5,8 However, recent evidence suggests that there is substantial heterogeneity in preintervention ABIs among patients undergoing revascularization for CLI.6,26 The discrepancy between ABI results and clinical diagnosis calls into question the utility of ABIs in the CLI population.6,26 More importantly, TBI should be measured to diagnose patients with suspected PAD when the ABI is >1.40 (noncompressible). 6 A TBI ≤0.70 is abnormal and suggestive of PAD. Patients with diabetes or advanced chronic kidney disease have a high incidence of noncompressible ankle and pedal arteries. Therefore, TBI assessment allows for the diagnosis of PAD in these patients with noncompressible arteries who have history or physical examination findings suggestive of PAD.6,8
As recently reviewed,
6
guideline changes have made great strides in addressing the variability of CLI treatment and highlighting the urgency to prevent tissue and limb loss. For example, the 2016 AHA/ACC guideline on the management of patients with lower extremity PAD
8
released an impactful update with a Class I recommendation stating that: “An evaluation for revascularization options should be performed by an interdisciplinary care team before amputation in the patient with CLI. Patients with CLI should be evaluated by an interdisciplinary care team. Before amputation, evaluation generally includes imaging for assessment of revascularization options [eg, duplex ultrasonography, computed tomography angiography (CTA), magnetic resonance angiography (MRA), or catheter-based angiography]. The objective of this strategy is to minimize tissue loss and preserve a functional limb with revascularization.”
In addition, the joint guidelines of the SVS, ESVS, and WFVS also state that “no patient with suspected CLI [chronic limb-threatening ischemia] who is a suitable candidate for limb salvage should be denied revascularization without first undergoing complete diagnostic angiography that includes the ankle and foot.” 3
Because timely diagnosis and treatment are essential to preserve tissue viability in CLI, the 2016 AHA/ACC guidelines also indicate that it is often most effective and expeditious to pursue invasive angiography with endovascular revascularization directly without delay and additional noninvasive imaging. 8 In certain clinical settings, quality noninvasive imaging studies for anatomical assessment (duplex, CTA, or MRA) may not be available because of lack of local resources or expertise. 8 In addition, there are clinical scenarios in which noninvasive studies for anatomical assessment may be perceived to confer greater risk to the patient than invasive angiography (eg, patient with advanced chronic kidney disease for whom MRA contrast agent is contraindicated or where the contrast dose for invasive angiography would be lower than that required for CTA). 8 Furthermore, these anatomical examinations may identify suprapopliteal artery disease and aid in access planning for angiography and revascularization, but the resulting images have limited quality for infrapopliteal arteries (Figure 1). Thus, the evaluation of infrapopliteal and below-the-ankle artery disease will commonly require digital subtraction angiography (DSA).
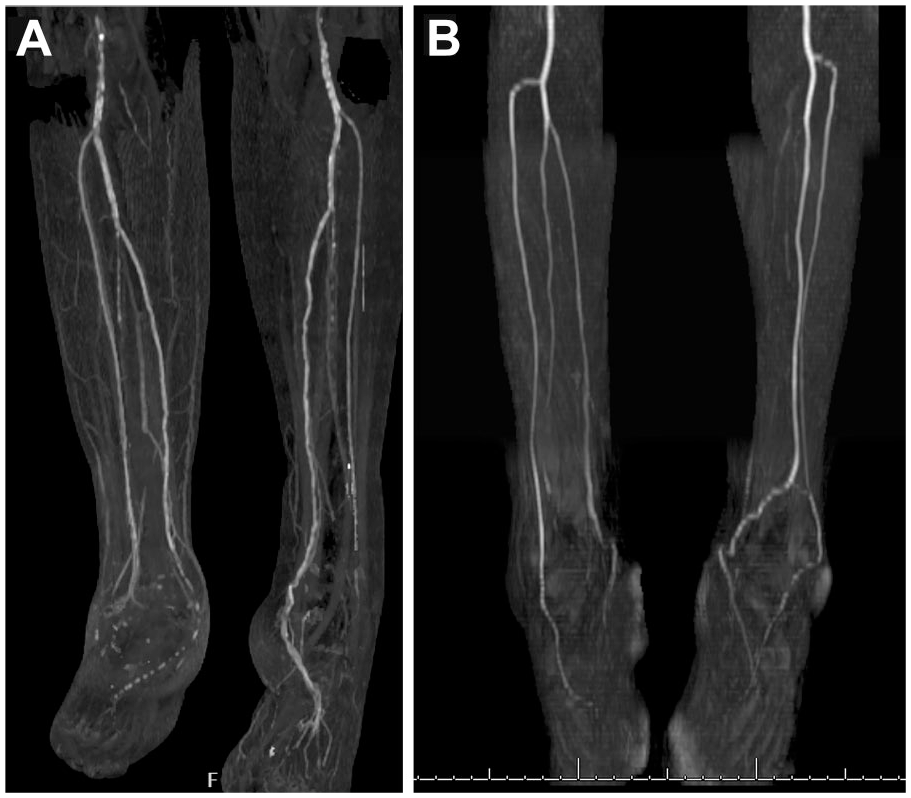
Limitations of computed tomography angiography (CTA) and magnetic resonance angiography (MRA) in below-the-knee vessels. (A) CTA imaging of tibial vessels is limited due to calcification. (B) MRA without contrast demonstrates lack of tibial resolution.
First-Line CLI Treatment Is Limb Preservation Not Primary Amputation
Finally, the term CLI implies chronicity and should be distinguished from acute limb ischemia (ALI), and as such, primary amputation is rarely the first line of treatment for CLI. Primary amputation may only be appropriately indicated for Rutherford category III ALI with an emergent unsalvageable limb (complete loss of motor and sensory function) and a proper vascular specialist assessment 8 ; however, even for ALI, if pain can be controlled and there is no evidence of motor dysfunction, infection, or rigor of the limb, amputation may be deferred if this meets with the patient’s goals. 8 In addition, recent ALI treatment guidelines from the ESVS also indicate that DSA is the standard investigation for ALI since it can delineate etiology and offers the advantage of allowing treatment in the same setting. 27
There is urgency to proceed with treatment of CLI patients as well, but this does not justify proceeding with a primary amputation prior to an interdisciplinary evaluation and a consideration of a properly acquired DSA that includes the ankle and foot. In addition, a recent study showed the average time to revascularization for a CLI patient after the first presentation is 9 days. 9 This is unacceptable when this disease has such high morbidity and mortality.
Expert Recommendation Statement to Optimize Limb Salvage
The CLI Global Society believes that the following recommendations may help reduce the incidence of primary amputation in the CLI population, resulting in better outcomes and lower burden on society.
Primary amputation should not be the first line of treatment for CLI unless there are mitigating circumstances (eg, life-threatening sepsis, intractable infection, extensive gas gangrene, bedridden status, severe dementia, or tissue loss/necrosis beyond salvage).
Ideally, an interdisciplinary specialty care team should determine if a CLI limb is salvageable.
DSA that includes the ankle and foot in properly indicated CLI patients should be utilized to further delineate a salvageable limb prior to amputation. The Society’s DSA algorithm detailed below (Figure 2) should be used in properly indicated CLI patients. This DSA algorithm in conjunction with an interdisciplinary specialty team evaluation can prevent unnecessary amputations or minimize the amputation level in CLI patients.
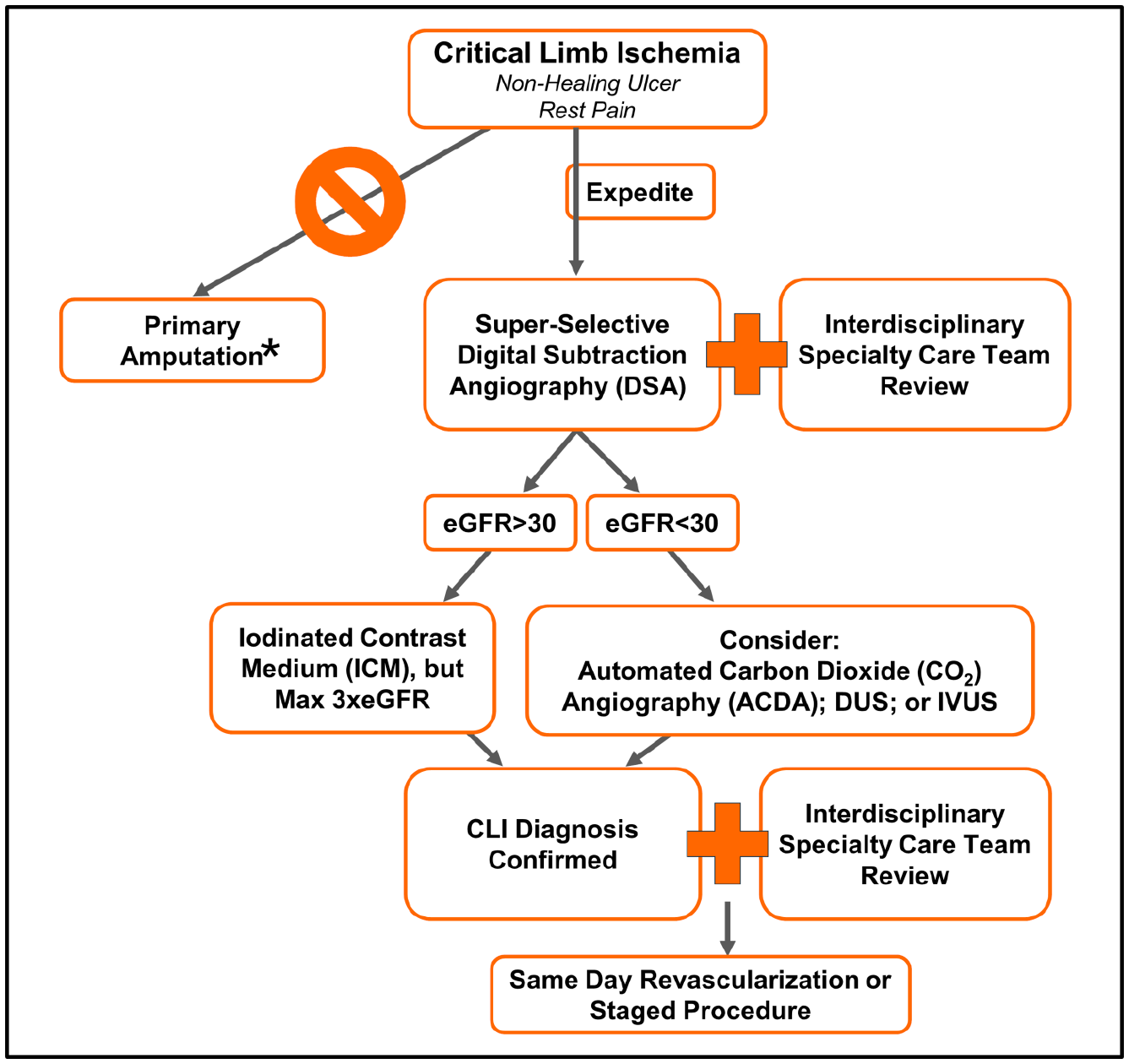
Digital subtraction angiography (DSA) algorithm for critical limb ischemia (CLI) patients. *Primary amputation should not be the first line of treatment for CLI unless there are mitigating circumstances (eg, life-threatening sepsis, intractable infection, extensive gas gangrene, bedridden status, severe dementia, or tissue loss/necrosis beyond salvage). DUS, duplex ultrasonography; eGFR, estimated glomerular filtration rate; IVUS, intravascular ultrasound.
DSA Algorithm for CLI Patients
Modern preprocedural imaging includes noninvasive modalities, such as CTA, contrast-enhanced MRA, quiescent-interval single-shot MRA, and high-frequency duplex ultrasonography, as well as invasive DSA.28–33 Although all of these modalities are appropriate in evaluating the large-diameter supragenicular arteries, the small-caliber below-the-knee outflow arteries are best evaluated using superselective DSA with the catheter positioned just above the infrapopliteal trifurcation (Figure 3).28–31 However, keep in mind that the collateral filling of an anterior tibial artery occlusion at the ostium via deep femoral artery collaterals may be missed in some cases, and the entire leg starting with the femoral bifurcation must be examined. Furthermore, to visualize pedal arteries under DSA, a 0.018-inch catheter (typically a crossing catheter with a 0.014-inch lumen) should be placed as distally as possible in the tibial arteries and/or the inframalleolar vessels.28,29,31 Proper imaging of the pedal arteries is also important since pedal arch flow is a positive prognostic marker for limb salvage and survival in patients with CLI. 34
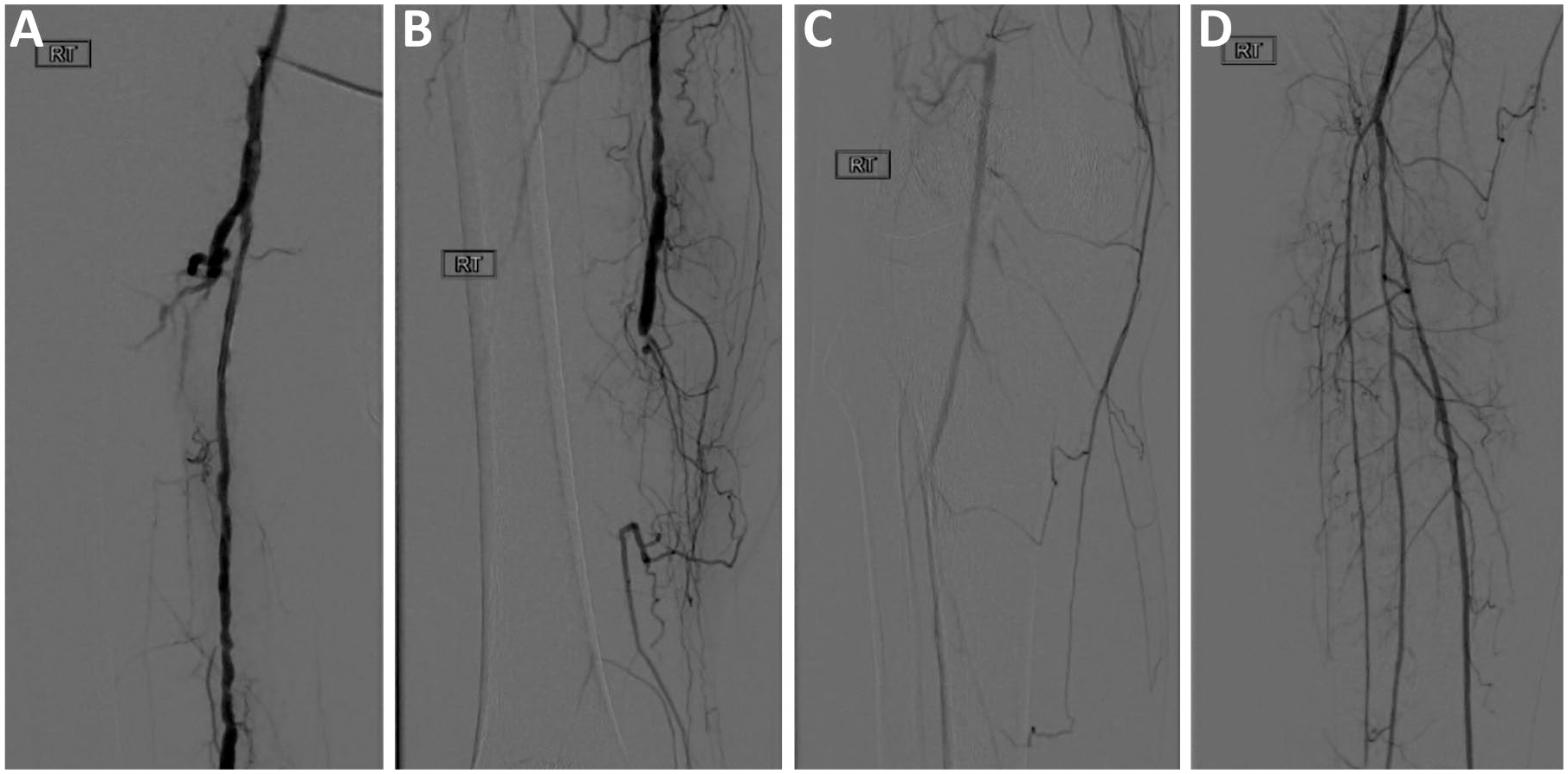
Accurate digital subtraction angiography (DSA) visualization is critical in making the right treatment decision for a critical limb ischemia (CLI) patient. (A) Nonselective DSA of the superficial femoral artery (SFA). (B) DSA of the SFA-popliteal artery showing the proximal occlusion and distal reconstitution. (C) Example showing the limitations of DSA visualization of distal arteries without selective angiography vs (D) with selective DSA, which can determine the anatomical configuration of arteries not visualized beyond the occlusion.
The risks of DSA should be carefully considered for patients with advanced chronic kidney disease (stages 3 and 4 and predialysis). Initial evaluation with duplex ultrasonography and possibly noncontrast MRA is recommended to aid in pre-angiography planning and to decrease the likelihood of contrast-induced nephropathy.29,35 The use of CO2 with an automated injector can provide excellent imaging for both diagnostic and therapeutic purposes in CLI patients, allowing operators to minimize radiation and contrast exposure.29,36,37 However, this may be true only for proximal tibial arteries; thus, general anesthesia should be considered in order to eliminate motion artifacts and obtain sufficient distal imaging quality.
Summary of Key Points
Primary amputation should not be the first line of treatment for CLI unless there are mitigating circumstances.
Ideally, an interdisciplinary specialty care team should determine if a CLI limb is salvageable.
DSA is considered the standard investigation for CLI to optimize limb salvage.
DSA that includes the ankle and foot in properly indicated CLI patients can further delineate a salvageable limb prior to amputation.
The risks of DSA should be carefully considered for patients with chronic kidney disease.
Conclusion
Despite recent guideline updates on PAD and CLI treatment, standard of care for CLI is still not uniform. As a result, contemporary management of CLI patients is highly variable, resulting in primary amputations prior to exploring options for interdisciplinary specialty evaluation and imaging assessment for revascularization. More important, CLI patients with below-the-knee disease can fail to receive definitive imaging evaluations. Thus, this expert recommendation statement from the CLI Global Society calls for a true interdisciplinary assessment prior to an amputation, using selective DSA as the definitive imaging modality, especially for distal occlusive disease associated with CLI.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors are members of the CLI Global Society. Jihad A. Mustapha is a consultant to BD/Bard, Boston Scientific, Cardiovascular Systems, Medtronic, Philips Healthcare, and Terumo. Fadi A. Saab is a consultant to BD/Bard, Boston Scientific, Cardiovascular Systems, Medtronic, Philips Healthcare, and Terumo. Brad J. Martinsen is an employee of and holds stock in Cardiovascular Systems. Constantino S. Pena is a consultant to BD/Bard, Abbott Vascular, Boston Scientific, Philips Healthcare, and Cook Medical. Richard F. Neville is a member of the Scientific Advisory Boards of W.L. Gore & Associates, Cormatrix, Graftworx, and Tissue Analytics; he holds equity investment in Graftworx and Tissue Analytics; and he received research grants from W.L. Gore & Associates and Medtronic. Robert Lookstein is a consultant to and member of the Scientific Advisory Boards of Boston Scientific and Medtronic. Thomas Zeller received honoraria for speaking or moderating educational programs from Abbott Vascular, Biotronik, Boston Scientific, Cordis, Cook, Medtronic, Shockwave Medical, Spectranetics, Veryan/Novate, Phillips/Volcano, and W.L. Gore & Associates; he is a consultant to Boston Scientific, Medtronic, W.L. Gore & Associates, Intact Vascular, Spectranetics, and Veryan/Novate; and he holds equity investment in QT Medical. Michael R. Jaff is a noncompensated advisor to Abbott Vascular, Biotronik, Boston Scientific and a consultant to Medtronic Vascular, Micell, Philips/Volcano, Venarum, and Vactronix; he holds an equity investment in eFemoral, PQ Bypass, Gemini, Vascular Therapies, Primacea, and Embolitech. Barry Katzen is a member of the Scientific Advisory Boards of Boston Scientific, W.L. Gore & Associates, and Philips Healthcare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the CLI Global Society ( www.cligobalsociety.org ), which receives funding support from Abbott Vascular, BD/Bard, Boston Scientific, Cardiovascular Systems, Inc, Medtronic, and Philips Healthcare.