
Abstract
Purpose:
To evaluate the safety and feasibility of the in situ needle fenestration (ISNF) technique for reconstruction of the left subclavian artery (LSA) during thoracic endovascular aortic repair (TEVAR) of complicated aortic arch pathologies.
Materials and Methods:
A retrospective review was conducted from January 2014 to December 2019 of 50 patients (mean age 60.2±11.1; 45 men) who underwent ISNF to revascularize the LSA during TEVAR. Twenty-one of the patients also required revascularization of the left common carotid artery (LCCA; n=19) and innominate artery (IA; n=2) using physician-modified in vitro fenestration. Overall, 73 supra-aortic branches were targeted for revascularization.
Results:
ISNF was successful in 48 patients (96%); one LSA could not be stented and a tortuous LSA prevented the needle from fenestrating the graft. No perioperative major adverse event occurred. There were no type I and 4 type III endoleaks (8%), 3 of which occurred among the first 20 cases. Types II and IV endoleaks were found in 3 (6%) and 6 (12%) cases, respectively; all disappeared during a median follow-up of 15 months (range 3–66). One death (2%) occurred within 12 months due to cerebral hemorrhage. Two patients (4%) required open reinterventions at 6 and 62 months.
Conclusion:
ISNF for revascularization of the LSA during TEVAR seems to be feasible with acceptable midterm outcomes. The learning curve and evolving patient selection criteria affected technical success, complications, and the need for reinterventions. Long-term durability requires further evaluation.
Keywords
Introduction
In the endovascular era, thoracic endovascular aortic repair (TEVAR) has become the first-line therapeutic modality for descending thoracic aortic diseases. 1 As experience has accumulated and the devices have been refined, the indications for TEVAR have expanded. Thanks to the development of the chimney technique and fenestrated/branched stent-grafts,2–6 TEVAR is now more widely used for arch pathologies with insufficient landing zones. However, total endovascular treatment of aortic arch pathologies is still challenging, and long-term results are awaited.
In situ fenestration (ISF) using a retrograde needle (ISNF) or energy-based device (radiofrequency or laser) has become a useful technique first described by McWilliams et al 7 for revascularizing the supra-aortic branches. After deploying the main aortic stent-graft, ISF is performed followed by placement of covered or uncovered bridging stents through the fenestrations to preserve the blood supply to the branch vessels. Recent studies mainly focused on ISF using a laser or radiofrequency device8–11; ISNF has been less frequently reported, with <200 cases recorded in the English-language literature up to now.12,13
This report provides midterm outcomes of ISNF for left subclavian artery (LSA) revascularization using a specially designed puncture needle 14 in a selected cohort of patients with challenging aortic pathologies involving the outer curve of the arch in zone 2.
Materials and Methods
Study Design and Patient Sample
A retrospective review was conducted of the 344 patients who underwent TEVAR with ISNF or ex vivo physician-modified stent-graft fenestration (PMSGF) between January 2014 and December 2019. During this time, an interdisciplinary board composed of endovascular and cardiovascular surgeons, radiologists, and anesthesiologists was responsible for comprehensively evaluating each patient to decide treatment modalities. Patients who met the following 2 criteria were considered suitable candidates for ISNF reconstruction of the LSA in TEVAR. The first criterion was the presence of an aortic dissection, penetrating aortic ulcer, aneurysm, or pseudoaneurysm on the outer curvature of the arch close to (<15 mm) or involving the LSA, where endoleak would be more likely to occur if the chimney or PMSGF techniques were used. The second criterion was a >45° takeoff angle of the LSA from the arch and no significant tortuosity in the proximal LSA. If the left common carotid artery (LCCA) and innominate artery (IA) were located in the landing zone but at some distance from the lesion (eg, an entry tear located at the inner curve opposite the LCCA/IA orifices), ISNF would be used for the LSA and the PMSGF technique for the LCCA/IA. When the LSA was located in the landing zone and the lesion involved only the concavity of the arch, PMSGF was preferentially utilized.
The exclusion criteria were (1) pathologies involving the ascending aorta; (2) concomitant cardiac pathologies that necessitated open chest surgery; (3) other anatomical formations not suitable for TEVAR, such as severe tortuosity and stenosis in the access arteries or a very large transaortic landing zone diameter severely limiting device use; (4) a dominant left vertebral artery originating from the aortic arch; or (5) renal insufficiency or severe cardiopulmonary diseases contraindicating general anesthesia.
Based on these criteria, 50 patients (mean age 60.2±11.1 years; 45 men) were selected to undergo ISNF to preserve the LSA; the other 294 patients had PMSGF-assisted TEVAR. Characteristics of the 50 patients are presented in Table 1.
Baseline Characteristics of the 50 Patients in the Study. a
Abbreviations: COPD, chronic obstructive pulmonary disease.
Continuous data are presented as the mean ± standard deviation; categorical data are given as the count (percentage).
The institutional review boards of Fuwai Hospital and Second Xiangya Hospital approved the ISNF procedure, and informed consent was obtained from all the patients and their relatives.
ISNF-Assisted TEVAR
The Ankura stent-graft (Lifetech Scientific Co., Ltd, Shenzhen, China) was selected for most procedures because its expanded polytetrafluoroethylene (ePTFE) membrane was reportedly easier to puncture and dilate than polyester fabrics, resulting in larger, better quality, elliptical fenestrations. 15 One Valiant stent-graft (Medtronic, Inc, Minneapolis, MN, USA) and a Zenith stent-graft (Cook Medical, Bloomington, IN, USA) were used in 2 patients.
An adjustable needle catheter (Lifetech Scientific Co, Ltd) with 3 puncture depths and a compliant balloon at its tip was delivered through a Fustar steerable sheath (Lifetech Scientific Co., Ltd) to the ostium of the LSA as described previously. 14 The balloon was inflated to fix the sheath and needle catheter in the correct perpendicular orientation, and the needle was deployed to puncture the graft (Figure 1). This device was used in all patients except the first, who underwent ISNF using a homemade tool.
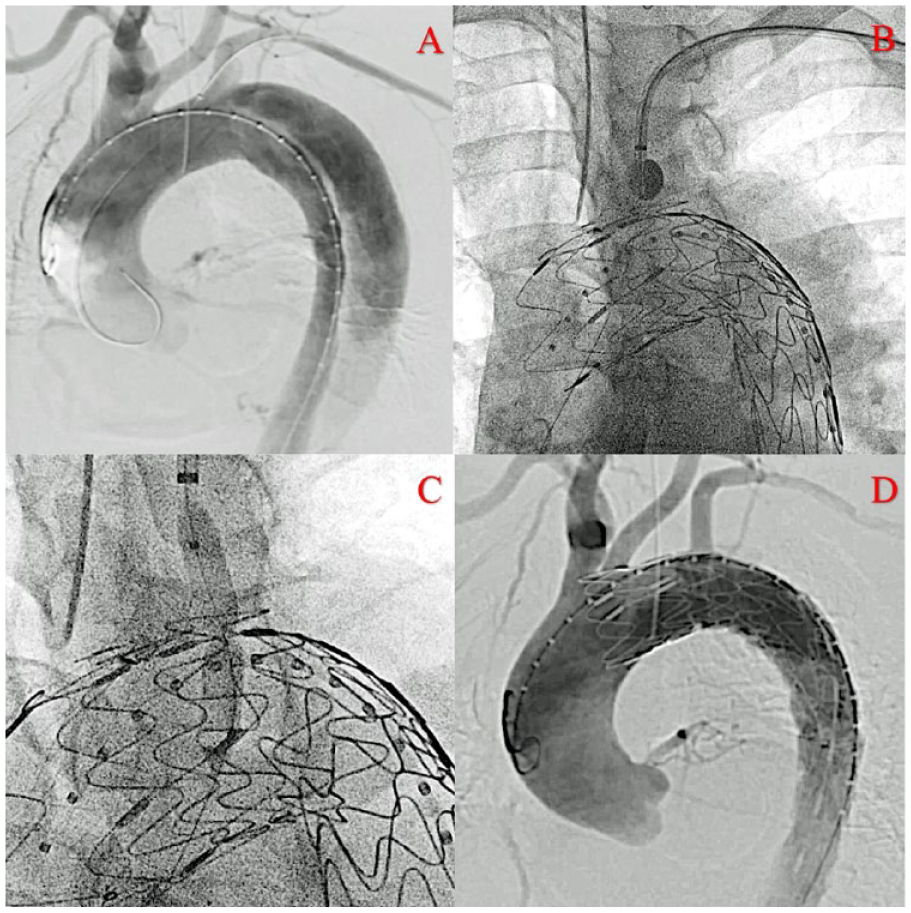
(A) The digital subtraction angiogram shows a proximal entry tear of an aortic dissection very near the left subclavian artery (LSA). (B) After the aortic stent-graft was implanted at the planned position, the puncture needle was introduced to the orifice of the LSA and the balloon inflated to fix the alignment of the needle with the graft. (C) A balloon catheter of comparable size was employed to dilate the fenestration. (D) The completion angiogram shows occlusion of the proximal entry tear while the LSA was successfully preserved.
Viabahn covered stents (W. L. Gore & Associates, Flagstaff, AZ, USA) or an Express LD bare stents (Boston Scientific Corp, Marlborough, MA, USA) were used as bridging stents to the target branches. Covered stents were used when arch pathologies involved the branch vessels, elevating the risk of endoleak. A Fustar steerable sheath was generally used to deliver the bridging stents through the fenestrations.
All patients were administered general anesthesia in a hybrid operating suite. The common femoral artery was exposed surgically or punctured percutaneously and sealed using a Perclose ProGlide suture device (Abbott Vascular, Santa Rosa, CA, USA); the left brachial artery was exposed surgically.
First, the puncture device was introduced through an 8-F or 9-F, 55-cm-long Fustar steerable sheath from the left brachial access and advanced retrogradely to the orifice of the LSA. Then, an angiography catheter was introduced from the femoral access into the aorta. A digital subtraction angiogram (DSA) was performed to evaluate the aortic lesion. The aortic stent-graft was introduced to the arch from the femoral access and deployed at the planned landing zone, intentionally covering the LSA. The balloon on the puncture device in the LSA was inflated, and the needle was deployed at the center of the LSA orifice, a crucial step to ensure a precise graft puncture (Figure 1). Then, the guidewire was passed through the newly created hole into the aortic lumen. The hole was serially dilated beginning with a 3-mm-diameter balloon (Sterling PTA Balloon; Boston Scientific Corp.) followed by incrementally larger balloons (Advance Low-Profile PTA Balloon; Cook Medical) with diameters of 5 to 8 mm. The largest balloon was selected to be 1 or 2 mm smaller than the bridging stent diameter to allow a more secure connection between the fenestration and the stent. After balloon expansion of the fenestration, a Fustar steerable sheath or a long sheath (Cook Medical) was introduced retrogradely from the brachial artery access to protect the bridging stent, bare or covered, as it was navigated across the fenestration and deployed with the proximal 10-mm segment protruding into the aortic lumen and the distal end fixed in the LSA. Finally, the stent was dilated with a comparably sized balloon if necessary, and the completion DSA was performed to check the result.
For 21 patients with the LCCA (n=19) and IA (n=2) in the landing zone, the PMSGF technique was used as previously described 16 to modify an unsheathed stent-graft on a back table. These fenestrations were typically 0 to 10 mm larger in diameter than the target vessels. In the current series, the Ankura stent-graft was fenestrated according to the 3-dimensional morphology of the lesion captured in the first DSA. After preparation, the fenestrated stent-graft was deployed at the planned landing zone at the arch to cover both the lesion and the LSA. Finally, ISNF as described above was used to revascularize the LSA from the brachial access, and the completion DSA was performed.
Early in our experience, the decision to bridge the fenestrations to the LCCA/IA depended on the correct position of the fenestration marker. When the marker was not in a good location or perfusion of the LCCA/IA became diminished, which might indicate imprecise orientation of the fenestration, stenting was performed to keep these important branches patent. As our experience increased, all fenestrations were routinely stented if possible.
If necessary, patients were prescribed antiplatelet drugs, antihypertensive drugs, and beta-blockers postoperatively. Follow-up imaging for each patient was scheduled at 3, 6, and 12 months and annually thereafter.
Statistical Analysis
Continuous data are expressed as the mean ± standard deviation or median (minimum-maximum) depending on the normality of the distribution. Cumulative survival was analyzed using the Kaplan-Meier method. Analyses were conducted using SPSS software (version 23.0; IBM Corporation, Armonk, NY, USA). GraphPad Prism (version 8; GraphPad Software, San Diego, CA, USA) was used to construct graphical representations of the data.
Results
Seventy-one fenestrations, including 50 ISNF and 21 PMIVF, were planned for 73 target vessels in 50 endografts (Table 2). Technical success, defined as endovascular exclusion of the aortic arch pathology and preservation of the LSA using ISNF, was achieved for 48 patients (96%). One of the failures was due to an inability to stent the LSA despite satisfactory fenestration of the ePTFE membrane. A bailout chimney stent-graft was performed to salvage the LSA, and the patient recovered uneventfully. The other case involved failure to make the fenestration owing to a tortuous LSA and type III arch. As the right vertebral artery was dominant, the fenestration was abandoned and the LSA was sacrificed. Nonetheless, the patient lived uneventfully without any complications over 24 months of follow-up. In a third patient, the LSA was not intended to be stented after successful ISNF owing to financial problems. In this case, the fenestration was dilated larger than usual; perfusion across the fenestration into LSA has been well maintained for the 11 months of follow-up.
Procedural and 30-Day Data on the 50 Procedures. a
Abbreviations: IA, innominate artery; ISNF, in situ needle fenestration; LCCA, left common carotid artery; LSA, left subclavian artery; PMSGF, physician-modified stent-graft fenestration.
Continuous data are presented as the mean ± standard deviation or median (minimum-maximum); categorical data are given as the count (percentage).
Death, stroke, paraplegia, conversion.
Thus, except for the 1 failure to reconstruct an LSA, 72 of 73 target vessels (99%) were preserved, including the LSA salvaged with a chimney graft. In all, 48 stents were used to bridge the fenestration to the LSA: 26 covered stents (25 with ISNF and 1 chimney) and 22 bare stents. In addition, 15 bridging stents (8 covered and 7 bare) were used to preserve the LCCA (Figure 2), while 6 LCCAs and 2 IAs had no bridging stent. The mean fluoroscopy times, defined as the period of time between the first and the last angiography during a procedure, were 28 and 39 minutes for ISNF-assisted TEVAR only and the combined ISNF and PMSGF cases, respectively.
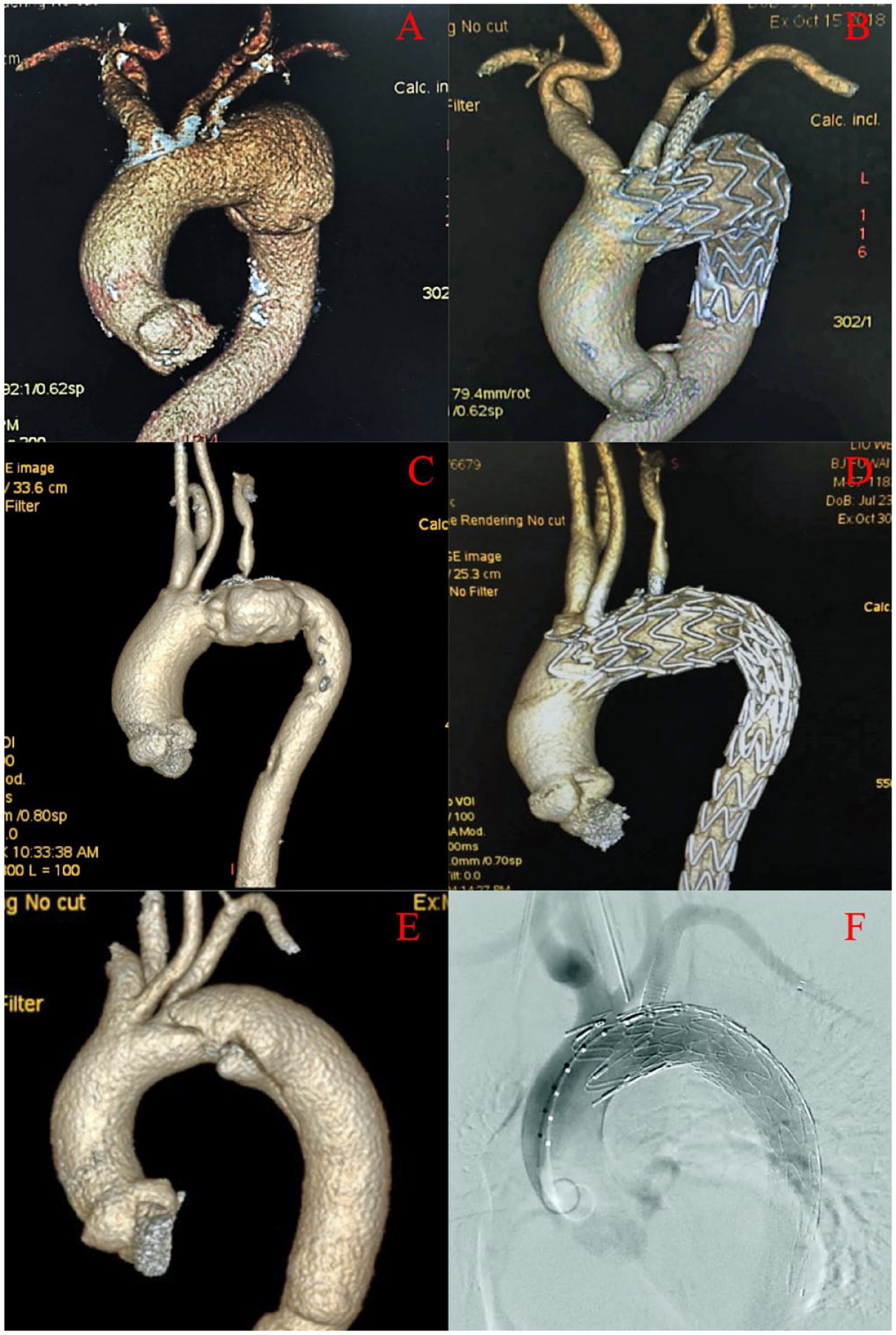
Three examples of in situ needle fenestration (ISNF) for the left subclavian artery (LSA) combined with ex vivo physician-modified stent-graft fenestration (PMSGF) to revascularize the left common carotid artery (LCCA) and innominate artery (IA). (A and B) A patient with a 65-mm aortic arch aneurysm involving the LSA orifice. (C and D) A patient with an aortic arch pseudoaneurysm involving both the LCCA and the LSA. (E and F) A patient with a bovine aortic arch who had an aortic dissection involving the LSA that required PMSGF for both the IA and LCCA (a 10×20-mm scallop) and ISNF for the LSA.
No perioperative major adverse event, such as death, stroke, or paraplegia, occurred within 30 days. Bilateral brachial blood pressure showed no significant change perioperatively, and the brachial incisions healed well. The pulses of the left radial arteries remained normal in all patients except the one failure of LSA reconstruction.
Type III endoleak at the LSA level was seen in 4 patients (8%), 3 of which occurred during the first 20 cases. Types I, II, and IV endoleaks occurred in 0, 3 (6%), and 6 (12%) patients, respectively. In these patients, antiplatelet drugs were stopped and blood pressure was controlled more strictly until the endoleak disappeared. For the endoleak patients with LCCA stents, antiplatelet drugs were stopped 3 months postoperatively and the stent was monitored closely with duplex ultrasound. All type II and type IV endoleaks disappeared during a median follow-up of 15 months (range 3–66). One patient with a type III endoleak had open arch replacement 6 months later as the dissected aorta in zone 3 remained enlarged. The 3 other patients with mild to medium type III endoleaks have been stable over 15 to 22 months of strict surveillance.
One patient (2%) died within 12 months of the operation because of sudden cerebral hemorrhage. The Kaplan-Meier survival curve is presented in Figure 3. One patient suffered a type A aortic dissection 62 months postoperatively and underwent open arch repair. According to follow-up imaging, all 72 target vessels have remained patent. There were no other stent-graft–related complications, including migration, compression, or collapse.
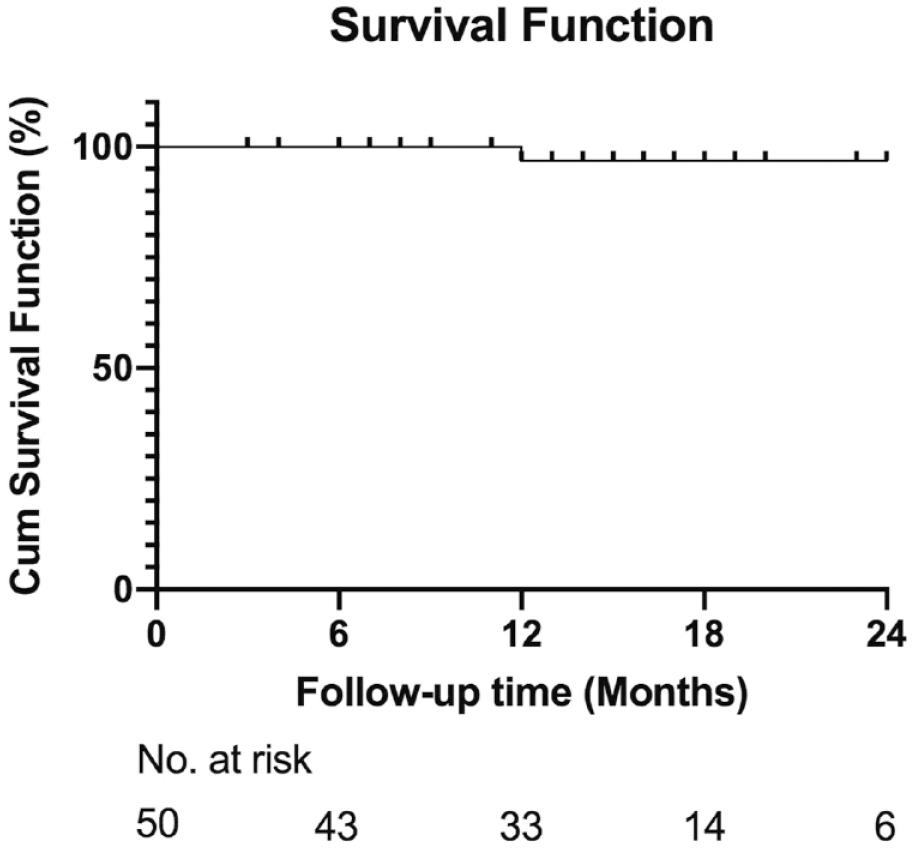
Kaplan-Meier curve for overall patient survival. The survival estimate was 96.9% (95% confidence interval 90.8% to 100.0%).
Discussion
Although open surgery remains the standard treatment option for aortic arch pathologies, the mortality and complication rates are high. The rapid development of endovascular therapies provides new treatment options to open surgery. For example, if the aortic pathology involves only the inner curve of the arch, especially in zones 2 or 3, and the upper curve is normal, open aortic repair is too stressful for these patients and may be unnecessary in the endovascular era. Compared with open surgery, total endovascular management is less traumatic and involves less blood loss and quicker recovery.
During the past 2 decades, several endovascular and hybrid techniques have evolved to preserve the supra-aortic vessels in TEVAR. PMSGF has major challenges in design, modification, and orientation and requires experienced physicians to execute it successfully. 16 Remote access via a tortuous delivery path, from the femoral artery through the abdominal and descending aorta, often means difficulties in orientation and precise fenestration alignment with supra-aortic vessels. Hence, using larger-sized fenestrations compared with the aortic branches is the common way to efficiently and accurately align the fenestration with the aortic branches. Unfortunately, larger fenestrations may impact the durability of stent-grafts and increase the possibility of type III endoleak when the lesion is too close to the target branches.8,9
Branched stent-grafts have been used with limited experience and acceptable results, but the learning curve can impact operative mortality. 17 TEVAR combined with surgical bypass of the supra-aortic arteries is feasible but usually not considered as the first option for high-risk patients because this hybrid technique increases incisions and the risk of nerve injury and stroke. 2
Three previous reports have shown that ISF appears to be a feasible and effective method for revascularizing the LSA during arch TEVAR.17–19 Three main mechanisms—needle, laser, and radiofrequency—were frequently used, and the short-term results were acceptable, with high success rates and low fenestration-related morbidity. The LSA was the most common aortic branch to receive ISF in the meta-analyzed reports, and most procedures were used in emergent bailout situations.
In the present study, 50 patients received ISNF for the LSA and the midterm results were encouraging, which indicates that ISNF might be a safe and feasible option to revascularize the LSA in challenging cases involving the outer curve of the arch. Based on our experiences, the short fluoroscopy times for ISNF only and combined ISNF and PMSGF might have contributed to the encouraging low perioperative complication rate.
Unlike chimney grafts and back table PMSGF, ISNF is not typically susceptible to endoleaks owing to the relatively smaller fenestration and the close proximity of the puncture site and the bridging stent.8–12 Besides, ISNF can be used to treat various aortic arch pathologies, even in challenging cases when the proximal lesions are very close to the branch arteries. According to our experience and others,14,20 ePTFE is considered the better choice for ISNF than polyester, although there are no long-term durability data. The anatomies of both the aortic arch and the aortic branches are not changed after ISNF-assisted TEVAR, and as a result, blood flow is physiological.
As the puncture and dilation angle make an impact on the shape and quality of fenestrations, 14 the major limitation of the ISNF is the requirement for a relatively vertical takeoff (generally >45°) of the target branch from the arch. Therefore, owing to the morphology of the aortic branches, reconstruction of the IA and the LCCA might be easier than the LSA, especially when the proximal segment of the LSA is twisted or angulated and thus susceptible to needle injury to the artery wall. However, as endovascular procedures involving the IA and LCCA have a higher risk of stroke, we recommend not using the ISNF technique for these branches during the learning curve. Similarly, even though we had experience with >300 PMSGF procedures, we used great caution to ensure the safety of our patients as our team overcame the ISNF learning curve. Hence, only 50 patients were selected for ISNF-assisted LSA revascularization from the hundreds undergoing PMSGF-assisted TEVAR at 2 large aortic centers.
In our experience, when the proximal intimal tear of an aortic dissection is very close to the branch arteries, ISNF may more likely prevent endoleak occurrence compared to the chimney or PMSGF techniques. However, type III endoleak may still occur from fabric tears or unsealed connections between the fenestration and the bridging stent. As we encountered 4 type III endoleaks in this cohort, ISNF should be cautiously utilized when the distance between the dissection tear and the LSA orifice is <3 mm, although it may be safer than PMSGF in these settings. For our team, PMSGF was used preferentially for a patient whose lesion involved only the inner arch curve, which means every ISNF patient had a lesion close to the supra-aortic branches and so were at risk for more type III endoleaks.
If the reason for type III endoleak is the disruption of the fibers surrounding the fenestration, then using covered stents for the target branches may be beneficial. However, despite incremental balloon dilation to expand the fenestration, an irregularly-shaped fenestration created by ISNF could sometimes make it difficult for a long sheath or bridging stent-graft to cross the fenestration. Therefore, a lower-profile bare stent could be used since the endoleak rate appears to be low. As we saw in one case, if it was too difficult for the stent to get through the fenestration, bailout chimney grafting could salvage the branch.
Another concern of ISNF is the lack of mature devices. Current publications regarding ISF mainly employ homemade devices, such as biopsy, hepatic, or reentry needles.12,13 The technical difficulty of using the puncture device in our study mostly depended on the experience of the surgeon, but the puncture device still requires major refinement. The development of a graft fabric that accommodates ISF would also be a plus.
Limitations
This was a single-physician experience involving highly selected patients with limited follow-up. The impact of the learning curve cannot be ruled out, particularly in terms of endoleak. The small cohort, the selection bias, and the retrospective nature of the study are shortcomings.
Conclusion
ISNF for LSA revascularization in TEVAR provides encouraging midterm results and seems to be feasible and effective after sufficient experience is amassed. Nonetheless, ISNF is an off-label technique that may affect the long-term durability of the stent-graft. In order to achieve ease of use, decrease procedure-related complications, and guarantee the safety of the ISNF process, patients should be selected carefully. The irregularly-shaped fenestration created by ISNF could result in type III endoleak when the lesion or entry tear is too close to the target branch. Improvements in equipment and technique are required to make ISNF more reliable, and data on long-term durability are needed before the technique is widely adopted.
Footnotes
Authors’ Note
This research was reported at the Veith Symposium (November 13–17, 2018, and November 19–23, 2019; New York, New York, USA); LINC (January 30–February 2, 2018, and January 22–25, 2019; Leipzig, Germany); Charing Cross (April 24–27, 2018; London, UK); and the Complex Cardiovascular Catheter Therapeutics Conference (June 17–20, 2018; Orlando, FL, USA).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation, China (No. 81870345), the Beijing Science and Technology Project (No. D171100002917004), and the Grant of CAMS Initiative for Innovative Medicine, China (NO. 2016-I2M-1-016).