
Abstract
Background:
Drug penetration into the deeper arterial wall of heavily calcified lesions is one of the limitations of drug-coated balloons and drug-eluting stents in vascular interventions. The Temporary Spur Stent (TSS) system is characterized by a self-expanding nitinol stent that is uniformly covered in radialspikes, which, when coated, should allow a deeper penetration and longer retention of the drug into the diseased artery walls by penetrating through the calcified plaques.
Materials and Methods and Results:
Uncoated TSS and paclitaxel (PTX)-coated TSS systems have been deployed in porcine peripheral arteries. Four weeks after the deployment of uncoated TSS systems, no adverse vascular remodeling or neointimal formation in the treated vessel segments were noticed. PTX-coated TSS systems transferred 9%±7% of the drug that was on the device to the targeted vessel area (196±163 ng PTX/mg arterial tissue) and the addition of the fluorescent dye Nile red to the coating showed that the spikes promote the transfer of the coating to the deeper layers of the vessel wall. The PTX-coated TSS systems showed a significant reduction in neointimal proliferation compared to the uncoated TSS systems: quantitative angiography showed a vessel diameter stenosis of 37.2%±11.0% and 16.4%±8.8% 4 weeks after the treatment with uncoated and PTX-coated TSS systems, respectively.
Conclusion:
The treatment with the TSS system was well tolerated and the spikesfacilitate the transfer of the coating into deeper layers of the vessel wall. Moreover, the PTX-coated TSS systems effectively inhibit neointimal proliferation.
Introduction
Endovascular treatment of peripheral artery disease (PAD) with percutaneous transluminal angioplasty (PTA) followed by drug-coated balloons (DCB) or drug-eluting stents (DES) has increasingly become standard therapy for lesions above the knee. 1 In contrast to the treatment of coronary artery disease, where DES coated with sirolimus or its analogues show excellent results in the short and medium terms, 2 treatment of PAD with paclitaxel (PTX)-coated devices, especially DCB, demonstrates improved primary patency when compared to PTA alone. In contrast to coronary vessels, peripheral vessels are subject to mechanical stress by the surrounding musculature and additional deformations in the area of the joints. 3 This is where the advantages of DCB become apparent, as they allow for (a) homogeneous drug transfer to the vessel wall, (b) capability to treat vessels with small diameter or tortuous vessels and vessel segments subjected to mechanical forces, which might lead to stent deformation or fracture, and (c) short-term drug delivery without leaving an implant in the vessel. 4 The implantation of stents may stabilize the initial result but DES may increase the risk of chronic inflammation and late thrombosis requiring the use of a long-term antiplatelet therapy. 5
Treatment of lesions of the superficial femoral artery (SFA) with DCB demonstrates improvement of short- and long-term patency compared with PTA alone. 1 A recent discussion on the safety of PTX-coated devices based on a meta-analysis 6 has been challenged, and further data suggest that there is not a safety concern.7,8 Positive clinical data have also recently been published for degenerated dialysis shunts. 9 However, data on the treatment of below the knee (BTK) vasculature have so far been contradictory. Several smaller studies from centers with well-defined wound care programs reported a significant benefit for DCB treatment BTK.10 –12 In contrast, other randomized multicenter studies did not show an advantage in terms of restenosis or safety parameters such as amputation.13,14
The reasons for the contradictory results of DCB in the BTK indication are not yet fully understood. Technical limitations of DCB include the loss of the drug during passage to the lesion site, delivery of an efficacious therapeutic dose of drug to the targeted area and limited deposition of drug to reside into deeper layers of the arterial wall. Treatment of heavily calcified lesions remains challenging with the use of both DCB and DES due to limited penetration of the antiproliferative drug through the vessel wall in the presence of vascular calcium deposits. 15 Vessel preparation such as atherectomy may be performed in the cases of severe calcified vessel segments prior to DCB or DES deployment, in order to remove part of the atherosclerotic plaque and to promote deeper drug penetration into the vessel wall. However, the possibility of distal embolization and the increased overall procedural time, and cost are 3 of the major disadvantages of atherectomy devices.
One method to improve local drug delivery is through anatomically adapted and escalated delivery modality into the vessel wall. The Temporary Spur Stent (TSS; Reflow Medical, San Clemente, CA, USA) system is a novel percutaneous transluminal device designed to be released and removed after treatment of calcified atherosclerotic vessel segments. The TSS, a temporary self-expanding nitinol stent system, is uniformly covered with radial nitinol spikes in a length that can range between 0.5 and 5 mm that can penetrate through the calcified plaques and reach the vessel wall. The capability of the spikes to enter the calcified lesion thanks to their sharpness and stiffness and to reach the different layers of the underlying vessel wall is influenced by the thickness of the calcification and the pressure used to dilate the Spur stent. The spikes, when coated with an antiproliferative drug, may allow deeper penetration, increased uptake and longer retention of the drug into the diseased artery walls. The first generation of the TSS was the temporary Spur Stent, which was loaded in an outer shaft and released when the target area was reached. In the second generation of the device, the spur is mounted on a balloon and loaded together in the outer shaft used for the delivery of the device. Once the spur and the balloon have been deployed at the target location, the balloon is inflated to promote luminal dilation, penetration of the spikes and to ensure full contact of stent struts with the vessel wall. Following treatment, in the same procedure the TSS will be retracted and no permanent implant will remain in the vessel. To prevent neointimal proliferation, the spur and the balloon may be coated with antiproliferative drug.
The uncoated TSS was clinically investigated in combination with a commercially available DCB in the DEEPER Trial in patients with BTK disease (ClinicalTrials.gov Identifier: NCT03807531). The 2-step procedure proved to be feasible, effective and well tolerated but was somewhat inconvenient as 2 devices were needed. Consideration was given to developing a drug-coated version of the device. A drug-coated TSS may promote the transfer of the drug deeper into the vessel wall, without the need of using a second drug-coated device. The aim of the present preclinical trials was to investigate the safety of uncoated TSS as well as drug transfer to and into the vessel wall, andinhibition of neointimal proliferation of drug-coated TSS in peripheral porcine arteriesusing the first- and second-generation TSS system coated with different dye and drug formulations.
Materials and Methods
The deployment of the TSS system (Spur stent 4.0×60 mm) and its effect in peripheral arteries was analyzed in vivo in an experimental porcine model. An overview on the studies is given in Table 1.
Overview of the In Vivo Studies Performed With the TSS Systems.
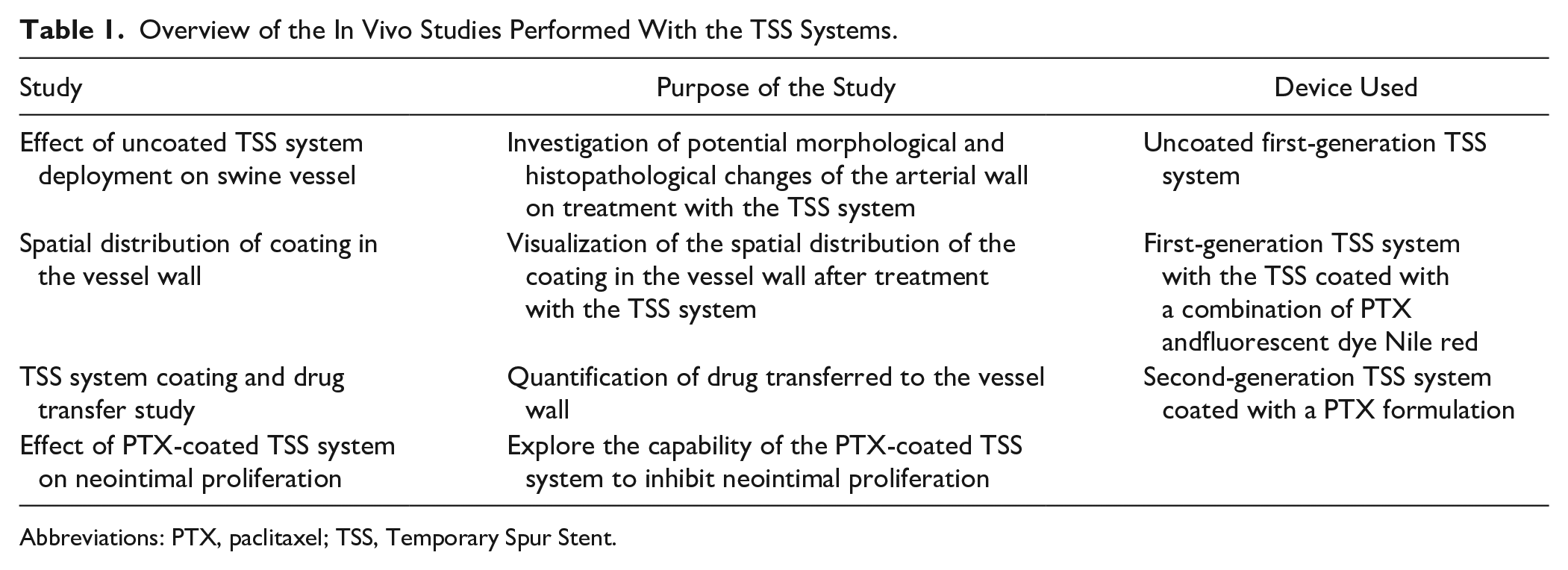
Abbreviations: PTX, paclitaxel; TSS, Temporary Spur Stent.
Animal Studies
All animal studies were conducted at the Institute of Medical Technology and Research (IMTR GmbH, Rottmersleben, Germany) in accordance with the guidelines of the commission directive 86/609/EEC and the German Animal Protection Act based on the Animal Ethics Committee approvals (Sachsen–Anhalt, Germany). Male domestic pigs (3 months, approximately 25 kg) underwent angioplasty in internal iliac, profunda femoral, and external femoral arteries. Details regarding the pharmacological treatment of the animal before, during and after the treatment were described previously in Kelsch et al. 16 For the deployment of the TSS system, a 6F intra-arterial sheath was introduced into a surgically exposed carotid artery. The peripheral arteries were visualized using a nonionic X-ray contrast agent.
General Deployment Procedure of the First-Generation TSS System
The TSS system was deployed in the peripheral arteries and postdilated by inflation of a suitable uncoated balloon (Pacific Plus 4.0×80 mm or 5.0×80 mm, Medtronic, Dublin, Ireland) within the TSS. After treatment, the TSS system and the balloon were retracted from the animal.
General Deployment Procedure of the Second-Generation TSS System
The coated TSS system comprising the balloon (4.0×80 mm) within the Spur was deployed in the peripheral arteries and the balloon was inflated. After treatment, the second-generation TSS system was retracted from the animal. In the case of the acute study, the still anesthetized animals were sacrificed approximately 10 minutes after the last procedure by intravenous injection of 10 mL supersaturated potassium chloride (25%). In the case of 4-week study, the carotid arteriotomy was sutured, and the dermal layers closed using standard techniques. At the 4-week time point, the treated vessels were visualized, the animals were sacrificed as mentioned above and the treated arterial segments were dissected.
Effects of TSS Treatment on Native Vessels
Two pigs were treated with 7 uncoated first-generation TSS systems in their peripheral arteries following the general procedure described above. After TSS deployment, a bare metal stent (BMS; Express Vascular SD 4.0×19 or 5.0×19 mm; Boston Scientific, Marlborough, MA, USA) was implanted in a portion of the treated vessel segment in order to induce neointimal proliferation. Four weeks after the intervention, angiographic images of the treated arteries were taken. Afterward, the animals were sacrificed and the vessels were dissected for histopathological analysis.
Drug Distribution in the Vessel Wall
The spikes and stent struts of 2 first-generation TSS were coated with a formulation containing both PTX and the fluorescent dye Nile red (NR) (Carl Roth GmbH, Karlsruhe, Germany) in a solvent mixture. The coated TSS systems were deployed in the left and right profound porcine femoral arteries. Immediately following the intervention, the animals were sacrificed, and the vessel segments were dissected and cryo-embedded on dry ice using OCT Tissue Tek (Sakura Finetek, Alphen aan den Rijn, Netherlands).The samples were cross-sectioned at a thickness of 100 to 150 µm using a cryostat (CM3050S, Leica, Nussloch, Germany) or cut longitudinally with a microsurgical spring scissor. Tissue sections were mounted on microscopy slides in DAPI (4′,6-diamidino-2-phenylindole) containing medium (Fluoroshield with DAPI, Sigma-Aldrich, Munich, Germany) and analyzed for fluorescence signals of NR and DAPI on a fluorescence microscope (Zeiss Observer Z1, Jena, Germany).
Drug Transfer Study
A drug transfer study was performed by deploying the second-generation TSS systems having both the Spur and the balloon coated using a PTX formulation containing in total 2,750 µg paclitaxel and an excipient. The coated devices were sterilized with ethylene oxide by DMB-Apparatebau GmbH (Wörrstadt, Germany). The deployment of the coated TSS systems was performed by following the general procedure described above. Shortly after intervention, the animals were sacrificed and the vessels were dissected and transferred into preweighed vials for PTX quantification via high-performeance liquid chromatography (HPLC).
Four-Week Efficacy and Tolerance Study of PTX-Coated TSS in Peripheral Arteries of Pigs
Twelve pigs were treated in both internal iliac and both profound femoral arteries by randomizing the vessels into 3 groups: (a) uncoated TSS as negative control, (b) second-generation PTX-coated TSS systems, and (c) PTX-coated balloon (Impact Admiral 4.0×60 mm, Medtronic, Dublin, Ireland) as positive control. The PTX formulation used to coat the Spur and the balloon of the TSS systems was the same used for the drug transfer study. Deployment of the second-generation TSS was performed following the general procedure described above and DCB deployment was carried out using standard balloon angioplasty technique. To enhance neointimal proliferation a BMS (Express Vascular SD 4.0×19 mm or 5.0×19 mm, Boston Scientific, Marlborough, MA, USA) was implanted in a portion of the treated vessel segments resulting in approximately 20% overstretch. Four weeks after the intervention, the pigs were sedated and anaesthetized and angiographic images of the treated arteries were taken. The animals were sacrificed and the treated vessel segments were dissected for histopathological analysis.
Quantitative Angiography (QA)
The CAAS II System (Pie Medical, the Netherlands) was used for quantitative analysis. The parameters that have been measured and the calculations performed to obtain the relevant parameters used for comparisons are described in detail for each study in the Results section.
Histological Analysis
Dissected vessel segments were macroscopically divided in untreated and treated parts. Vessel segments that were permanently stented in a portion of the coated TSS or DCB-pretreated area, were macroscopically divided into stented and nonstented segments. The nonstented segments were embedded in paraffin. Sections of 5 µm were cut and mounted on microscopy slides (Superfrost Plus, Thermo Scientific, Schwerte, Germany), deparaffinized and hematoxylin and Eosin (H&E) stained. The arterial segments with a permanent stent were dehydrated, infiltrated and embedded in methyl-methacrylate (Technovit 9100, Heraeus Kulzer, Wehrheim, Germany) according to manufacturer’s protocol. Three segments (proximal, mid, distal) were cut with a coping saw and reembedded in methylmethacrylate. Tissue sections of 8 µm thickness were sectioned on a rotary microtome with a tungsten carbide knife (D-profile, Leica, Nussloch, Germany), mounted on microscopy slides, deplasticized and H&E stained. Stained tissue sections were analyzed on a Zeiss Observer Z1 microscope or scanned with a NanoZoomer slide scanner (Hamamatsu, Herrsching, Germany).
The following histomorphometric parameters were evaluated: luminal area, internal elastic lamina (IEL) area, external elastic lamina (EEL) area, maximal neointimal thickness, lumen diameter, IEL diameter and EEL diameter. Injury scores were assigned as described by Schwartz et al, and inflammation scores as presented by Kornowski et al, 17 for each individual stent strut. Fibrin depositions were graded modified to Joner et al 18 with a scoring of: 0 no fibrin around the stent strut; 1 depositions at 25%; 2 25% to 50%; 3 50% to 75%, and 4 100% around the stent strut. The scores for each cross-section were calculated as the sum of the score per strut divided by the number of struts in the examined section.
Sample Preparation and Quantitative Analysis of Paclitaxel by HPLC
In order to quantify the amount of PTX in the PTX-coated TSS systems, the Spur and the balloon were dry released in 15 mL Falcon tubes. The drug was extracted using acetonitrile and by placing the tubes in an ultrasound bath to promote drug dissolution. Treated arteries from the drug transfer study were homogenized in absolute ethanol using Precellys 24 Dual Homogenizer (PEQLAB Biotechnologie GmbH, Erlangen, Germany). The samples were adjusted to 20% (m/v) of tissue with absolute ethanol and extracted for 30 minutes under ultrasound sonication. The homogenate was centrifuged (3050×g, 10 minutes). PTX was determined in the supernatant by HPLC with ultraviolet detection. Column: C18, 5 μm, 4.6×250 mm. Isocratic mobile phase: 45% phosphate buffer 5 mM and 55% acetonitrile, flow: 1 mL/min. Detection: 230 nm. Column temperature: 30 °C. A standard curve was performed during the same run (concentration between 5 and 500 μg/mL).
Statistical Analysis
Histomorphometric data and scores of the three cross-sectional segments (proximal, mid, distal) were averaged to obtain a mean value per treated vessel. Histomorphometric data, scores, and QA parameters were tested for statistical significance difference using either unpaired 2-tailed t test or 1-way analysis of variance with post hoc Tukey’s test. The level of statistical significance was set at p≤0.05. The p-values are defined as ns = p>0.05 (nonsignificant), *=p≤0.05, **=p≤0.01, and ***=p≤0.001.
Results
Effect of Uncoated TSS System Deployment on Porcine Peripheral Arteries
In order to investigate potential effects of the spike penetration into the vessel wall, uncoated TSS were deployed in peripheral arteries, as shown in Figure 1. As control for vascular remodeling and neointimal formation, a BMS was implanted in a section of the TSS-treated area. Four weeks after the treatment, the arteries were examined by QA and histopathological analysis.
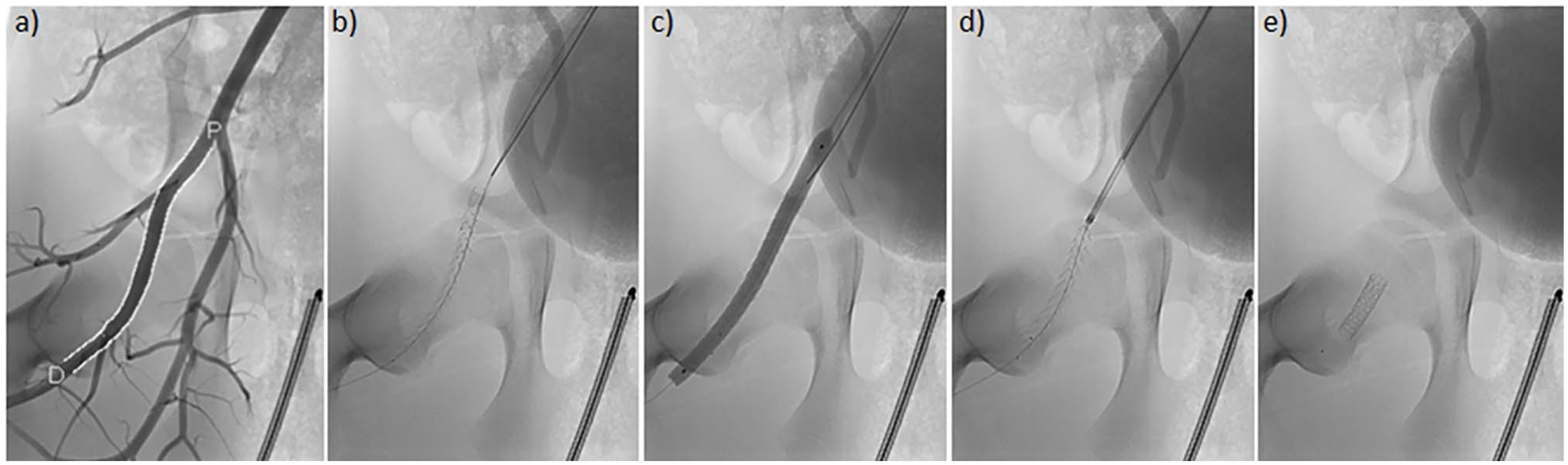
Representative deployment procedure of Temporary Spur Stent (TSS) in the femoral artery of a swine: (a) identification of the vessel segments to be treated, (b) release of the TSS from the delivery catheter, (c) postdilation of TSS using an uncoated balloon, (d) recapture of the TSS, and (e) implantation of permanent stent in a portion of the treated area.
The vessel segments that were treated with the TSS but were not permanently stented showed no statistically significant changes in minimum lumen diameter (MLD) before and 4 weeks after the treatment (2-tailed Student’s t test, p=0.50). In contrast, mean late lumen loss (LLL) in the stented portions, calculated as the difference in the MLD after stent implantation and after 4 weeks, was 1.22±0.73 mm (Table 2) and a statistically significant reduction in the MLD was observed 4 weeks after stent implantation (2-tailed Student’s t test, p=0.013). Diameter stenosis was much more pronounced in permanently stented segments (42%±25%) compared with nonstented segments (11%±9%).
QA Analysis of Vessel Segments Treated With the Uncoated TSS System (n=7, Mean ± SD).
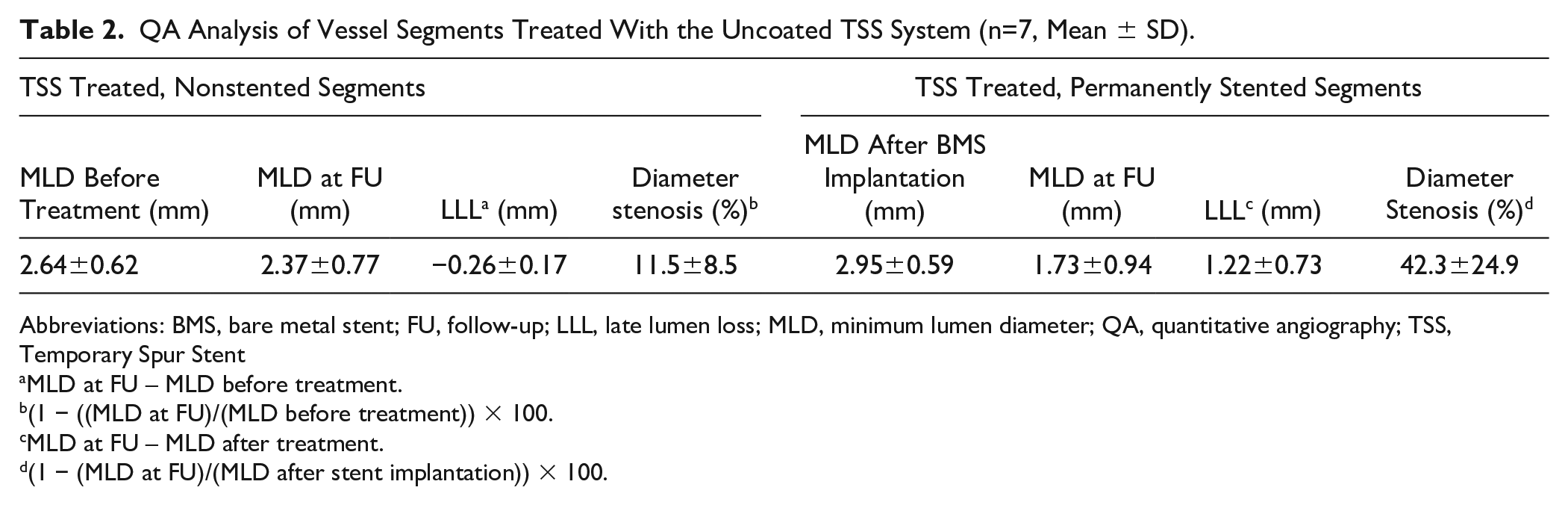
Abbreviations: BMS, bare metal stent; FU, follow-up; LLL, late lumen loss; MLD, minimum lumen diameter; QA, quantitative angiography; TSS, Temporary Spur Stent
MLD at FU – MLD before treatment.
(1 − ((MLD at FU)/(MLD before treatment)) × 100.
MLD at FU – MLD after treatment.
(1 − (MLD at FU)/(MLD after stent implantation)) × 100.
The histological analysis of treated arterial segments confirmed the absence of neointimal formation in the TSS treated vessel segments (Figure 2A and B) 4 weeks after deployment. Segments with a permanent stent developed statistically significant neointimal thickening (Figure 2C) compared with nonstented, TSS-treated vessel segments (Figure 2D).
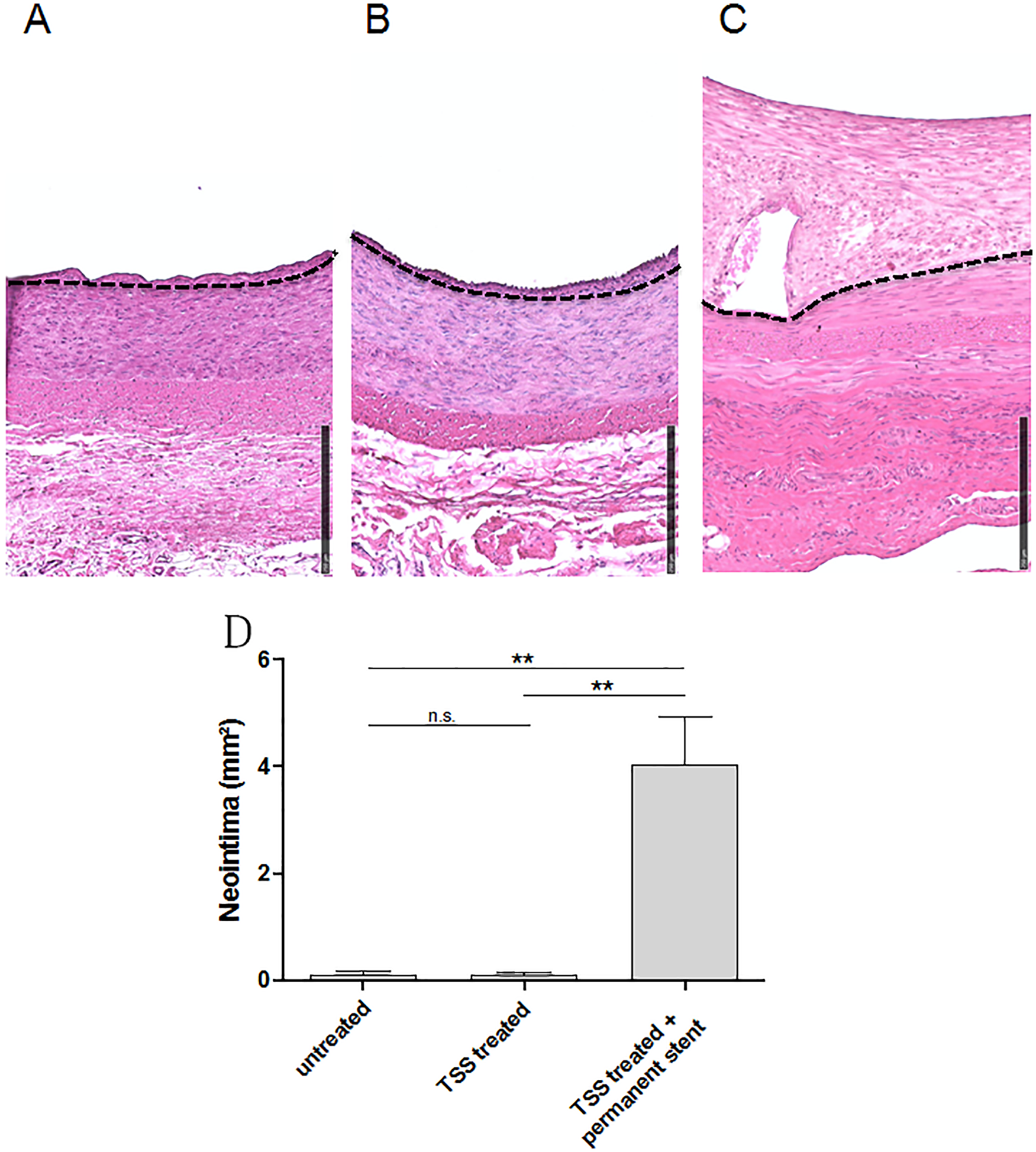
Representative hematoxylin and eosin (H&E) stained cross-sections of (A) untreated area, (B) Temporary Spur Stent (TSS) treated area, (C)) TSS treated and permanently stented area. The dashed line indicates the internal elastic lamina (IEL). Neointimal area (mm2) (D) of untreated (n=5), TSS treated (n=7) and TSS treated and permanently stented (n=7) vessel segments. Data shows mean ± SD. ns, not significant, **p≤0.01. Neointimal area was calculated as internal elastic lamina (IEL) area – lumen area. Bar = 250 µm.
Spatial Distribution of Drug Coating in the Vessel Wall (First Generation)
In order to visualize the spatial distribution of the drug coating in the vessel wall, the TSS was coated with a mixture of PTX and the fluorescent dye NR (Figure 3) and the system was deployed in peripheral porcine arteries. NR fluorescence was visible in distinct spots in vessel wall cross sections (Figure 4a and b). NR doted coating was located deep in the medial and adventitial layers of the vessel wall. A regular distribution of NR spots in the vessel wall was observed when analyzing the vessel longitudinally (Figure 4c).
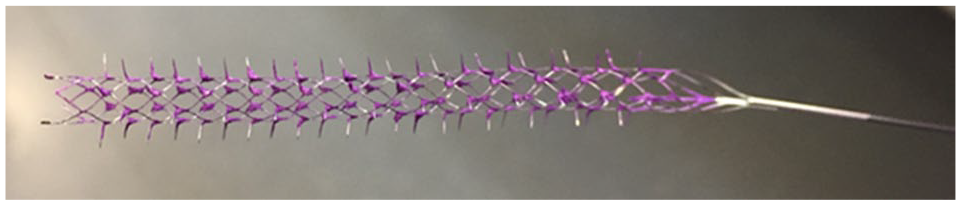
Temporary Spur Stent (TSS) coated with a mixture of paclitaxel (PTX) and Nile red (NR).
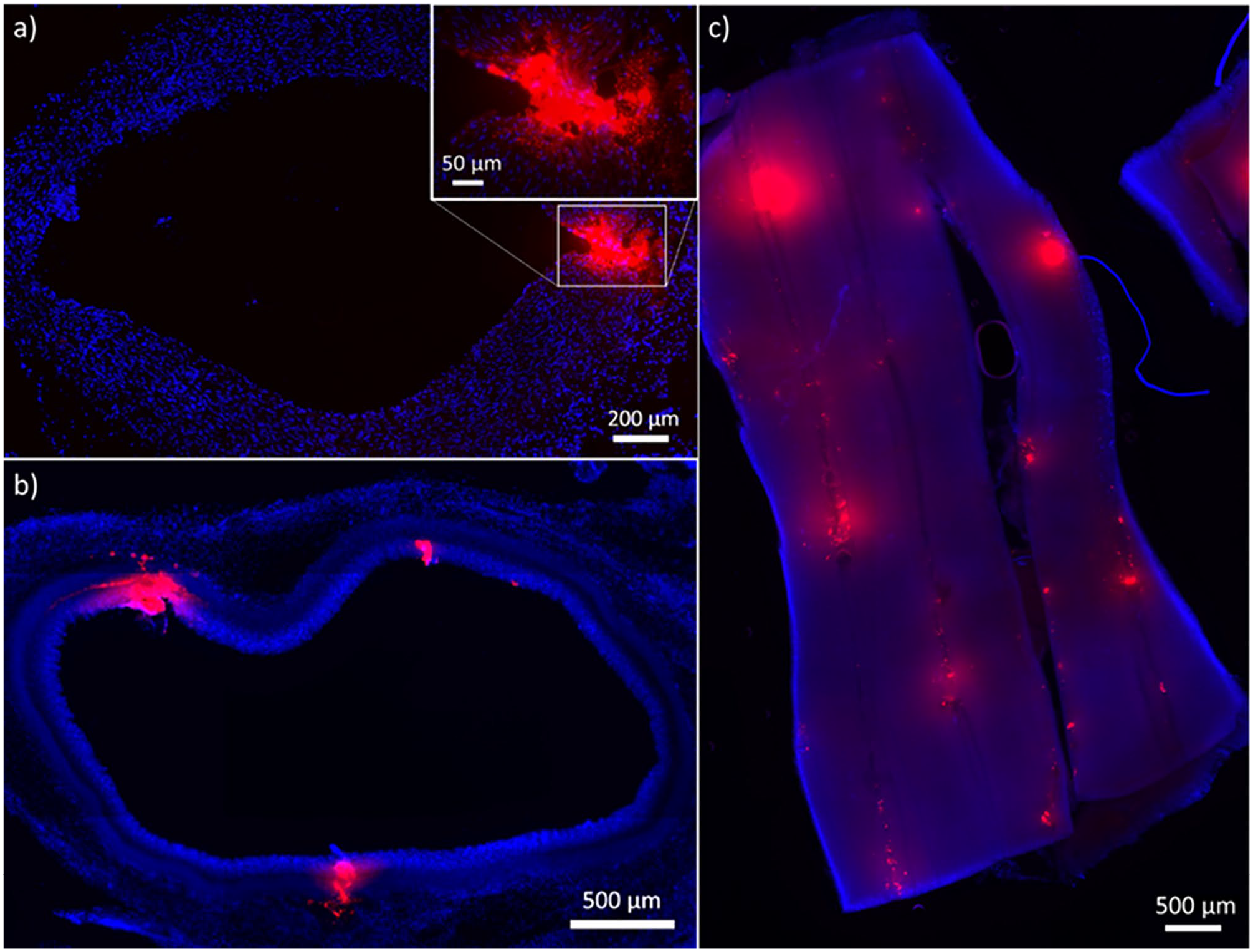
Arteries treated with Nile red/paclitaxel (NR/PTX) coated Temporary Spur Stent (TSS): (a) cross-section (5 µm) showing NR fluorescence in medial and adventitial areas, (b) cross section (100 µm) showing multiple NR spots, and (c) longitudinal section showing multiple NR spots visible in the vessel wall. Cell nuclei were counterstained with DAPI (blue).
TSS System Coating and Drug Transfer Study (Second Generation)
The Spur and the balloon of the second-generation TSS system were coated with a PTX formulation containing an excipient. In previous experiments, the presence of the excipient in the formulation was associated with improved drug transfer to the vessel wall compared with the same formulation without excipient (data not shown). The coating covered both the stent struts and the spikes even though it was noticed that the coating preferentially located at the connection of the spikes with the mesh of the stent (Figure 5). In the case of the second-generation TSS, also the balloon that was already included in the device, was coated with the same formulation used to coat the Spur stent. After coating the Spur stent and the balloon separately, the Spur was bonded on the balloon catheter, as shown in Figure 6. The total amount of drug in the TSS device after sterilization and before animal deployment was 2749±82µg PTX (n=3). The amount of drug transferred to the treated arteries after deployment and retrieval of the TSS was on average 246±181µg (n=3), which corresponded to 9%±7% of the total PTX dose of the device, with a PTX concentration of 196±163 ng/mg of arterial tissue.

Representative image of stent coated with paclitaxel (PTX).

Representative image of Temporary Spur Stent (TSS) and balloon coated with paclitaxel (PTX).
Effect of PTX-Coated TSS System on Neointimal Proliferation (Second Generation)
The effect of the deployment of the PTX-coated second-generation TSS systems on neointimal proliferation was investigated 4 weeks after the treatment. Uncoated TSS and PTX-coated balloon catheters (In.Pact Admiral) served as negative and positive control, respectively. In order to induce neointimal proliferation, a BMS was placed in a section of the TSS-treated arterial segments. The angiograms at follow-up showed a reduction of the lumen diameter in stented vessel segments (Figure 7), especially if arteries were not treated with paclitaxel. The QA analysis showed that the mean vessel lumen diameter (MLD) of the treated vessel segments determined at the time of intervention as well as stent diameter and overstretch ratio did not differ significantly between the treatment groups (Table 3).
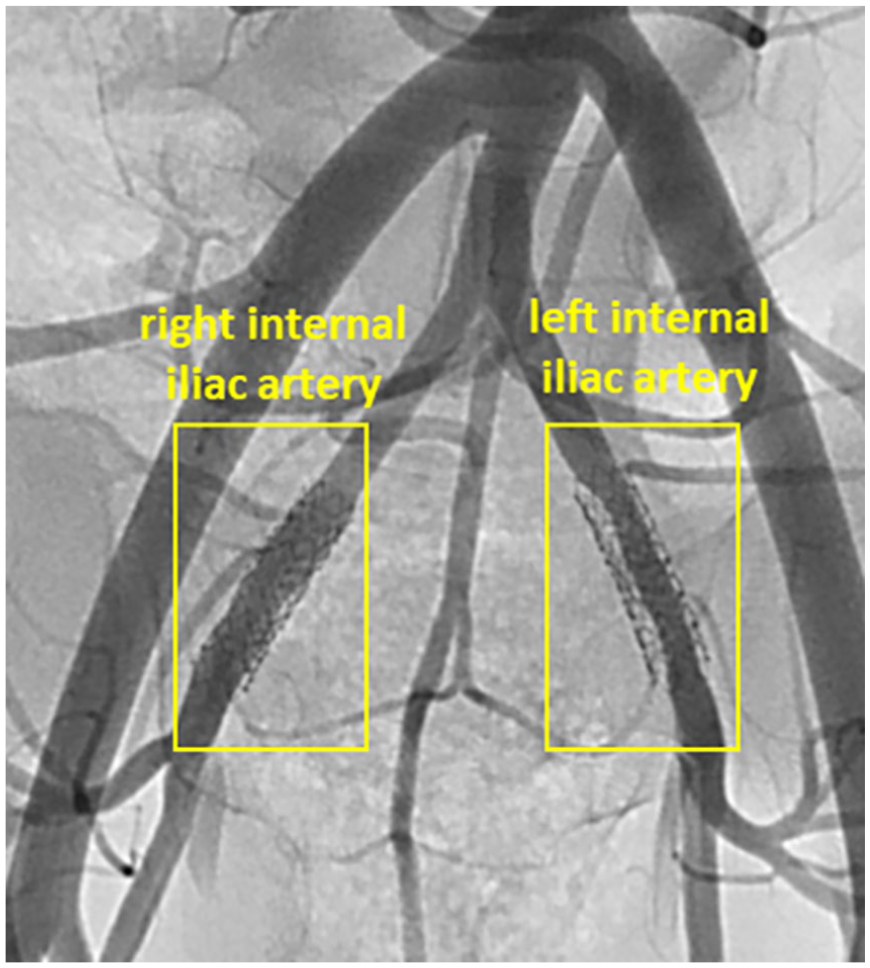
Representative angiographic images of vessel segments 4 weeks after the treatment with uncoated Temporary Spur Stent (TSS) (left internal iliac artery) and paclitaxel ((PTX)-coated TSS (right internal iliac artery). Stenosis, visualized as distance between the vessel lumen and the stent struts, can be noticed mainly in the left internal iliac artery (no drug).
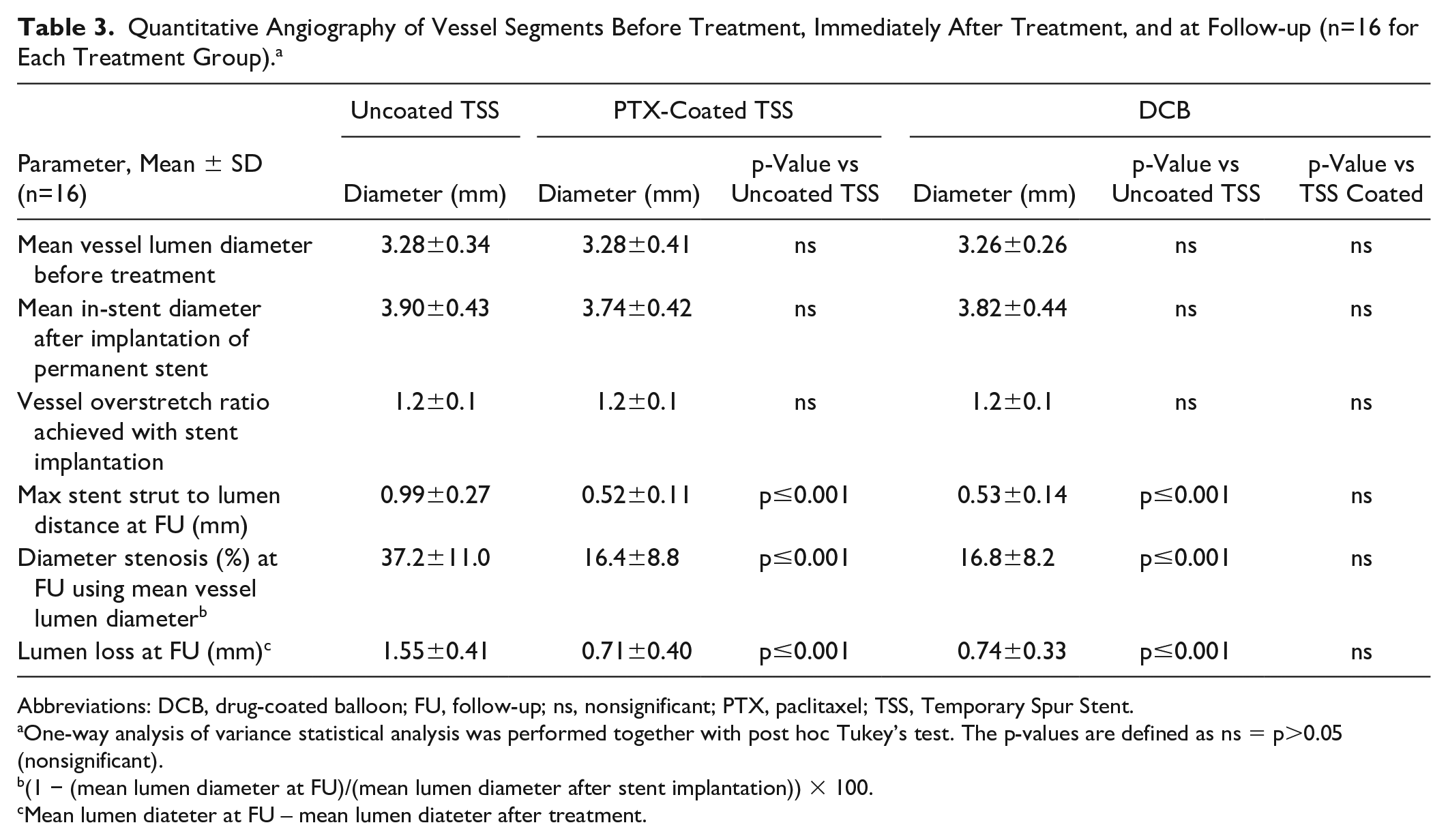
Quantitative Angiography of Vessel Segments Before Treatment, Immediately After Treatment, and at Follow-up (n=16 for Each Treatment Group). a
Abbreviations: DCB, drug-coated balloon; FU, follow-up; ns, nonsignificant; PTX, paclitaxel; TSS, Temporary Spur Stent.
One-way analysis of variance statistical analysis was performed together with post hoc Tukey’s test. The p-values are defined as ns = p>0.05 (nonsignificant).
(1 − (mean lumen diameter at FU)/(mean lumen diameter after stent implantation)) × 100.
Mean lumen diateter at FU – mean lumen diateter after treatment.
The mean values of the maximum stent strut to lumen distance at follow-up of the arteries treated with the TSS system coated with PTX (0.52±0.11 mm) and those treated with the In.Pact Admiral DCB (0.53±0.14 mm) were significantly smaller than the respective distances in the arteries treated with the uncoated TSS (0.99±0.27 mm). The diameter stenosis at follow-up detected in the arteries treated with the uncoated TSS (37.2%±11.0 %) was about double compared to the vessels treated with the Spur coated with PTX (16.4%±8.8%) and with the In.Pact Admiral DCB (16.8%±8.2%). Similarly, the lumen loss at 4 weeks of the vessels treated with the PTX-coated Spur and the ones treated with the In.Pact Admiral DCB was about half of the average lumen loss at follow-up of the arteries treated with the uncoated TSS. The histomorphometric analysis showed that the treatment of peripheral arteries with the PTX-coated TSS and the In.Pact Admiral DCB induced a significant inhibition of neointimal proliferation. PTX-treated vessel segments showed a decrease in neointimal area, lumen loss, and maximal neointimal thickness compared to treatment with the uncoated TSS (Figure 8). Semiquantitative analysis of vessel injury, inflammation, and fibrin content on the basis of H&E-stained sections indicated increased presence of inflammatory cells and fibrin depositions in PTX-treated vessel segments compared with vessels treated with the uncoated TSS (Figure 9). Injury scores were not significantly different between the treatment groups.
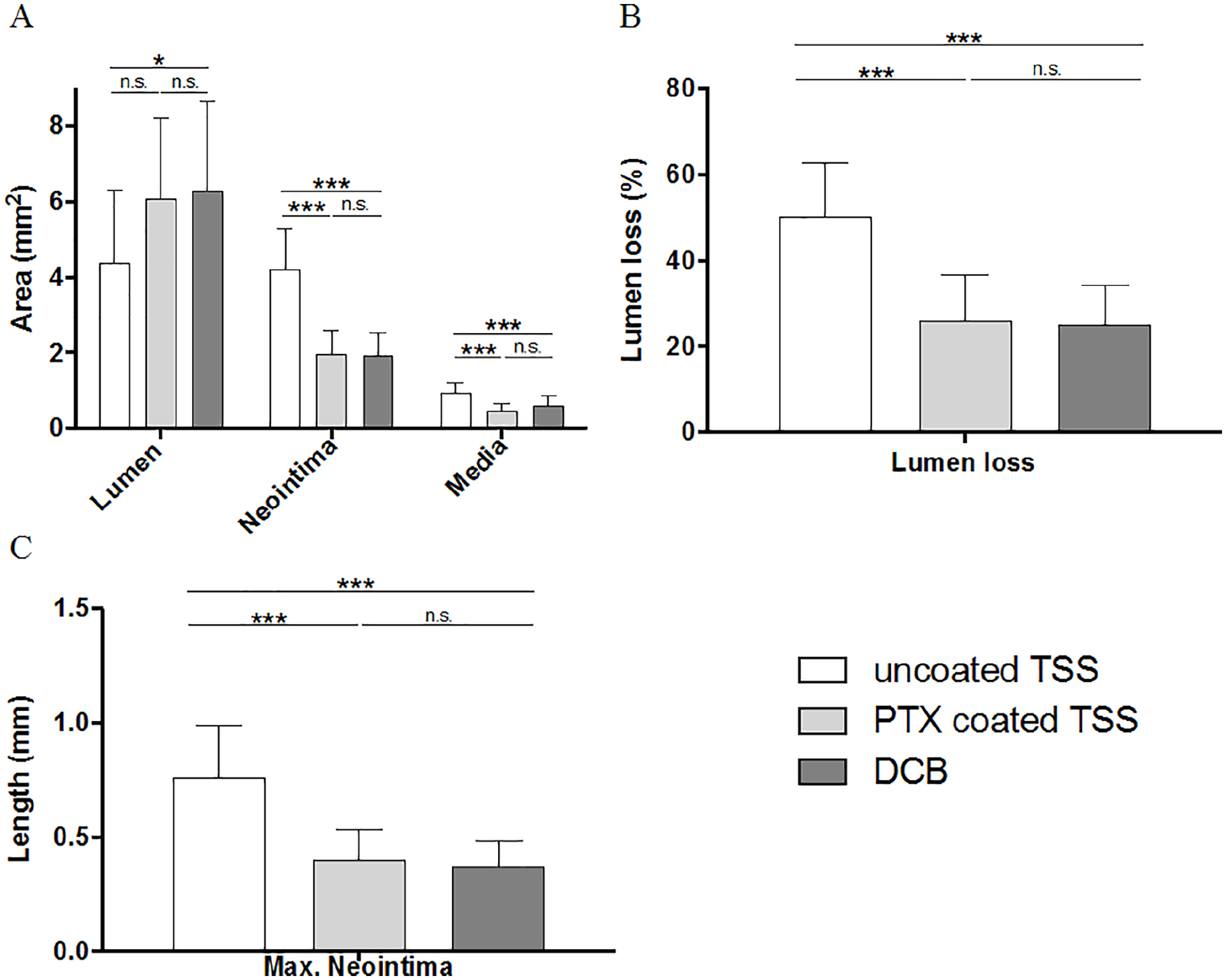
Effect of treatment with paclitaxel (PTX)-coated devices on (A) lumen, neointima, media; (B) lumen loss (% of area); and (C) maximal neointimal thickness. Data are based on n=16 vessel segments for each group, mean ± SD are shown. Statistical analysis was performed with 1-way analysis of variance test with post hoc Tukey’s test. ns, nonsignificant, *p≤0.05, ***p ≤ 0.001.
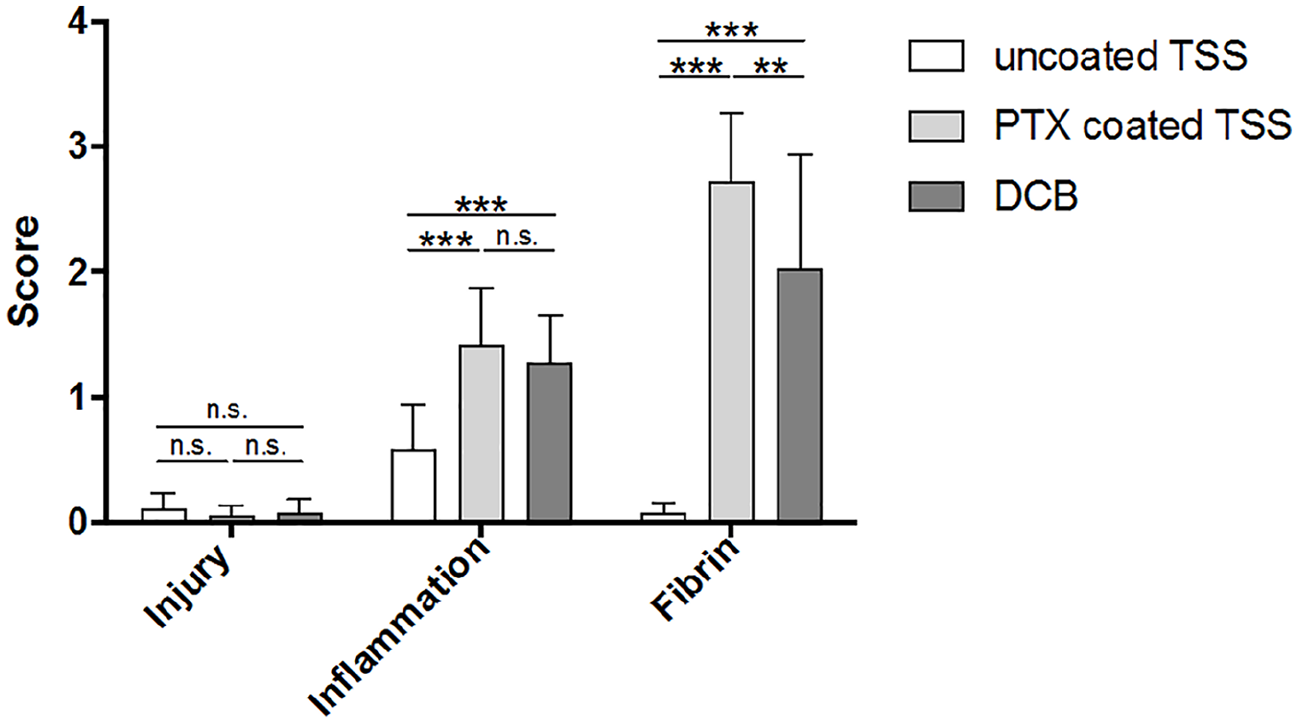
Scoring of vessel injury, inflammation and fibrin deposition on the basis of hematpxylin and eosin (H&E) stained histological sections. Data are based on n=16 vessel segments for each group, mean ± SD are shown. Statistical analysis was performed with 1-way analysis of variance test with post hoc Tukey’s test. ns, nonsignificant, **p≤0.01, ***p≤0.001.
Discussion
Devices such as balloons and stents, which are well established in endovascular therapy, are simple to use and meet the highest safety standards. However, there are still limitations of such devices, especially in achieving long-term results in challenging lesions such as calcified arteries. A new treatment concept to overcome such limitations, such as the TSS presented here, may avoid leaving a permanent implant in the vessel, and its spiked stent may facilitate drug delivery through the calcium deposits to the vessel wall resulting in improved antirestenotic efficacy compared with current available technologies. Furthermore, it should meet the corresponding safety and efficacy standards. Quantitative angiography and histopathological analysis indicated no recognizable changes in vascular morphology 4 weeks after the treatment with the uncoated TSS. The absence of neointimal thickening and negligible lumen loss in the areas without BMS demonstrates that the deployment of the temporary TSS does not induce undesired effects up to 4 weeks after the treatment. On the contrary, the permanent stent implanted in the same vessel segment at the same time caused neointimal thickening and lumen loss. The formation of a neointimal layer on BMS implantation after uncoated and coated TSS treatment has been subsequently explored to evaluate the effect of an antiproliferative coating on neointimal proliferation.
The detection of NR in the arterial wall after the treatment with coated TSS indicates that part of the coating of the stent was transferred to deeper layers of the vessel wall. The visualization of spots instead of a homogenous distribution suggests that the coating transfer took place where the spikes penetrated the vessel wall. On one hand, the lack of NR along the inner wall of the artery might be due to the coating distribution on the stent: The coating is mainly located at the connection of the spikes with the mesh of the stent (Figure 3). On the other hand, it might be that the NR dye has been washed away from the inner vessel wall by the blood flow whereas it stayed in the perforations. The regular NR distribution in the longitudinal presentation matches with the spike organization on the TSS surface, supporting the assumption that the spikes promote the coating transfer to the vessel tunics.
The coating method was demonstrated to be reproducible and suitable for the TSS, with 2749±82 µg PTX found on the whole system (Spur stent 4.0×60 mm + balloon 4.0×80 mm) surface. The average drug transfer achieved with these formulations (246±181 µg, 196±163 ng/mg of arterial tissue) is in the same range obtained with commercially available PTX-coated balloons. 19 A PTX concentration of 58.8±54.2 ng/mg arterial tissue was detected in the vessels 1 hour after treatment with Lutonix DCB, while 4 hours after treatment with Ranger DCB or In.Pact Admiral DCB the PTX concentration was in average 50 ng/mg arterial tissue.19,20
Angiographic and histological analysis showed comparable results: The TSS devices coated with PTX reduced the vascular stenosis in the animal model caused by overstretch and continuous irritation due to permanent stent implantation. The results confirm the efficient transfer of antiproliferative coating from the coated TSS device to the vessel wall leading to a significant inhibition of neointimal proliferation in this stenosis model compared with the vessels treated with the uncoated TSS system. Moreover, the efficacy of the coated TSS in reducing excessive neointimal proliferation induced by the BMS implantation was comparable to that of the commercially available DCB used as control. All parameters indicating neointimal proliferation from the QA and histological analysis of the arteries treated with these 2 systems are similar, and no statistically significant difference or tendency in favor of one of them was found.
The risk and potential harm of emboli if particles of the coating are released in the blood has been discussed and was extensively investigated. 20 Histological examinations of downstream tissues confirmed the existence of microemboli. However, embolization to the myocardium would result in immediately detectable and persistent functional deficits, which were not seen even at high overdose in animal experiments.21 –24 Clinical experience in hundred thousand of critically ill patients and the experience especially in coronary trials confirm that no consequences may be expected.25 –27 Finally, DCB have been used in intracranial vessels without causing neural deficits.28,29 In contrast, consideration of the release of embolic debris with lower solubility and by a far larger mass and volume as an unavoidable consequence of angioplasty and stent implantation has been widely neglected 30 because in most interventions and vessel territories it remains with no clinical consequence. For the TSS system, a further reduction of the downstream volume can be expected due to the combination with the temporary stent and an improved drug transfer.
It is important to note that In.Pact Admiral is a conventional DCB and therefore the drug transfer to the arterial wall is different from the TSS. The potential advantage of the TSS system over DCB relies on the capability of the spikes to penetrate into thick, calcified atherosclerotic vessel walls and presumably promote deeper drug uptake in arteries of patients suffering from the disease. However, the applied animal model does not allow this question to be answered since the vessel walls of the used young pigs are very thin and not calcified. Considering the limitation of the animal model used here, the envisioned advantage of the PTX-coated TSS, including spikes over the conventional PTX-coated balloons and the effectiveness of the treatment in hindering neointimal proliferation should be confirmed by treating calcified plaques. Semiquantitative scoring of vessel sections confirmed similar injury in all treatment groups. Furthermore, the analysis indicates that PTX`s inhibitory effect on neointimal proliferation comes along with increased inflammation and fibrin depositions.
Conclusion
The present study shows that the treatment of peripheral porcine arteries with the uncoated and PTX-coated TSS is well tolerated: the vessels showed no relevant damage, thrombotic occlusion or late lumen loss up to 4 weeks after the treatment and no significant neointimal hyperplasia compared to untreated vessel segments proximal to the treated segments. It was also demonstrated that the TSS promotes the transfer of the coating into deeper layers of the vessel wall. The second generation TSS systems coated with a PTX formulation significantly reduced neointimal proliferation in comparison with the uncoated TSS in porcine arteries. This demonstrates the capability of the second generation TSS to locally deliver drugs to peripheral arteries to effectively inhibit neointimal proliferation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NB and SSK are employees of InnoRa GmbH, Berlin, Germany. IR and TJ are employees of Reflow Medical Inc, USA. BS is shareholder of InnoRa GmbH and was named as co-inventor on patent applications submitted by Charité University Hospital, Berlin, Germany.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.