
Abstract
Purpose:
This study aimed to investigate the effect of distal aortic segmental enlargement (DASE) after thoracic endovascular aortic repair for complicated type B aortic dissection (cTBAD).
Materials and Methods:
From March 2003 to October 2018, 814 patients with acute cTBAD from 5 medical centers were retrospectively identified. DASE is indicated as the enlargement of distal aortic segmental volume ≥1.6 fold of the preoperative volume compared with the most recent postoperative computed tomography angiography (CTA) scan. Of these patients, 635 (78%) were identified as non-DASE, and 179 (22%) were identified as DASE. Competing risk analysis was performed to compare late death and distal aortic reintervention between the groups. The morphological variables and false lumen thrombosis at 7 aortic levels were measured based on the preoperative CTA and the most recent CTA. Univariate and multivariate Cox regression analyses were used to assess the independent predictors of DASE.
Results:
The mean follow-up time of the entire cohort was 5.6 years (interquartile range: 2.4–8.3 years). There were total of 208 late deaths, including 94 (14.8%) deaths in non-DASE group versus 114 (63.7%) deaths in the DASE group. Distal aortic reintervention was observed in 89 patients, with 43(6.7%) in the non-DASE group versus 46 (25.7%) in the DASE group. The cumulative incidence of late death and distal aortic reintervention were significantly higher in the DASE than in the non-DASE group (p<0.001). In morphological analysis, significant incomplete false lumen thrombosis was observed in all distal aortic segments above the aortic level of celiac artery (p<0.01). According to multivariate analysis, the Marfan syndrome, stent coverage to the level of diaphragm and the level of celiac artery were independent predictors of the DASE (p<0.001). Patients with extended stent coverage to the level of celiac artery have shown a lower incidence of DASE (p<0.010).
Conclusion:
Compared with the non-DASE group, patients with DASE demonstrated a higher rate of late death and distal aortic reintervention. For the cTBAD population, extended stent-graft coverage to the aortic section between diaphragm and celiac artery might serve as a “cost-efficient” cutoff point aiming to reduce the risk of DASE.
Keywords
Introduction
For complicated type B aortic dissection (cTBAD), studies have shown that thoracic endovascular aortic repair (TEVAR) provides better aortic remodeling1,2 than the best medical treatment, including the true lumen (TL) enlargement and the false lumen (FL) reduction. TEVAR eliminates the antegrade FL flow by endograft coverage of the proximal thoracic aorta, but this strategy often leaves distal aortic tears unsealed. Unsealed tears may cause false lumen pressurization and expansion by distal proximal perigraft entry flow (type IB entry flow) from the TL to the FL. 3 As a result, 15% to 40% of patients with TBAD would develop distal aortic segmental enlargement (DASE) after the repair,4–6 and DASE has been reported to be related to adverse outcomes. 7 Studies have illustrated a variety of predictors of aortic growth and aortic events in TBAD.5,8,9 However, the DASE-related death, distal aortic reintervention and the natural evolution of the distal aortic remodeling following the TEVAR remain unevaluated. As our understanding of the nature of aortic dissection improves, pre-emptive endovascular treatment in distal dissection is emerging as a way to prevent late complications. 10 Although better aortic remodeling was reported for the stent-graft covered aorta, 11 the role of extended stent-graft coverage remains inconsistency. 5 The optimal range of stent coverage and the potential factors that influencing the DASE and late aortic remodeling remain unclear.12,13 Therefore, in this study, we aimed to evaluate the clinical and morphological outcomes of patients with or without DASE, the independent predictors of the DASE, and the optimal range of endografting in TEVAR for preventing DASE.
Materials and Methods
Study Population
This is a multicenter, retrospective, comparative study. The clinical data were collected for 5769 consecutive patients (Figure 1) with aortic disease from March 2003 to October 2018 at 5 high-volume medical centers that participated in the Chinese Collaborator Group for Aortic Dissection. According to the criteria, 1748 patients were identified as TBAD from the database, as described in the Consolidated Standards of Reporting Trials (CONSORT) diagram (Figure 1). The inclusion and exclusion criteria are shown in Figure 1. The inclusion criteria were as follows: (1) cTBAD occurred in the acute and subacute phases; 14 (2) TEVAR was performed for the patients with TBAD; (3) the thoracic aorta was covered by the stent-graft; and (4) the patients’ distal false lumen was persistent after the TEVAR. The exclusion criteria were as follows: (1) aortic ulcer or intramural hematoma were present; (2) patients displayed uncomplicated TBAD; (3) the first TEVAR procedure was not performed at the 5 participating hospitals; (4) patients were lost to follow-up or lack of at least 1 computed tomography (CT) image during the follow-up; (5) the follow-up time was <6 months. This study was approved by the Institutional Review Board (No. IRB20190711) and the Research Ethics Committee of each participating hospitals.
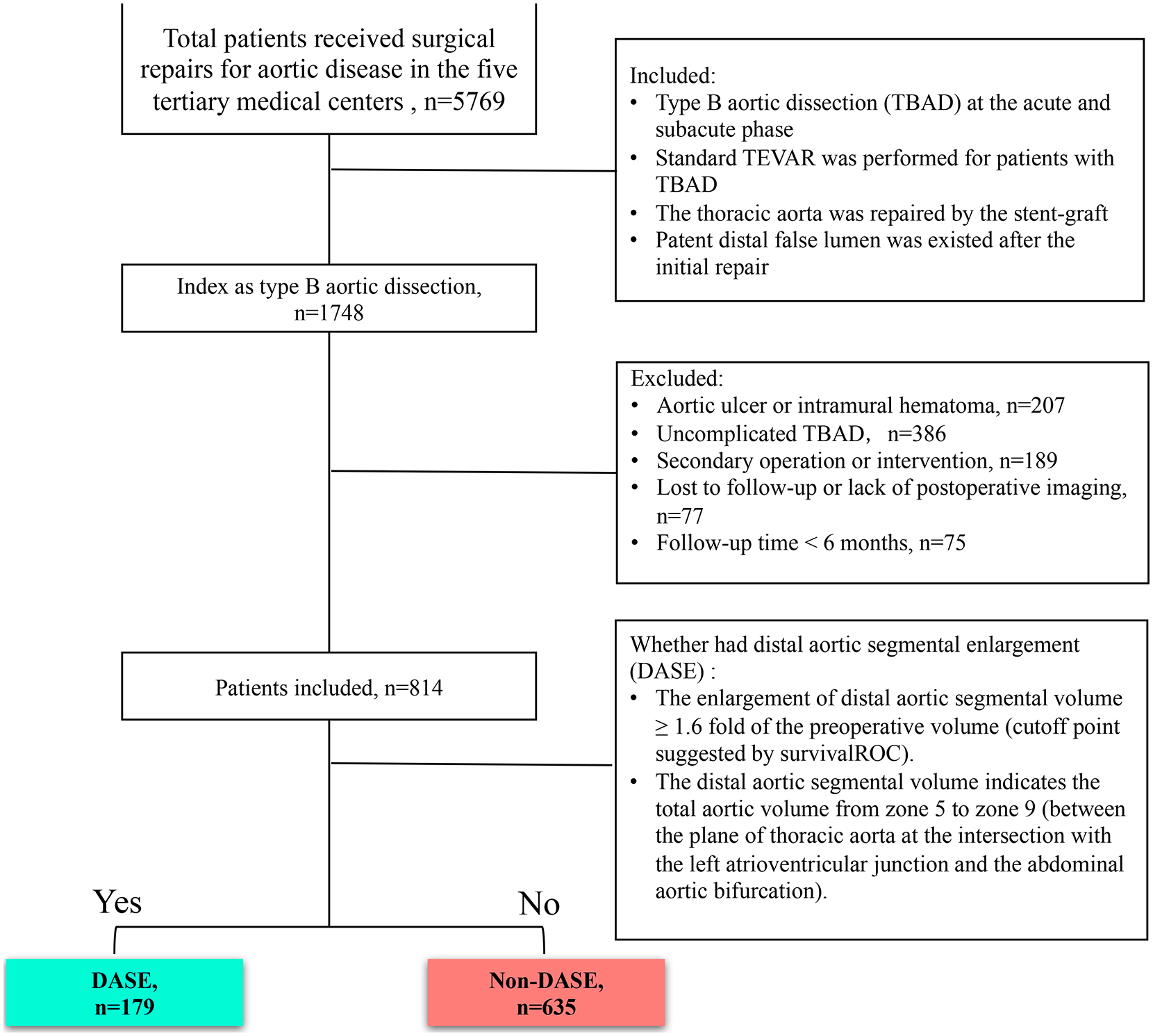
The CONSORT flow diagram. The consort diagram details the inclusion and exclusion flow of this study, and the criteria for the DASE group and non-DASE group. DASE, distal aortic segmental enlargement; TBAD, type B aortic dissection; TEVAR, thoracic endovascular aortic repair.
Definitions and the Outcomes
According to the literature, 15 cTBAD is defined as the presence of at least one of the following: malperfusion syndrome (visceral or lower extremity), aortic rupture, hypotension or shock, neurologic sequelae, recurrent or refractory pain, hypertension refractory to medical therapy, early aortic dilation, or propagation of the dissection. The primary outcome is the cumulative incidence of late death with distal aortic reintervention as a competing risk. Late death referred to all-cause mortality occurring during the follow-up, excluding perioperative mortality (which was defined as deaths within 30 days of the intervention). Distal aortic reintervention includes any endovascular reintervention for the distal aorta. There were several techniques applied including the FL Coli embolization, parallel stent-graft technique, 16 fenestration/branched stent-graft, 17 distal landing zone optimization with the deployment of the bare metal stent (BMS) in the TL and stent-graft bridging advanced from the TL, passed the tear and FL, and into the target artery. The indications for reintervention were organ/limb malperfusion, sign of aortic rupture, SINE, Type I endoleak, and expansion of aortic diameter >5 mm per 6 months.
The secondary outcome includes the morphological features of the long-term aortic remodeling (based on the most recent CTA scans) and the association between the plane of stent coverage and the occurrence of DASE. According to the reporting standards for type B aortic dissections of the Society for Vascular Surgery (SVS) and Society of Thoracic Surgeons (STS), 18 the distal aortic segmental volume indicates the total aortic volume from the zone 4 to zone 9 (between the plane of the thoracic aorta at the intersection with the left atrioventricular junction and the abdominal aortic bifurcation). The rationale for the definition of DASE is described in the statistical analysis. Addtionally, the comorbidities were collected and quantified following the reporting standard. 18 The detailed subtype of false lumen thrombosis was defined following the previous reports:19–21 Non-thrombosed FL indicates the FL was patent; Partial-thrombosed FL indicates the presence of both the presence of thrombosis and contrast in the FL; Complete-thrombosed FL indicates the FL is completely thrombosed and no flow is present. The distal stent graft-induced new entry (dSINE) 22 was defined as the new appearance of an intermedia injury resulting in a new patent false lumen in close relationship with the distal stent graft as a consequence of mechanical friction and sheer stress between the distal stent graft and the descending aorta.
Data Collection, Morphological Evaluation, and the Follow-up
The clinical data were collected from the electronic database. Morphological data were extracted from anonymized pre- and postoperative CTA images. All CTA images were performed on multisided CTA scanners. The DASE was dichotomized for the optimal cutoff value by evaluating the distal aortic volume with the risk of death using the “survivalROC” package plot via the K–M method in R software and the distribution of the fold change of aortic volume of the entire cohort was visualized by the “sur_cutpoint” function of the “survminer” packages in R (Supplementary Figure 1). DASE is submitted as the enlargement of distal aortic segmental volume ≥1.6 fold of the preoperative volume compared with the most recent postoperative CTA scan. (Supplementary Figure 1, AUC=0.917, sensitivity=0.553 specificity=0.893).
The acquired CTA data sets were transferred to a TeraRecon Vascular 4.4.6 workstation (Aquarius iNtuition Edition, TeraRecon) in DICOM (Digital Imaging and Communications in Medicine) format for analysis. A central vessel reconstruction in central line (CL) protocol reconstruction mode was obtained for all CTAs (Supplementary Figure 2A). The CL was created from the aortic valve annulus to the distal segments of the iliac artery (Supplementary Figure 2B). The measurement of the torsion angle of the FL is carried out in multiplanar reconstruction (MRP) mode. The orientation of FL is that FL rotates in the direction of clockwise or counterclockwise with respect to the center of TL. We defined a 12 o’clock table on the cross section and set the direction of the spinous at the 12th thoracic vertebral plane as 6 o’clock. The aorta and its remodeling were evaluated based on CTA before the operation and according to the latest radiological result obtained in the follow-up. The aortic diameter and volume of the TL and FL, the length and location of the aortic dissections were evaluated according to the reported protocol (Supplementary Figure 2C and D). The TL volume was measured on the curved planar reformations that were stretched along the centerlines of the total aorta and TL, respectively, whereas the FL volume was obtained by subtracting the TL volume from the total aortic volume. The dissected aorta was assessed at the 7 planes according to the method given in previous reports. 23 The images were independently evaluated by 2 vascular surgeons (MY Liu and J Liu). Inter- and intraobserver agreements of the measurement of aortic morphologic features were calculated using Bland–Altman analysis (Supplementary Figure 3).
Follow-up CTA scans were scheduled at 1, 6, and 12 months after the procedure and annually thereafter. If a DASE was confirmed during the follow-up, subsequent CTA surveillance every 6 months was required and early intervention was strongly suggested. The DASE evaluation was performed at the scheduled CT follow-up or obtained before the reintervention. All patients were treated with antihypertensive agents, and their systolic blood pressure (SBP) was controlled to be ≤140 mmHg. The medications for DASE and non-DASE can be found in the Supplementary Table 1.
Statistical Analysis
The discrete variables are reported as numbers with percentages and continuous data are reported as the mean ± standard deviation and median [interquartile range (IQR) Q1, Q3]. Differences between groups were tested using the χ2, Fisher’s exact test or Mann–Whitney U test for categorical variables and the independent samples t-test for continuous variables. The cumulative incidence of death and the competing risk-distal aortic reintervention were evaluated by the competing risk analysis using the “cmprsk” package in R. Univariate and multivariate Cox proportional hazards models were used to examine independent factors that were associated with the risk of DASE for the dichotomized groups separately. The Kaplan–Meier method was used to analyze the freedom from DASE for the patients with or without prolonged stent coverage, and the difference between the curves was tested by a log-rank test. Statistical significance was defined as probability (p) values <0.05, and all p values were 2-sided. The inter- and intraobserver agreements of the measurement of aortic measurement were calculated using Bland–Altman analysis via MedCalc (MedCalc Software Version 12.3.0, Mariakerke, Belgium), and the remaining statistical tests were performed with R software (http://www.R-project.org).
Results
Characteristics of Baseline Demographics, Comorbidities, Procedures, and Clinical Outcomes
Figure 1 illustrates the inclusion and exclusion flow of this study, and criteria for the DASE group and non-DASE group. Finally, 814 cTBAD patients were enrolled in this study, including 179 patients (22%) in the DASE group and 635 patients (78%) in the non-DASE group. The majority of patients achieved a sufficiently long follow-up (mean 5.6 years, interquartile range: 2.4–8.3 years). The incidence of DASE after the TEVAR was 179/814 (22%), and the mean occurrence time of DASE was 5.0 years (interquartile range: 2.0–7.7 years). Data for the characteristics of the baseline and comorbidities of the non-DASE and DASE groups are summarized in Table 1. The mean age of was 57.0±14.6 years and 53.0±17.8 (Table 1, p=0.032), in the non-DASE group and the DASE group, respectively. The DASE group had a higher proportion of arrhythmia [18 (10.1%) vs 27 (4.3%), p=0.007], Marfan syndrome [(10(5.6%) vs 9(1.4%), p=0.001] and alcohol abuse [13 (7.2%) vs 8 (1.3%), p=0.012]. The other index was not significantly different between the non-DASE group and DASE group (Table 1).
The Demographics and Comorbidities.
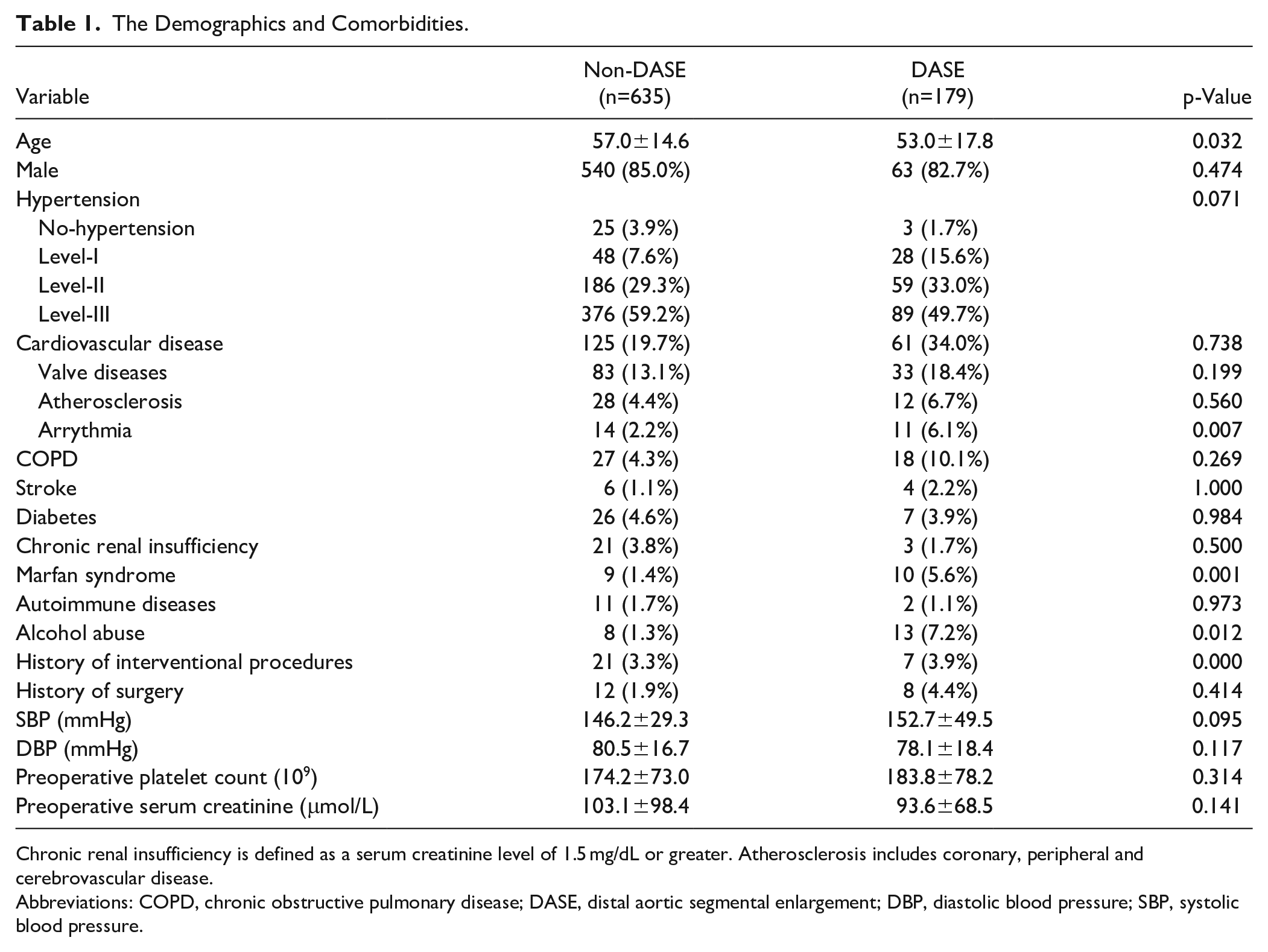
Chronic renal insufficiency is defined as a serum creatinine level of 1.5 mg/dL or greater. Atherosclerosis includes coronary, peripheral and cerebrovascular disease.
Abbreviations: COPD, chronic obstructive pulmonary disease; DASE, distal aortic segmental enlargement; DBP, diastolic blood pressure; SBP, systolic blood pressure.
Differences in procedure characteristics were observed between the groups, as summarized in Table 2. The patients with DASE had a significantly shorter length of stent-graft coverage in the descending aorta (p<0.001), a higher proportion of cuff or BMS implantation (p<0.001) and less restrictive bare metal stent (RBMS) deployment than the non-DASE patients (p=0.006). Cuff and BMS were deployed to eliminate intraoperative type I endoleak. Postoperative endoleak (p=0.01), dSINE (p<0.001) and distal aortic reintervention were more commonly observed in the DASE group than in the non-DASE group (Table 2, p<0.001). However, postoperative complications and the distal oversizing were not significant different between the groups (Table 2, p>0.05).
Procedural Characteristics and Outcome.
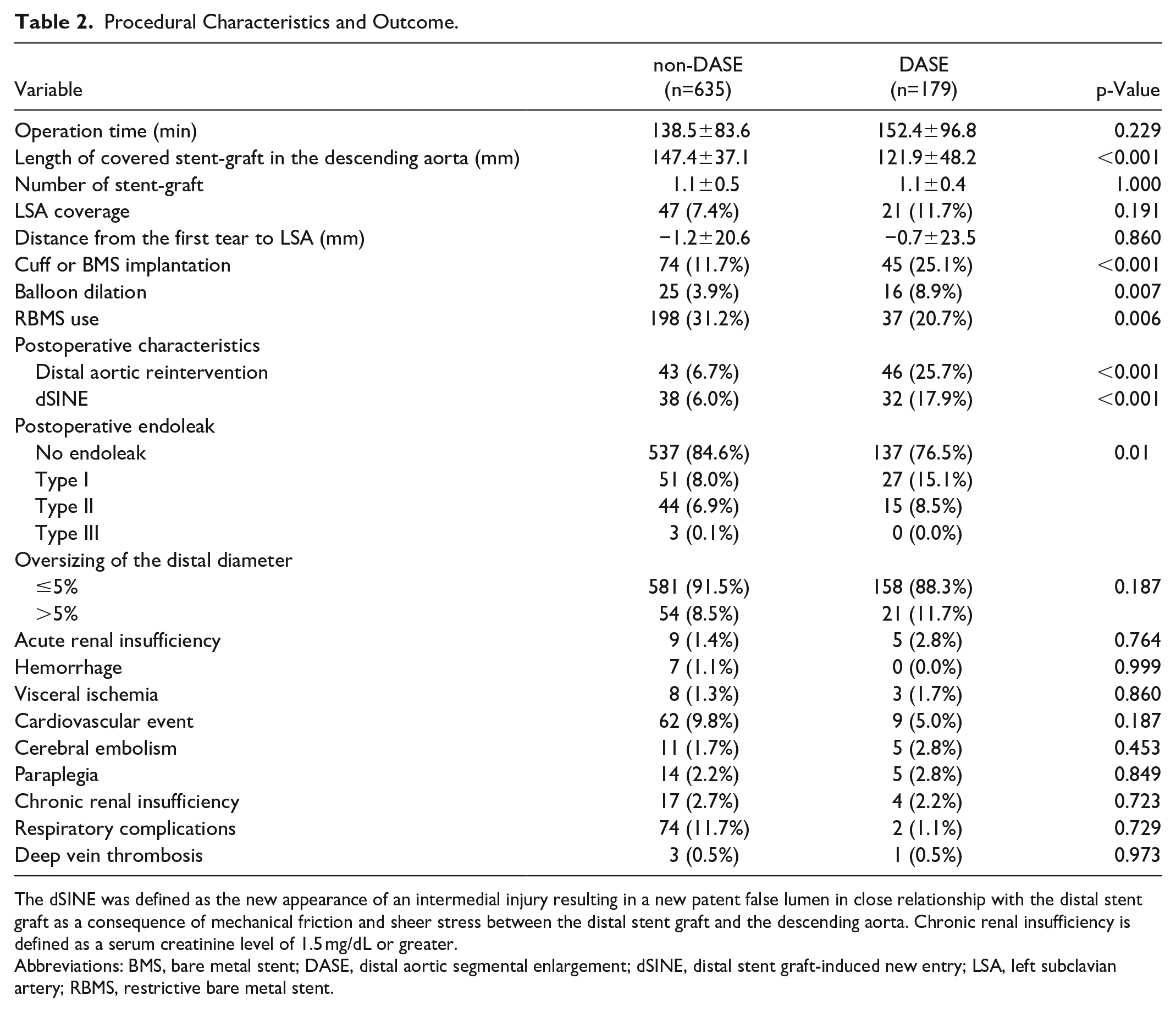
The dSINE was defined as the new appearance of an intermedial injury resulting in a new patent false lumen in close relationship with the distal stent graft as a consequence of mechanical friction and sheer stress between the distal stent graft and the descending aorta. Chronic renal insufficiency is defined as a serum creatinine level of 1.5 mg/dL or greater.
Abbreviations: BMS, bare metal stent; DASE, distal aortic segmental enlargement; dSINE, distal stent graft-induced new entry; LSA, left subclavian artery; RBMS, restrictive bare metal stent.
Late Death and Distal Aortic Reintervention
The cumulative incidence of late death and distal aortic reintervention of the entire cohort and the categorical groups are shown in Figure 2. There were totally 208 late deaths, including 94 (14.8%) deaths in the non-DASE group and 114 (63.7%) deaths in the DASE group. Distal aortic reintervention was observed in 89 patients, with 43 (6.7%) in the non-DASE group versus 46 (25.7%) in the DASE group. Detailed data can be found in the Supplementary Table 2. The cumulative incidence of late death for the entire cohort, non-DASE and DASE were 0.7% (95% CI, 0.3%–1.6%), 0.3% (95% CI, 0.1%–1.1%), and 2.2% (95% CI, 0.7%–5.3%) at 1 year; 11.1% (95% CI, 8.7%–13.6%), 9.7% (95% CI, 7.2%–12.6%), and 16.9% (95% CI, 10.9%–24.1%) at 5 years, respectively. The cumulative incidence of distal aortic reintervention for the entire cohort, non-DASE and DASE were 2.2% (95% CI, 0.3%–1.6%), 0.8% (95% CI, 0.3%–1.8%), and 7.3% (95% CI, 4.1%–11.7%) at 1 year and 1.3% (95% CI, 8.5%–13.4%), 7.7% (95% CI, 4.9%–9.7%), and 21.8% (95% CI, 15.9%–28.4%) at 5 years, respectively. The DASE group had a higher incidence than the non-DASE group for both late death (Figure 2B, p<0.001) and the distal aortic reintervention (Figure 2C, p<0.001).
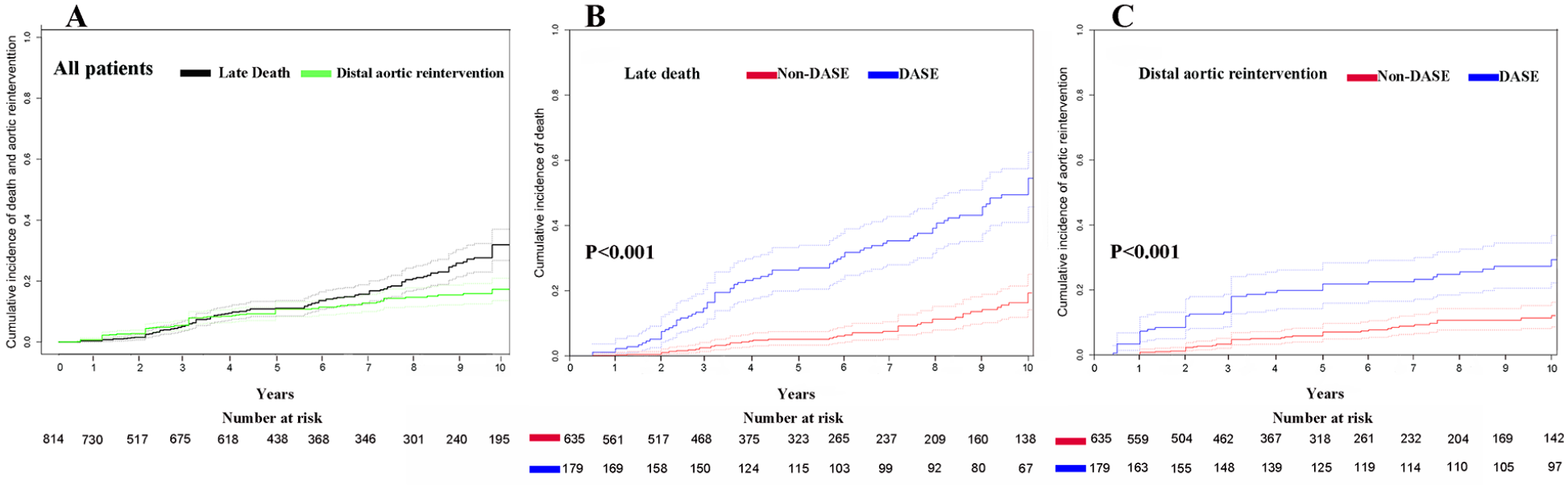
Cumulative incidence of death with distal aortic reintervention as a competing risk for the DASE and Non-DASE groups after TEVAR. Cumulative incidence of death (black) with distal aortic reintervention (green) as a competing risk for all the patients (A). Cumulative incidence of death (B) with distal aortic reintervention (C) as a competing risk for the non-DASE (red) and DASE (blue) groups. The full lines indicate cumulative incidence. The dashed lines indicate 95% confidence intervals. DASE, distal aortic segmental enlargement; TEVAR, thoracic endovascular aortic repair.
False Lumen Remodeling at Different Aortic Levels
To explain the variation in FL remodeling, we analyzed the change in FL thrombosis at the 7 index aortic levels 18 based on the most recent postoperative CTA scans (Figure 3A). Compared with the non-DASE group, the percentage of incomplete FL thrombosis (including non-thrombosed and partial-thrombosed FL) was significantly higher in the DASE group at 4 planes (Figure 3B, planes A–D), which included the middle plane of the thoracic descending aorta (Plane A, p<0.001), the plane of the left atrioventricular junction (Plane B, p<0.001), the plane of the diaphragm (Plane C, p<0.001), and the plane of celiac artery (Plane D, p=0.006). However, this trend was restrained below the plane of the celiac artery. The incomplete FL thrombosis did not have a statistically different below the plane of the renal arteries (Plane E, p=0.094), the middle plane of the abdominal aorta (Plane F, p=0.152) or the widest plane of the iliac artery (Plane G, p=0.079).
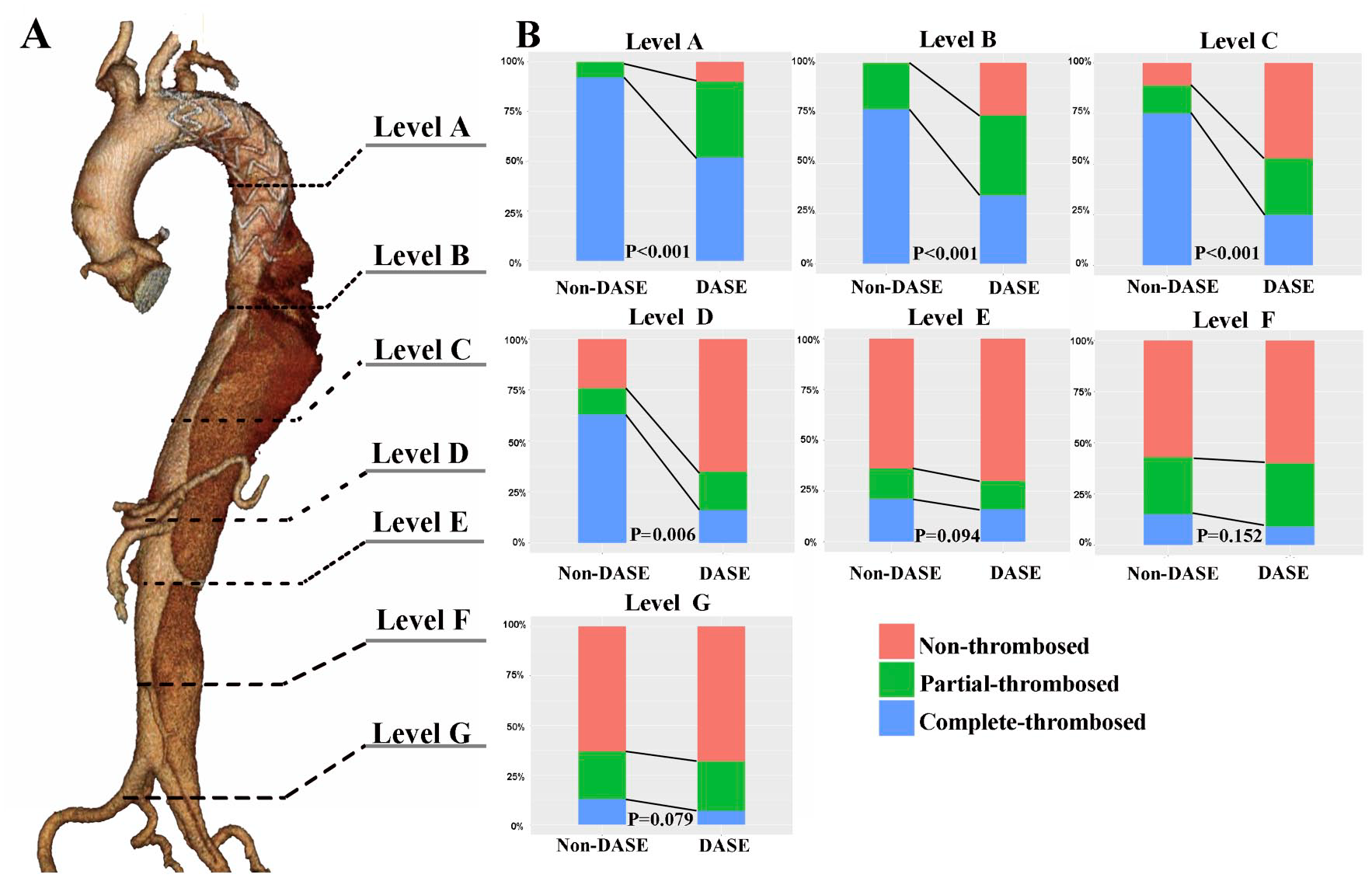
Comparison of the false lumen thrombosis for DASE versus non-DASE at multiple levels. (A) Schematic diagram of the measurement for false lumen thrombosis at the 7 indicated planes of the aorta. (B) The 7 indicated level of the aorta: Level A is the middle plane of the thoracic descending aorta; Level B is the plane of thoracic aorta at the intersection with the left atrioventricular junction; Level C is the plane of the diaphragm; Level D is the plane of the celiac artery; Level E is the plane of the renal arteries; Level F is the middle plane of the abdominal aorta; Level G is the most-wide plane of the iliac artery. Non-thrombosed indicates that the FL was patent; Partial-thrombosed indicates the presence of both presence of thrombosis and contrast in the FL; complete-thrombosed indicates FL is completely thrombosed and no flow was present. DASE, distal aortic segmental enlargement.
Independent Predictors of DASE
Factors that differed between the groups including the Marfan syndrome, alcohol abuse, arrythmia and the range of the stent coverage at different aortic levels, were included in the univariate and multivariate Cox proportional hazards models. The univariate cox model (Table 3) indicated that Marfan [HR, 7.607 (95% CI, 4.567–12.645), p<0.001] and arrythmia [HR, 2.539 (95% CI, 1.233–5.230), p=0.011] were the factors that significantly increased the risk of DASE whereas stent-grafts that extended to level C [HR, 0.415 (95% CI, 0.282–0.610), p<0.001] and level D [HR, 0.111 (95% CI, 0.040–0.306), p<0.001] were the factors that ameliorated the DASE. In the multivariate Cox model (Figure 4), only Marfan [HR, 5.36 (95% CI, 3.065–9.380), p<0.001] was associated with an increased risk of DASE, whereas stent-grafts extended to level C [HR, 0.42 (95% CI, 0.283–0.610), p<0.001] and level D [HR, 0.111 (95% CI, 0.042–0.310), p<0.001] were solid factors impairing DASE.
The Univariate Cox Proportional Hazards Regression Model for the Independent Predictors of DASE.
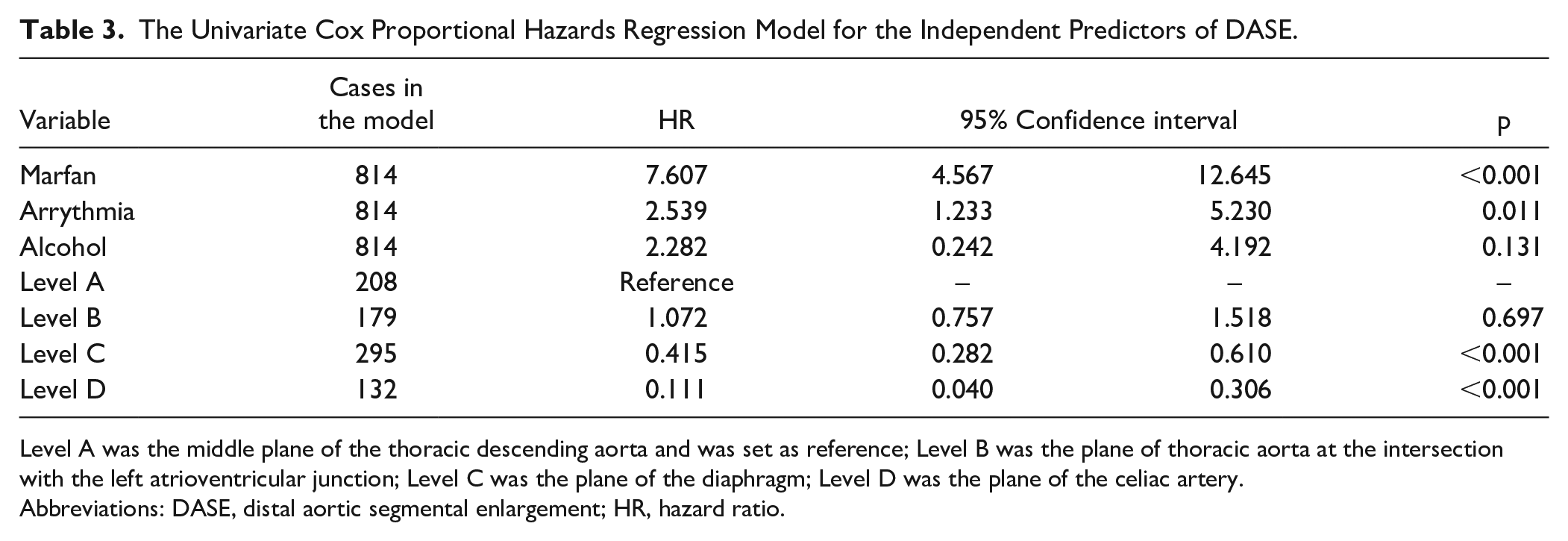
Level A was the middle plane of the thoracic descending aorta and was set as reference; Level B was the plane of thoracic aorta at the intersection with the left atrioventricular junction; Level C was the plane of the diaphragm; Level D was the plane of the celiac artery.
Abbreviations: DASE, distal aortic segmental enlargement; HR, hazard ratio.
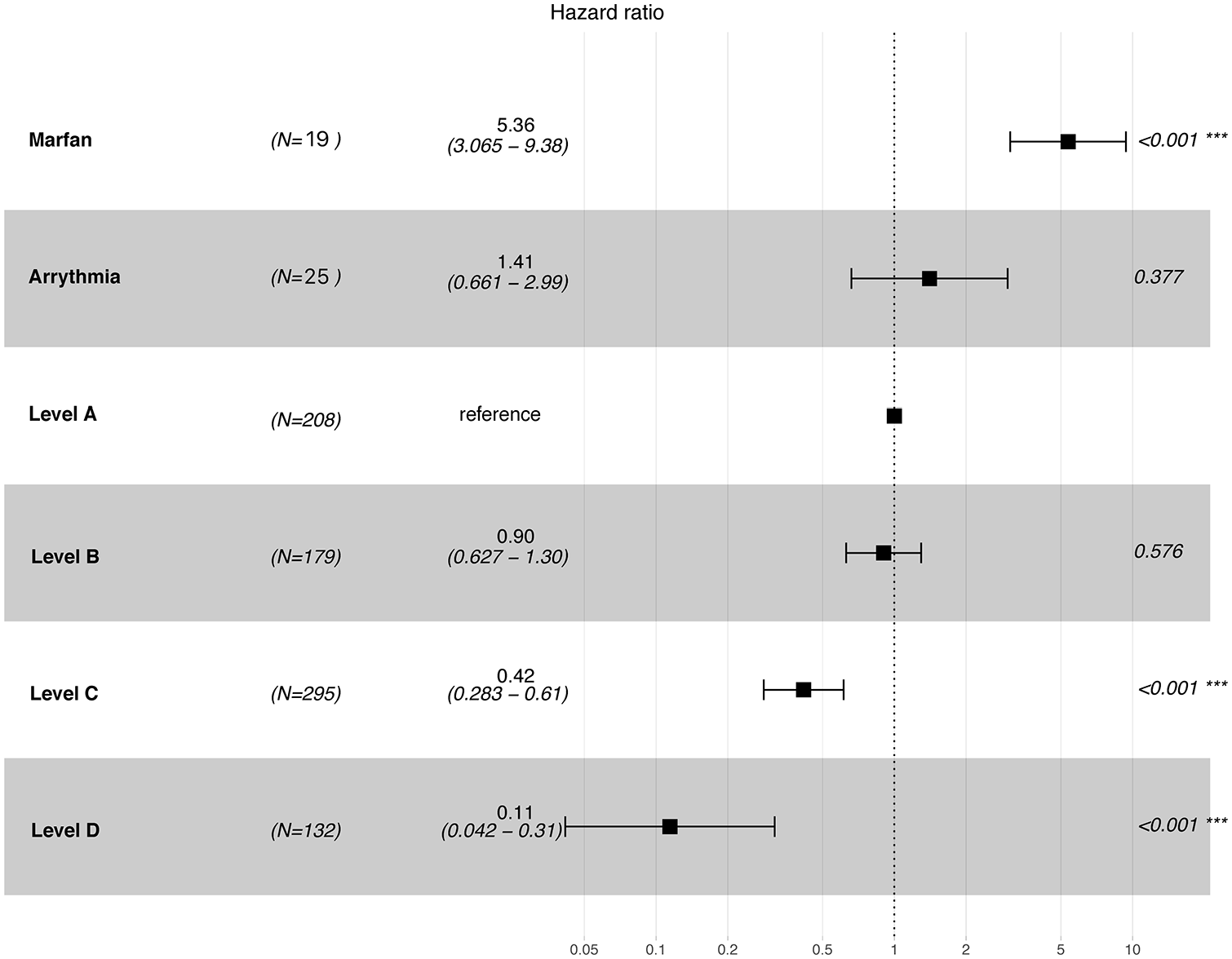
Multivariate Cox proportional hazards models for the independent predictors of DASE. The entire cohort was dichotomized by the range of stent coverage at the each indicated level with the occurrence of DASE as events. Level A was the middle plane of the thoracic descending aorta and was set as a reference; level B was the plane of thoracic aorta at the intersection with the left atrioventricular junction; level C was the plane of the diaphragm; and level D was the plane of the celiac artery. DASE, distal aortic segmental enlargement; HR, hazard ratio.
To examine the effect of extended stent-graft coverage the level D – celiac artery (CA), we computed the freedom from DASE for the entire cohort (pink), and for patients dichotomized by whether stent coverage extended to the CA (Figure 5). The freedom from DASE for the entire cohort (pink) was 97.0% (95% CI, 95.8%–98.3%) at 1 year, 83.1% (95% CI, 80.1%–86.3%) at 5 years and 52.5% (95% CI, 46.6%–59.0%) at 10 years. The freedom from DASE for the patients with (green) and without (blue) stent coverage extended to CA at 1, 5, 10 years was 100% versus 97.0% (95% CI, 95.8% –98.3%), 88.7% (95% CI, 81.6%–96.6%) versus 82.0% (95% CI, 78.6%–85.5%), and 77.4% (95% CI, 62.1%–96.5%) versus 50.0% (95% CI, 44.0%–56.8%), respectively (Figure 5). Overall, the patients who had stent coverage extended to CA exhibited a significantly higher rate of freedom from DASE than patients who did not (p=0.005, by log-rank test).
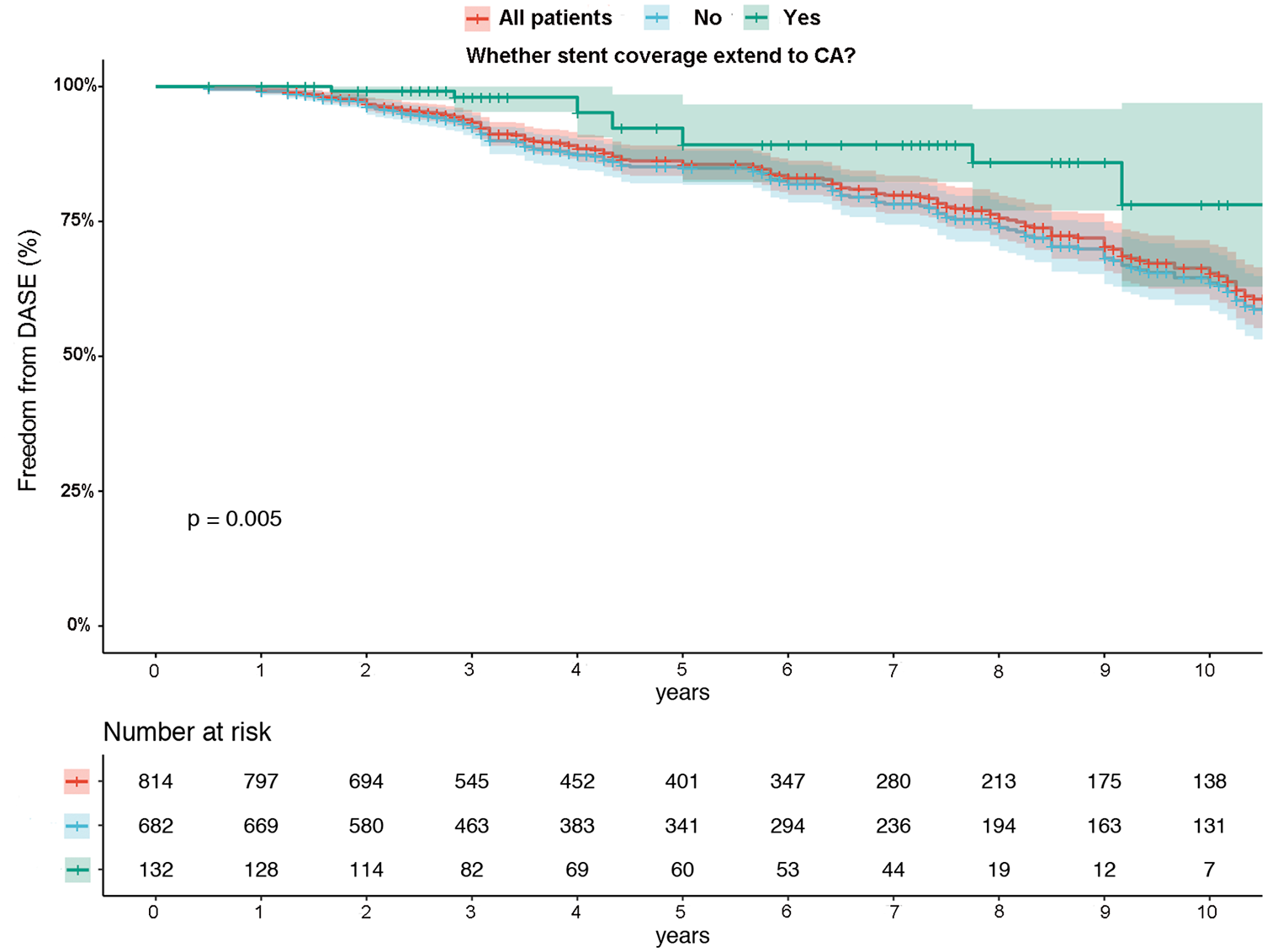
Kaplan–Meier estimates of the freedom from DASE stratified by stent coverage extended to the celiac artery. Kaplan–Meier analysis of freedom from DASE for all of the patients (pink), for patients with stent coverage extended to the celiac artery (green) versus patients without stent coverage extended to the celiac artery (blue). The full lines indicate crude survival estimates. The shaded area indicates the 95% confidence interval. CA, celiac artery; DASE, distal aortic segmental enlargement.
Distal Aortic Remodeling
The details of the morphological features for aortic remodeling are summarized in the Table 4. The length of aortic dissection, complete patent FL, the partial-thrombosed FL, and the total volume of the distal aortic segment were significantly increased in the DASE compared with the non-DASE group, whereas the length of complete-thrombosed FL was decreased in the DASE group (Table 4). We set the postoperative first tear (normally located at the thoracic descending aorta) as the reference to evaluate the distal perfusion in FL. The remodeling-protective predictors (Table 4) were significantly elevated in the non-DASE group compared with the DASE group, including the distance from the postoperative first tear to retrograde perfusion (RP) (shorter RP, p<0.001), and the distance from the postoperative first tear to LSA (lower position, p<0.001). To acquire more details, the readers are referred to Table 4 and Supplementary Table 3. The inter- and intraobserver mean difference for the aortic volume measurement was 0.91 (95% limits of agreement −0.152 to 1.978) and the p value was 0.09, indicating insignificant inter-observer and intra-observer mean differences with regard to the aortic measurement (Supplementary Figure 3). Most commonly, the presentation was pain onset correlated with the location of the dissection. Malperfusion syndromes (≥1 organ) were seen in 15.7% (128/814) of the entire population. Supplementary Table 4 lists the compositional criteria of the cTBAD enrolled in the present study.
Morphological Features of the Aortic Remodeling.
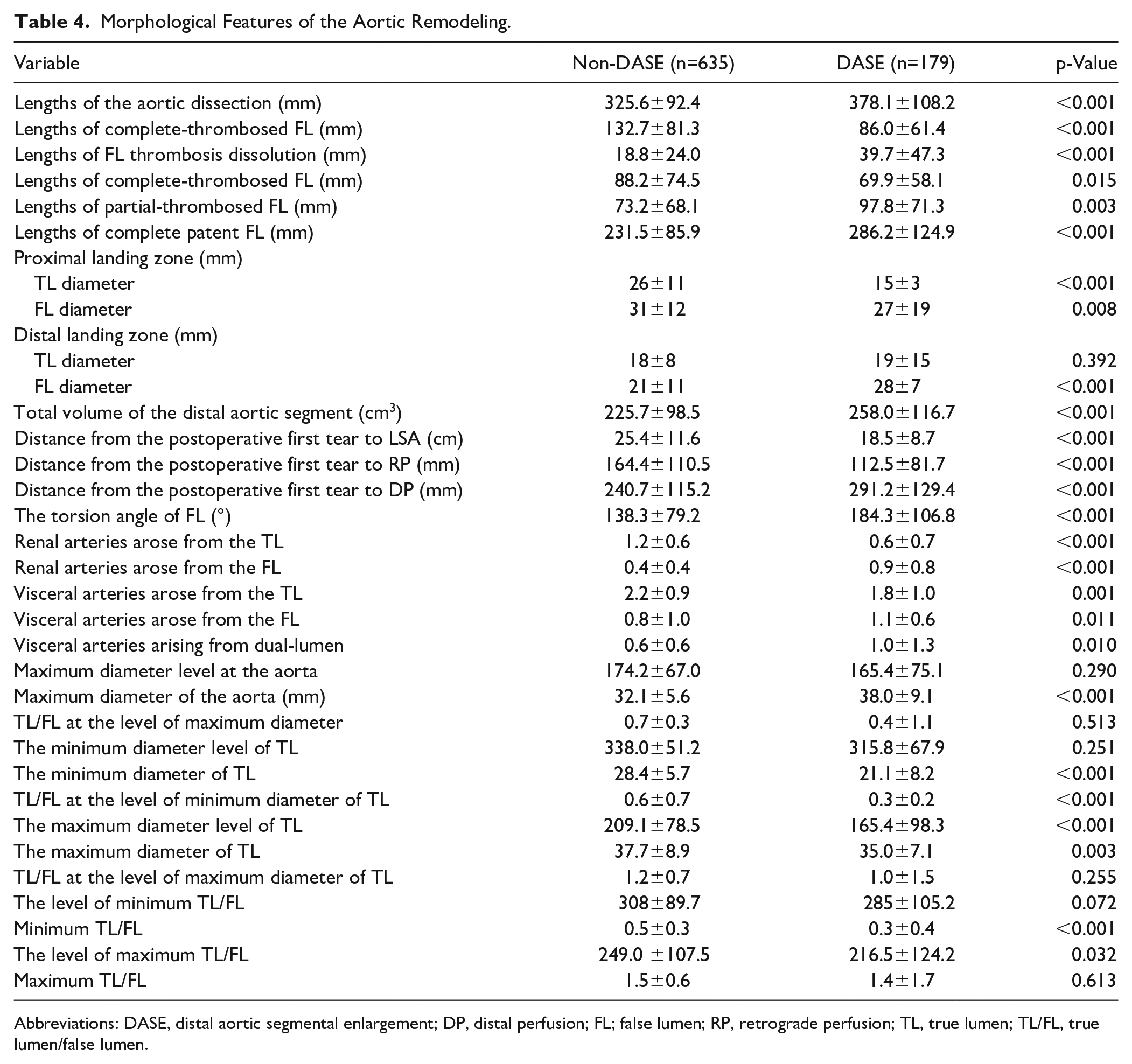
Abbreviations: DASE, distal aortic segmental enlargement; DP, distal perfusion; FL; false lumen; RP, retrograde perfusion; TL, true lumen; TL/FL, true lumen/false lumen.
Discussion
According to the literature, DASE develops in 20%–67% of patients with untreated TBAD,4,6,24 which leads to catastrophic events including aortic dilation, rupture and organ malperfusion. However, the long-term outcome of DASE (including late death and distal aortic reintervention) and the subsequent distal aortic remodeling in a general population with TBAD are still unevaluated. In the present study, the curve of late death with distal aortic reintervention as a competing risk was depicted and analyzed according to whether patients had DASE. The non-DASE group showed a lower rate of late death and distal aortic reintervention than the DASE group (p<0.001, Figure 2). Our data reported the advantage of late death starting in the second years after hospital discharge. It should be noted that the changes in the survival rate normally lagged behind the occurrence of DASE (Figure 5). Despite suggestions of a need for life-long surveillance for patients with TBAD,25,26 early rigorous surveillance (<2 years) of DASE may be valuable for preventing the late death and reintervention.
Previous studies have shown that the patent FL increases the possibility of aortic enlargement,6,9 and might be responsible for a lower survival rate than complete-thrombosed FL. However, little is known about the morphological changes in the distal aortic segments. Therefore, the long-term distal aortic remodeling was evaluated based on a relatively large cohort in our study. Our data confirmed that the length of partial thrombosis FL and complete patent FL in the DASE group were significantly longer (Table 4, p=0.003) than those in non-DASE group whereas the lengths of complete-thrombosed FL were significantly shorter than those in the non-DASE group. However, patients with DASE showed a significantly increased proportion of incomplete FL thrombosis than the non-DASE group above the level of celiac artery (Figure 3). In contrast, there was no marked difference in FL thrombosis between the 2 groups below the level of renal arteries (p>0.05). Because the dissection in the visceral segments requires additional techniques and is not regularly repaired in the index TEVAR procedure, we evaluated the levels of the aorta above the celiac artery. Our result is consistent with a radiological study, which identified that increased partial false lumen thrombosis is strongly associated with late adverse events. 27 Taken together, these results suggest that incomplete FL thrombosis at the level above the celiac artery may be a clue that worthy of investigation for DASE.
According to findings from large registries, the longer stent coverage in thoracic descending aorta is associated with preferred distal aortic remodeling.9,19,28,29 We have previously demonstrated that a short length of stent coverage was an independent risk factor for reoperation in TBAD. 30 The data from the current study suggest that the length of stent-graft coverage was remarkably shorter in the DASE (Table 4, p<0.001) group. Additionally, the occurrence of dSINE was significantly higher in the DASE patients. The aim of extensive aortic stent coverage is to maximize the aortic remodeling benefits of TEVAR, as this has been demonstrated to reduce the aortic dilation and aortic-specific mortality. 31 A meta-analysis for combining proximal covered stent grafting with PETTICOAT (distal adjunctive bare stenting) technique, showed the potential ability to reduce the partial thoracic FL thrombosis rate and the rates of SINE and reintervention but was not associated with lower aorta-related mortality or the complete FL thrombosis rate. 32 Stent-grafting in the distal aorta has an irreplaceable role in improving aortic remodeling. However, in patients with connective tissue disease such as Marfan, remodeling is less successful and endovascular strategies are often discouraged. In the present study, Marfan syndrome was identified as an independent factor that positively associated with DASE.
Pre-emptive endovascular treatment in distal dissection is emerging as a way to prevent late complications. However, longer stent-graft coverage inevitably increases the risk of spinal cord injury (SCI). The optimal range of stent-graft coverage for the general population with fewer spinal complications is unclear.12,13 Xue et al 33 proved that a percentage of stented descending aorta >31.3% (approximately one-third of the length of the descending aorta) would significantly decrease in the risk of thoracic aortic expansion. Our data demonstrated that stent-graft coverage extended to the level between the diaphragm and celiac artery were the significant factors that opposed the occurrence of DASE in a multivariate cox regression model. Patients with prolonged stent coverage to the level of the celiac artery had a significantly lower incidence of DASE than patients who did not (Figure 5). The level of celiac artery may be a “user-friendly” landmark for physicians to locate the range of stent coverage.
The most significant concern associated with extending the stent coverage is SCI. 34 Recently, studies have shown that extended stent coverage carries an acceptable low-risk of spinal cord ischemia in patients with TBAD,33,35 which is consistent with our data. In our cohort, paraplegia was seen in 14 (2.2%) and 5 (2.8%) patients with non-DASE and DASE, respectively (p=0.849). All of the patients who required extensive coverage of the thoracic descending aorta (zone 5–zone 8) and additional distal reintervention received cerebrospinal fluid drainage before the procedures. During the procedure, patients were monitored by a neurologic exam and SBP was augmented to >140 mmHg. This facilitating approach was previously reported. 33
Previous studies have demonstrated better aortic remodeling in the stent-covered aorta and positive remodeling in the proximal thoracic descending aorta was observed earlier than that in the abdominal aorta. 11 Our data showed more extensive stent-graft coverage appears to prevent the DASE after TEVAR. However, the risk of spinal cord injury should be considered prior to extended stent-graft coverage. The present study suggests a reasonable coverage range for reducing the incidence of DASE and the section between diaphragm and celiac artery might serve as a “cost-efficient” plane for reducing DASE. However, further study with long-term follow-up is required to verify these findings.
Limitation
The present study has some limitations. First, this was a multi-center retrospective observational study and it has certain unavoidable limitations due to its retrospective nature. The relative low incidence of DASE (22%) in the total cohort was because this study had excluded the patients who had complications, died or lost to follow-up within 6 months. Second, to reduce the heterogeneity of the study population, the present study did not include the uncomplicated TBAD treated with medication and TBAD in the chronic phase. Third, techniques and strategies have certainly evolved during the long study period, and the outcome is also dependent on the individual presentation.
Conclusion
The current study shows that TBAD patients with DASE had a higher rate of late death and distal aortic reintervention than their non-DASE peers. Our data identified that the level of celiac artery might serve as a “cost-efficient” cutoff point for stenting of the dissected aorta in TEVAR. Extended stent coverage to the level of the celiac artery strongly decreased the incidence of DASE for TBAD.
Supplemental Material
sj-docx-1-jet-10.1177_15266028211036479 – Supplemental material for Extended Stent Coverage Decreases Distal Aortic Segmental Enlargement After the Endovascular Repair of Acute Complicated Type B Aortic Dissection: A Multi-Center Retrospective Study of 814 Patients
Supplemental material, sj-docx-1-jet-10.1177_15266028211036479 for Extended Stent Coverage Decreases Distal Aortic Segmental Enlargement After the Endovascular Repair of Acute Complicated Type B Aortic Dissection: A Multi-Center Retrospective Study of 814 Patients by Junjun Liu, Chaojun Yan, Lubin Li, Hai Feng, Shengmao Xie, Guohui Zhang, Wei Cheng, Mingjin Guo and MingYuan Liu in Journal of Endovascular Therapy
Supplemental Material
sj-docx-2-jet-10.1177_15266028211036479 – Supplemental material for Extended Stent Coverage Decreases Distal Aortic Segmental Enlargement After the Endovascular Repair of Acute Complicated Type B Aortic Dissection: A Multi-Center Retrospective Study of 814 Patients
Supplemental material, sj-docx-2-jet-10.1177_15266028211036479 for Extended Stent Coverage Decreases Distal Aortic Segmental Enlargement After the Endovascular Repair of Acute Complicated Type B Aortic Dissection: A Multi-Center Retrospective Study of 814 Patients by Junjun Liu, Chaojun Yan, Lubin Li, Hai Feng, Shengmao Xie, Guohui Zhang, Wei Cheng, Mingjin Guo and MingYuan Liu in Journal of Endovascular Therapy
Supplemental Material
sj-docx-3-jet-10.1177_15266028211036479 – Supplemental material for Extended Stent Coverage Decreases Distal Aortic Segmental Enlargement After the Endovascular Repair of Acute Complicated Type B Aortic Dissection: A Multi-Center Retrospective Study of 814 Patients
Supplemental material, sj-docx-3-jet-10.1177_15266028211036479 for Extended Stent Coverage Decreases Distal Aortic Segmental Enlargement After the Endovascular Repair of Acute Complicated Type B Aortic Dissection: A Multi-Center Retrospective Study of 814 Patients by Junjun Liu, Chaojun Yan, Lubin Li, Hai Feng, Shengmao Xie, Guohui Zhang, Wei Cheng, Mingjin Guo and MingYuan Liu in Journal of Endovascular Therapy
Supplemental Material
sj-docx-4-jet-10.1177_15266028211036479 – Supplemental material for Extended Stent Coverage Decreases Distal Aortic Segmental Enlargement After the Endovascular Repair of Acute Complicated Type B Aortic Dissection: A Multi-Center Retrospective Study of 814 Patients
Supplemental material, sj-docx-4-jet-10.1177_15266028211036479 for Extended Stent Coverage Decreases Distal Aortic Segmental Enlargement After the Endovascular Repair of Acute Complicated Type B Aortic Dissection: A Multi-Center Retrospective Study of 814 Patients by Junjun Liu, Chaojun Yan, Lubin Li, Hai Feng, Shengmao Xie, Guohui Zhang, Wei Cheng, Mingjin Guo and MingYuan Liu in Journal of Endovascular Therapy
Supplemental Material
sj-png-7-jet-10.1177_15266028211036479 – Supplemental material for Extended Stent Coverage Decreases Distal Aortic Segmental Enlargement After the Endovascular Repair of Acute Complicated Type B Aortic Dissection: A Multi-Center Retrospective Study of 814 Patients
Supplemental material, sj-png-7-jet-10.1177_15266028211036479 for Extended Stent Coverage Decreases Distal Aortic Segmental Enlargement After the Endovascular Repair of Acute Complicated Type B Aortic Dissection: A Multi-Center Retrospective Study of 814 Patients by Junjun Liu, Chaojun Yan, Lubin Li, Hai Feng, Shengmao Xie, Guohui Zhang, Wei Cheng, Mingjin Guo and MingYuan Liu in Journal of Endovascular Therapy
Supplemental Material
sj-tif-5-jet-10.1177_15266028211036479 – Supplemental material for Extended Stent Coverage Decreases Distal Aortic Segmental Enlargement After the Endovascular Repair of Acute Complicated Type B Aortic Dissection: A Multi-Center Retrospective Study of 814 Patients
Supplemental material, sj-tif-5-jet-10.1177_15266028211036479 for Extended Stent Coverage Decreases Distal Aortic Segmental Enlargement After the Endovascular Repair of Acute Complicated Type B Aortic Dissection: A Multi-Center Retrospective Study of 814 Patients by Junjun Liu, Chaojun Yan, Lubin Li, Hai Feng, Shengmao Xie, Guohui Zhang, Wei Cheng, Mingjin Guo and MingYuan Liu in Journal of Endovascular Therapy
Supplemental Material
sj-tif-6-jet-10.1177_15266028211036479 – Supplemental material for Extended Stent Coverage Decreases Distal Aortic Segmental Enlargement After the Endovascular Repair of Acute Complicated Type B Aortic Dissection: A Multi-Center Retrospective Study of 814 Patients
Supplemental material, sj-tif-6-jet-10.1177_15266028211036479 for Extended Stent Coverage Decreases Distal Aortic Segmental Enlargement After the Endovascular Repair of Acute Complicated Type B Aortic Dissection: A Multi-Center Retrospective Study of 814 Patients by Junjun Liu, Chaojun Yan, Lubin Li, Hai Feng, Shengmao Xie, Guohui Zhang, Wei Cheng, Mingjin Guo and MingYuan Liu in Journal of Endovascular Therapy
Footnotes
Acknowledgements
The authors appreciate the dedicated works of Dr. Ning Mao and Ping Yin, Radiologists from the Department of Radiology, Yantai Yuhuangding Hospital; and Shanshan Wu from the Clinical Epidemiology and EBM Unit, National Clinical Research Center for Digestive Diseases, Beijing Friendship Hospital, Capital Medical University for performing the complex statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by research grants from National Natural Science Foundation of China (No. 81900418 and No. 82000429), Beijing Municipal Hospital Scientific Research Training Program Foundation (PX2021002) and Scientific and Technology Program of Beijing Education Commission (KM202110025016).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.