
Abstract
Purpose:
Although rare in occurrence, symptomatic severe aortic stenosis and large thoracoabdominal aortic aneurysm (TAAA) found in combination pose a real therapeutic challenge, especially in elderly frail patients. Surgical approaches for combined treatment are complex and at high risk of complications while staged procedures carry the risk of an unfavorable evolution of the condition temporarily left untreated. Minimally invasive approaches may therefore prove a more suitable strategy for these patients.
Case Report:
We present the case of a 78-year-old woman with symptomatic severe aortic stenosis (AS) and a TAAA of 7.8 cm in diameter. Transcatheter treatment of both conditions was successfully performed in a staged manner. The first intervention consisted of combined transfemoral transcatheter aortic valve implantation (TAVI) immediately followed by a zone 3 thoracic endovascular aortic endoprosthesis deployment. In order to reduce the extent of intercostal arteries coverage and mitigate the risk of medullar ischemia, a second-stage percutaneous endovascular treatment of the TAAA was performed with a customized 4-fenestration prosthesis. Early and 12-month clinical and radiologic follow-up were favorable.
Conclusion:
This case demonstrates how a strong multidisciplinary collaboration allows for successful resolution of complex clinical scenarios.
Keywords
Introduction
Frail patients presenting with both severe aortic stenosis and large thoracoabdominal aortic aneurysm (TAAA) pose a challenge. An optimal management strategy aims at timely treatment of both potentially fatal conditions while mitigating the risks of combined vs staged procedures. Considering the availability of surgical, transcatheter, or hybrid procedures and different timing scenarios, multiple pathways of treatment can be derived. Combined interventions may be complex and lengthy while convalescence time and complications following initial procedures might postpone further treatment and increase the risk of unfavorable evolution, including aneurysm rupture. 1 It is now well established that frail patients deemed at higher risk for open surgery benefit from minimally invasive techniques in both fields.2–5 However, the optimal sequence of treatment is unknown. In this report, we discuss the rationale and techniques applied to achieve successful multidisciplinary management of a patient presenting with severe aortic stenosis and a large thoracoabdominal aneurysm.
Case Report
A 78-year-old woman was transferred to our aortic center following fortuitous discovery of a large TAAA. She initially presented with worsening dyspnea New York Heart Association classification grade 3/4. Her past medical history included hypertension dyslipidemia, multifactorial anemia, and asthma, whereas surgical history was unremarkable for a previous uncomplicated bladder intervention.
Upon initial investigation, chest X-ray revealed a large thoracic aneurysm. A computed tomography angiography (CTA) confirmed a 7.8 cm type 5 TAAA. The aneurysm extended down to the origin of the superior mesenteric artery. The celiac trunk, superior mesenteric artery, and both renal arteries were patent. The ascending thoracic aorta was 5.0 cm in diameter. The aortic valve was heavily calcified, and physical examination was compatible with severe aortic stenosis. A transthoracic echocardiogram confirmed the diagnosis of 0.8 cm2 severe stenosis on a native tricuspid aortic valve. Biventricular function was preserved and pulmonary artery pressures were normal. The patient was autonomous and performed self-care; however, a minor neurocognitive disorder was suspected. Blood tests revealed chronic renal insufficiency (38 mL/minute/1.73 m2 glomerular filtration rate) as well as mild normocytic anemia (hemoglobin 106 g/L and hematocrit 33.9%). Subsequent coronary angiography demonstrated only mild coronary artery disease.
At this point, 2 treatment options were considered. The first scenario consisted of surgical replacement of both the stenotic aortic valve and the 5-cm-dilated ascending aorta. Following a period of convalescence, a staged endovascular fenestrated treatment of the TAAA would be executed. This option had the advantage of definitive treatment of the ascending aorta but involved a high-risk cardiothoracic surgery and would delay TAAA repair with the associated increased risk of rupture.
The other option combined a transcatheter aortic valve implantation (TAVI) procedure followed by staged treatment of the TAAA. First stage would consist of proximal zone 3 thoracic endovascular repair (TEVAR) immediately after the TAVI, providing this step was uneventful. Second stage would consist of a percutaneous endovascular treatment with a customized 4-fenestration prosthesis. This option allowed for faster treatment of the large TAAA and minimally invasive management of both conditions. The risk of medullar ischemia would be reduced by limiting intercostal coverage and allowed for vascular adaptation between the staged endovascular repairs. However, the ascending aorta dilation would be left untreated and require careful surveillance for potential progression during follow-up. After thorough multidisciplinary discussion, the team and patient opted for this latter strategy.
The procedure was performed under general anesthesia in a hybrid operating room. Transfemoral TAVI with a 26-mm Edwards SAPIEN 3 valve was performed uneventfully. Using the same transfemoral access, 2 proximal thoracic endoprosthesis (Cook ZTA-PT-38-34-217 and Cook ZTA-PT-36-32-161, Bloomington, USA) were inserted and deployed from zone 3, just past the left subclavian artery, down to the distal descending thoracic aorta, above the celiac trunk.
During the hospital stay, the patient required permanent pacemaker implantation for a fascicular block and was treated for pneumonia. She was discharged 19 days after the combined procedure. The customized fenestrated descending thoracoabdominal endoprosthesis was ordered the day of the first operation and was manufactured and available 4 weeks later.
Stage 2 was therefore undertaken 38 days after stage 1 under general anesthesia with a spinal drain in place and percutaneous arterial access using the preclose technique. The customized fenestrated endoprosthesis was inserted through the left transfemoral access site and deployed in the distal thoracic stent area such that the fenestrations were appropriately oriented toward the visceral arteries. Three fenestrations and their destined visceral vessels (the superior mesenteric artery and renal arteries) were selectively cannulated and bridging covered stents of 8 mm×32 mm, 6 mm×32 mm, and 7 mm×32 mm were deployed. A molding balloon was used to ensure adequate sealing before the visceral bridging stents deployments. The celiac trunk was then cannulated with a steerable sheath, allowing the last bridging stent implantation. Angiographic control demonstrated good permeability of the visceral and internal iliac arteries. No major endoleaks were observed and blood loss was less than 100 cc.
The patient was discharged home 2 days later with no complications. The first control CTA performed at 6 weeks showed complete thrombosis of the TAAA with no endoleaks. The ascending aorta diameter was stable. Follow up echocardiography revealed a functional TAVI prosthesis with a mean pressure gradient of 6 mmHg and trace paravalvular regurgitation. Clinical and imaging follow-up at 6 and 12 months were favorable with a reduction in TAAA diameter of 10 mm on CTA (Figure 1).
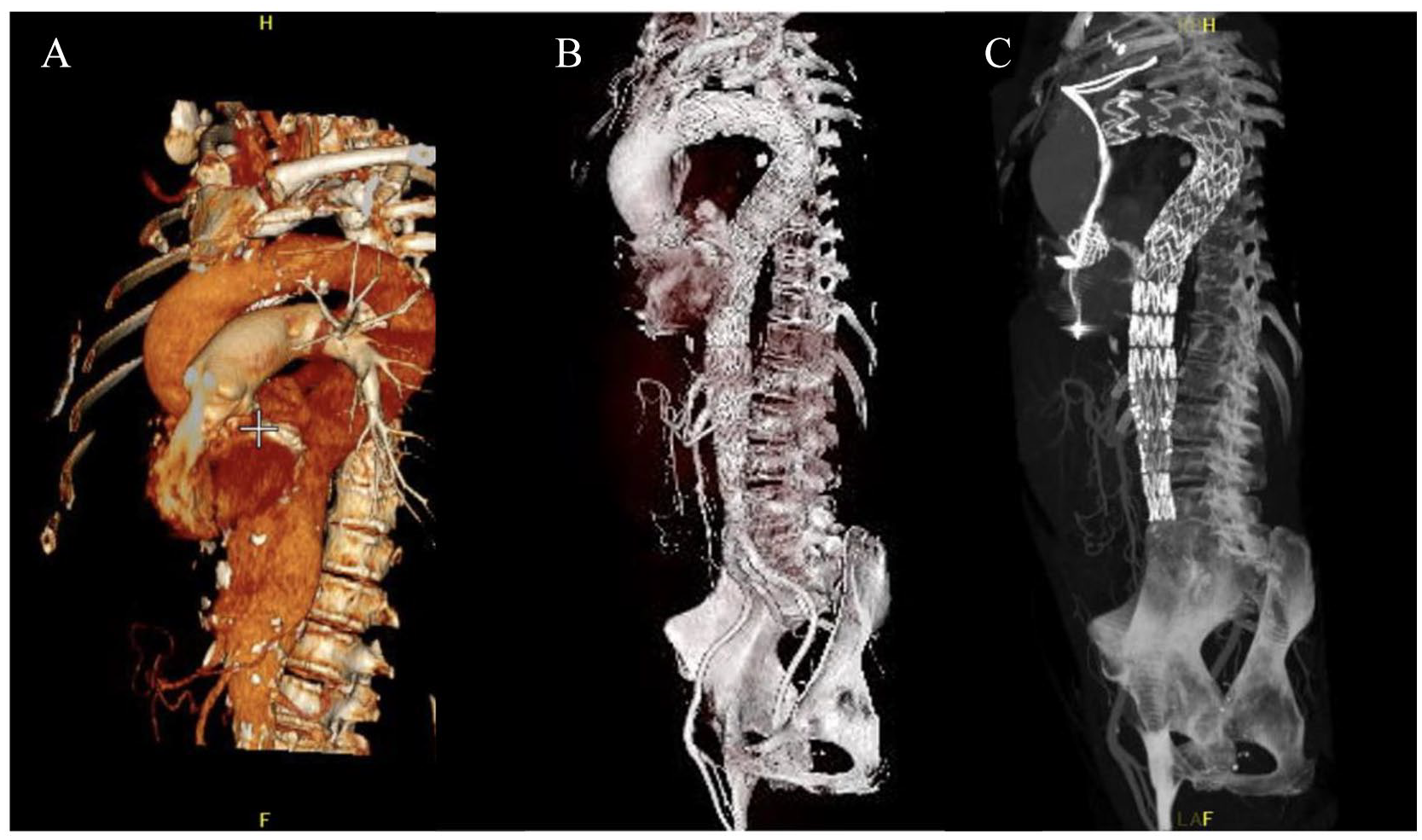
(A) Preoperative 3D imaging of the thoracoabdominal aortic aneurysm. (B) and (C) Postoperative 3D reconstruction with the aortic valve and the aortic thoracic and fenestrated endoprosthesis in place.
Discussion
In patients with both a severe aortic stenosis and large aortic aneurysm, TAVI allows faster treatment of associated aortic aneurysm. This is especially useful in frail patients with large aneurysm.
Once TAVI is performed, blood pressure often rises after removal of the pressure gradient of the aortic valve. This might increase the risk of aneurysm rupture. 6
We present a staged surgical intervention, which consists of a TAVI associated with a staged TAAA repair in order to reduce the risk of medullar ischemia. The multidisciplinary collaboration for careful preparation of the intervention have been highlighted.
Most case reports found in the literature describe the successful use of a combined TAVI and aortic aneurysm treatment in the context of a descending thoracic or an infrarenal aortic aneurysm.7–9 In situations where the risk of spinal cord ischemia is lower, and the endovascular treatment simple, a combined definitive treatment can be offered to immediately reduce the risk of aneurysm rupture. We also had success treating those patients with a combined approach. Endovascular aortic or iliac treatment can also be combined with TAVI in case of the rare complications of iatrogenic aortic rupture during TAVI.
However, when AS is associated with an asymptomatic thoracoabdominal aneurysm, we preferred to stage the aortic coverage, which might reduce the risk of medullar ischemia that is associated with TAAA treatment. 10 Reducing the extent of aortic coverage and therefore the number of intercostal arteries covered in a single session allows the spinal cord collateral network to adapt to a reduction in perfusion pressure. 11
In our case, it was determined that a customized device was the most appropriate treatment option. The fenestrated component was designed to land within the distal thoracic component implanted as a first stage. The device was configured with large (strut free) fenestrations for the celiac trunk and superior mesenteric artery, and small fenestrations for the renal arteries. The custom endograft required 4 weeks to be produced and it imposed a delay before the final stage of repair with an associated risk of rupture. A single-center study concluded that intercurrent aneurysm rupture is a rare event (18/906, 2%); however, larger aneurysms are at higher risk of rupture during the waiting time for a customized stent graft. In this specific study, the delay between endograft order and procedure was 12 weeks. 12 Other options are to be considered when this delay is unacceptable such as patients with ruptured or symptomatic aneurysm or large aneurysm. Off the shelf endograft such as the T-branch from Cook might be offered depending on aortic and visceral artery morphology and allow immediate treatment. While we have limited experience with off the shelf option, iliac access, visceral arteries diameter and downward direction, and aortic luminal diameter at the level of the visceral arteries were all favorable for a T-branch in this case. Other options include hybrid treatment with open debranching of the visceral arteries followed by endograft exclusion of the TAAA. Finally, an open TAAA repair, in situ laser fenestration, physician- modified endograft and chimney or periscope, are also other options that can be considered.
Conclusion
In conclusion, a patient with symptomatic severe aortic stenosis and large TAAA was successfully treated in a staged manner by a combined TAVI immediately followed by a zone 3 thoracic endovascular aortic endoprosthesis deployment and a second-stage percutaneous endovascular treatment of the TAAA with a customized 4-fenestration prosthesis. The staging of the aortic coverage allowed to reduce the risk of medullar ischemia that is associated with TAAA treatment. This case demonstrated how a multidisciplinary collaboration allows for successful resolution of complex clinical scenarios.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.