
Abstract
Objective
Endovascular treatment through either percutaneous transluminal angioplasty (PTA) alone or stenting has been previously used as a treatment for transplant renal artery stenosis (TRAS). This review aimed to investigate the results of endovascular treatment for renal artery stenosis in transplanted kidneys as compared with the outcomes of interventions, medical management, and graft survival in non-TRAS patients.
Methods
A systematic review of PubMed, Google Scholar, Cochrane, and Scopus was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines in which studies that reported outcomes of the treatment of TRAS via the endoluminal approach were identified, and their results were meta-analyzed.
Results
Fifty-four studies with a total of 1522 patients were included. A significant reduction of serum creatinine level was found, favoring the stenting group, with a mean difference of 0.68 mg/dL (95% confidence interval (CI), 0.17–1.19; Z=2.60, p=0.0009). Comparison of pre- and post-intervention values of any intervention revealed a significant decrease in overall serum creatinine level (0.65 mg/dL; 95% CI, 0.40–0.90; Z=5.09, p=0.00001), overall blood pressure, with a mean difference of 11.12 mmHg (95% CI, 7.29–14.95; Z=5.59, p=0.00001), mean difference in the use of medications (0.77; 95% CI, 0.29–1.24; p=0.002), and peak systolic velocity (190.05; 95% CI, 128.41–251.69; p<0.00001). The comparison of serum creatinine level between endovascular interventions and best medical therapy favored endovascular intervention, with a mean difference of 0.23 mg/dL (95% CI, 0.14–0.32; Z=5.07, p<0.00001). Graft survival was similar between the treated patients and those without TRAS (hazard ratio, 0.98; 95% CI, 0.75–1.28; p=0.091). The overall pooled success rate was 89%, and the overall complication rate was 10.4%, with the most prevalent complication being arterial dissection.
Conclusion
The endovascular treatment of TRAS improves graft preservation and renal function and hemodynamic parameters. PTA + stenting appears to be a more effective option to PTA alone in the stabilization of renal function, with additional benefits from decreased restenosis rates. Further high-quality studies could expand on these findings.
Keywords
Introduction
Renal transplantation remains the mainstay definitive treatment for end-stage renal disease. 1 Transplant renal artery stenosis (TRAS) is a possible vascular complication with an incidence of approximately 1% to 23% that results in compromised graft perfusion and function.2,3 The onset of TRAS may be acute or gradual, presenting as worsening renal function and/or cardiac destabilization syndrome, commonly worsening or refractory hypertension, and less frequently as acute pulmonary edema or congestive heart failure.4,5 TRAS may ultimately lead to allograft failure.5,6
The pathophysiology of TRAS is a complex interplay of various immune, infectious, atherosclerotic, and surgical components. Surgical nuances, such as the surgical technique, anastomosis technique, and trauma, have been identified to play a significant role.6–12
The application of various noninvasive imaging modalities to assist diagnosis in clinically suspicious cases is a commonly employed strategy. These include color Doppler ultrasonography (DUS), magnetic resonance imaging (MRI), or computed tomography (CT); however, the usefulness of the 2 latter modalities may be limited by patients’ renal functions. 13 Consensus over ultrasonographic cutoff values for TRAS is yet to be reached; however, most authors used a peak systolic velocity (PSV) of 200 cm/s on DUS, which is the same proposed cutoff for native renal artery stenosis (RAS). 14 Though invasive, angiography allows confirmation and endovascular treatment during the same intervention.15,16 Prompt identification and treatment are critical in preventing increased risks of graft loss and death. 6
Surgery through direct visualization of the vessel was considered the classic norm for the treatment of TRAS; however, endovascular treatment through percutaneous transluminal angioplasty (PTA) largely displaced open surgical approaches.4,17 This intervention can restore kidney perfusion in up to 90% of cases, with associated improvement in renal function, which translates clinically to the normalization of renal function and blood pressure.2,12,18–21 Adequate prompt treatment has improved survival in patients with TRAS; prior studies concluded similar 10-year survival rates in patients with TRAS who underwent endovascular treatment and transplanted patients without TRAS. 22
Diversity in the available literature is mainly limited by its low level of evidence. This review and meta-analysis aimed to pool evidence and answer 4 main questions as follows: Is PTA an effective treatment for reducing blood pressure, creatinine level, and medication consumption? Is it more effective than pharmacological treatment? Is stenting more effective than PTA alone? Do endovascular interventions improve graft survival?
Materials and Methods
Search and Identification Strategy
By following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 23 guidelines, a systematic review of the current English literature was performed to identify articles describing the endovascular treatment of patients with TRAS up to February 2021. The databases included were PubMed, Cochrane, Google Scholar, and Scopus. The search keywords used were “Transplant Renal Artery Stenosis,” “Endovascular Treatment,” “Management,” “Percutaneous Transluminal Angioplasty,” and “Transplant.” Articles were initially screened through their titles and/or abstracts. Relevant manuscripts were retrieved for screening, further review, and data extraction by 2 authors (SUVDL and MTM). Data were conciliated by a third author (LCBG). Exclusions were applied to studies predating 1999, case reports, and case series of fewer than 3 patients. Articles describing endovascular management of TRAS through either PTA or PTA and stenting (PTAS), and reporting outcomes were included. Defined through a patient, intervention, comparison, outcome, and sometimes time (PICOT) question formulation, the selected articles included patients with TRAS treated with interventions such as PTA/PTAS. Various controls were included, such as patients without TRAS in the studies that compared graft survival, patients with pre-intervention patient values in studies that compared pre- and post-intervention outcomes, and patients who underwent PTA in studies that compared PTA alone and stenting. The measured outcomes were creatinine levels, blood pressure levels, use of medications, PSV, and survival hazard ratios (HRs). Studies that omitted statistical comparisons of interest but detailed their diagnostic or success criteria were included for summarizing the parameters and qualitative synthesis. The PRISMA flowchart is displayed in Figure 1.
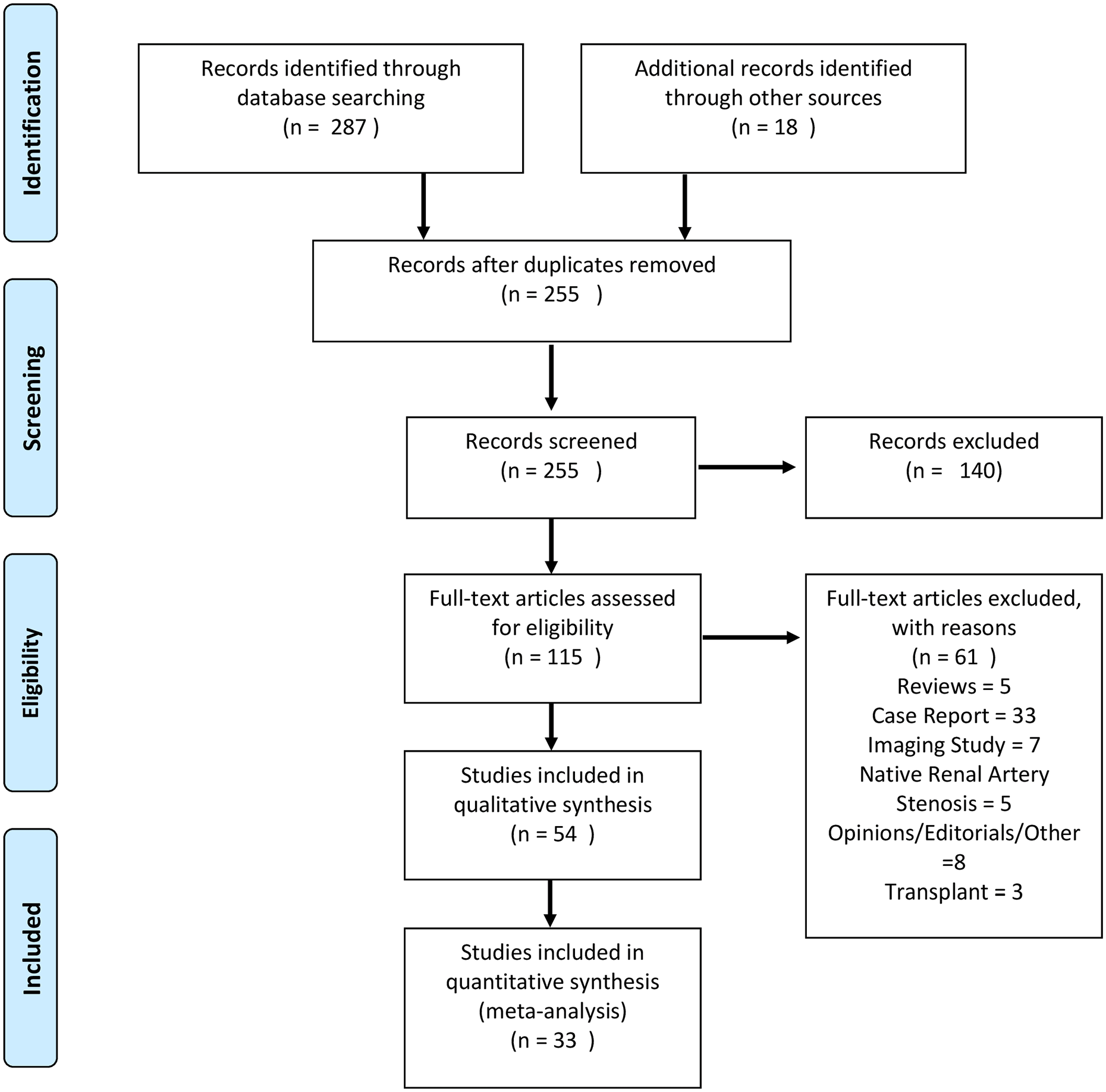
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart.
Data Extraction and End Points
As previously stated, creatinine level, blood pressure, medication use, and PSV were extracted from the studies that provided pre- and post-intervention values, and those that compared PTA and PTAS, or PTA and medical treatment. HR was estimated from the graft survival curves in studies that compared between patients with endovascularly treated TRAS and non-TRAS transplantees.
Bias Analysis and Evidence Grading
Evidence was graded using the Oxford Centre for Evidence-Based Medicine-Levels of Medicine grading system. 24
Data Analysis
A meta-analysis was performed using Review Manager 5.2 (Cochrane Collaboration). Heterogeneity was assessed using Q-statistic and its resulting I2 value and p-value. Values >50% or <0.05 were considered significant for data heterogeneity. Should heterogeneity in data be identified, the analysis was performed using a random-effects model, as opposed to a fixed-effects model in data with no significant heterogeneity. Comparison between the 2 interventions was determined by measuring the effects of treatment on changes in creatinine level, blood pressure, number of antihypertensive medications needed, and PSV between the baseline and endpoint values of the studies. When articles did not report the mean and standard deviation (SD) of the change from baseline to end point, the following equations were used to calculate them as follows:

Studies that compared pre- and post-intervention variables introduced the results as pre- and post-intervention values. When studies provided results at various time points, the results were grouped into short-term (post-intervention to 1 month), medium-term (3–6 months), and long-term studies (12+ months). Studies not describing time periods were included in the short-term group. Studies that provided various time points that could be allocated into a single group were considered on the basis of the closest established time frame. Egger’s funnel plots were visually inspected for asymmetry for possible publication bias. These can be found in Supplemental Figure S2 for Creatinine, mean arterial pressure (MAP), Restenosis, Creatinine, and Graft Survival. 26 Cochrane’s risk of bias tool was not used, as no randomized studies have been conducted on this topic and instead, studies were graded for quality using Oxford’s Evidence Grading Score. 24
Results
Overview
A total of 54 original articles met the inclusion criteria, including 1522 patients diagnosed as having TRAS with angiographic confirmation of >50% luminal stenosis. The median cohort size was 24; the patient age ranged from 7 to 81 years, and the median of the mean age was 47 years. Only 35 studies provided enough data for meta-analysis. An overall summary of the included studies, size, and evidence grading can be found in Supplemental Table S12,4,7,12,27-77. We propose a diagnostic and therapeutic algorithm that reflects the findings, which is displayed in Figure 2 on the basis of the frequency of reporting cutoff parameters. Table 1 summarizes the findings of the meta-analysis.
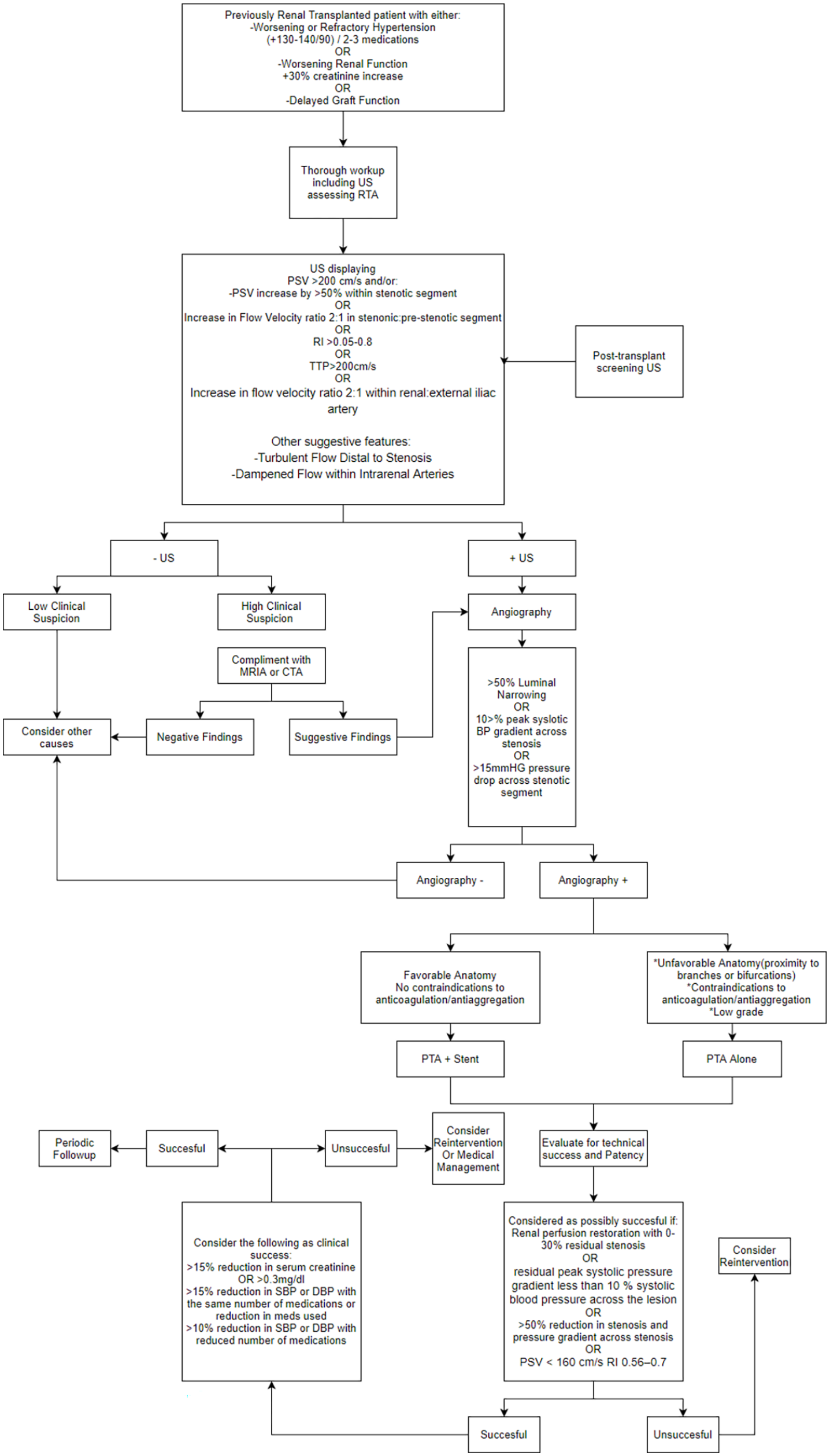
Proposed diagnostic and therapeutic algorithm based on the frequency of the report of definitions and meta-analyzed data suggesting the effectiveness of endovascular interventions.
Summarizes Overall Findings of Our Meta-Analysis of Included Studies Including Comparisons Between Pre- and Post-Interventions, Medical Management, Effect Size Between Different Interventions, and Graft Survival Compared to TRAS Patients.
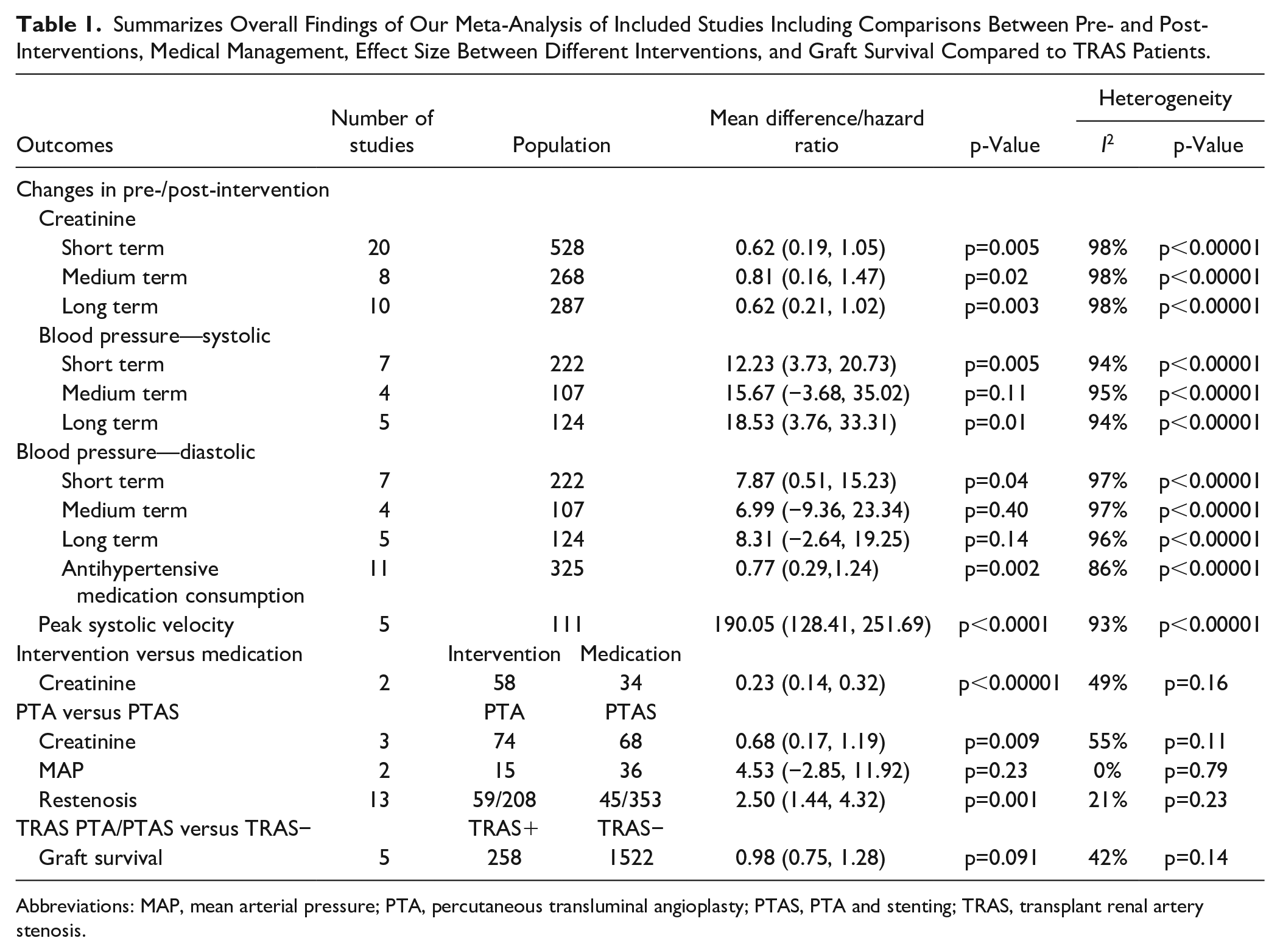
Abbreviations: MAP, mean arterial pressure; PTA, percutaneous transluminal angioplasty; PTAS, PTA and stenting; TRAS, transplant renal artery stenosis.
Clinical Presentation
The clinical presentation was described in 1121 patients, of which 371 (33.0%) presented with hypertension, 363 (32.7%) presented with worsening renal function, and 340 (30.2%) presented both. Only 47 asymptomatic patients (4.1%) were detected through post-transplant imaging screening.
Diagnostic Criteria
Various studies reported clinical and imaging criteria, either through angiography and/or ultrasonography, for the diagnosis. These varied widely within studies and are summarized in Supplemental Table S2.
Comparison of Percutaneous Angioplasty Alone and Stenting
Three studies compared PTA alone and PTAS.
Creatinine
Three studies provided data on mean change in creatinine levels after PTA or PTAS. A total of 74 patients underwent PTA, and 68 underwent PTAS, yielding a mean difference of 0.68 mg/dL (95% confidence interval (CI), 0.17–1.19; Z=2.60, p=0.0009) in creatinine levels, favoring stenting. Findings in Figure 3A. Funnel plot is displayed in Supplemental Figure S2A.
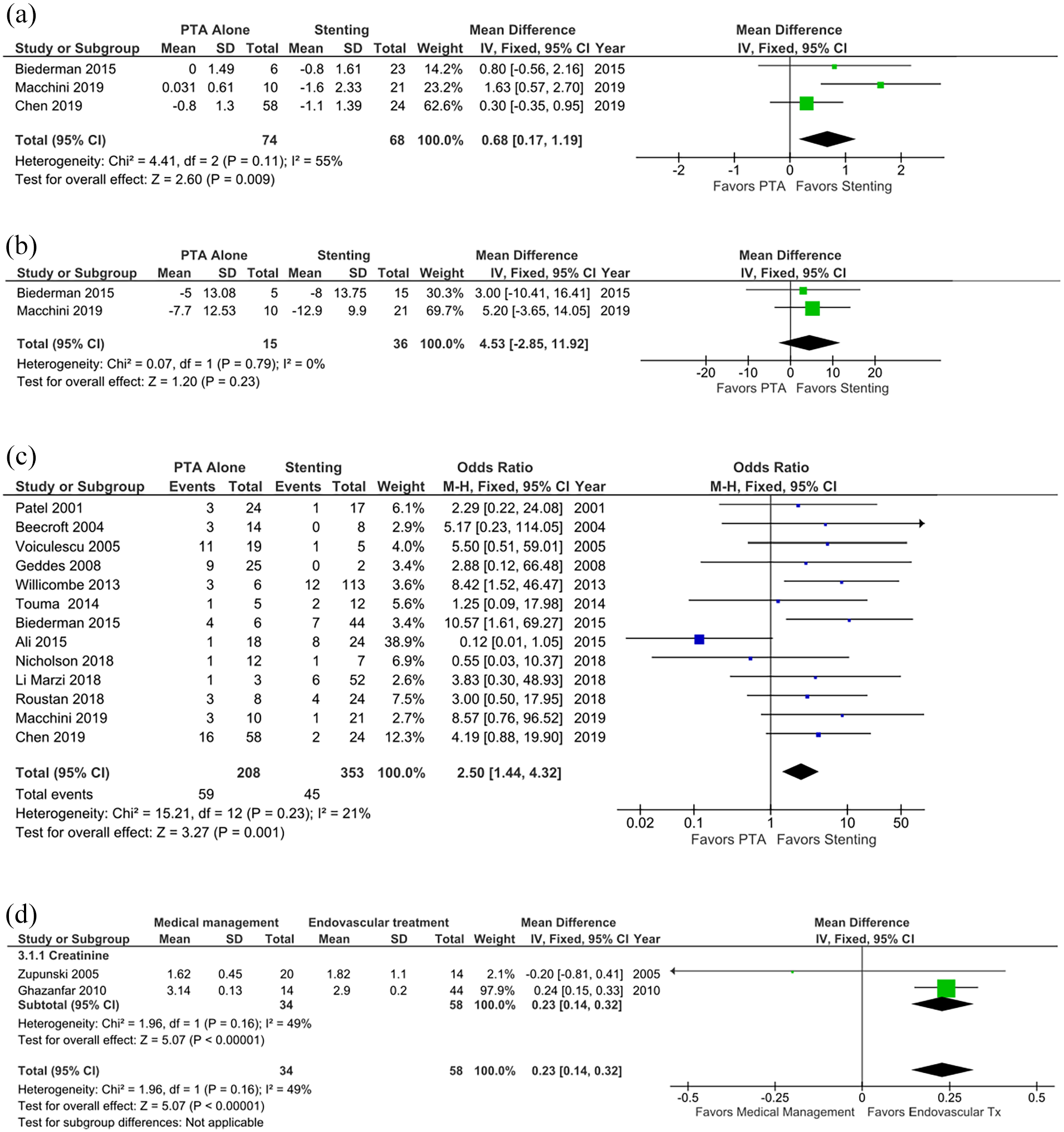
Forest plot of analyzed parameters across various comparisons of differing interventions. (A) Forest plot comparing outcomes of reported comparisons of serum creatinine and mean arterial pressure (MAP) in PTA alone versus PTA with stenting. (B) Forest plot comparing outcomes of reported comparisons of MAP in PTA alone versus PTA with stenting. (C) Forest plot comparing restenosis rates after PTA alone versus PTA with stenting. (D) Compares outcomes of serum creatinine in best medical management versus endovascular treatment.
Mean Arterial Pressure
Two studies provided post-intervention MAP data. A total of 15 patients who underwent PTA were compared with 36 patients who underwent PTAS. A meta-analysis revealed a mean difference of 4.53 mmHg (95% CI, −2.85 to 11.92; Z=1.20, p=0.23). These findings are displayed in Figure 3B. Funnel plot is displayed in Supplemental Figure S2A.
Restenosis
While only 3 studies provided direct statistical comparisons between PTA and PTAS, 13 mentioned restenosis rates in patients treated with either PTA alone or PTAS. Of 208 patients who underwent PTA, 59 developed restenosis, whereas 45 cases of restenosis were found in 353 patients treated with PTAS. A meta-analysis of these data yielded a significant odds ratio of 2.50 (95% CI, 1.44–4.32; p=0.001), which suggests decreased restenosis when stents were used. The findings are shown in Figure 3C. Funnel plot is displayed in Supplemental Figure S2B.
Comparison Between Endovascular Intervention and Medical Treatment
Two studies compared endovascular management and the best available medical treatment. Medical management was used in 34 patients, whereas endovascular interventions were performed in 58 patients. The results that compared serum creatinine levels between the groups favored endovascular intervention, showing a 0.23 mg/dL (95% CI, 14–0.32) mean difference (Z=5.07 and p=0.00001). These findings are displayed in Figure 3D.
Impact of Endovascular Intervention
Serum creatinine concentrations, blood pressure measurements, use of medications, and PSV were provided by up to 20 studies in various time frames. These were stratified into short-term (0–1 month), medium-term (3–6 months), and long-term groups (12+ months).
Serum Creatinine
A grand total of 20 studies provided pre- and post-intervention values, adding a total of 528 patients. Significant differences in creatinine levels before and after intervention were found among the 3 groups. The mean differences were 0.62 mg/dL (95% CI, 0.19–1.05; p=0.005) for 528 patients in the short-term group, 0.81 mg/dL (95% CI, 0.16–1.47; p=0.02) for 268 patients in the medium-term groups, and 0.62 mg/dL (95% CI, 0.21–1.02; p=0.003) for 287 patients in the long-term groups. These yielded an overall decrease of 0.65 mg/dL (95% CI, 0.40–0.90; p=0.00001). These findings are displayed in Supplemental Figure S1A. Funnel plot is displayed in Supplemental Figure S2C.
Blood Pressure
Graphing of pre- and post-intervention blood pressure measurements, such as systolic, diastolic, and mean arterial blood pressure showed favorable post-intervention values, with statistically significant mean differences in systolic, diastolic, and mean blood pressure readings between various time points. These findings are further detailed and summarized in Supplemental Figure S1B. Funnel plot is displayed in Supplemental Figure S2D.
Antihypertensive Medication Use
Eleven studies compared the use of medications before and after the intervention, providing pooled data of 325 patients. Analysis results favored intervention showing a mean difference of 0.77 (95% CI, 0.29–1.24; Z=3.17, p=0.002), concluding a significant decrease in the use of antihypertensive medications after undergoing endovascular intervention. These findings are displayed in Supplemental Figure S1C.
Peak Systolic Velocity
Changes in PSV are described in 5 studies, with a total population of 111 patients. An analysis revealed a significant reduction in PSV after intervention, with a mean difference 190.05 cm/seg (95% CI, 128.41–251.69; Z=6.04, p<0.000001). This is displayed in Supplemental Figure S1D.
Graft Survival
Five studies compared graft survival between 258 patients with TRAS treated with endovascular management and 1526 transplanted patients without TRAS. Three of these studies featured patient matching, and 2 featured consecutive cases. Plotting of data extracted from survival curves revealed no significant difference in survival rates between patients with endovascularly treated TRAS and the transplanted patients without TRAS (HR, 0.98; 95% CI, 0.75–1.28; p=0.091). The results are further shown in Figure 4. Funnel plot is displayed in Supplemental Figure S2E.
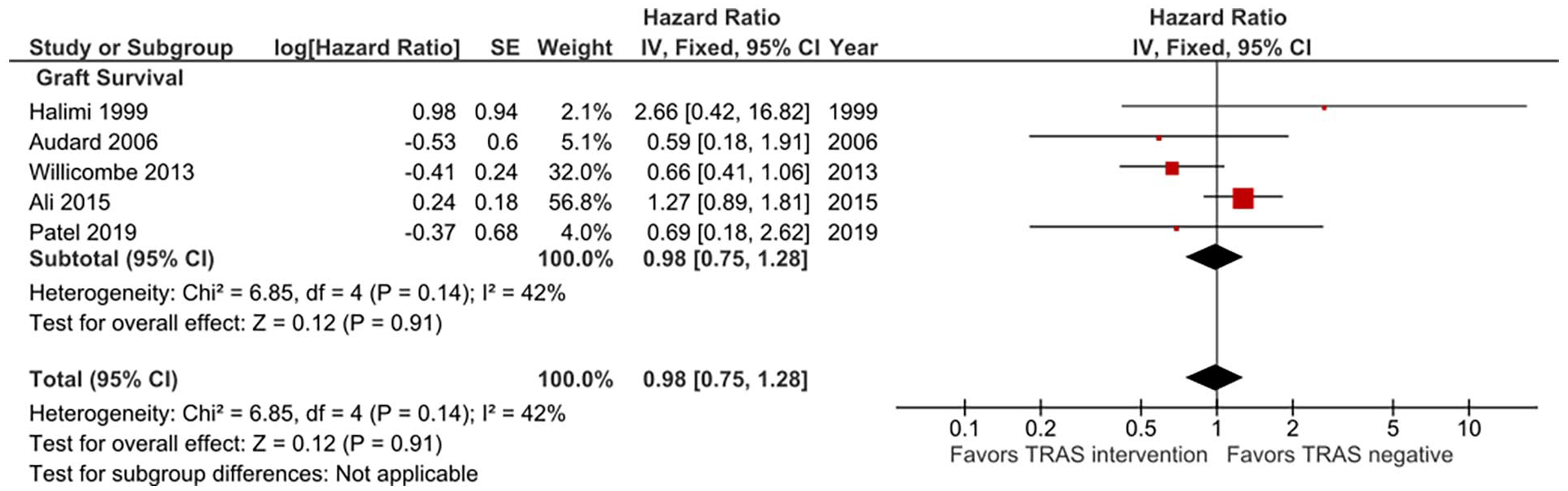
Forest plot comparing hazard ratios of patients without TRAS to those with TRAS treated through endovascular management for graft survival.
Clinical Success and Complications
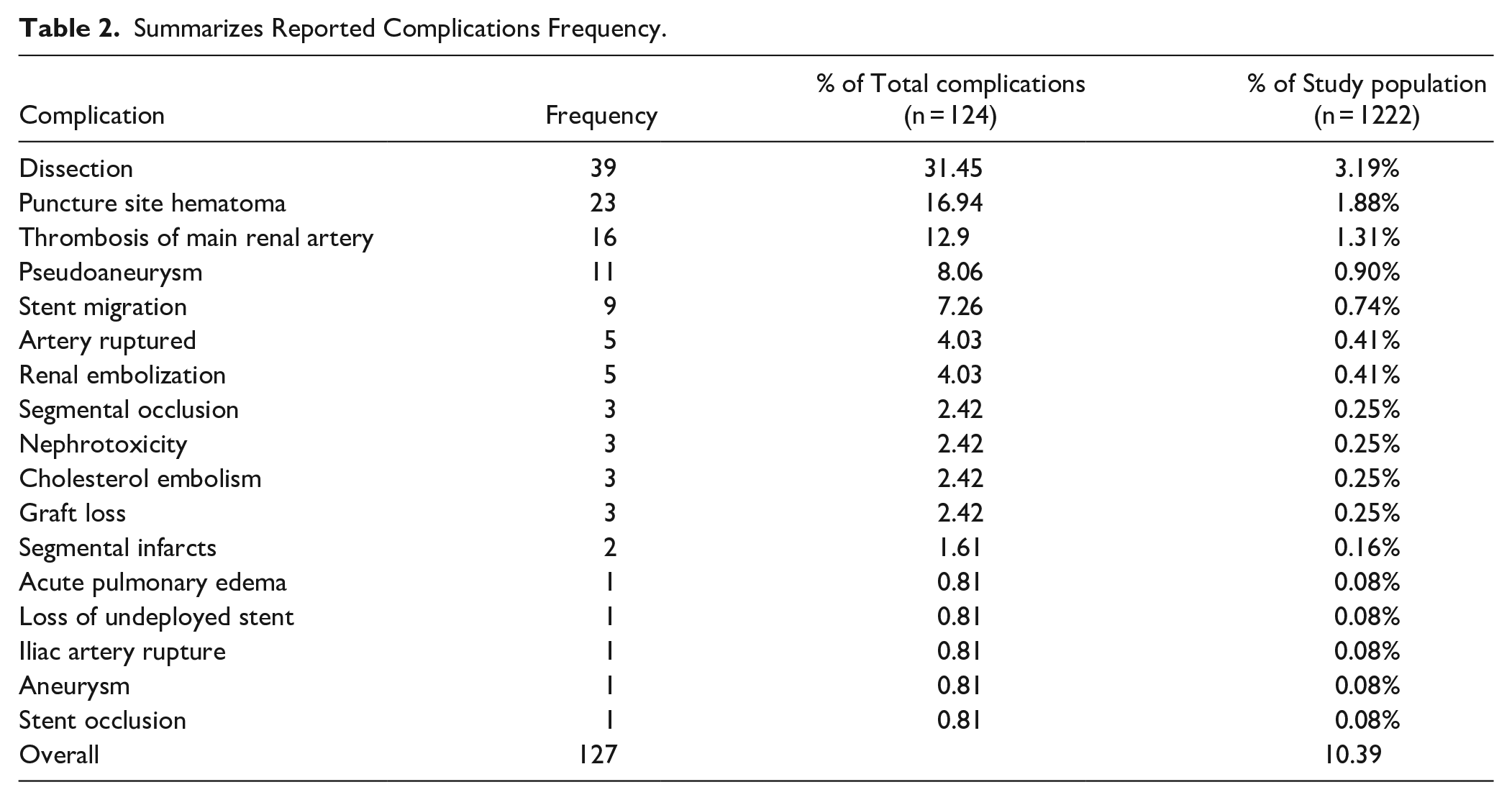
We used varying definitions of technical success on the basis of post-intervention angiography and clinical parameters, such as residual luminal narrowing, normalizing creatinine level, and blood pressure. These are aggregated in Supplemental Table S2. While the clinical success rate ranged from 65.5% to 100%, with a median of 97%, the pooled success rate was 89%. The overall pooled complication rate was 10.4%, with the most common being arterial dissection, representing 31.4% of complications and 3.1% of all cases. The definitions of success are summarized in Supplemental Table S2. The reported aggregated complications are summarized in Table 2.
Summarizes Reported Complications Frequency.
Discussion
The RT remains to be the definitive treatment for end-stage renal disease, offering improvements in quality of life when compared with other therapeutic options such as hemodialysis. 78 Decades of research on surgical techniques, patient matching, and post-transplant management have led to excellent outcomes. 79 The current estimated patient survival rates at 1, 5, and 10 years are 96.6%, 91.5%, and 87.1%, respectively. 22
Compromises in renal vascular flow pose a major threat to renal function and, in the case of transplanted patients, a risk to graft viability, thus necessitating prompt treatment. Willicombe previously described decreased graft survival in patients with untreated TRAS and the positive impact of endovascular intervention on graft survival. 56 The findings that we derived from analyzing available evidence suggest the vital role of endovascular management of patients with TRAS, as this intervention shows non-different graft survival in patients with endovascular treatment for TRAS and transplanted patients without TRAS.
An accurate diagnosis must first be preceded by clinical suspicion, in which similarities in presentations of native RAS and TRAS may be observed. These commonly manifest clinically as treatment-resistant hypertension or worsening renal function in specific demographic groups. These features should be further investigated by a thorough workup, including imaging. DUS is a common choice owing to its low cost and invasiveness and diagnostic capabilities; however, its diagnostic accuracy is variable and dependent on the user’s expertise.80–83 Diagnostic cutoff values are yet to be properly defined; nevertheless, most included studies used the cutoff value of 200 cm/s, the same value used in native RAS. Some authors have raised concerns over the sensibility and specificity of these values in TRAS, signaling the need for further dedicated high-quality studies. Nonetheless, reviewed studies most frequently used 200 cm/s as a cutoff in combination with other variables further displayed in Supplemental Table S2. Other imaging applications such as CT angiography and MRI may be used to a similar effect. 84 Patients with flow abnormalities identified through screening represented a few cases and would benefit from dedicated studies; however, the currently published literature suggests endovascular treatment as an adequate therapeutic option.
Confirmation is achieved through angiography, and most studies used a 50% to 70% luminal narrowing of the transplant renal artery as a diagnostic cutoff. While invasive, angioplasty and stenting can be performed during the procedure, allowing for treatment and verification of therapeutic success. 83 Results described in this meta-analysis highlight the importance of intervention due to its positive impact on renal function, hemodynamic, and graft survival.
With previous reports by Ngo et al 13 as reference, we sought to expand their efforts in reporting definitions and outcomes with updated evidence, while adding for the first time to the literature a meta-analysis of available data Lack of a clear consensus led to the need for a first step in defining adequate diagnosis and treatment guidelines for patients with TRAS. We proposed a diagnostic and therapeutic algorithm; however, in the absence of high-quality studies that compared cutoff values for diagnosis and long-term outcomes, we opted to base the algorithm on the frequency of reported values while further studies fully elucidate the optimal application of diagnostic and therapeutic applications (Figure 2).
Native RAS and its treatment have been widely studied by high-quality studies, including randomized clinical trials such as ASTRAL, CORAL, and HERCULES.85–87 These studies have yet to fully define the fringe between endovascular treatment and medical therapy in the setting of native RAS. The timing of interventions, as either a last resort or an early intervention, remains unclear.85,86,83,88–90 Such high-quality studies are yet to be replicated in the setting of TRAS; however, current limited available evidence, as synthesized and analyzed in this review, has shown endovascular interventions have potential usefulness for TRAS. These include significant sustained decreases in blood pressure, creatinine level, PSV, and medication consumption after intervention. While limited, PTA is also an effective intervention for reducing creatinine level when compared with medical management. While stenting seems to lead to improved outcomes, these findings must be further explored in future studies by adequately matching comparisons between PTA and PTAS. Current studies that compared both techniques report increased baseline luminal narrowing in patients undergoing stenting, suggesting possible biases in patient selection and susceptibility. Chen et al 64 suggested defaulting to PTA in cases with <70% stenosis, whereas Macchini et al 66 used stenting after suboptimal primary PTA. Biederman 58 , however, has highlighted the benefits of stenting in restenosis rates; this finding is supported by evidence produced by this meta-analysis, showing significantly reduced restenosis when stenting is applied. Further higher-quality studies are needed to fully define optimal treatment. An analysis of available evidence revealed that stenting offers greater benefits in hemodynamic and renal parameter normalization, and decreased restenosis rates. Even in studies where baseline differences were identified, stenting offered a greater significant reduction in luminal narrowing. 64 Thus, the currently available limited evidence suggests better outcomes in PTAS and should be considered as the main intervention. Patient evaluation and tailoring remain key, as factors such as proximity to bifurcations and tolerance anticoagulation and/or antiplatelet therapy should be considered as possible contraindications to stenting. The evidence presented in this study will surely allow the production of higher-quality studies in the future.
Alternatives to traditional contrast agents, such as CO2, have emerged. This provides a feasible alternative in patients with contraindications to iodide or gadolinium agents, as contrast-induced nephrotoxicity remains a threat in this population, is responsible for up to one-third of all cases of intrahospital kidney failure. 91 Its applications as a diagnostic and therapeutic agent have been previously published by Elmously et al, 71 who successfully performed PTAS in patients with TRAS with comparable outcomes to iodine contrast.
Various important limitations are present in our study, derived from the previously described heterogeneity. The lack of a universal definition for diagnosis and screening is one of the hurdles that would benefit from a study on its own. The great variations in follow-up period, methodology, and reported outcomes hinder further possible analysis. This is compounded by the lack of high-quality studies that have previously benefited native RAS such as ASTRAL, CORAL, and STAR, among others, resulting in our arbitrary grouping of time periods. However, even such studies are criticized owing to their methodology. 92 High-quality studies might be difficult to perform owing to the rarity of this pathology; however, standardized reporting even in retrospective studies seems feasible, and future authors are encouraged to build upon limitations of prior literature. Another important limitation is the limited number of studies and related low-group sizes comparing intervention and medical management, and PTA and PTAS, the latter having an apparent patient selection bias, which weakened the strength of our findings in the corresponding segments. Additionally, Funnel plots revealed asymmetry, suggesting bias in publication in this topic. Future authors must report a core set of data, including comprehensive patient demographic data and clear comparisons between the techniques used, reporting at least pre- and post-intervention creatinine levels; eGFR; systolic, diastolic, and MAP; medication consumption; PSV; and angiographic luminal narrowing with interval follow-up, along with detailed complication and restenosis rates. Graft survival analysis, both between interventions and matched to non-TRAS transplanted patients, management of restenosis are also strongly encouraged to facilitate further analysis. Additionally, there is scarce literature on describing untreated TRAS, with further expansions being unlikely. This limits our ability to directly explore endovascular treatment on graft survival; however, conclusions were drawn in this study by comparing survival to healthy controls.
Conclusion
The efficacy of endovascular treatment in the significant reduction of blood pressure, creatinine level, PSV, and medication consumption is supported by the numerous studies analyzed. Treatment of TRAS remains crucial for graft preservation, and current evidence has proven endovascular treatment to be an effective intervention. The currently available evidence suggests PTAS to be a more effective treatment than PTA as evidenced by the normalization of renal function and decreased restenosis risk; however, further larger studies are needed. Individual patient characteristics, such as anatomy and pharmaceutical tolerance, must also be considered when tailoring treatment. Further high-quality studies are needed to compare the differences between treatment strategies and their outcomes. This study is heavily limited by the diversity in methodology and outcomes, and inconsistency in reporting. Nonetheless, it is an important first step in defining the current evidence and role of endovascular management for further studies to refine.
Supplemental Material
sj-docx-1-jet-10.1177_15266028211038593 – Supplemental material for Endovascular Treatment of Transplant Renal Artery Stenosis: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-1-jet-10.1177_15266028211038593 for Endovascular Treatment of Transplant Renal Artery Stenosis: A Systematic Review and Meta-analysis by David Eugenio Hinojosa-Gonzalez, Gustavo Salgado-Garza, Mauricio Torres-Martinez, Sergio Uriel Villegas-De Leon, Luis Carlos Bueno-Gutierrez, Francisco Eugenio Herrera-Carrillo, Mauricio Gonzalez-Urquijo, Victor Segura Ibarra, Mario Alejandro Fabiani and Eduardo Flores-Villalba in Journal of Endovascular Therapy
Supplemental Material
sj-docx-2-jet-10.1177_15266028211038593 – Supplemental material for Endovascular Treatment of Transplant Renal Artery Stenosis: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-2-jet-10.1177_15266028211038593 for Endovascular Treatment of Transplant Renal Artery Stenosis: A Systematic Review and Meta-analysis by David Eugenio Hinojosa-Gonzalez, Gustavo Salgado-Garza, Mauricio Torres-Martinez, Sergio Uriel Villegas-De Leon, Luis Carlos Bueno-Gutierrez, Francisco Eugenio Herrera-Carrillo, Mauricio Gonzalez-Urquijo, Victor Segura Ibarra, Mario Alejandro Fabiani and Eduardo Flores-Villalba in Journal of Endovascular Therapy
Supplemental Material
sj-docx-3-jet-10.1177_15266028211038593 – Supplemental material for Endovascular Treatment of Transplant Renal Artery Stenosis: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-3-jet-10.1177_15266028211038593 for Endovascular Treatment of Transplant Renal Artery Stenosis: A Systematic Review and Meta-analysis by David Eugenio Hinojosa-Gonzalez, Gustavo Salgado-Garza, Mauricio Torres-Martinez, Sergio Uriel Villegas-De Leon, Luis Carlos Bueno-Gutierrez, Francisco Eugenio Herrera-Carrillo, Mauricio Gonzalez-Urquijo, Victor Segura Ibarra, Mario Alejandro Fabiani and Eduardo Flores-Villalba in Journal of Endovascular Therapy
Supplemental Material
sj-docx-4-jet-10.1177_15266028211038593 – Supplemental material for Endovascular Treatment of Transplant Renal Artery Stenosis: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-4-jet-10.1177_15266028211038593 for Endovascular Treatment of Transplant Renal Artery Stenosis: A Systematic Review and Meta-analysis by David Eugenio Hinojosa-Gonzalez, Gustavo Salgado-Garza, Mauricio Torres-Martinez, Sergio Uriel Villegas-De Leon, Luis Carlos Bueno-Gutierrez, Francisco Eugenio Herrera-Carrillo, Mauricio Gonzalez-Urquijo, Victor Segura Ibarra, Mario Alejandro Fabiani and Eduardo Flores-Villalba in Journal of Endovascular Therapy
Supplemental Material
sj-tif-1-jet-10.1177_15266028211038593 – Supplemental material for Endovascular Treatment of Transplant Renal Artery Stenosis: A Systematic Review and Meta-analysis
Supplemental material, sj-tif-1-jet-10.1177_15266028211038593 for Endovascular Treatment of Transplant Renal Artery Stenosis: A Systematic Review and Meta-analysis by David Eugenio Hinojosa-Gonzalez, Gustavo Salgado-Garza, Mauricio Torres-Martinez, Sergio Uriel Villegas-De Leon, Luis Carlos Bueno-Gutierrez, Francisco Eugenio Herrera-Carrillo, Mauricio Gonzalez-Urquijo, Victor Segura Ibarra, Mario Alejandro Fabiani and Eduardo Flores-Villalba in Journal of Endovascular Therapy
Footnotes
Acknowledgements
We thank Lorena Tamez Hernandez and her invaluable assistance in editing.
Authors Note
This work has not been presented in any meeting, congress, or similar event.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study complies with the principles laid down in the Declaration of Helsinki. Appropriate ethical committee clearance was obtained as needed.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.