
Abstract
Purpose:
To investigate early- and long-term outcomes of endovascular aneurysm repair (EVAR) for infrarenal abdominal aortic aneurysm (AAA) in young and low surgical risk patients.
Methods:
The global registry for endovascular aortic treatment (GREAT) was queried for all patients with AAA undergoing standard EVAR; patients were excluded if had previous AAA repair or underwent concomitant procedures. Young patients were defined if age <60; surgical risk was assessed through the validated Medicare perioperative risk score (MPRS) based on age, sex, renal function, heart failure, and peripheral vascular disease. Patients were classified as low (MPRS<3), average (MPRS 3–11), or high (MPRS>11) risk. Young versus older patients and low-risk versus average/high-risk patients were compared. The primary endpoints were early (30 days) major adverse events (MAEs), 5-year freedom from overall mortality, aortic-related mortality, and freedom from device-related reinterventions. Time-to-event endpoints were calculated by Kaplan–Meier curves.
Results:
Of 3217 included patients, 182 (6%) were <60 years old, 956 (30%) had a low surgical risk, 1561 (49%) an average risk, 700 (22%) a high risk. Young patients had a less angulated proximal neck (27.2±18.4° vs 30.9±21.5°; p=0.05); in low-risk compared to average/high-risk patients, a longer neck length (3±1.8 vs 2.8±1.4 cm; p=0.01) and lower neck angulation (29.7±21.8° vs 33.2±22.2°; p=0.01) were present. Young age alone had no significant impact on early mortality (0% vs 0.6%; p=0.62.) and MAEs (3.9% vs 6.1%; p=0.20), while these were significantly lower in low-risk compared to average/high-risk patients (early mortality: 0.1% vs 0.7%, p=0.04; MAEs: 4.1% vs 6.7%, p=0.005). At 5 years, overall survival was significantly higher in young (88% vs 76%; p<0.001) and lower-risk (77% vs 54%; p<0.001) patients; low-risk patients also had significantly decreased aortic-related mortality (0% vs 2%; p=0.04) and reintervention rates (6% vs 11%; p=0.007). There were no statistically significant differences in mortality (0% vs 2%; p=0.42) and reintervention rate (10% vs 10%; p=1.00) between young and older patients.
Conclusion:
In this real-world registry, EVAR was more often offered in cases with suitable anatomy in young and low-risk patients. Low operative risk, rather than young age alone, predicted excellent early outcomes and low 5-year mortality, aortic-related mortality, and reintervention rates.
Keywords
Introduction
Endovascular aneurysm repair (EVAR) is today accepted as a valid alternative to open surgical repair (OSR) for the treatment of infrarenal abdominal aortic aneurysms (AAA).1,2 Compared to OSR, EVAR is a less invasive treatment that is associated with lower early mortality and complication rate, as well as a shorter length of hospitalization and earlier return to daily life activities. 2 However, EVAR is still associated with worsened long-term outcomes in terms of reintervention rate, overall mortality, and aneurysm-related mortality.3,4 This evidence may make EVAR a less desirable option for young and low-risk patients with AAA, in which more durable results are warranted. Conversely, these results may also reflect the outcomes only of older generation endografts, without accounting for the evolution of the devices, techniques, and patient selection that has evolved in the last 15 years. 5
On this regard, two main aspects in the selection of EVAR patients remain controversial. The first one regards the current role of EVAR in young and/or low surgical risk patients. This represents a subset of patients who would benefit also from OSR; therefore, it is important to understand how to improve patients’ selection in order to optimize the endovascular outcomes. The second one is the role of EVAR in older and high-risk patients, for which the clinical question is whether to opt for the endovascular solution or for no treatment, given the high risk of complications and the limited life expectancy. 6
This study analyzed data from a large multicenter prospective registry on aortic interventions, the global registry for endovascular aortic treatment (GREAT), to investigate the current outcomes of EVAR, stratified by age and operative risk score. The aim of the study was to compare early and 5-year results between young and older patients and between low-risk and average/high-risk patients.
Methods
GREAT Registry
The GREAT is a prospective observational multicenter cohort registry on Gore (W.L. Gore & Associates, Flagstaff, AZ, USA) aortic endografts including 113 centers worldwide, counting 5023 patients with thoracic, abdominal, or thoracoabdominal aortic diseases. Enrollment began in 2010 and concluded in 2016. Ethical committee approval was acquired for each center, and informed consent was obtained for every patient. Each patient could be enrolled before or after the procedure, but not after discharge from the hospital, and sites were trained to enroll all consecutive patients receiving a Gore endograft.
Data Collection
Collected data were recorded on a web-based electronic report form (iMedidata, Medidata Worldwide Solutions, Inc., New York, NY, USA). Data management was performed by the Gore Clinical Research Department (W.L. Gore & Associates). All collected data were reviewed, and if missing or inconsistent data were detected, relevant queries were posed to the investigators for resolution. Monitoring visits were performed at each enrollment site to verify necessary study documents, including signed informed consent for each patient. Consistency between electronically imported data and source documents was also examined. Demographic, anatomical, and procedural data and outcomes were obtained from the database. Collected data included early (30 days) medical and surgical complications and 5-year outcomes.
Patients’ Population
All patients with an infrarenal AAA undergoing standard EVAR with a Gore Excluder device were included. Patients receiving concomitant proximal extension (without renal artery coverage), iliac stenting, or non-excluder iliac limbs were also included. Patients with previous AAA repair and patients undergoing concomitant renal stenting or iliac branch device implantation were excluded from the analysis. Patients were included if had undergone other prior aortic repair (ascending, arch, or thoracic).
Exposure Variables
Two main exposure variables were considered, age and operative risk. Patients were classified as young if aged <60 years, old if ≥60 years; this age cutoff was selected based on the existing literature.7 –9 The Medicare perioperative risk score (MPRS) was used 10 to assess the perioperative score. This represents a validated perioperative score specific for AAA repair (open or endovascular) and is accepted as a possible tool to estimate the perioperative mortality in patients with AAA. The advantage of this score is that it can be calculated based on simple clinical characteristics, including patient’s age, sex, renal function, history of chronic heart failure, and peripheral or cerebrovascular disease. Patients were classified into 3 risk categories based on the MPRS: low risk (MPRS <3), average risk (MPRS 3–11), and high risk (MPRS >11).2,10
Endpoints
Primary endpoints were early (30 days) mortality and 5 years overall mortality, aortic-related mortality, and device-related reintervention rate. Aortic-related mortality was defined as any death from aneurysm rupture, reintervention, graft infection, or fistula after repair. Device-related reinterventions were defined as reinterventions for endoleaks, device migration, device fracture, and limb stenosis or thrombosis.
The secondary endpoint was the early complication rate. Myocardial infarction, respiratory insufficiency, acute kidney failure (>50% decrease in estimated glomerular filtration rate or new-onset dialysis), any type I or III endoleak or endograft migration were considered as major adverse events (MAEs). The primary and secondary outcomes were compared between the groups defined in relation to age and operative risk.
Statistical Analysis
Continuous data are presented as mean ± standard deviation, and categorical data as number and percentage. Bivariate comparisons were performed using either chi-square test or Fisher’s exact test for categorical variables, and the t-test, Mann–Whitney test, Kruskal–Wallis test, or ANOVA for continuous variables as appropriate. Univariable and multivariable logistic regression models were performed to identify predictors of early mortality or MAE. Long-term mortality and reintervention rates were estimated as Kaplan–Meier curves. Univariable and multivariable Cox proportional hazard models were used to identify baseline clinical and anatomical factors associated with long-term mortality, aortic-related mortality, and reinterventions. A step-wise backward elimination method was used for predictor elimination in the regression modeling. In case of colinearity, separate reduced models with inclusion of each colinear covariate were built, and the most significant model was selected. The most parsimonious model with inclusion of clinical and statistical confounders was selected as final multivariate model. A p-value <0.05 was considered statistically significant.
Results
Patients’ Cohort
Of 5023 patients included in the registry, 3217 matched the inclusion criteria for this study. About 182 (6%) patients were younger than 60 years, and 3035 (94%) were ≥60 years old. Regarding the operative score, 956 (30%) patients were classified as low risk, 1561 (48%) were at average risk, and 700 (22%) were at high risk. Detailed demographics and risk factors stratified by age group and risk category are provided in Table 1. Median follow-up of the overall cohort was 3.2 years.
Demographics and Risk Factors.
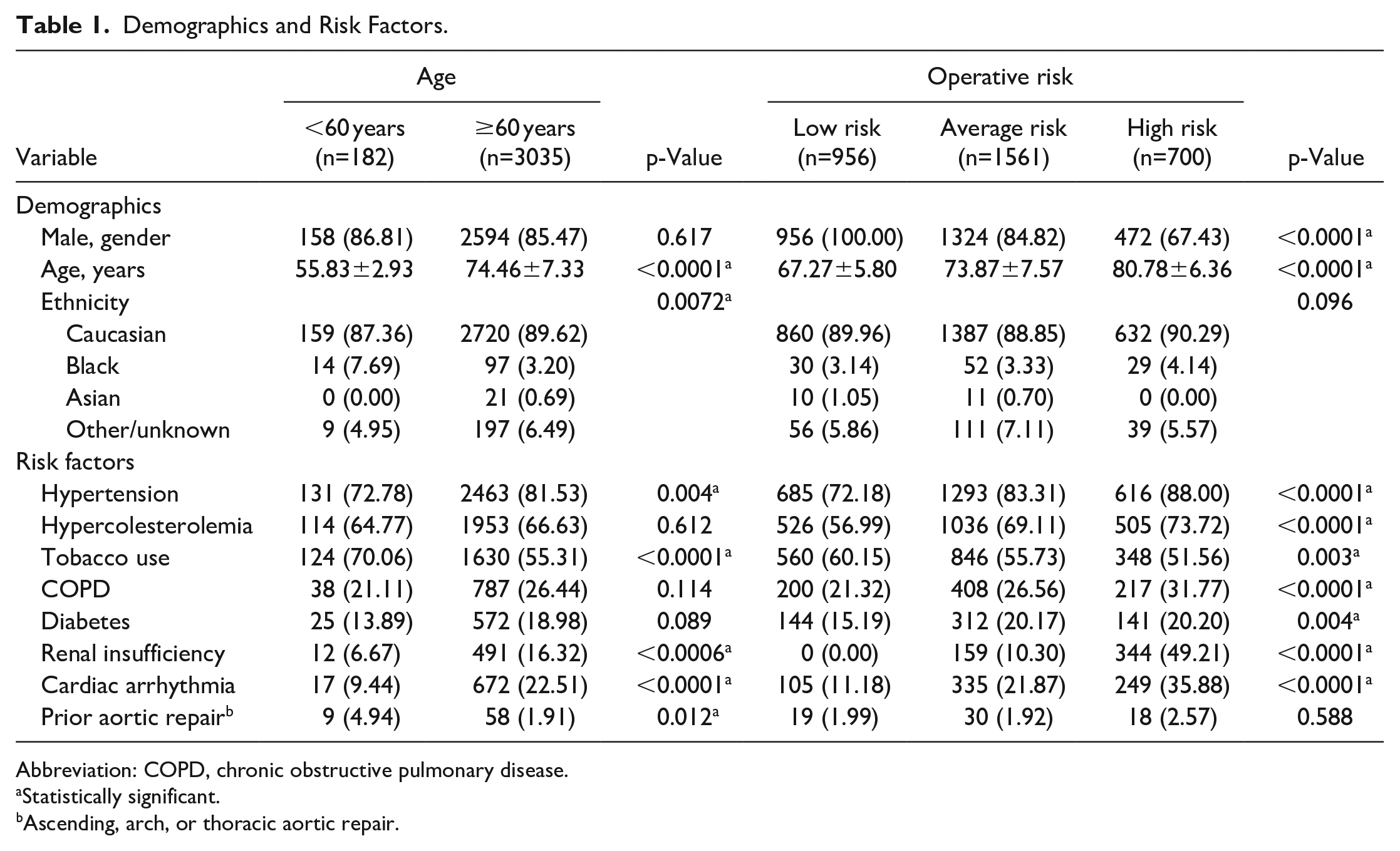
Abbreviation: COPD, chronic obstructive pulmonary disease.
Statistically significant.
Ascending, arch, or thoracic aortic repair.
Impact of Age on Anatomical Complexity
Young patients had a lower mean angle of the infrarenal neck (27.2°±18.4 vs 30.9°±21.5; p=0.05) compared to older patients, and more frequently received EVAR within the instructions for use (IFU) for the proximal neck (94% vs 88%; p=0.019) (Table 2). Anatomical characteristics of the iliac arteries and distal landing zone were similar. The preferred method of access was a femoral surgical cut-down for both groups (53% vs 55%; p=0.483).
Anatomical and Procedural Data.
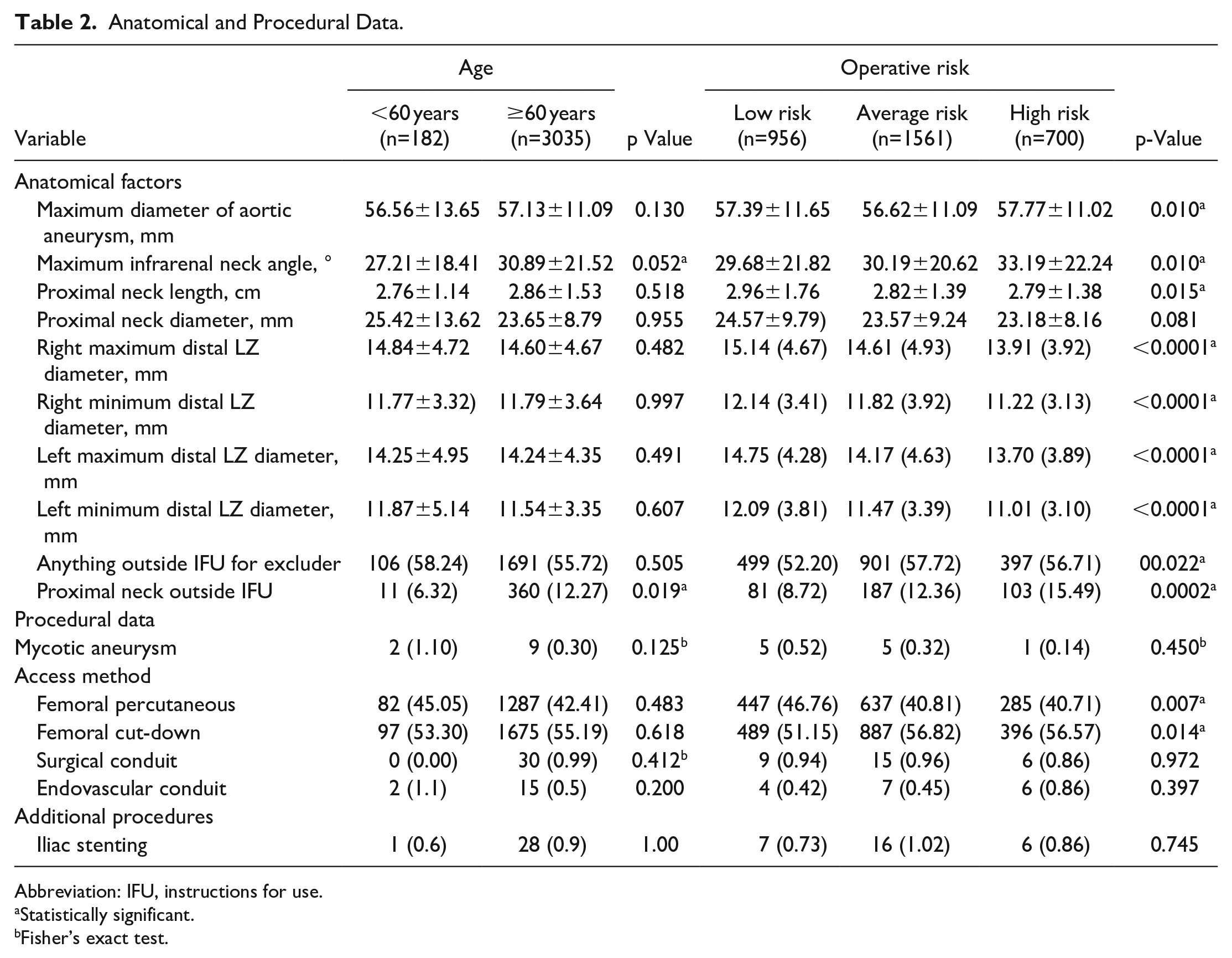
Abbreviation: IFU, instructions for use.
Statistically significant.
Fisher’s exact test.
Impact of Age on Early Outcomes
Early mortality was 0% in patients <60 years and 0.6% in patients >60 years (p=0.620); also length of hospitalization was similar (3.8 vs 4 days; p=0.997). Any MAE occurred in 3.8% vs 5.9% of patients (p=0.243); there were no differences between the two groups in terms of early surgical or systemic complications (Table 3). Age was not significantly associated with any MAE at the multiple logistic regression (Table 4).
Early (30-Days) Outcomes.
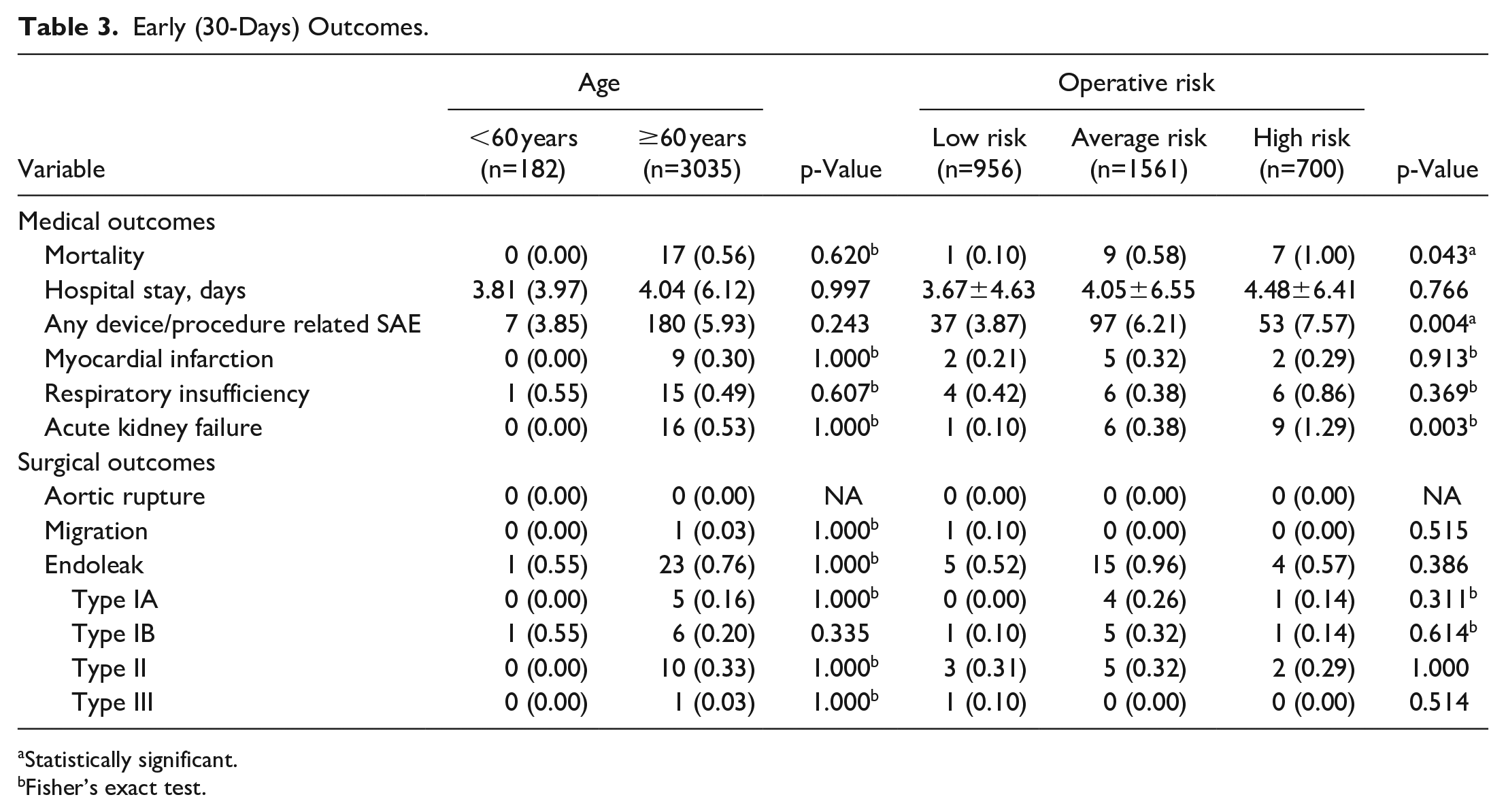
Statistically significant.
Fisher’s exact test.
Univariable and Multivariable Analysis for Early Mortality or Any MAE.
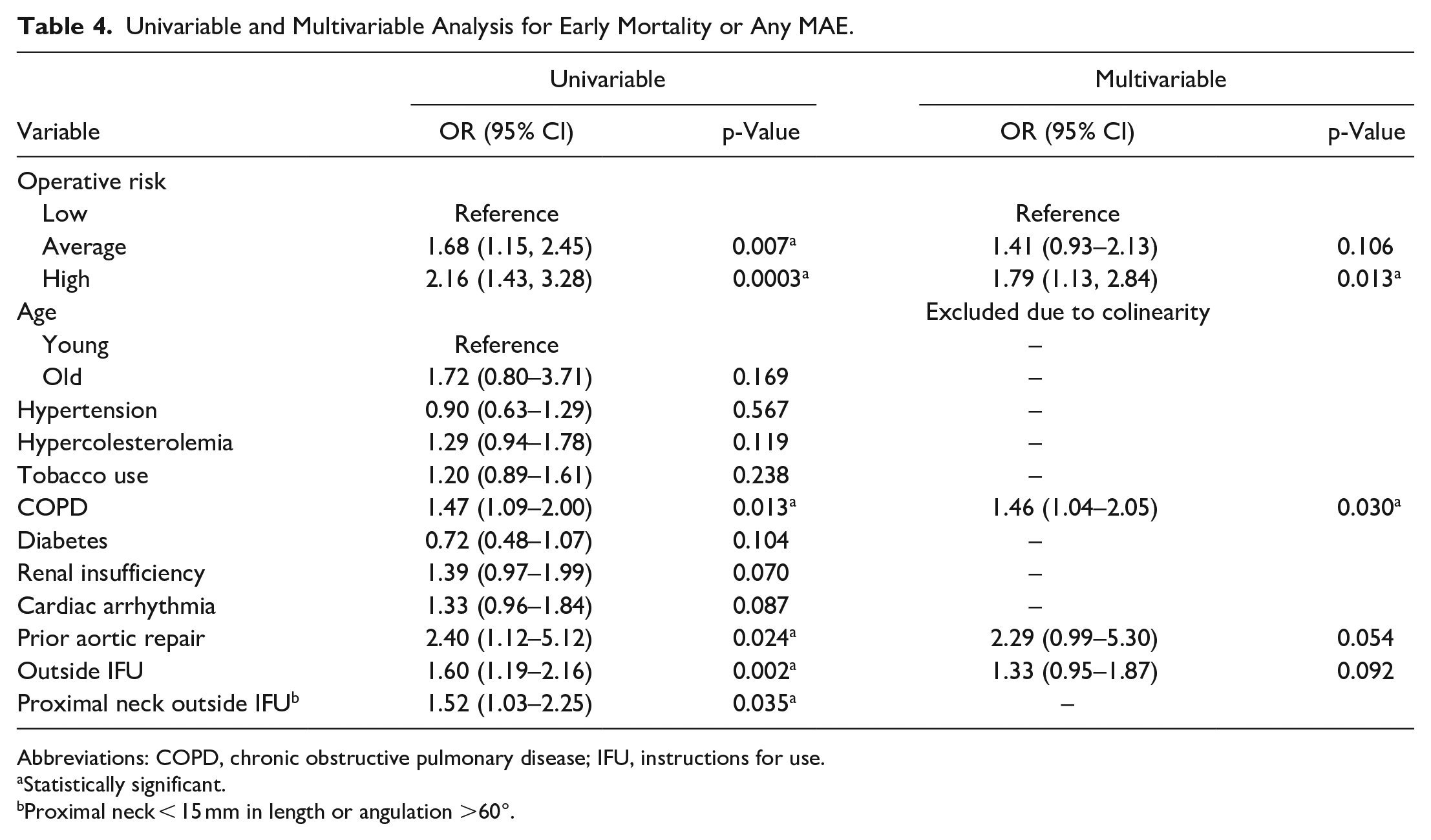
Abbreviations: COPD, chronic obstructive pulmonary disease; IFU, instructions for use.
Statistically significant.
Proximal neck < 15 mm in length or angulation >60°.
Impact of Age on Long-Term Outcomes
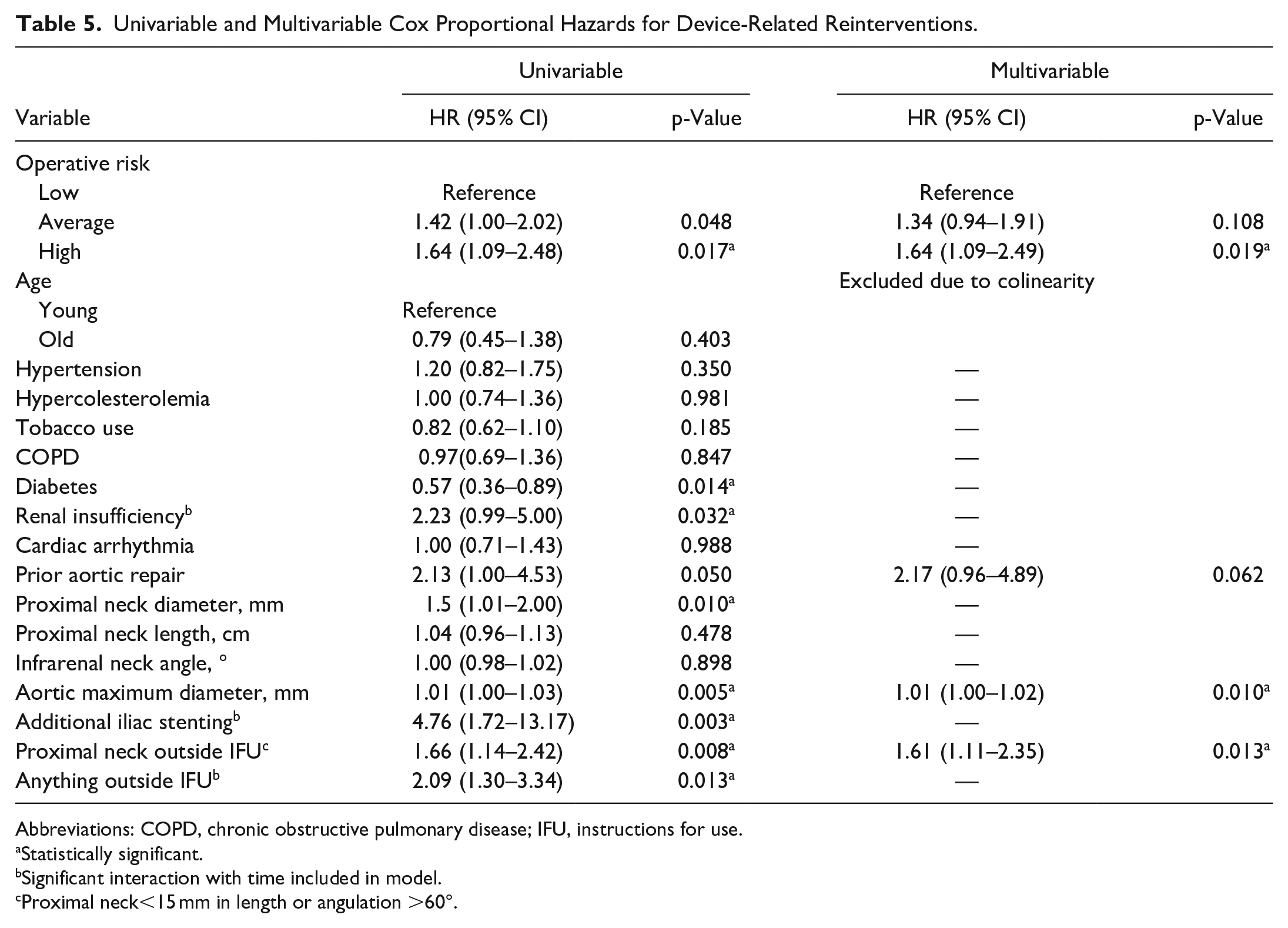
After 5 years of follow-up, overall survival was 88% (95%CI) in young patients versus 66% in older patients (p<0.001) (Figure 1), but there were no significant differences in aortic-related mortality (0% vs 2%; p=0.183) (Figure 2) and reintervention rate (10% vs 10%; p=0.402) (Figure 3). Age alone was not a significant predictor of reintervention (OR 0.79, 95%CI 0.45–1.38; p=0.403) (Table 5) or aortic mortality (Table 6) at the univariate analysis. Age was dropped from the final multivariate model as it was not associated with reintervention or aortic-related mortality and was affected by colinearity with MPRS; MPRS was maintained instead after model fitting.
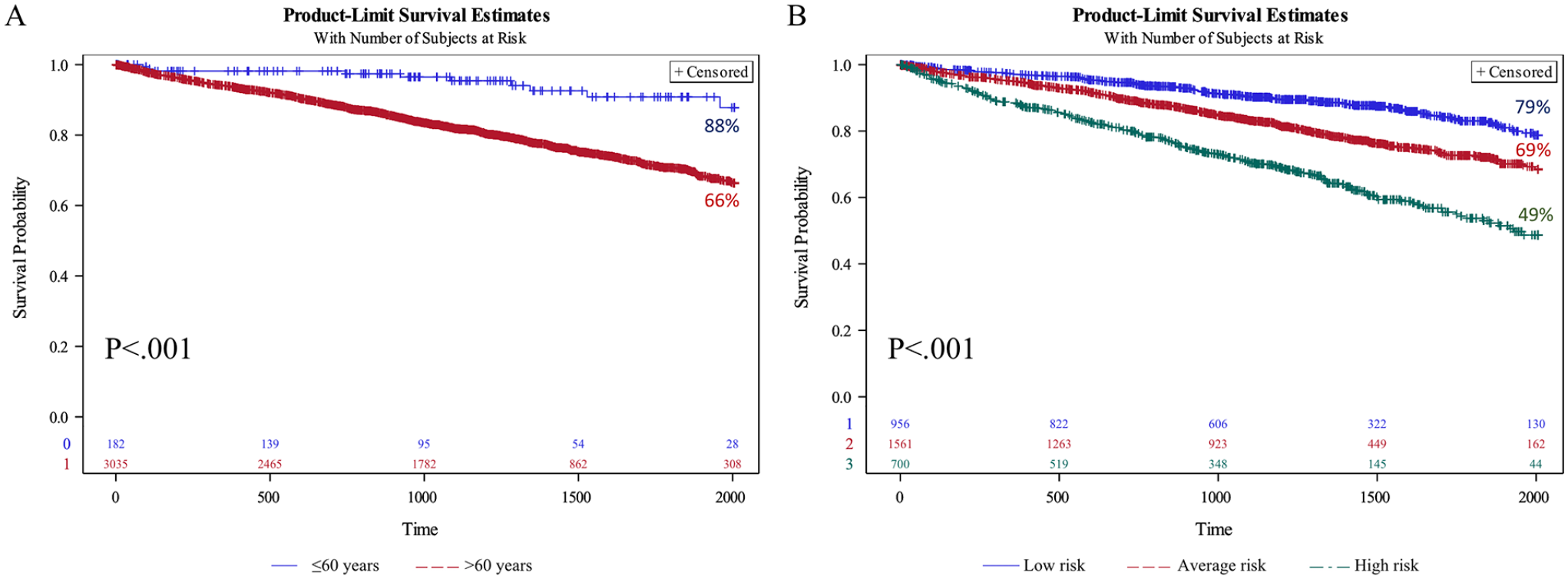
Overall survival after 5 years from endovascular aneurysm repair (EVAR), stratified by age group (A) and comorbidity score (B). SE<10%.
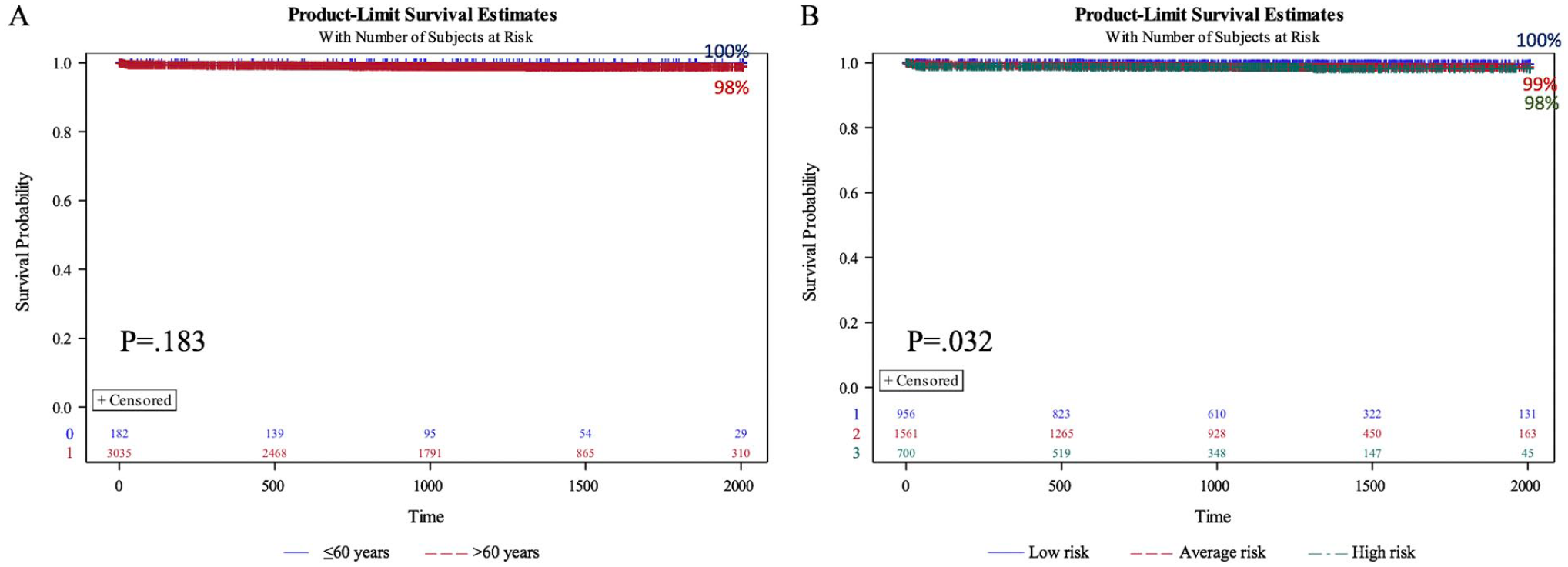
Freedom from aortic-related mortality after 5 years from endovascular aneurysm repair (EVAR), stratified by age group (A) and comorbidity score (B). SE<10%.
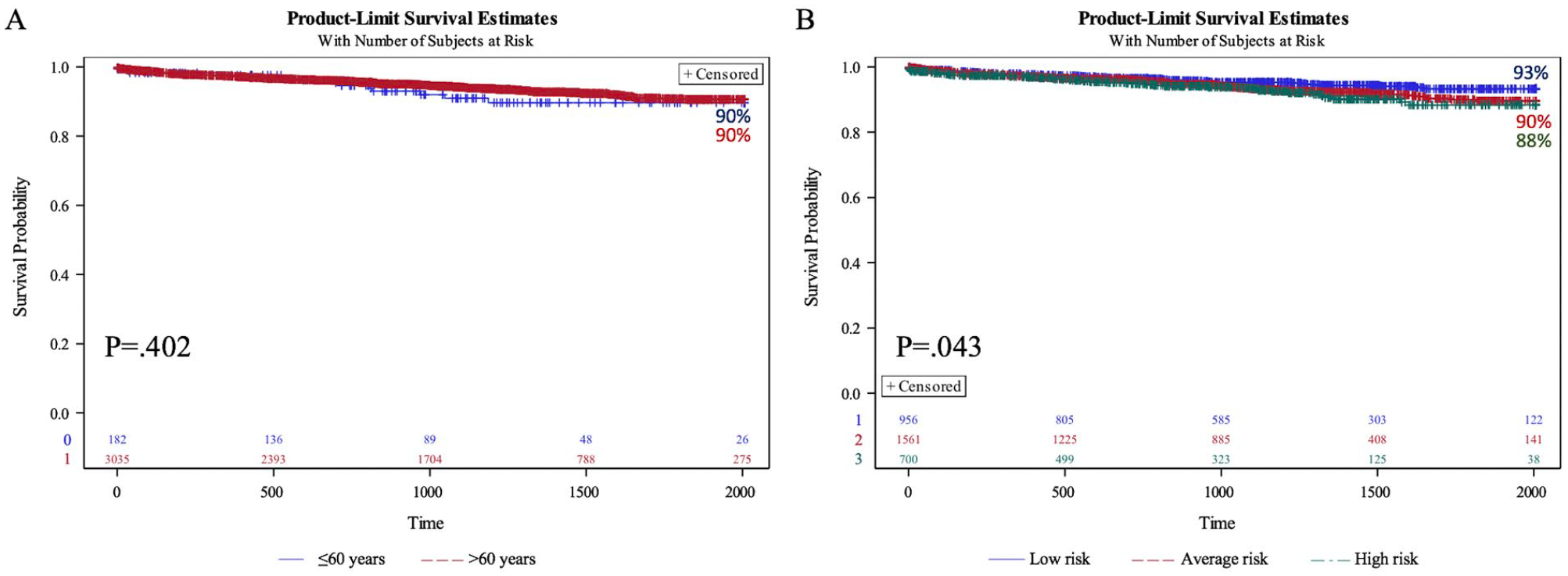
Freedom from reintervention after 5 years from endovascular aneurysm repair (EVAR), stratified by age group (A) and comorbidity score (B). SE<10%.
Univariable and Multivariable Cox Proportional Hazards for Device-Related Reinterventions.
Abbreviations: COPD, chronic obstructive pulmonary disease; IFU, instructions for use.
Statistically significant.
Significant interaction with time included in model.
Proximal neck<15 mm in length or angulation >60°.
Univariable Cox Proportional Hazards for Aortic-Related Mortality.
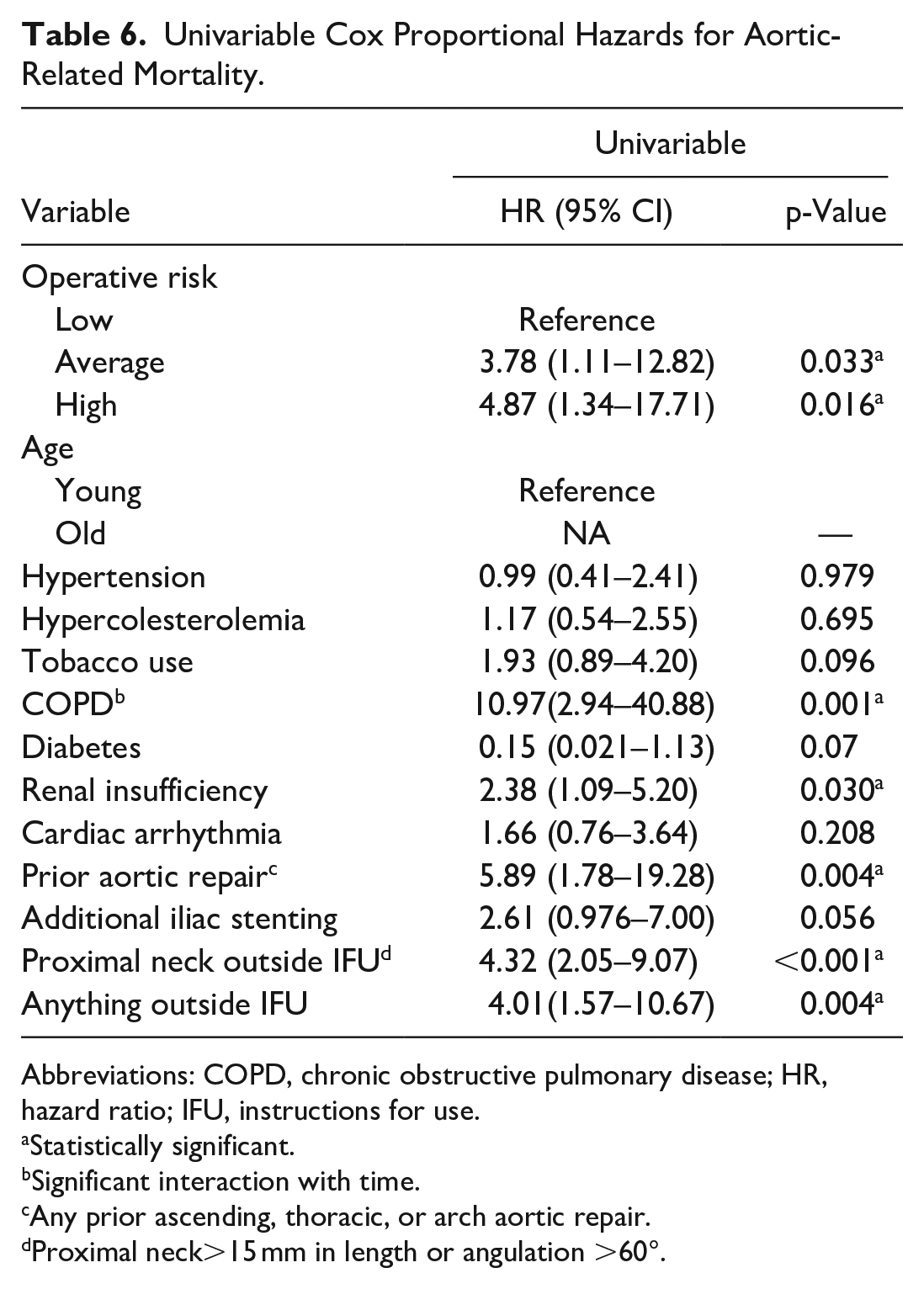
Abbreviations: COPD, chronic obstructive pulmonary disease; HR, hazard ratio; IFU, instructions for use.
Statistically significant.
Significant interaction with time.
Any prior ascending, thoracic, or arch aortic repair.
Proximal neck>15 mm in length or angulation >60°.
Impact of Operative Risk on Anatomical Complexity
Low-risk patients showed inferior anatomical complexity compared to average- and high-risk patients, with less infrarenal neck angulation (29.7±21.8 vs 30.2±20.6 vs 33.2±22.2; p=0.010) and longer neck length (3.0±1.8 vs 2.8±1.4 vs 2.8±1.4; p=0.010); the number of patients receiving EVAR outside the proximal neck IFU was lower for low-risk patients (9% vs 12% vs 57%; p=0.022). The right (15.1 vs 14.6 vs 13.9 mm; p<0.001) and left (14.8 vs 14.2 vs 13.7 mm; p<0.001) maximum iliac diameters were higher in low-risk patients. Overall, EVAR outside IFU was performed in 52% of low-risk patients, 58% in average-risk, and 57% in high-risk patients (p=0.022).
Low-risk patients were more likely to receive a percutaneous access rather than a femoral cut-down (47% vs 415 vs 41%; p=0.007). A surgical (1% vs 1% vs 1%; p=0.972) or endovascular (0.5% vs 0.5% vs 0.9%; p=0.397) conduit was used in a minority of patients in all groups.
Impact of Operative Risk on Early Outcomes
Early mortality was significantly lower in low-risk patients (0.1% vs 0.6% vs 1%; p=0.043). There were no differences regarding cardiac (0.2% vs 0.3% vs 0.3%; p=0.913) and respiratory (0.4% vs 0.4% vs 0.9%; p=0.369) complications, whereas high-risk patients had more renal complications (0.1% vs 0.4% vs 1.3%; p=0.003) after EVAR. MAE rate was higher in case of EVAR performed outside IFUs (OR 1.60, 95%CI 1.19–2.16; p=0.002) by the univariate analysis. The rate of surgical complications was similar between the different risk categories (Table 3); the rate of any MAE was significantly associated with the perioperative risk (3.9% vs 6.2% vs 7.6%; p=0.004). The risk group was confirmed as significantly associated with any MAE after adjustment for chronic obstructive pulmonary disease (COPD) (OR 1.46, 95%CI 1.04–2.05; p=0.030), prior aortic repair (OR 2.29, 95%CI 0.99–5.30; p=0.054), and outside IFU EVAR (OR 1.33, 95%CI 0.95–1.87; p=0.092) by multivariate analysis (Table 4).
Impact of Operative Risk on Long-Term Outcomes
After 5 years, overall survival was 78.8% for low-risk patients, 68.5% for average risk patients, and 48.7% for high-risk patients (p<0.001) (Figure 1). In addition, freedom from aortic-related mortality was significantly different between risk groups (low risk: 99.6%, average risk: 98.7%, and high risk: 98.2%; p=0.032) (Figure 2); freedom from reintervention was 93.2% for low-risk patients, 89.6% for average-risk patients, and 88.3% for high-risk patients (p=0.043) (Figure 3). After adjustment for EVAR outside IFU (HR 1.61, 95%CI 1.11–2.35; p=0.013), the high-risk group had a higher risk of reinterventions (HR 1.64, 95%CI 1.09–2.49; p=0.019) compared to low-risk and average-risk patients (Table 5).
Discussion
Endovascular repair of infrarenal aortic aneurysms (EVAR) has significantly improved during the past 29 years, since Parodi et al 11 first reported their landmark cases. The modern endovascular approach today can benefit from several commercially available devices that are approved for EVAR in different countries, and this allows for an extensive use of this approach in most patients worldwide.
However, for some subcategories of patients, it is still debated whether the endovascular approach is the correct choice in relation to its counterpart open repair. 12 The most often debated subgroup of EVAR candidates is represented by the young and low-risk patients. As previously pointed, several randomized and non-randomized studies tried to demonstrate the role of EVAR in this subcategory7,13 –17; however, many of these studies had been conducted in the period of first-generation devices (between 1995 and 2010), and different types of endografts were used in each study, depending on the centers and surgeons preferences. Finally, to the best of our knowledge, these previous studies compared EVAR with OSR, and there are no contemporary data from large registries evaluating the outcomes of EVAR alone using a single type of device, in relation to age and perioperative risk.
The GREAT Registry was started in 2010 and collected only patients receiving the Gore Excluder endograft; this device provides an infrarenal fixation; therefore, an adequate proximal neck is mandatory. This may represent a positive aspect of this study because the obtained results may reflect a more homogeneous group of standard EVAR cases, and not complex EVAR cases. The overall anatomical data, and in particular data with the proximal neck length (2.8±1.4 cm) and angle (29±20°) in this series seem to support this consideration.
In this registry, the use of EVAR in young patients was limited (only 6% of the entire cohort); this number is in line with a previous study reported by Gupta et al 8 that in 2012 compared the survival between EVAR and OR in young patients, defined as aged <60. Although the occurrence of an AAA larger than 5 cm may be considered, a relatively rare incident in the young population, previous studies demonstrated an increasing trend of EVAR cases with more than 5000 patients/year treated in United States aged between 50 and 64. 15
Age alone did not significantly modify EVAR outcomes in this registry; in fact, no differences were found in early mortality and MAE, as well as for long-term aortic-related mortality and reintervention rate, in young patients compared to older patients. In our study cohort, young age patients had a more strict adherence to IFU regarding proximal neck characteristics. Our results may support the concept that EVAR in young patients is feasible without significant worsened early and 5-year outcomes, if performed within IFUs. Patient’s preference represents a crucial point in the choice between open repair and endovascular repair, and young patients may prefer the lower perioperative complication/mortality rate and short hospitalization of EVAR, rather than the lower long-term reintervention rate of OSR, 9 since they are often employed and a fast return to work and daily life activities is desired.
Differently, what significantly impacted as predictor of EVAR outcomes was the comorbidity score, rather than age alone. The higher the MPRS, the higher was the rate of early MAE (p=0.013), long-term reinterventions (p=0.019), and aortic-related mortality (p=0.016), mostly driven by a lower rate of complications in low-risk patients (MPRS<3). This result may be partially explained by the more often use of EVAR outside the IFU in high-risk patients (57%; p=0.02). Although in contrast with previous studies, 18 this explanation is supported by the observation that endovascular treatment of AAA outside the Excluder (W.L. Gore & Associates, Flagstaff, AZ, USA) IFU was an overall predictor of both early complications (p=0.03) and long-term reinterventions (p=0.013). After multivariate analysis, the presence of outside IFU characteristics was more strictly associated with device-related reinterventions than neck length, angle, or diameter when considered alone, likely because IFUs include together a spectrum of different hostile neck characteristics and not just a specific one. However, also after the adjustment for complex anatomical characteristics, the comorbidity score remained an independent predictor of early MAE, 5-year reintervention, and aortic mortality, suggesting that not only AAA anatomical features have a role on the natural history after EVAR. In fact, IFUs essentially consider only diameters, lengths, and angulation at the level of landing zones, whereas the characteristics of the proximal aorta and distal iliac arteries may predispose to disease progression, and the atherosclerotic process may be more extended and severe in older/high-risk patients also in case of standard AAA anatomy.
The subcategory of patients who are both young and at low-risk may represent a singular situation. These patients are suitable for open repair, but EVAR may still be considered due to the lower invasiveness, the early return to daily life activities, and the lower costs. 19 The most recent guidelines do not have any specific recommendation on this regard. 2 Altaf et al 16 already highlighted that the results of EVAR in young patients with comorbidities are comparable to OSR in young fit patients. A randomized trial in 2011 13 demonstrated that in patients at intermediate or low risk, EVAR is as safe as OSR but with the disadvantage of a higher reintervention rate. A recent metanalysis 20 analyzing the results of EVAR versus OSR in young patients concluded that there are insufficient data to exclude patients from EVAR based solely on the age criterion, and the endovascular treatment should not be discouraged in young patients with AAA. Together, this body of evidence suggests that a careful preoperative patient evaluation is warranted also in young patients in order to identify underdiagnosed comorbidities that may impact on the early- and long-term results.
This study has several limitations. Only Gore Excluder endografts were used in the GREAT registry, and the results may not be fully generalizable to other types of endografts. Inclusion of patients in the registry was at physician’s discretion leading to possible related bias. The follow-up was limited, and also longer-term results may be useful to drive the clinical decisions for patients with a long life expectancy, as the assessment of graft durability and second-line treatment events may not be sufficient with a 5-year follow-up. This study is strengthened by the multicenter design, the prospective data collection, and the high number of included patients. The use of a validated comorbidity score allows reproducibility of the study, and the study period provides updated results for currently used endografts.
Conclusion
In this real-world registry, EVAR in young and low-risk patients was more often offered in cases with suitable anatomy and in particular with adequate proximal sealing zone. Age alone did not influence EVAR outcomes, but the presence of low comorbidities had a significant positive impact on EVAR, both for early and 5-year results.
In good-health patients who may be candidate for EVAR, if anatomical suitability is guaranteed, it is more important to carefully identify those patients at low risk, rather than considering young age alone. In this subset of patients, EVAR may be safely offered providing effective and durable results.
Supplemental Material
sj-docx-1-jet-10.1177_15266028211045703 – Supplemental material for Early and Long-Term Outcomes of Endovascular Aortic Repair in Young and Low Surgical Risk Patients in the Global Registry for Endovascular Aortic Treatment
Supplemental material, sj-docx-1-jet-10.1177_15266028211045703 for Early and Long-Term Outcomes of Endovascular Aortic Repair in Young and Low Surgical Risk Patients in the Global Registry for Endovascular Aortic Treatment by Michele Piazza, Francesco Squizzato, Velipekka Suominen, Franco Grego, Santi Trimarchi and Michele Antonello in Journal of Endovascular Therapy
Footnotes
Acknowledgements
The authors would like to acknowledge Dr. Hillary Alberta, MSPH, PhD, Clinical Affairs/Abdominal/Clinical Science Liaison (W.L. Gore & Associates) and the Gore Clinical Research Department (W.L. Gore & Associates) for their assistance in this study.
Authors’ Note
The Global Registry for Endovascular Aortic Treatment Registry is maintained and financially sponsored by W.L. Gore (Flagstaff, AZ, USA). W.L. Gore provided the raw data but did not influence the choice of end points, interpretation of adverse events, statistical method used, or conclusions drawn, nor did they request the addition or deletion of any notable content in our report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.