
Abstract
Purpose:
The purpose of this article is to study 1-year results of Zenith branch iliac endovascular graft (ZBIS) with the off-label use of a 13 mm spiral Z limb to connect to the aortic main body.
Materials and Methods:
A retrospective review from 2015 to 2019 of all iliac branch devices (IBDs) was performed at 1 institution that were connected to an aortic main body with a 13 mm spiral Z limb and had at least 1-year follow-up with computed tomography (CT). Primary endpoints are freedom from ZBIS separation from the connection limb, endoleak (EL), or reintervention at 1 year. Secondary endpoints are primary and secondary ZBIS patency, presence of any EL, and aortic reinterventions.
Results:
Of 149 IBDs implanted in this period, 45 ZBIS in 35 patients were connected with a 13 mm limb and had a 1-year CT; 97% of patients had common iliac artery (CIA) aneurysms, 7% of patients had hypogastric artery (HA) aneurysms, and 30% of patients had bilateral ZBIS implantation. Technical success was 98%. In 84% of cases, the Advanta V12 was used as the HA mating stent; 56% of patients had an EL, mostly type II, which resolved spontaneously in 70% at 1 year, and 9% of ZBIS required reinterventions at 1 year (2 for thrombosis, 2 for type Ic EL from HA mating stent). One-year ZBIS primary patency and secondary patency were 96% and 100%, respectively. No EL was noted to be related to the 13 mm connection limb. No migration or separation of the devices occurred.
Conclusions:
The use of 13 mm spiral Z limb to connect a ZBIS with the main body in our series yields a high technical success rate and good 12-month outcomes without device separation or migration.
Keywords
Introduction
The common iliac artery (CIA) is involved in 20% to 30% 1 of patients presenting with abdominal aortic aneurysm (AAA); thus, in case of indication for surgery, a concomitant repair is frequently required. With the use of endovascular therapy, iliac aneurysms can be treated by different approaches. One option is the placement of a large diameter flared iliac limb (bell bottom technique). However, the bell bottom technique can lead to enlargement and need for subsequent intervention in 10% to 20% of the cases.2,3 Embolization and coverage of a unilateral hypogastric artery (HA) is another method to obtain adequate seal; nonetheless, it may lead to buttock claudication or erectile dysfunction in up to 50% of the patients 4 and may increase the risk of spinal cord ischemia when a fenestrated or branched endovascular aortic repair (f-b EVAR) is performed covering longer aortic segments. 5
Over 15 years ago, iliac branch devices (IBDs) were introduced, consistently showing excellent outcomes with long-term patency well over 90% and low reintervention rates,6,7 making IBDs an ideal choice for HA preservation. The Zenith branch iliac endovascular graft (ZBIS; Cook, Bloomington, Indiana) received European Conformity (CE) mark approval in 2006 with several studies demonstrating its feasibility and good outcomes.7,8 The original instructions for use (IFU) recommend the use of a 16 mm limb to connect the ZBIS to the main EVAR body component to prevent migration and device separation. In 2011 Cook introduced Zenith Spiral-Z AAA Iliac Leg Grafts (ZSLE) and in 2017 the Zenith Alpha Spiral-Z Endovascular Legs (ZISL), adding spiral nitinol stents that determine better conformability than the older limbs9,10 also making them a choice to connect with the ZBIS, offering a different range of distal diameters including 13 mm. From that time on, we have preferentially used 13 mm ZSLE or ZISL limbs to connect the ZBIS to the main bifurcated device to reduce the volume of fabric within the overlap of components. We aim to review the IBDs performed in our institution with the Cook ZBIS device, using a 13 mm spiral limb as the off-label bridging component to the aortic main body.
Methods
Data from consecutive patients undergoing aortoiliac aneurysm repair with endovascular IBDs from 2015 to 2019 at our institution were reviewed. All patients in whom a ZBIS device was connected to an aortic main body (EVAR/f-b EVAR) with a 13 mm spiral leg limb and had at least 1-year follow-up with a computed tomography angiogram (CTA) were selected. Indications for intervention included the presence of any CIA aneurysm >22 mm or HA aneurysm >30 mm, including those associated with a thoracoabdominal, juxtarenal, or infrarenal AAA. The decision to implant an IBD or to embolize the HA and extend to the external iliac artery (EIA) was based on the treating surgeon`s preference.
Patients treated with a ZBIS not connected to an aortic main body were not included in the present study. According to the local ethical committee, ethical approval was not deemed necessary for this retrospective study using anonymized data.
The ZBIS is composed of a common iliac segment, where the hypogastric branch takes off, and an external iliac segment. There are different configurations, with the common iliac segment being 45 or 61 mm long (including the length of the hypogastric branch). The 45 mm version allows 1½ stent overlap (26 mm) with the limb that connects to the main body, and the 61 mm version allows 2½ stent overlap (42 mm). The furthest distal point where the connection limb can land is marked by a proximal gold marker in the zone where the hypogastric branch starts. There is also a distal gold marker which signals the furthest proximal point the HA mating stent can land (Figure 1).
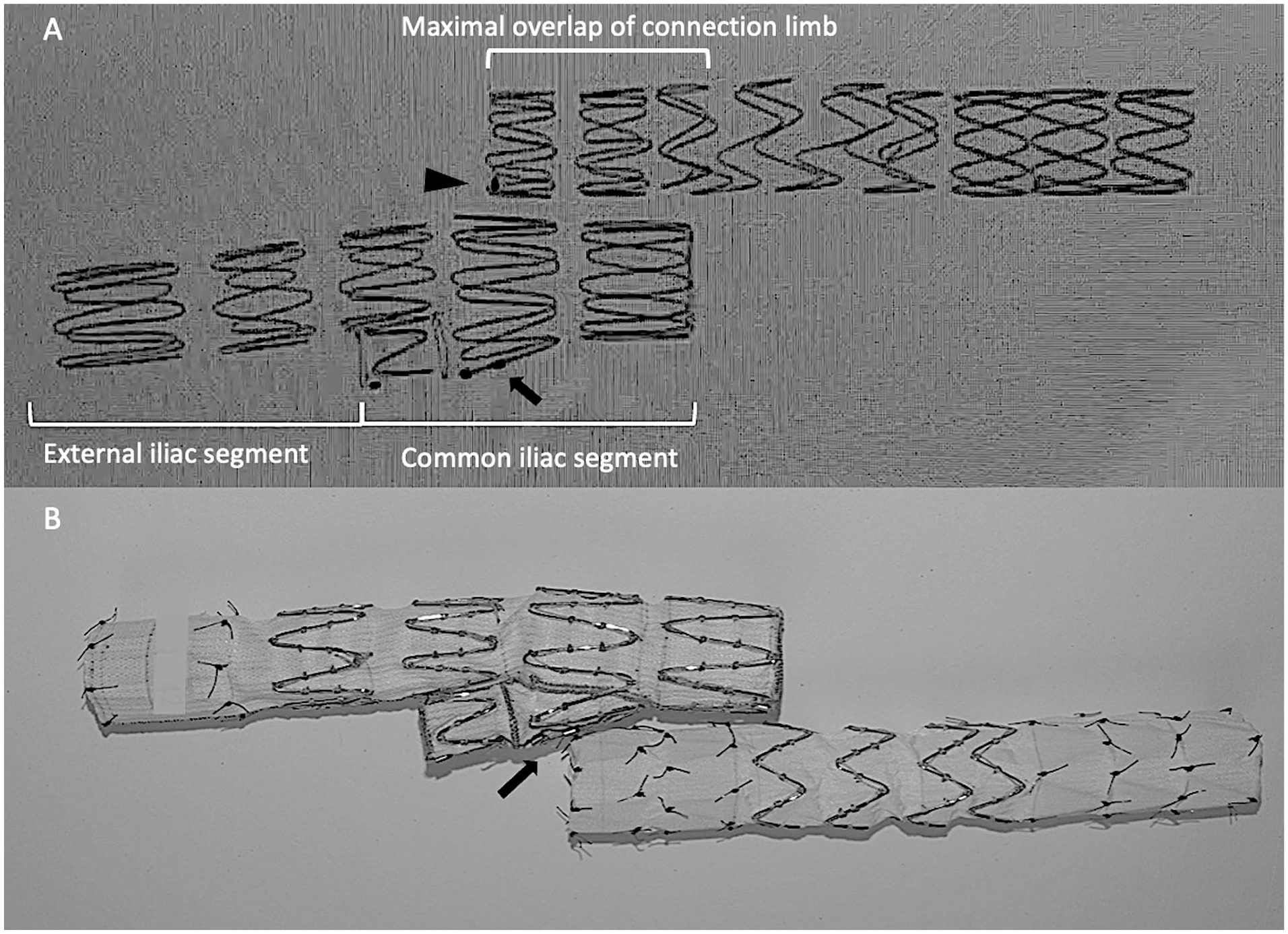
Short common iliac length Zenith branch iliac endovascular graft (ZBIS; 45 mm) fluoroscopic capture (A) and photography (B). (A) Common and external iliac lengths marked. Gold marker in distal stent of connecting limb (black arrowhead). Proximal gold marker in the hypogastric cuff shows the most distal overlap for the connection limb (black arrow).
Electronic records, preoperative and postoperative computed tomography (CT) scans and angiograms of the procedure and any reinterventions, were reviewed.
All cases were planned with the use of a dedicated planning software (Aquarius Intuition, TeraRecon Inc, San Mateo, California). All procedures were performed in a hybrid operating room with a fixed imaging system (Phillips Allura, Philips Healthcare, Best, Netherlands). Technical success was defined as successful implantation of the IBD in the iliac vessel with exclusion of the underlying aneurysm and preservation of antegrade flow to the HA and EIA. Patient characteristics, type of aneurysm and endograft used, overall aortic reinterventions, as well as postoperative endoleak (EL) presence on early CTA and 1-year postoperatively were analyzed on a per-patient protocol.
A per-implanted ZBIS analysis was also performed, including both sides in cases with bilateral ZBIS and 13 mm bridging limbs. Lengths of ZBIS, HA mating stents, and main HA trunk landing zones were analyzed.
The CTAs were analyzed on Aquarius Intuition using multiplanar reconstruction (MPR) to create an orthogonal view of the vessel adjusting crosshairs in 3 planes (Figure 2). Length measurements were undertaken by 1 author (J.T.) in the postoperative and 1-year CTA to assess for separation or migration between the ZBIS and the connection limb, defined as the length difference between the proximal ZBIS gold marker (where the hypogastric branch starts) and the distal edge of the 13 mm connection limb (Figure 2).
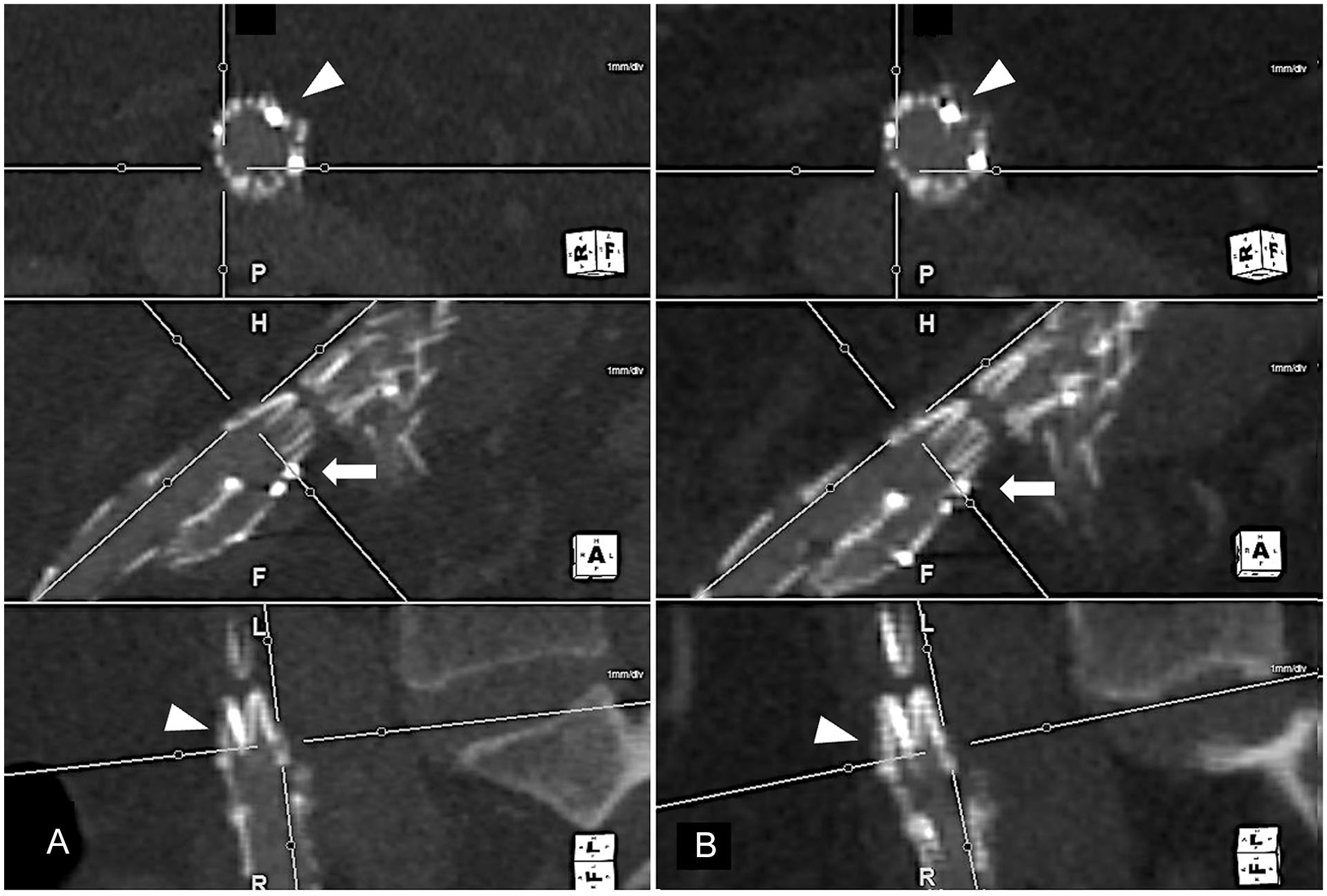
Postoperative landing zone. Distal tip of the connection limb stent (white arrowhead) landing at proximal golden marker in hypogastric cuff (white arrow). Adjusted crosshairs in 3 planes show no 13 mm connection limb migration between early (A) and 1-year (B) postoperative computed tomography angiogram (CTA), using golden marker as reference point.
Primary endpoint of the study was freedom from ZBIS proximal connection separation or migration, EL, or reintervention at 1 year. Secondary endpoints were 1-year ZBIS primary patency and secondary patency, the presence of any EL, and non-ZBIS-aortic-related reintervention at 1 year. Data are presented as total number (n) and percentage (%) for qualitative variables and median with interquartile range (IQR) expressed as (Q1, Q3) for quantitative variables. Comparison between groups was performed with unpaired t test with a threshold for statistical significance of p<0.05.
Results
From 2015 to 2019, 149 IBDs were implanted in 119 patients. After excluding IBDs other than ZBIS and connection limbs other than 13 mm limbs, there were 66 ZBIS in 55 patients. Sixty-five percent (36/55) of the patients completed follow-up and represent the cohort of 45 ZBIS under study. Figure 3 shows a flowchart with the selection process.
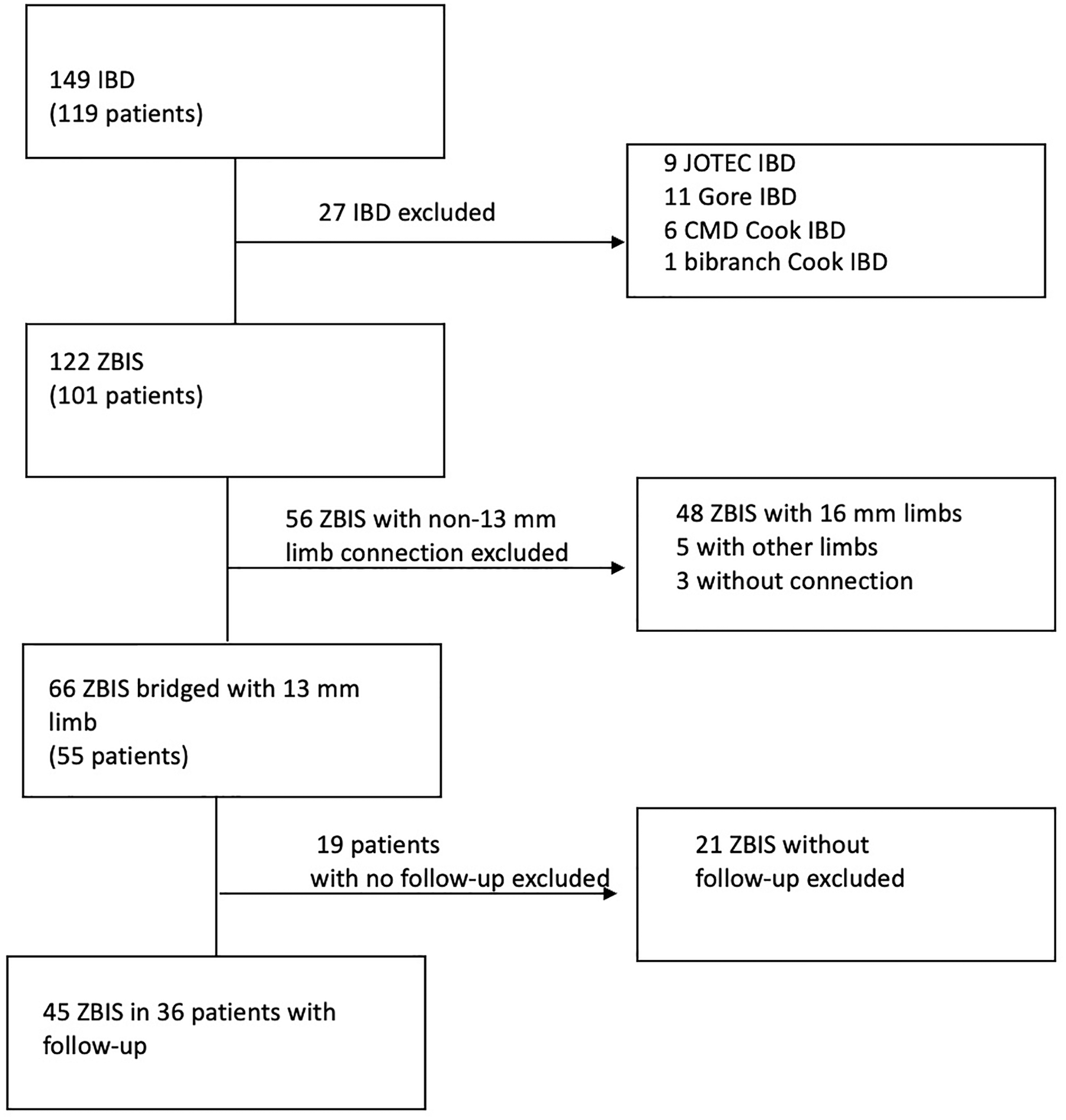
Flowchart with the cohort selection process. IBD, iliac branch device; ZBIS, Zenith branch iliac endovascular graft; CMD, custom made device.
Overall, 61% of these patients had an infrarenal AAA, 97% (35/36) had CIA aneurysms, and 17% (6/36) had HA aneurysms. Thirty-six percent of the patients had bilateral CIA aneurysms. Table 1 shows baseline morbidity and characteristics of aneurysms.
Baseline Characteristics.
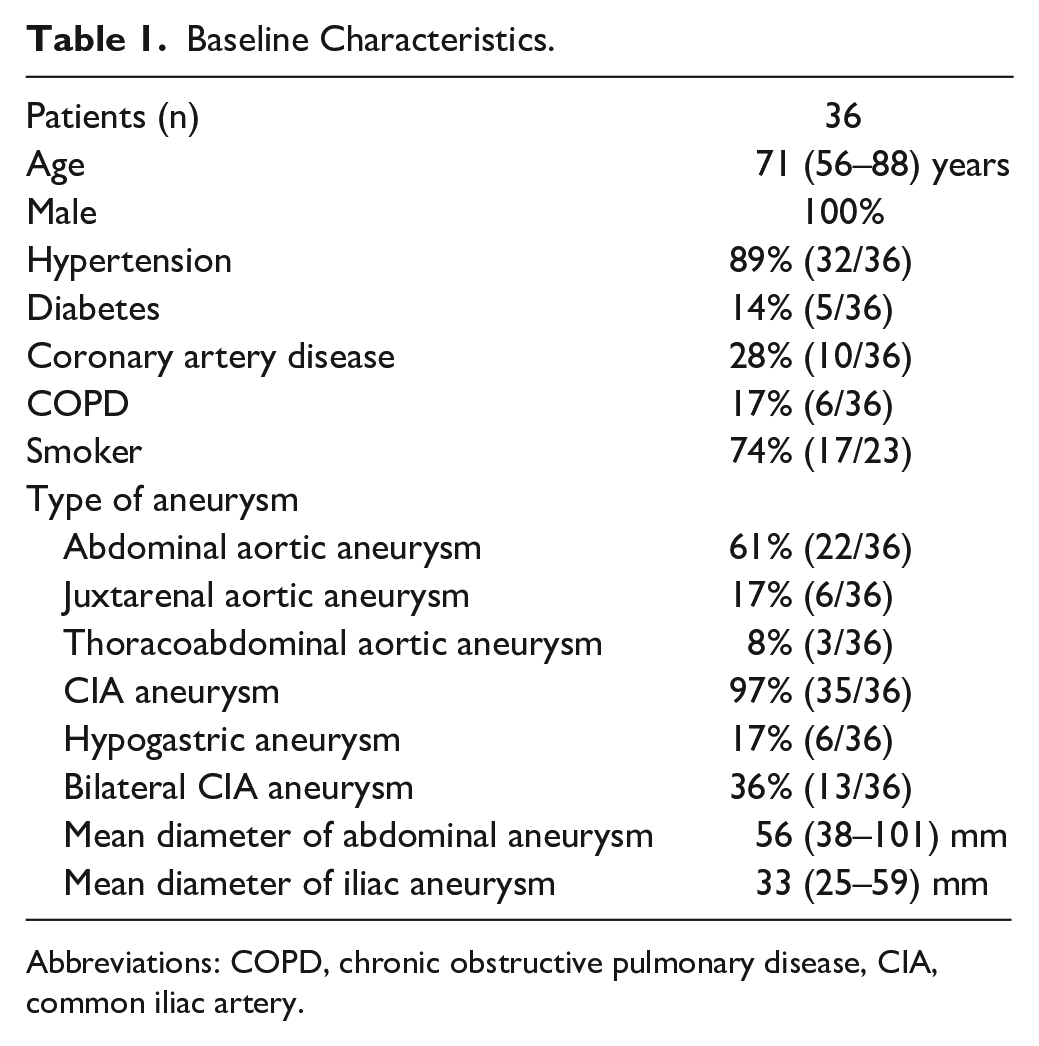
Abbreviations: COPD, chronic obstructive pulmonary disease, CIA, common iliac artery.
Of the 36 patients, 25 (70%) had unilateral and 11 (30%) had bilateral ZBIS implantation (9 patients had bilateral ZBIS connected with 13 mm limbs, 1 patient received a ZBIS in 1 iliac artery and a bibranch in the contralateral, and another patient had a contralateral ZBIS connected with a balloon expandable stent [BES] graft; neither of these IBDs were included in this analysis). Two patients had a ZBIS and contralateral HA embolization with limb extension to the EIA.
Short proximal ZBIS configurations were used 62% (28/45) of the time, with the longer configurations used 38% (17/45) of the time. Median (IQR) overlap differed significantly between the short and long configurations with 21 (19, 24) mm and 33 (30, 37) mm, respectively (p<0.001).
Of the 45 ZBIS, 53% were implanted on the right side. Technical success was achieved in 98% of the ZBIS (44/45), with the exception of 1 early type Ic EL from an HA mating stent. HA mating stent characteristics are summarized in Table 2. In 31% (14/45) of the cases, a bare BES was used to support the cuff transition or rectify tortuosity within the HA mating stent.
Characteristics of Implanted Devices.
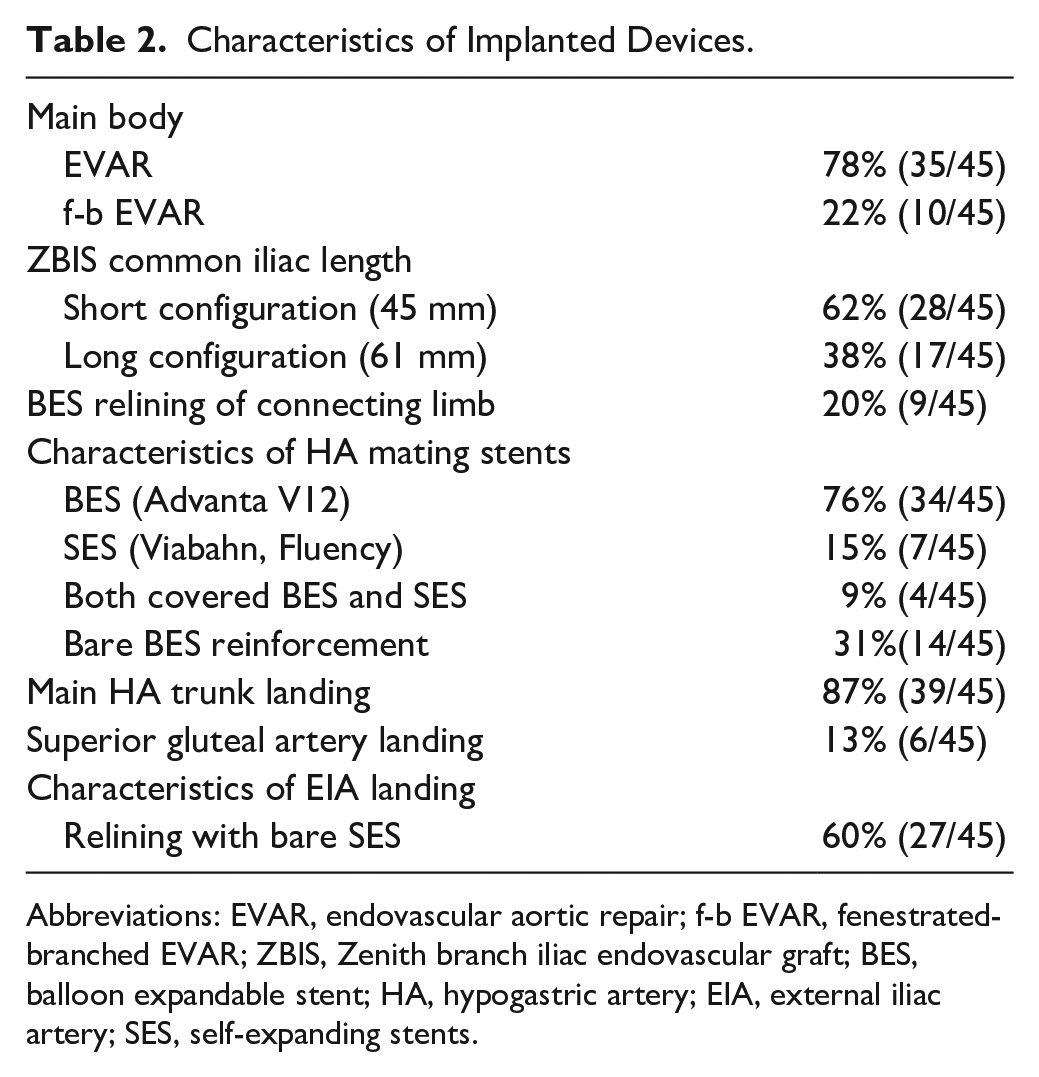
Abbreviations: EVAR, endovascular aortic repair; f-b EVAR, fenestrated-branched EVAR; ZBIS, Zenith branch iliac endovascular graft; BES, balloon expandable stent; HA, hypogastric artery; EIA, external iliac artery; SES, self-expanding stents.
In 13% (6/45) of cases, the distal landing zone was the superior gluteal artery to exclude an HA aneurysm, with 4 cases requiring concomitant embolization of gluteal branches to seal. Relining of the EIA with bare self-expanding stents (SES) was utilized in 60% of the IBDs, 92% (25/27) of times with a Wallstent (12–16 mm; Boston Scientific Corporation, Marlborough, Massachusetts) and 8% with a Protégé self-expandable stent (Medtronic/Covidien, Minneapolis, Minnesota). In 20% (9/45) of cases, a BES was used, in 3 cases as kissing BES to reinforce the iliac limb in narrow aortic bifurcations and the rest to rectify tortuosity of the CIA, with only one of these stents in contact with the ZBIS overlap.
Twenty (56%) patients had an early postoperative EL. Eighty-five percent (17/20) were type II EL and resolved spontaneously in 71% at 1 year, with persistence in 5 patients. There was 1 type Ia EL, 1 type-Ic-ZBIS-related EL, and 1 type III EL. The type III EL was from a defect in the main body at the level of the limb bifurcation. It was relined with a custom-made bifurcated component. The type Ic EL was treated with an extension of the HA mating stent. The type Ia EL has been followed for 3 years with a decreasing iliac aneurysm diameter (original indication for repair). There was 1 new type Ic-ZBIS-related EL 6 months after the procedure, coming from the HA that was successfully intervened and there was also a new type IIIc from a renal branch 1 year postoperatively, successfully relined.
At 1 year, 9% (4/45) of ZBIS required reintervention, with 2 cases of percutaneous thrombectomy plus stent relining of the ZBIS (1 immediate postoperative thrombosis with a kink on the common iliac zone of the ZBIS, 1 with reline of the HA mating stent) and the 2 aforementioned cases of HA stent extension due to type Ic EL. The composite rate of freedom from EL, migration, and ZBIS-related reintervention was 91% at 1 year. Eleven percent (4/36) of the patients required aortic reinterventions not related to the ZBIS at 1 year (relining for the aforementioned IIIc EL from a renal branch and type III EL from the graft, a thrombectomy and relining of a renal branch in a branched EVAR [bEVAR], 1 open repair of a contralateral iliac aneurysm). No EL was related to the 13 mm connection limb.
The median (IQR) length between the proximal ZBIS gold marker and the distal edge of the 13 mm connection limb was 5.5 (3.9) mm, with no differences among early and 1-year CTA. No migration or separation of the devices occurred. One-year ZBIS primary patency and secondary patency were 96% (43/45) and 100%, respectively. No differences in outcomes were observed between long or short common iliac length ZBIS configurations. Outcomes are presented in Table 3.
Early and 1-Year Outcomes.
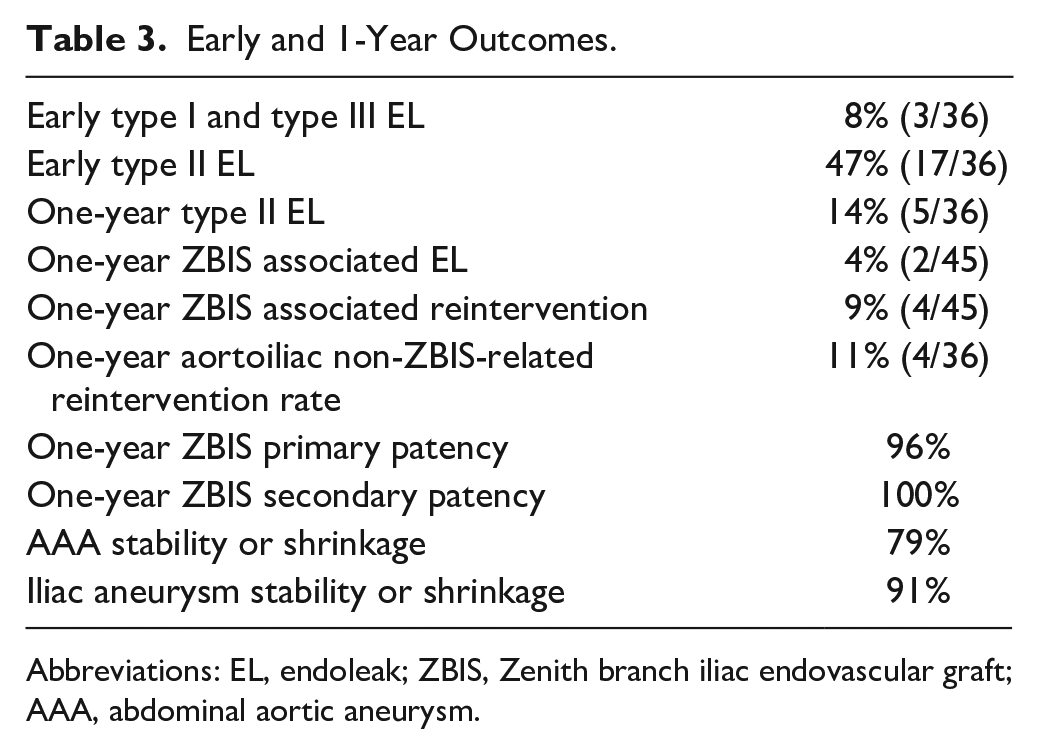
Abbreviations: EL, endoleak; ZBIS, Zenith branch iliac endovascular graft; AAA, abdominal aortic aneurysm.
Overall, 79% of patients experienced shrinkage or stability of the aortic aneurysmal sac as well as 91% of the iliac aneurysms, with a median (IQR) diameter decrease of 6 (0.9) mm for the aorta and 3 (2.8) mm for the iliac aneurysms.
Discussion
We present the 1-year outcomes with the use of a 13 mm iliac limbs to connect the main aortic body and the ZBIS device. When a 13 mm limb is used to connect the main body with the 12 mm diameter common iliac segment of the ZBIS, there is an oversize of around 10% instead of 30% when a standard 16 mm limb is used. This reduced oversize might bring a risk of device separation between components; however, even though some series have shown 1% to 3% risk of device separation of the standard bridging component,11,12 we did not experience any migration or device separation, even in patients with overlap length as short as 14 to 16 mm.
At the time of ZBIS introduction, there was only 1 length configuration available, with 26 mm as the maximal overlap 13 (Figure 1). Sixteen millimeter diameter limbs were recommended in the IFU for connections to prevent migration and device separation with this short overlap and to distally land in the short flared part at the level of the proximal gold marker. This IFU recommendation has not changed since the introduction of the ZBIS IBD. However, using 16 mm limbs to bridge the 12 mm wide proximal ZBIS corresponds to over 30% oversizing, which in our opinion is too much and may contribute to obstruction caused by excessive graft material in the overlap. Limb thrombosis risk is higher when limb oversize is more than 15% in EVAR. 14 Fairman et al 15 found among other factors that oversizing of iliac limbs over 3.5 mm led to a 12-fold increase of limb thrombosis in patients treated with standard EVAR. Extrapolating these results to a stiffer and less compliant segment of overlapping devices cautions us of a high risk of graft infolding within the limb if generous oversizing is applied, with the subsequent risk of thrombosis. This issue could become especially apparent in cases of high tortuosity of the CIA, perhaps contributing in some degree to the IBD thrombosis.
The IBDs present a relatively low risk of thrombosis around 1% to 9%,11,16 mostly attributed to CIA/EIA tortuosity, calcification, presence of thrombus, or HA aneurysm. 17 However, no detailed analysis of limb thrombosis has been reported, and so we think the diameter of the connection limb and the resulting degree of oversizing should be considered as a potential source of complications.
We experienced 2 IBD occlusions in the current study, due to a non-recognized kinking of the distal CIA segment and an HA stent stenosis, successfully reintervened.
The excellent primary and secondary patency rates at 1 year in this study are favorably comparable with other reports,6,11,12,16 as is the IBD-related reintervention rate of 9% with no reintervention related to the 13 mm spiral limb connection stent. Over 90% of patients with 13 mm connecting limb showed shrinkage or stability of the aneurysms supporting previous reports and the efficacy of this device with the use of a 13 mm limb to connect to the main body.
Limitations
This is a retrospective cohort study of selected patients at a highly specialized center and therefore limited in its generalizability. Length measurements were taken only by 1 author; however, it was based on orthogonal views and objective references to avoid major biases, as shown in Figure 2. The observations of this study have a limited value due to the short-term follow-up and should be confirmed with a longer follow-up and possibly a higher number of patients.
Conclusions
The use of 13 mm spiral Z limb to connect a ZBIS with the main body in our series yields a high technical success rate and good 12-month outcomes without device separation or migration.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. T.K.: Consultant, proctoring, IP, royalties, research, and travel grants with Cook Medical. N.T.: Educational grant and Proctoring Cook Medical.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.