
Abstract
Purpose:
Percutaneous transluminal angioplasty (PTA) with conventional plain old balloon (POBA) and/or drug-coated balloon (DCB) is the primary intervention to treat peripheral artery stenoses. However, acute dissections during the procedure and potential for future target lesion revascularization remain procedural complications. The purpose of this study was to assess the acute and 12-month outcomes in patients who underwent novel vessel preparation with longitudinal, controlled-depth micro-incisions prior to PTA.
Materials and Methods:
Patients with symptomatic lower extremity peripheral arterial disease with a Rutherford class of 2 to 6 and >70% de novo stenosis of the superficial femoral or popliteal arteries were included in this retrospective study. Patients with thrombotic or embolic lesions, restenosis, or in-stent restenosis were excluded. The FLEX Vessel Prep System (FLEX VP) was used to prepare the vessel prior to PTA by creating micro-incisions at the target lesion. The FLEX VP was followed by POBA or paclitaxel DCB.
Results:
The study included 65 patients. Lesion characteristics were 90% median stenosis (range = 70%–100%), 75.4% mild-to-severe calcifications, and 33.8% occlusion rate, and median lesion length was 196 (range = 10–480) mm. Following vessel preparation, 82.1% of the patients had low severity dissection or no flow-limiting dissection. The provisional stent rate postprocedure was 16.9%, with a median stent length of 60 mm. The freedom from target lesion revascularization (FFTLR) in 63 evaluable patients at 6 and 12 months was 98.4% and 93.7%, respectively. Freedom from amputation was 100%.
Conclusion:
In this real-world/all-comers patient population with long, stenotic lesions across the calcification spectrum, vessel preparation with longitudinal micro-incisions prior to PTA was associated with low dissection rate, low dissection severity, low stent implantation, and high FFTLR with the absence of amputation at 12 months relative to published reports in long-lesion cohorts. These results support vessel preparation via micro-incisions.
Keywords
Introduction
Lower limb arterial occlusive disease is frequently associated with atheromatous stenosis/occlusion of the superficial femoral artery (SFA) and popliteal artery (PA). 1 Percutaneous transluminal angioplasty (PTA) of these arteries may alleviate patients’ symptoms of claudication or critical ischemia. 2 However, this endovascular procedure performed with either plain old balloon (POBA) or drug-coated balloon (DCB) introduces the risk of uncontrolled dissections that require bailout stenting. The number, length, and severity of dissections influence the acute and long-term outcomes of endovascular procedures and predict restenosis and necessity for re-intervention in the SFA and popliteal arteries.3-5 Absence of dissections and National Heart, Lung and Blood Institute (NHLBI) dissections class A and B are predictors of improved long-term patency, whereas dissections C to F are predictors of poor short-term patency. 6 The worse the severity and extent of dissections, the more likely stenting is required. These factors are magnified in long and complex lesions, a prominent patient subset that is now being recognized in recent prospective studies and real-world patient registries.7,8
Various adjunct methods of vessel preparation are being incorporated to reduce the number and severity of dissections associated with PTA, such as prolonged balloon inflation, low pressure inflation, and scoring, excising, or debulking plaque, or creating micro-fractures or micro-fissures in plaque.9,10 The FLEX Vessel Prep System (FLEX VP) is a novel device designed to modify plaque, improve vessel compliance, and facilitate drug delivery from DCBs by creating longitudinal, controlled-depth, circumferential micro-incisions along the entire length of a lesion using a retrograde pullback approach. 11 This mechanism of action is intended to provide immediate improvement in vessel compliance and lumen gain with a predictable plaque modification to reduce the acute need for bailout stent placement and improve long-term outcomes, both potentially significant improvements in peripheral arterial disease (PAD) management. 12 The micro-incision approach may also facilitate dilatation of the stenosis at lower balloon inflation pressures, 13 reducing the barotrauma that may potentiate restenosis. This retrospective study was designed to assess the acute and long-term outcomes in patients who received vessel preparation via FLEX VP prior to PTA for SFA and PA.
Materials and Methods
Patient Selection
All consecutive patients presenting with peripheral artery occlusive disease with significant de novo lesions of SFA or of PA that were treated with longitudinal micro-incisions before angioplasty were considered for inclusion in this retrospective study. The study was conducted in a 320-bed university hospital. Patients were included if they were ≥18 years old and had a diagnosis of PAD, established by noninvasive imaging and confirmation of the lesion location and severity by angiography. The protocol included de novo ≥70% stenosis or occlusion of the SFA and/or PA, without limitation of lesion length. Inflow arteries (iliac and common femoral arteries) had to be free of lesions (>50% stenosis) or successfully treated before inclusion. Inclusion criteria required at least 1 patent tibial run-off vessel. Patients with Rutherford class of symptom 2 to 6 were included. We excluded patients whose interventions were not sufficiently documented, patients who experienced a recent artery thrombosis with risk of distal embolization during the percutaneous procedure, patients requiring tortuous contralateral access, and patients with restenotic lesions or in-stent restenosis (ISR).
Severity of lesion calcification was graded as follows: 1 = no calcification (no opacity visible in the vessel wall during unsubstracted angiography), 2 = mild calcifications (some opacities, not exceeding 180° of vessel circumference), 3 = severe calcification (calcifications exceeding 180° but not filling the lumen), and 4 = massive calcifications (extensive, over 360°, and filling the lumen). There was no exclusion regarding the breadth of lesion calcifications, despite their role in patency prognosis.14,15
Study Design and Statistical Analysis
The design is an investigator-initiated single-center retrospective, single-arm study. All patients gave their informed consent for the intervention and the study was approved by our local ethics committee (Study ID 2018-01056). Patient data were retrieved from the hospital’s electronic files, letters, and vascular interventions database, using keywords such as “longitudinal micro-incisions,” “arterial preparation,” “FLEX vessel preparation tool.” We retrospectively searched all consecutive interventions performed in the interventional suite with the technique of vessel preparation detailed below. Baseline characteristics, images, report of the intervention, and clinical follow-up up to 12 months were analyzed. Data are presented as median and range for nonparametric values and as percentages for categorical variables, respectively. Statistical analyses were performed with Stata version 12.0 (StataCorp LP, College Station, Texas).
Study Outcomes
The patients were followed by visit in our outpatient clinic at 6 and 12 months. At every visit, patients were evaluated by clinical evaluation, including physical examination and PAD stage (Rutherford class of symptoms) for all, duplex scan for all, ankle-brachial index (ABI) for claudicant, and toe-brachial index (TBI) for critical ischemia, following routine practice. The ABI was not performed for all patients, and some patients first investigated by TBI before vessel prep intervention were then controlled by ABI, due to clinical improvement.
The primary outcome was freedom from target lesion revascularization (FFTLR) at 12 months. The target lesion was defined as the single or multiple segments of the SFA and PA that were prepared by longitudinal micro-incisions and angioplasty during the initial procedure. The secondary clinical outcomes included FFTLR at 6 months postprocedure, major limb amputation, and improvement in Rutherford class of symptoms and death. Secondary interventional outcomes were defined as the grade of dissection after vessel preparation and angioplasty, the degree of residual stenosis, the rate of stent implantation, and the technical success of the device as defined by completion of deployment, micro-incision creation, and retrieval without adverse event.
Study Device
The FLEX VP is an endovascular medical device designed for modifying plaque in the SFA and PA before PTA (POBA, DCB) (Venture Med Group, Minneapolis, Minnesota). The FLEX VP is an over-the-wire sheathed catheter with a 3-strut treatment element at the distal tip, with 6 French sheath compatibility and 0.014 inch or 0.018 inch guidewire compatibility in 2 working lengths (40 or 120 cm). The proximal portion of each treatment element strut includes a 0.010″ microsurgical blade. Once the device is advanced past the lesion, the treatment element is deployed and expanded, and the catheter is slowly drawn back, allowing the microsurgical blades on the proximal end of each treatment element strut to independently engage in the lesion and create 3 parallel, circumferential continuous micro-incisions, with a depth of approximately 250 microns, along the entire length of the lesion. Once the lesion is crossed, the treatment element is re-sheathed and advanced again through the lesion, rotated approximately 30° before the treatment element is re-deployed and the retrograde pullback described above is repeated. This process is repeated, as required, based on individual lesion anatomy. For example, a procedure with 4 passes of the device prepares the artery by performing 12 longitudinal micro-incisions in the fibrotic/atheromatous deposit. Artery preparation with longitudinal micro-incisions facilitates a concentric dilatation of the atheroma when either the POBA or DCB balloon is inflated (Figure 1).
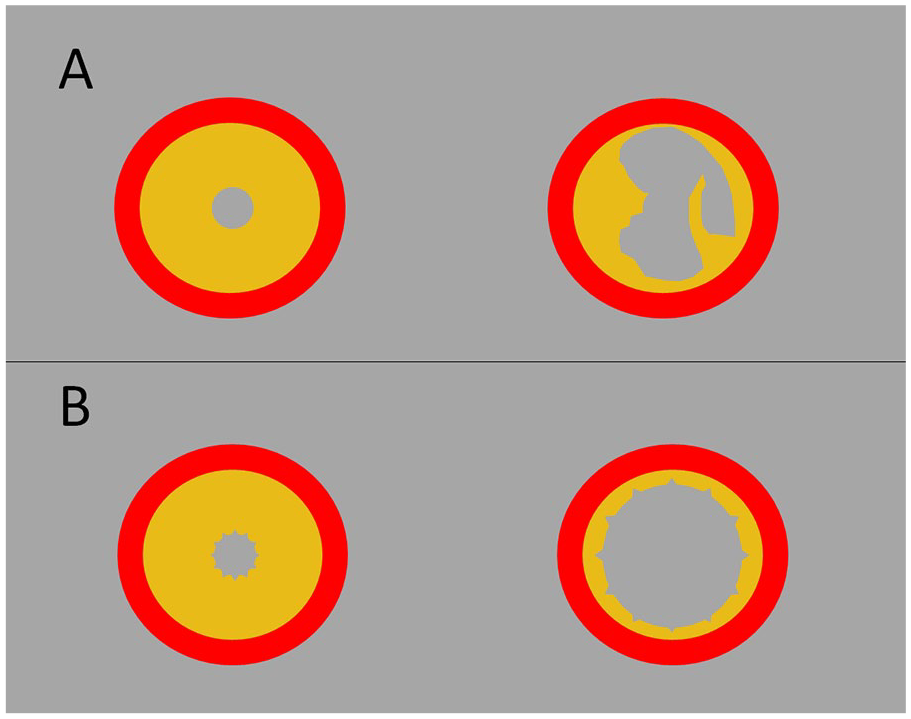
Illustration of proposed mechanism of action of vessel preparation with longitudinal micro-incisions: (A) Angioplasty without preparation result in uncontrolled dissection. (B) Longitudinal micro-incisions before angioplasty favor plaque spreading and provide less severe dissection.
Endovascular Procedure
A conventional angiography of the affected limb was performed with a 6 French introducer sheath placed in the groin. Bi-planar angiographies of the limb were performed from the groin down to the foot with at least 60° incidence difference. The target lesion was defined as the segment from the proximal healthy edge to the distal healthy edge of the lesion. An 0.018 inch guidewire was placed intraluminally through the target lesion, with traversing determined as mainly intraluminal if no reentry device was used to go back in the lumen. After preparation of the target lesion by FLEX VP, a single angiogram of the lesion was obtained, followed by inflation of a POBA or paclitaxel-coated angioplasty balloon (3 µg/mm2; Freeway; Eurocor, Bonn, Germany) for a standard 3 minutes after attaining nominal pressure all along the target lesion, aiming at the reference diameter of the artery. Postdilatation was performed when necessary. A focal nitinol stent was implanted in case of a flow-limiting dissection or residual stenosis ≥ 50% postdilatation. At the end of the procedure, biplanar angiography was performed at the same angulations on the target lesion with the same incidences as at the diagnosis procedure.
Dissection Evaluation
This outcome was evaluated by grading any dissections using angiography after the preparation phase and angioplasty, before implanting any stent. Target lesions were examined by an independent author who did not participate in the interventions. As previously utilized for peripheral dissections, we used the NHLBI dissection grade to classify dissections in 6 categories from A to F based on multiple incidence angiograms, with Dissections of A and B considered to be minor. 6
Results
Patients and Lesion Characteristics
From April 2017 to April 2019, 65 patients (60% men, median [range] = 72 [43–95] years) with de novo femoral-popliteal lesions were treated with FLEX VP before conventional PTA and/or DCB ± stent. The clinical characteristics of these patients are shown in the Table 1. Patients suffered from claudication in 76.7% and critical limb ischemia in 23.1%. The median lesion length was 196 (10–480) mm with a median 90% stenosis (70%–100%). A total occlusion was present in 22 patients (33.8%) with a median occlusion length of 160 (10–450) mm. Calcifications were present in 75.4% of the cases (classification 1 or 2 = 23.1%, classification 4 = 6.2%).
Baseline Demographics and Clinical Characteristics.
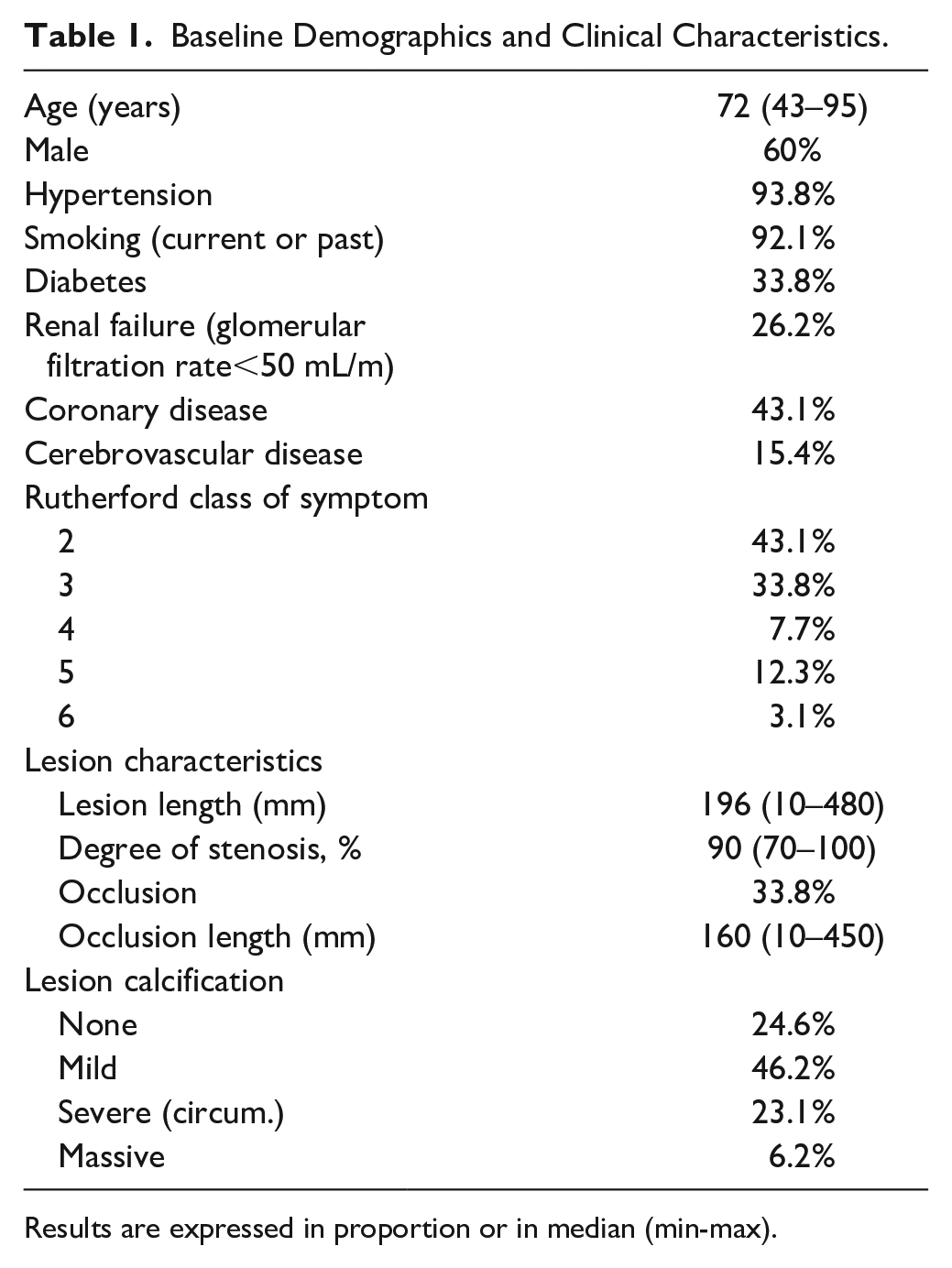
Results are expressed in proportion or in median (min-max).
Technical Success of the Vessel Preparation
Access was antegrade for 90.8% of patients, with a 6 French 10 cm sheath for all (Table 2). A predilatation with a 3 mm PTA balloon was necessary in 4.6% of patients to allow the passage of the device, due to highly calcified occlusions. There was 100% technical success noted of the vessel preparation device, and all patients could be treated with 4 passes (12 longitudinal micro-incisions) before angioplasty. Paclitaxel DCB PTA was performed in 93.8% of patients (61/65) with POBA PTA performed in 6.2% (4/65) of the patients. Although POBA PTA was used in a small population of patients, they were included in the subsequent analysis on technical and clinical outcomes associated with micro-incision vessel preparation agnostic of PTA.
Technical Success of the Interventions (N=65).
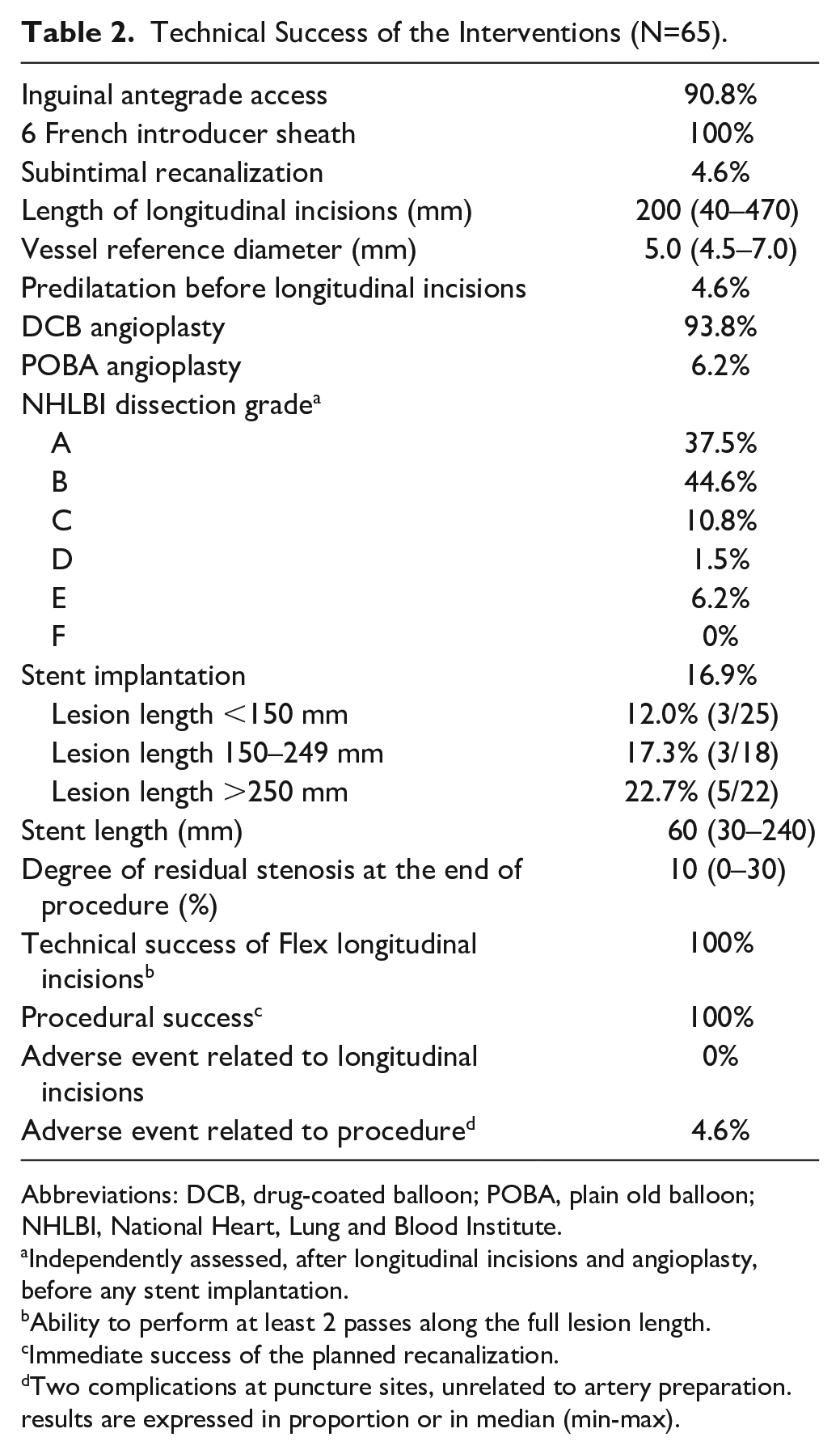
Abbreviations: DCB, drug-coated balloon; POBA, plain old balloon; NHLBI, National Heart, Lung and Blood Institute.
Independently assessed, after longitudinal incisions and angioplasty, before any stent implantation.
Ability to perform at least 2 passes along the full lesion length.
Immediate success of the planned recanalization.
Two complications at puncture sites, unrelated to artery preparation.
results are expressed in proportion or in median (min-max).
Dissection Grade and Stent Implantation
Dissection grade, assessed after vessel preparation and angioplasty, was low (A and B) in 82.1% of patients (37.5% and 44.6%, respectively). In 10.6% of patients, a C grade dissection was present, and 7.7% of patients had a more severe dissection. Provisional stent implantation was performed in 16.9% of patients (11/65) with 3 stents placed in lesions <150 mm long, 3 stents placed in lesions 150 to 249 mm long, and 5 stents placed in lesions >250 mm long. Median stent length was 60 mm. Residual stenosis at the end of intervention was 10% (0%–30%) (Table 2). The interventions were well tolerated, without any technical events or adverse events related to the artery preparation. There were no vessel perforations or distal embolizations observed. Figure 2 shows a typical example of long stenosis/occlusion recanalized with the FLEX VP and PTA, achieving satisfactory vessel patency without a stent.
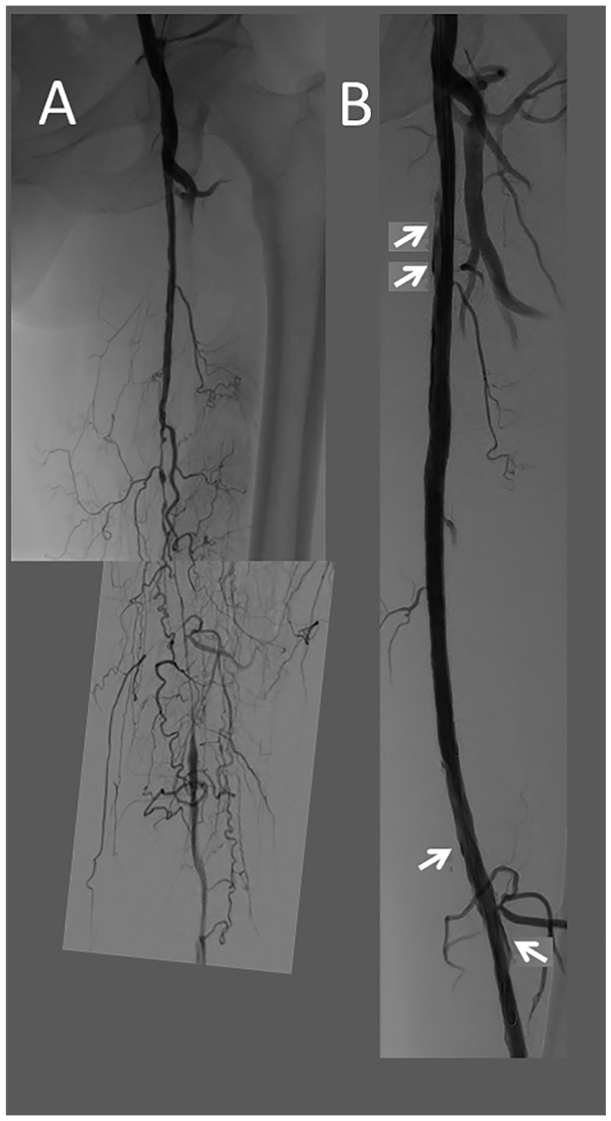
Recanalization of a long SFA/pop lesion: (A) Initial angiography. (B) Result after FLEX VP and DCB. The longitudinal dissections (arrows) do not limit the flow. SFA, superficial femoral artery; FLEX VP, FLEX Vessel Prep System; PTA, percutaneous transluminal angioplasty.
Clinical Outcomes
Two patients (3.1%) died prior to the 6-month evaluation of causes unrelated to the baseline procedure (hip fracture followed by pneumonia; cholangeitis with multiple complications). The remaining 63 patients were evaluable at 6 and 12 months with no additional adverse events observed during follow-up. Table 3 shows the main clinical outcomes. The FFTLR of evaluable patients at 6 and 12 months was 98.4% (62/63) and 93.7% (59/63), respectively. All evaluable patients with lesion lengths less than 250 mm (41/41) were 100% free from TLR at both timepoints. No patients required limb amputations during follow-up. The clinical improvement after intervention was a median gain of 2 (–1 to +5) points in the Rutherford classification of symptoms. The FFTLR at 6 months for patients requiring provisional stents was 90.9% (10/11) with 100% FFTLR extending to 12 months of evaluable patients (10/10 patients who demonstrated FFTLR at 6 months).
Clinical Outcomes at 6 and 12 Months.
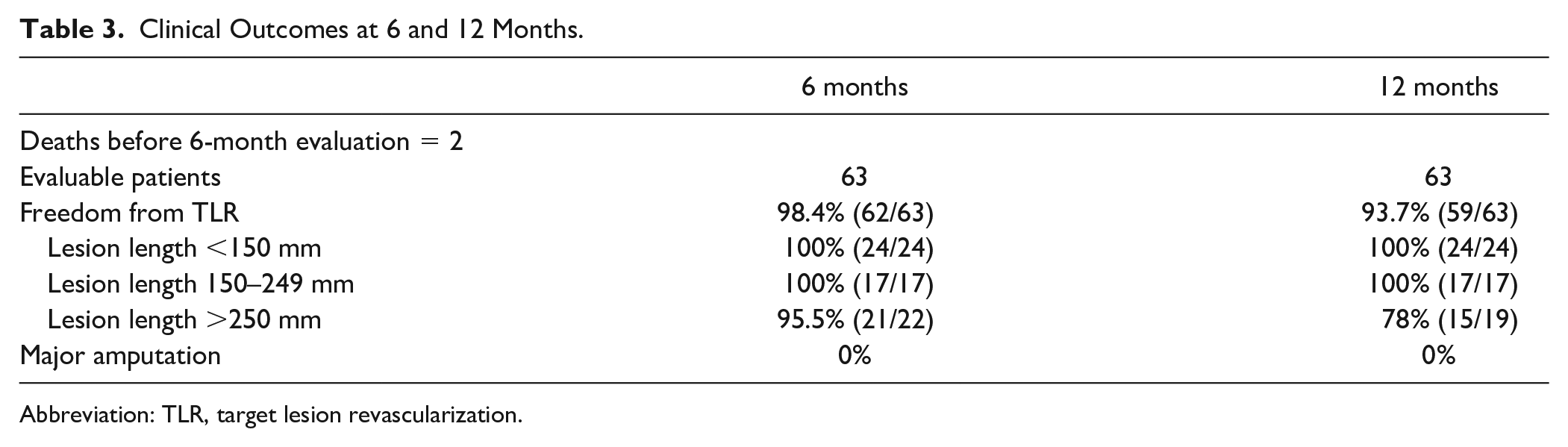
Abbreviation: TLR, target lesion revascularization.
Table 4 presents the clinical outcomes by stratification of stenosis cases (n=41) versus occlusion cases (n=22). The FFTLR in stenosis cases was 97.6% at 6 months (40/41) and 95.1% (39/41) at 12 months. For patients with occlusions, FFTLR was 100% at 6 months (22/22) and 90.1% at 12 months (20/22).
Clinical Outcomes Stratified for Stenosis Versus Occlusion.
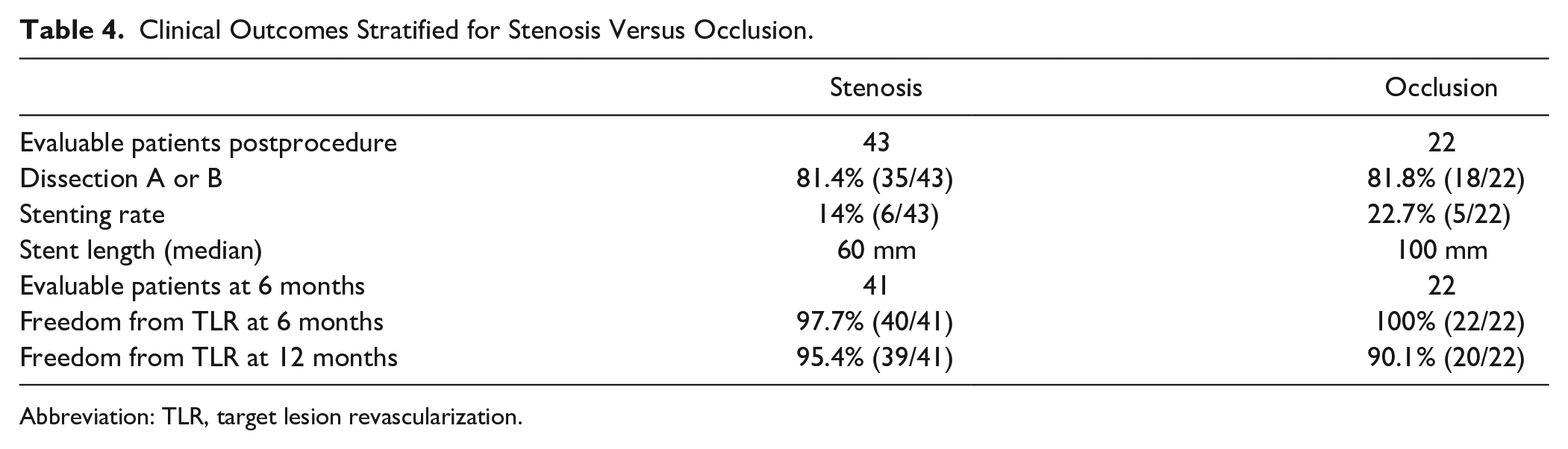
Abbreviation: TLR, target lesion revascularization.
Discussion
This retrospective study reports acute and long-term clinical outcomes in patients with long, calcified lesions who underwent vessel preparation using the FLEX VP System prior to PTA. The FLEX VP System is designed to modify plaque and improve vessel compliance by creating predictable longitudinal and circumferential micro-incisions. The acute results of low dissection severity and provisional stent rate of 16.9% support a prospective study by Zeller and colleagues who reported provisional stenting in 19.2% of 255 patients with long femoral-popliteal lesions (133±88 mm) treated with FLEX VP prior to conventional endovascular treatment. 13 Furthermore, the stent rate and stent length are lower than the 32% to 35% bailout rate and 168.4 mm, respectively, reported in previous studies in DCB-treated patients with long lesions (>14 cm).7,8 Focusing in on the longest lesions, provisional stents were required in 22.7% of lesions >25 cm (5/22) relative to a 50.9% reported in the this long-lesion cohort by Scheinert and colleagues. 7
The long-term outcomes of 93.7% FFTLR and the absence of major amputation are promising, considering that most cases were long and calcified lesions. The clinical outcomes reported here are comparable with 12-month FFTLR rates reported in evaluations of DCB for long SFA and PA lesions in the IN.PACT Admiral Global Study (91.1%) 7 and the Lutonix Global SFA Registry (93.4%). 8 When considering lesion length, FFTLR was 100% in evaluable patients with baseline lesions less than 250 mm. Reduced FFTLR associated with lesions greater than 250 mm (81.8% at 12 months; 18/22) is similar to results reported in a long-lesion cohort of DCB-treated patients. 7 In addition, similar FFTLR rates were observed when considering long-term clinical outcomes based on provisional stenting, with the nonstented population and stented population demonstrating 12-month FFTLR of 92.9% and 100%, respectively. 7
Paclitaxel coated balloons have become a common endovascular option to treat PAD by inhibiting potential restenosis via exposure of the vessel walls to the drug while leaving “nothing behind.” Although vessel preparation prior to endovascular interventions has typically been promoted to reduce acute complications (eg, prolonged balloon inflation, uncontrolled dissection, bailout stenting),9,10 recent attention has focused on the potential advantage of vessel preparation to enhance DCB drug transfer.16,17 The FFTLR at 12 months following Freeway DCB treatment has been reported in patients with ISR (49%) and patients assigned to primary stenting prior to DCB (77.4%).18,19 Here, we are reporting FFTLR rates following FLEX VP + Freeway paclitaxel DCB treatment of long complex de novo lesions that are comparable with FFTLR rates associated with the IN.PACT Admiral paclitaxel DCB (Medtronic, Minneapolis, Minnesota) in the IN.PACT Global study. Although we are unaware of published studies evaluating the Freeway DCB in de novo SFA lesions, Freeway DCB treatment was associated with lower FFTLR rate at 12 months in patients with SFA/PA ISR (49%) compared with similar patients treated with the IN.PACT Admiral DCB (92.9%).18,20 Thus, the encouraging 12-month patency results observed here suggest that vessel preparation with circumferential, controlled-depth, and continuous micro-incisions may optimize DCB drug delivery to reduce post-PTA cell proliferation and migration. 21
A limitation of this study is the lack of a matched cohort for PTA only or PTA with an alternative vessel preparation method, thus preventing direct comparison of therapeutic regimens. In addition, the retrospective nature of this study limited the degree and standardization of clinical outcomes to review, such as inclusion of ABI as an endpoint.
Conclusion
This single-center retrospective study shows that most femoral or popliteal real-world lesions, regardless of their length and degree of calcification, can be safely and efficiently recanalized by this technique without adverse events. These results suggest that arterial preparation using longitudinal, concentric micro-incisions to modify obstructive plaque may provide both short- and long-term benefit by improving vessel compliance, lower the rate and severity of dissections, thereby reducing the need for stenting, thus supporting the clinical intention to “leave nothing behind,” maintaining clinical outcomes, and providing more options in the event of subsequent treatment. Results from this retrospective observational study are currently being investigated in the BELONG prospective study (NCT03721939).
Footnotes
Acknowledgements
We thank Amy Moore, PhD, for manuscript review.
Authors’ Note
Data from this manuscript have been accepted for presentation at LINC 2021
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.