
Abstract
Purpose:
The endovascular approach for eccentric calcified lesions of the no-stenting zone is challenging. This study aimed to investigate the effect of a novel technique for these lesions.
Methods:
We performed EVT for severe and eccentric calcified lesions using the technique, which is presented previously and named aggressive wire recanalization in calcified atheroma and dilatation (ARCADIA). In brief, a guidewire is passed to the residual lumen firstly. Next, another guidewire is advanced into and cross through the calcified plaque and returned to the distal original lumen with intravascular ultrasound (IVUS) guided. The calcified plaque is dilated by using a scoring-balloon or non-compliant balloon.
Results:
Consecutive 14 peripheral artery disease patients with isolated and eccentric calcification in a no-stenting zone were treated using ARCADIA technique between January 2018 and March 2020. In IVUS data, lumen cross-section area was significantly increased from 5.2 ± 2.0 mm2 to 18.1 ± 6.9 mm2 (p < 0.01), lumen area was expanded roundly evaluating as symmetry index from 0.45 ± 0.09 to 0.81 ± 0.12 (p < 0.01). There were no distal embolization and perforation after ARCADIA technique. One-year target lesion revascularization occurred in only 2 cases. The primary patency of 1 year was 85.7%.
Conclusion:
ARCADIA technique is safe and appropriate, and can be 1 option to treat for eccentric calcified lesions of the no-stenting zone as an optimal wire crossing method.
Introduction
Endovascular therapy (EVT) for the management of peripheral artery disease (PAD) has been increased and established as a first-line strategy. 1 Recently, stent-less EVT using a drug-coated balloon (DCB) has become a novel and effective strategy for PAD, especially for no-stenting zone (common femoral artery [CFA] and popliteal artery [PopA])2,3 A no-stenting zone is a site that should be avoided stenting like the name owing to the flexibility of the hip or knee joint4,5 Therefore, a no-stenting zone should be treated by balloon-based angioplasty.
Moreover, in the no-stenting zone, the eccentric calcified plaque is one of the most difficult tissue character and morphology to treat at the point that is hard to be expanded well and is easy to create dissection even though the stenting should be avoided. It is crucial for vessel preparation to minimize major dissections and to maximize the luminal gain before using not only DCB but also any scaffolding devices.
To obtain adequate luminal gain after balloon angioplasty as possible, we performed aggressive wire recanalization in calcified atheroma and dilatation (ARCADIA) technique to PAD with an eccentric calcified lesion as for a novel original technique. 6 Since the recommended method of optimal preparation has not been established for eccentric calcified lesions especially for a no-stenting zone, we investigated the effect of the ARCADIA technique before using DCB for eccentric calcified lesions of the no-stenting zone (CFA or PopA) in this study.
Methods
ARCADIA Technique
We performed EVT for PAD with an isolated and eccentric calcified lesion of the no-stenting zone. First, a guide-wire was passed to the residual lumen. Next, another guide-wire was advanced into the calcified plaque and returned into the distal original lumen with intravascular ultrasound (IVUS) guided (Figure 1A) and dilated the calcified lumen by non-compliant or scoring balloon with/without flossing using CROSSER (Figure 1A-1C) to cross devices such as IVUS, microcatheters, and balloons. In the cases using CROSSER, we used it only for a purpose to help devices to cross the calcified lesion. Finally, we performed a drug application using DCB (Figure 1D).
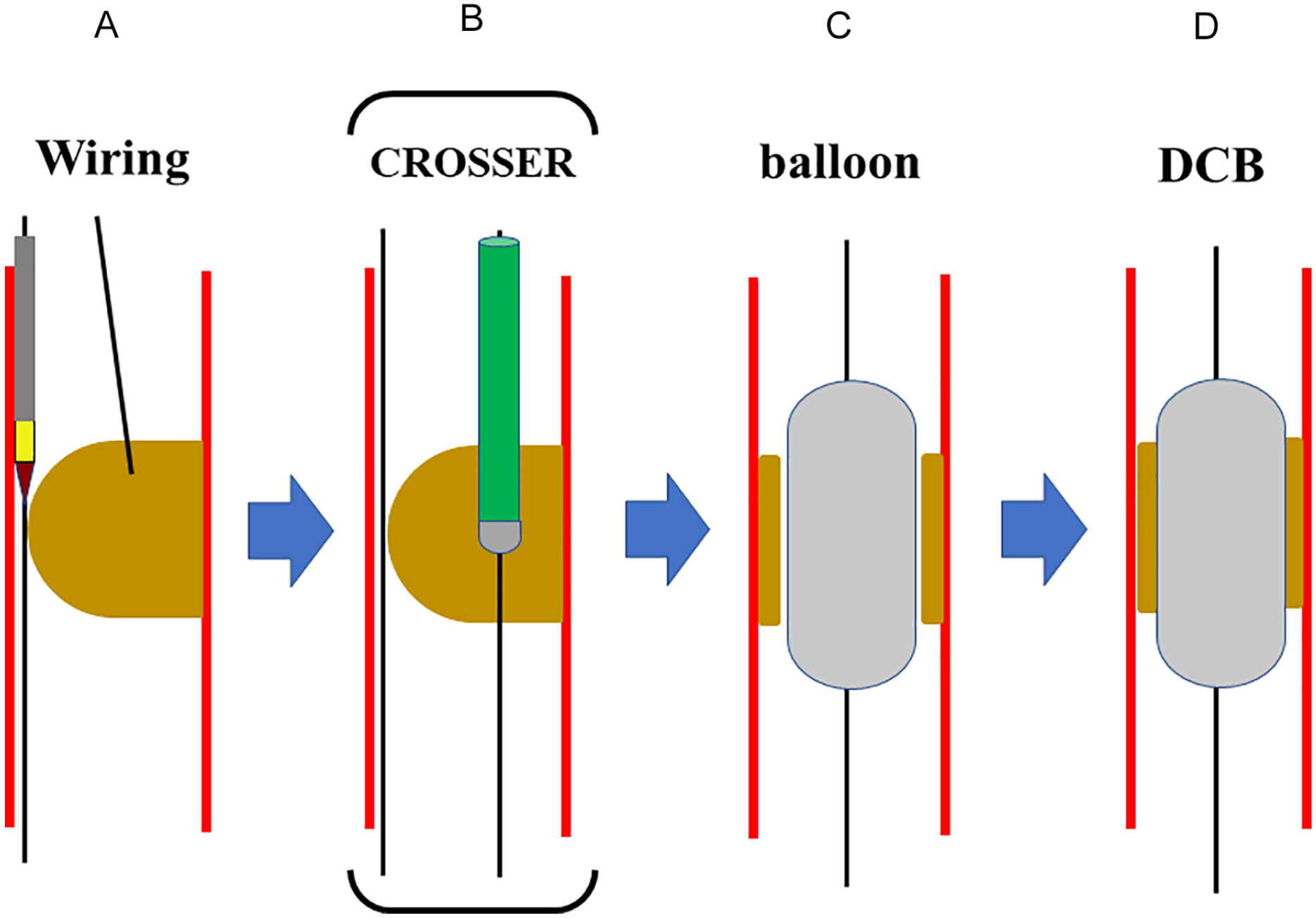
ARCADIA technique: (A) first, a guide-wire was passed to the residual lumen. Next, another guide-wire was advanced into the calcified plaque and returned into the distal original lumen with intravascular ultrasound (IVUS) guided, (B, C) dilate the calcified lumen by scoring-balloon with/without using CROSSER, and (D) a drug application using DCB. ARCADIA, aggressive wire recanalization in calcified atheroma and dilatation; DCB, drug coated balloon.
A representative case of the ARCADIA technique is shown in Figure 2.
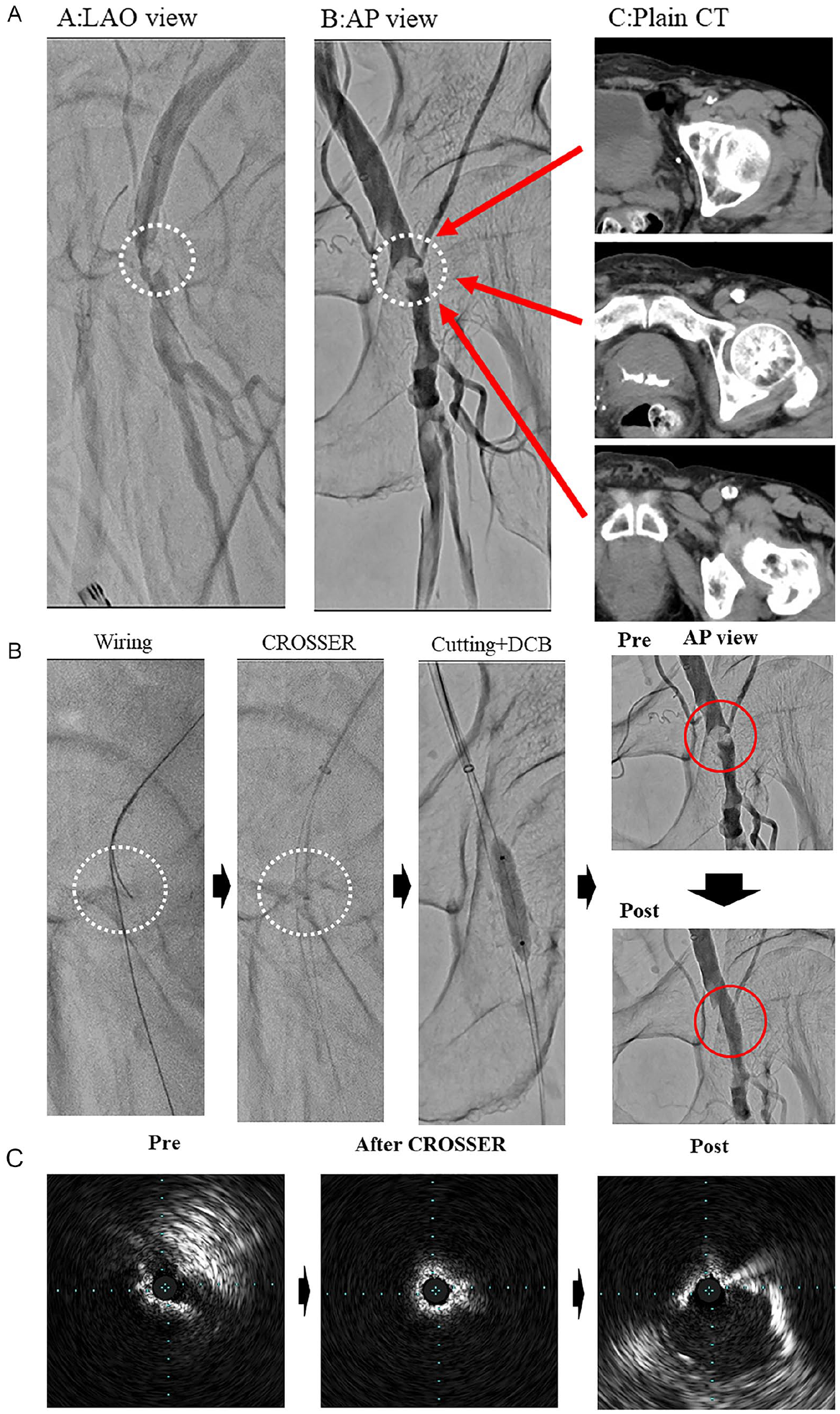
A representative case of the ARCADIA technique: (A) pre-procedure angiography (A-P view and LAO view) and plain CT 76-year-old male, the target lesion was the left common femoral artery with severe eccentric calcified plaque, (B) ARCADIA technique. A second wire (40g tip load) was advanced into the calcified plaque using a dual lumen catheter. The calcified plaque was dilated by using CROSSER and cutting-balloon. Then a drug application was done using DCB, AND (C) IVUS data (pre, after CROSSER, and post-procedure) at MLD IVUS image in the calcified plaque after CROSSER: looked like “napkin ring” The eccentric calcified plaque was well dilated roundly without dissection. ARCADIA, Aggressive Wire Recanalization in Calcified Atheroma and Dilatation; CT, Computed Tomography; LAO, Left Anterior Oblique; DCB, drug coated balloon; IVUS, intravascular ultrasound; MLD, minimum lesion diameter.
Patients and Data Collection
The present study was a single-center, observational, retrospective cohort study and included consecutive patients who underwent EVT at Toyohashi Heart Center (Aichi, Japan) between January 2018 and March 2020. Among them, the object lesions of this study were isolated CFA or PopA (no-stenting zone) with eccentric calcified plaque. The exclusion criteria for analysis were the unsuccessful cases of the ARCADIA technique. In Japan, since any atherectomy devices, such as the Silver Hawk (Foxhollow Technologies, Inc., Redwood City, California), Turbo Hawk (Medtronic-Covidien, Dublin, Ireland), and Jetstream PV (Boston Scientific, Marlborough, Massachusetts) have not yet been available, we did not use any atherectomy devices in this study. The hospital’s internal review board approved this study. Informed consent was obtained from all patients.
Baseline data included age, sex, revascularization procedure-related factors, and comorbidities were collected from each patient. Lesion diameter, length, and diameter stenosis were measured by quantitative end-vascular angiography system (Q Angio XA7.3 [Medis Medical Imaging System, Leiden, the Netherlands]). The severity of vessel dissection after balloon angioplasty was classified by angiography (Non and A-F grade). 7 IVUS analysis was as follows. IVUS imaging was performed at pre-procedure and post ARCADIA technique from lesion distal to proximal. Manual contour detection of both the lumen and the external elastic membrane (EEM) was performed by 2 experienced analysts who were blinded to baseline clinical and angiographic lesion characteristics. The lumen cross-sectional area (CSA), EEM CSA, the long and short-axis diameter of lumen area at minimum lesion diameter (MLD) were measured by IVUS. The evaluation of lumen roundness was examined as symmetry index (lumen short-axis diameter divided by long-axis diameter).8,9 The patients were followed by measuring ankle-brachial index (ABI) every 2 or 3 months. In the case of ABI decrease > 0.15, we checked ultrasound (> 50% reduction in luminal diameter suggested by a peak systolic velocity ratio [PSVR] ≥ 2.5 comparing the stenosis with a proximal reference segment was judged as restenosis). 10 The target lesion revascularization (TLR) was defined as any repeat EVT or surgical revascularization because of restenosis (ABI: decrease of > 0.15 and Ultrasound: > 50% reduction in luminal diameter suggested by a PSVR ≥ 2.5) associated with limb symptoms. The data of TLR were collected by serial contact with patients and medical records.
Statistical Analysis
The results are expressed as mean ± SD or medians (interquartile range) for continuous variables and as percentages (%) for categorical variables. Pre and post-procedural data were compared using paired t-test. All data were analyzed using JMP 10.0 MDSU statistical software (SAS Institute, Cary, North Carolina).
Results
Patients and Procedural Characteristics
During the study period, a total 436 patients were undergone EVT. 94 patient’s target lesions were contained a no-stenting zone (CFA or PopA). Among them, 15 patient’s lesions were isolated CFA or PopA with eccentric calcified plaque. Only 1 case was excluded from analysis because of unsuccess by ARCADIA technique. Finally, 14 patients were succeeded by the ARCADIA technique and analyzed (Figure 3). Half of the patients were hemodialysis (Table 1).
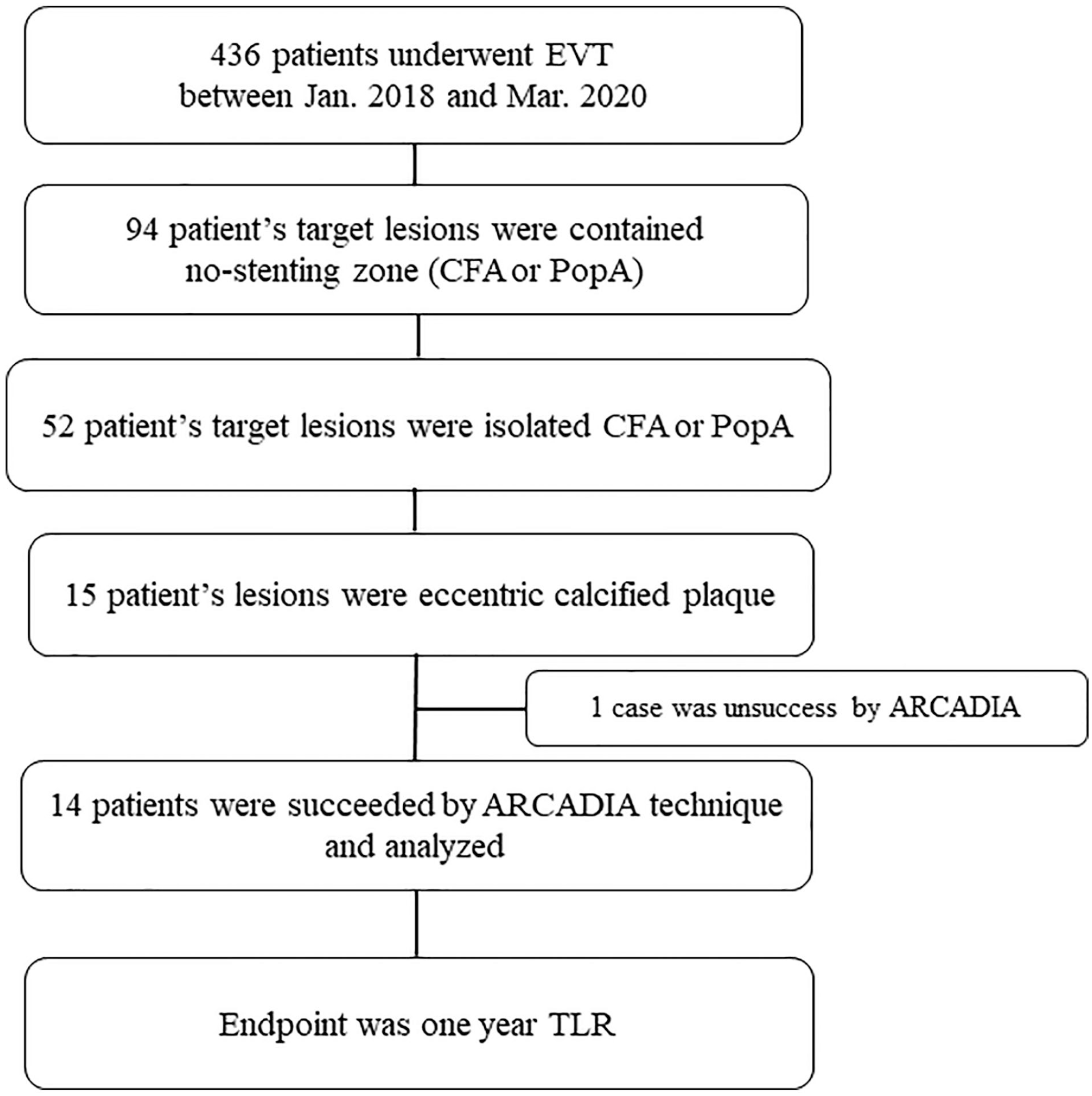
Study populations.
Baseline Clinical Data of Patients.
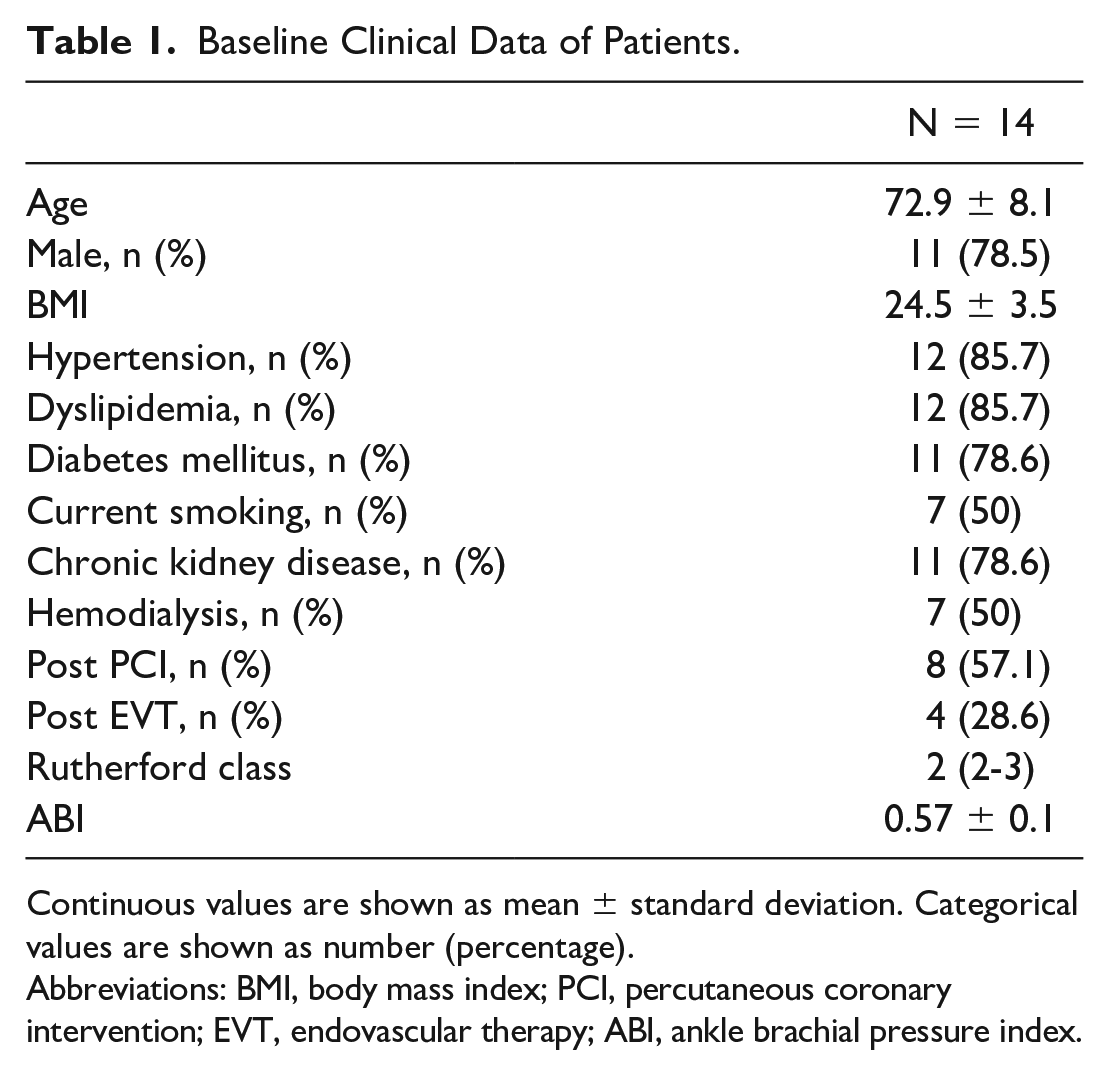
Continuous values are shown as mean ± standard deviation. Categorical values are shown as number (percentage).
Abbreviations: BMI, body mass index; PCI, percutaneous coronary intervention; EVT, endovascular therapy; ABI, ankle brachial pressure index.
Tapered stiff wire 40 g tip load was used in most cases (71.5%) as the final passed wire. The inflation duration of ballooning into calcified plaque was 300 seconds. The mean fluoroscopic time was 57.8 minutes (Table 2).
Angiographic and Procedural Characteristics.
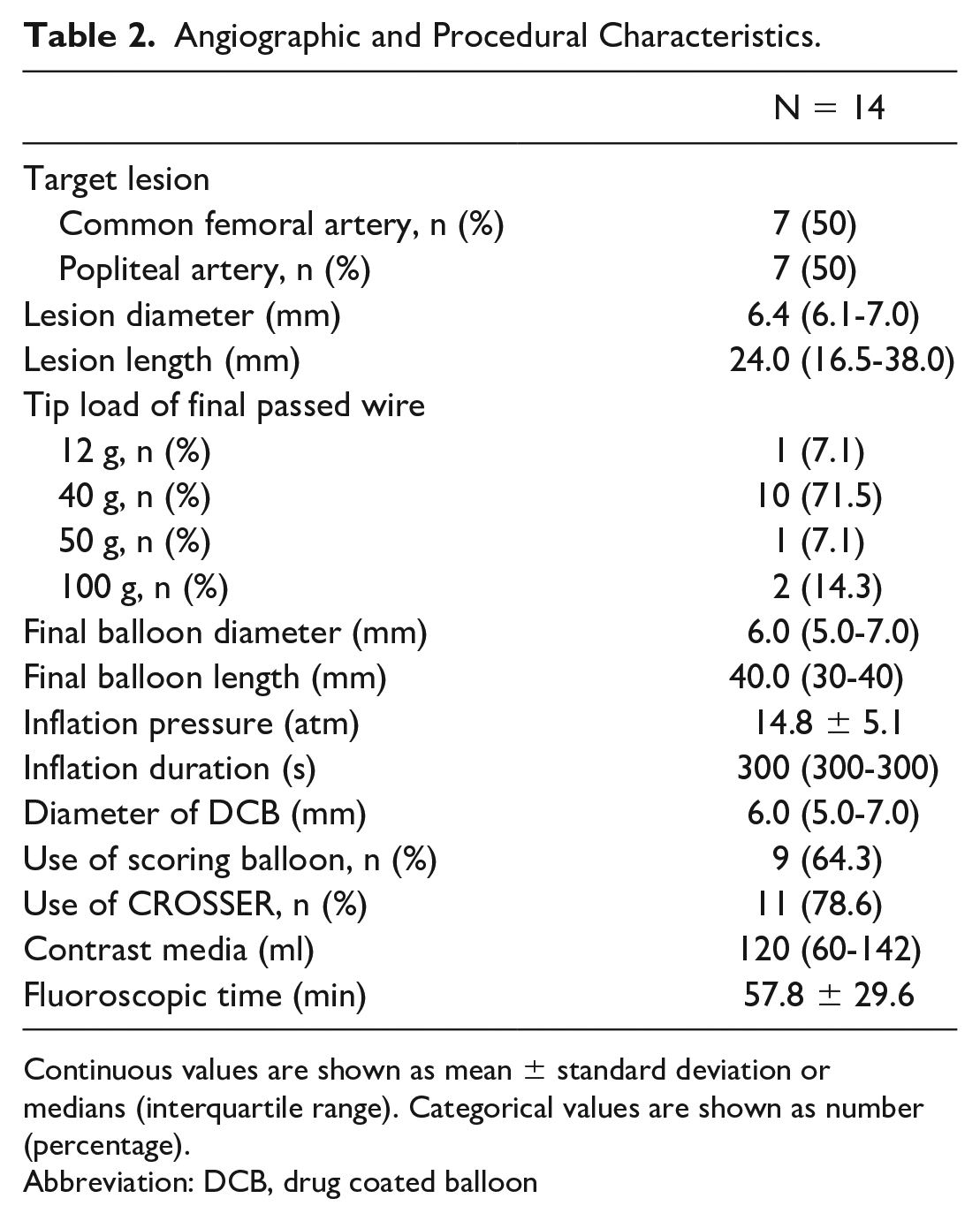
Continuous values are shown as mean ± standard deviation or medians (interquartile range). Categorical values are shown as number (percentage).
Abbreviation: DCB, drug coated balloon
Procedural Results
The success rate of the ARCADIA technique was 93.3% (14/15). The rate of procedural complication (hematoma, wire perforation, dissection, and embolism) was 0% (0/15). The dissection grade after ballooning was under grade A in almost all cases (13/14). Lumen CSA was significantly increased from 5.2 ± 2.0 mm2 to 18.1 ± 6.9 mm2 (p < 0.01), Symmetry index was also significantly increased from 0.45 ± 0.09 to 0.81 ± 0.12 (p < 0.01) compared between pre- and post-EVT (Table 3).
Procedural Results.
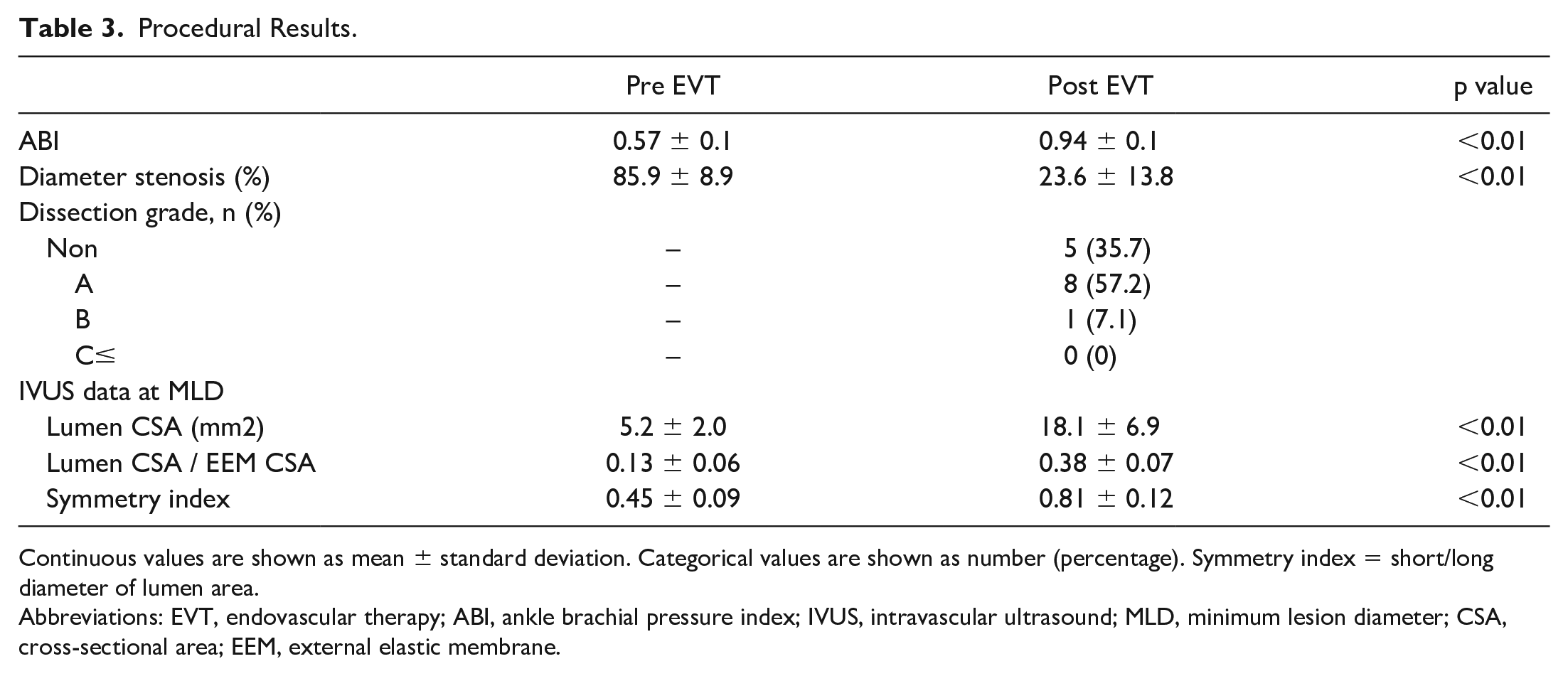
Continuous values are shown as mean ± standard deviation. Categorical values are shown as number (percentage). Symmetry index = short/long diameter of lumen area.
Abbreviations: EVT, endovascular therapy; ABI, ankle brachial pressure index; IVUS, intravascular ultrasound; MLD, minimum lesion diameter; CSA, cross-sectional area; EEM, external elastic membrane.
Follow-Up
All cases (14/14) were followed at 1 year. The primary patency of 1 year was 85.7% (TLR [2/14]) (Table 4).
1 Year Follow-Up Data.
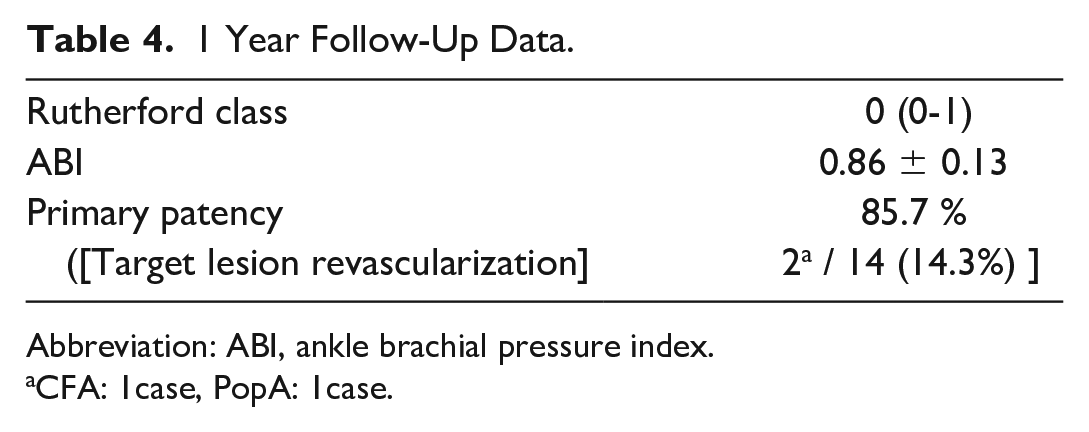
Abbreviation: ABI, ankle brachial pressure index.
CFA: 1case, PopA: 1case.
Discussions
The major findings of our present study were as follows: (1) ARCADIA technique before using DCB was an effective strategy for eccentric calcified lesion (1-year primary patency 85.7%), (2) Success rate of the ARCADIA technique was high (93.3%) and no complications, and (3) It was possible to dilate eccentric calcified plaque certainly and like a circle by the ARCADIA technique.
The severe calcified plaque has been one of the difficult lesions for EVT. Especially, the eccentric calcified plaque is one of the most difficult morphology at the point that is hard to be expanded well and is easy to create vessel dissection or perforation. In the case of vessel dissection or perforation, stents or stent-graft were implanted as a bailout strategy. However, these bailout strategies are not suitable for the no-stenting zone (CFA and PopA) since CFA and PopA are located in regions of joint motion, where flexion and extension levels are high.4,5 Therefore, the endovascular approach for eccentric calcified lesions of the no-stenting zone is challenging. The recommended percutaneous method of optimal preparation has not been established for the eccentric calcified lesion. We developed a useful technique for crossing a calcified plaque and dilatation, which was presented previously and named ARCADIA. 6
There have been some previous reports about techniques for eccentric calcified plaque. Maruyama T and colleagues reported GLASS CUT technique. 11 After the first wire passed the residual lumen, the CROSSER was passed through the other wire which was crossed the calcified plaque to create new cracks and lumens, then a large scoring balloon was inflated to the residual lumen. The difference point between the GLASS CUT and ARCADIA technique was the dilatation site. In GLASS CUT, the dilatation site was the residual lumen (passed first wire). On the other hand, in ARCADIA, the dilatation site was calcified plaque itself (passed second wire). Since there are no IVUS data and follow-up data in GLASS CUT, we don’t know about lumen obtaining and clinical outcome. The lumen area was significantly increased from 5.2 ± 2.0 mm2 to 18.1 ± 6.9 mm2 (p < 0.01) after ARCADIA technique. Furthermore, lumen area was expanded roundly evaluating as symmetry index (from 0.45 ± 0.09 to 0.81 ± 0.12 [p < 0.01]). One-year primary patency was 85.7%. Hayakawa N and colleagues reported BAMBOO SPEAR technique. 12 The calcified plaque was punctured from distal CFA and penetrated using a metal needle, and dilated using a scoring balloon. This technique is a similar concept as ARCADIA in the point of expanding the calcified plaque well. However, this technique is more invasive compared with ARCADIA because of bleeding and patient’s pain followed by puncturing with a metal needle from outside of the vessel directly. Therefore, the BAMBOO SPEAR technique should be better to try if the ARCADIA technique was failed. Since the success rate of ARCADIA is very high (93.3%), BAMBOO SPEAR can be 1 option of wire crossing method for more solid and tough calcified lesion, which is hard to cross using ARCADIA technique. Nagatomi S and colleagues reported SMASH technique. 13 This technique resembled the ARCADIA technique in the point of expanding the calcified plaque. The difference point was the number of routes passing through the calcified plaque. In the SMASH technique, the guide wires were advanced into the calcified plaque multiple routes, followed by balloon angioplasty via each route. Therefore, the calcified plaque was turned off and the fragments may cause distal embolism. The distal embolism by calcified plaque is difficult to bail out because there is no way to dissolve calcium fragments. On the other hand, since we crossed the second wire into the center of the calcified plaque only 1 route in the ARCADIA technique, there were no cases complicated with distal embolism in our previous and present study. 6
Supera peripheral stents (Abbott Vascular) have a significantly higher radial resistive force and crush resistance (if correctly implanted) compared with other stents.14,15 Therefore, Supera stents were chosen as for bailout stent strategy in a no-stenting zone. Some previous data confirmed the Supera stents have shown safety and excellent patency in the no-stenting zone (CFA or PopA).16,17 In the ARCADIA technique, since there were no cases of major dissection, we didn’t need to implant stents as for bailout in the present data. However, if major dissection occurred after ballooning for calcified plaque, the implantation of Supera stents might be suitable. Though Supera stents have a strong radial force and crush resistance, this performance is demonstrated if stents are correctly implanted. If the vessel is not adequately prepared with angioplasty, the stents are deployed to the smaller diameter and will elongate according to how constrained it is on deployment. This occurs because the stent manifests an inverse length-to-diameter relationship. Therefore, it is very important to achieve maximal expansion before implantation of the stents to have the full benefit of its radial force and to maximize lumen area. The eccentric calcified plaque is the most difficult lesion to expand well without vessel perforation by the standard angioplasty. On the other hand, it was possible to dilate eccentric calcified plaque certainly and like a circle by the ARCADIA technique. This preparation might be also important in the case of Supera stents implantation in eccentric calcified plaque. Though Supera stents have been designed to resist stent fracture, this stent is not perfect, sometimes be fractured the same as other stents. 18 Naturally, a no-stenting strategy using DCB is the best option in CFA or PopA lesions. Especially for CFA, since the CFA is an important access site of percutaneous coronary intervention or cardiac supporting devices, we had better try to treat the CFA without stents, if it’s possible. The present study confirmed ARCADIA technique before using DCB was an effective preparation for eccentric calcified lesions without debulking (or ablating) device (1-year primary patency 85.7%). Also, there were no cases complicated with perforation after balloon dilatation even in a super-eccentric calcified lesion in this study. The effect of DCB might be limited in patients with a higher degree of calcium (> 270°) plaque. 19 However, calcified plaque modification might alter local drug delivery for peripheral atherosclerosis. 20 Since the calcified plaque is not only dilated from the inside, but also dilated using a scoring balloon and/or CROSSER in the ARCADIA technique, we expect the effect of DCB though it is a calcified lesion in the present study.
We have developed a useful new technique (ARCADIA) for eccentric calcified plaque, especially the no-stenting zone. The difficult point of this technique is to cross the second wire through the calcified plaque (Figure 1A). The tips of this technique were (1) understanding the distribution of calcified plaque by using IVUS and (2) using above 40 g tip load wire as for second wire to advance into and cross through the calcified plaque.
The present observational study has some limitations. The study cohort was a small and retrospective study. Since the surgical endarterectomy for CFA disease is still considered the gold standard for treatment, the number of EVT cases is limited. Since the factors of restenosis become unclear in the case of diffuse lesions, we focused on the isolated CFA or PopA lesion in this study. This study was a single-arm study including no cases in which ARCADIA technique was not performed. Although angiographical and IVUS data were analyzed by 2 experienced analysts who were blinded to baseline clinical characteristics, there was no adjudication of an independent core lab. Although IVUS guided wiring is useful for ARCADIA technique to achieve successful guidewire crossing of the calcified lesion, fluoroscopy-guided wiring is also required to advance the wire into the calcified plaque in the case of not passing the IVUS through the residual lumen.
Conclusion
Eccentric calcified plaque can be well dilated and compressed by balloon angioplasty after ARCADIA technique, leading to getting optimal luminal gain. The technique is safe and appropriate to treat eccentric calcified lesions of no-stenting zone as an optimal wire crossing method for lesion preparation before finalizing with DCB.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.