
Abstract
Purpose:
Although a majority of cervical artery dissections can be managed conservatively, patients presenting with cerebral embolization or significant stenosis require a more aggressive approach. However, complications associated with endovascular repair are quite frequent and optimal interventional technique still remains to be established.
Materials and methods:
The aim of this post hoc survey was to analyze results of endovascular treatments for symptomatic dissections of the internal carotid and vertebral arteries, which were performed under protection and with the use of double-layer mesh stents. During endovascular procedure catheters, stents and protection systems were tailored according to the angioarchitecture of dissection, particularly to its location, length and coexisting stenotic or aneurysmatic lesions. We evaluated retrospectively midterm and late results of endovascular treatment of 25 patients presenting with symptomatic dissection of cervical arteries, including 11 patients with dissections of intracranial segments of the internal carotid artery. Follow-ups were scheduled 1, 3 and 6 after the procedure, and then every 6 months. Control computed tomography (CT) or digital subtraction angiography (DSA) arteriographies were performed 1–6 months and 12 months after endovascular repair.
Results:
There were no periprocedural major adverse events. All patients completed the 12-month follow-up. There were neither fatalities nor new neurologic adverse events at the 30-day follow-up, and no such adverse events during long-term follow-up. At 12-month follow-up, in all patients, angiographies revealed patent stents, full coverage of lesions by stents and complete thrombotic closure of the pseudoaneurysms.
Conclusions:
A tailored endovascular management of symptomatic dissection of cervical arteries is safe and efficient, also in a long run.
Introduction
Dissection of arteries supplying the brain is a relatively rare disease. Spontaneous dissections occur in approximately 3 individuals out of 100,000 people per year.1–3 Dissections of iatrogenic and traumatic etiology are probably more frequent, especially given the increasing rates of diagnostic and therapeutic endovascular procedures performed through these arteries, although actual prevalence of these events in general population remains largely unknown. 4 Typically, cervical artery dissection is asymptomatic or presents with benign clinical course, but in about 10% to 20% of patients, particularly those younger than 45 years, can manifest with symptoms of cerebral ischemia. 5 Most common symptoms of the dissection of these arteries comprise cervical pain, headache and Horner’s syndrome. In a majority of patients, there is a remission after pharmacological treatment. Yet, those patients who do not improve after standard management and still present with the symptoms of cerebral ischemia represent a real clinical challenge. Invasive treatment of symptomatic cervical dissections is difficult, irrespective of the pathomechanism responsible (atherosclerosis, trauma, or iatrogenic), especially if a dissection is localized intracranially, or there is an aneurysmatic dilatation of the dissected artery. In the past, when endovascular procedures were not available, full neurological recovery was seen in a small percentage of such patients. 6 Nowadays, endovascular angioplasty and stenting is becoming a preferred method of treatments for symptomatic carotid dissections.1–3,5,7 In a large meta-analysis, endovascular management has been found to be more effective than open surgical repair, with acceptable frequency of serious adverse events.8–10 Still, the rate of periprocedural complications associated with the repair of these dissections is quite high (in a majority of centers it is at the level of 15% to 20%), as well as with a high incidence of severe restenoses in implanted stents.9–12
The aim of this post hoc survey was to analyze the midterm and late results of endovascular treatments for symptomatic dissections of the internal carotid and vertebral arteries, which were performed with the use of protection systems.
Materials and Methods
This survey is a continuation of the previously published paper, 13 in which we analyzed early and midterm results of endovascular management of dissections in the same cohort. In the current study, we analyzed the results of treatment of 25 consecutive patients (previously there were 16 patients) who were managed by our team from March 2015 to March 2020. Their mean age was 50.3±17.9 years; there were 9 female and 16 male patients. Spontaneous dissection occurred in 16 patients, traumatic in 8 patients, and in 1 case, the dissection was iatrogenic. Fifteen patients (60%) presented with stroke, 3 (12%) with transient cerebral ischemia and 7 patients (28%) with a headache or neck pain, in some cases coexisting with Horner’s syndrome. Clinical characteristics of the patients are given in Table 1.
Demographic and Clinical Characteristics of Patients.
Ultrasound examination of the carotid and vertebral arteries was used for screening purposes and was followed by computed tomography (CT) angiography to confirm the presence of lesions and to evaluate intracranial segments of the arteries. Indication and contraindication criteria for endovascular treatment are presented in Table 2. The decision on endovascular intervention instead of a standard conservative treatment was taken after multidisciplinary assessment, including neurological, neuroradiological and vascular consultations.
Indications and Contraindications for Endovascular Treatment of the Dissection.
Abbreviation: CT, computed tomography.
Details of the periprocedural management and endovascular technique were described in our previous paper. All endovascular procedures were performed by the same interventionalist who had a high expertise in the management of the extra- and intracranial arteries. All procedures were performed under protection. The choice of either proximal or distal protection depended on the morphology of dissection, and also on anatomical and functional angioarchitecture of cervical arteries, which was assessed pre- and intraprocedurally. As a proximal protection system, we used either the Mo.Ma Ultra 8F (Medtronic, Minneapolis, MN, USA) device or the Cello catheter (Covidien, ev3 Endovascular, Inc., Plymouth, MN, USA). Alternatively, we used distal protection filters, such as the SpiderFX™ Embolic Protection Device (Covidien, ev3 Endovascular, Inc., Plymouth, MN, USA) or the Emboshield® NAV6 TM Embolic Protection System (Abbott Vascular, Abbott Park, IL, USA). As stents, we primarily applied the RoadSaver™ stent (Terumo, Tokyo, Japan), which is a double-layer mesh, self-expanding and flow-diverter device. This type of stent was used in all patients. In 11 patients (44%), to address the entire lesion, it was necessary to implant an additional stent. For this purpose, in 1 patient we used the Carotid WallstentTM stent (Boston Scientific, Natick, MA, USA) and in 2 patients the Leo+Baby stents (Balt Extrusion, Montmorency, France). After gaining more expertise, we implanted exclusively the RoadSaver stents when more than one stent was needed (8 patients). Examples of symptomatic patients suffering from symptomatic dissections of the carotid artery and the vertebral artery who were managed endovascularly are shown in Figures 1 and 2.
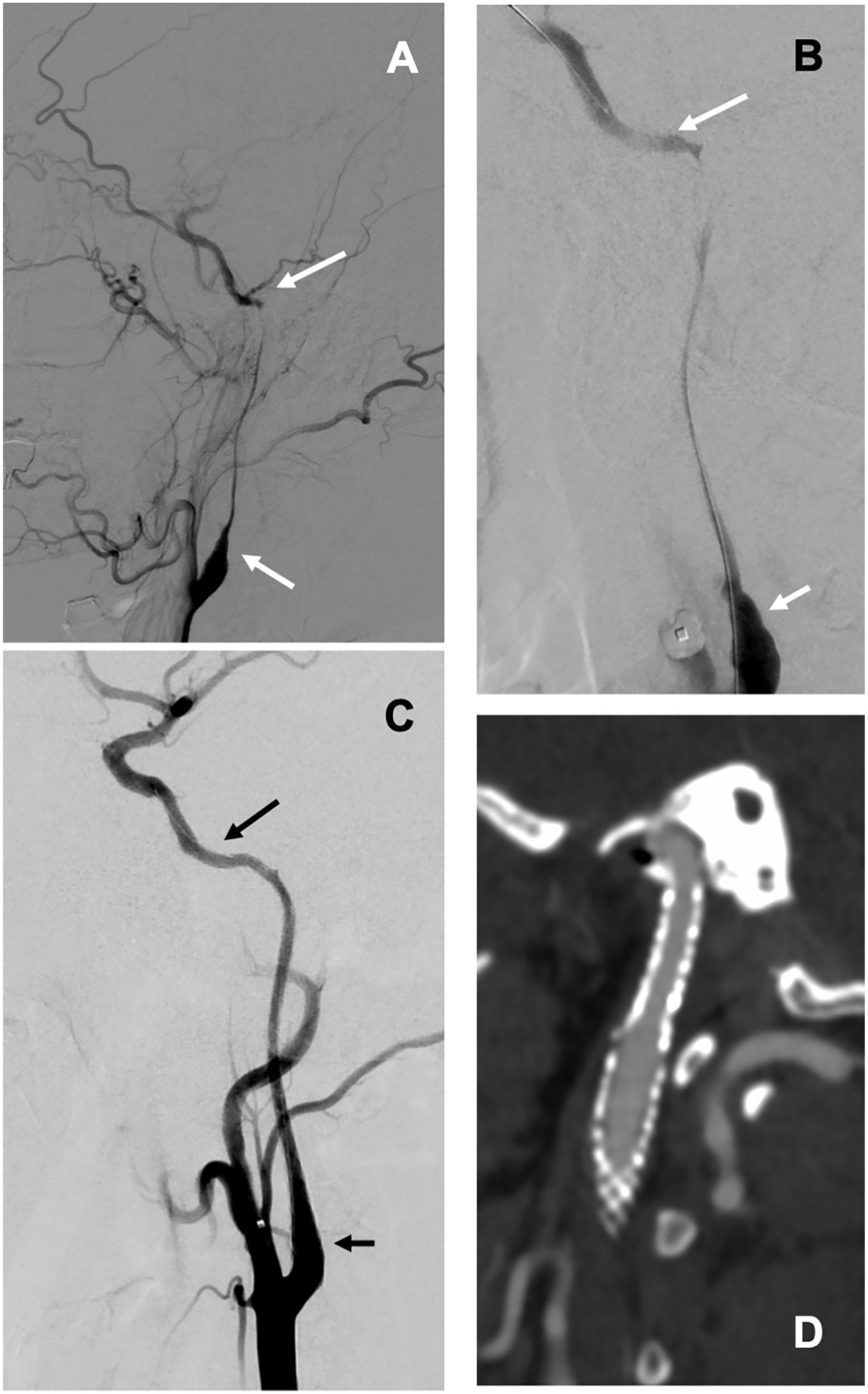
Patient with a long symptomatic dissection of the left internal carotid artery in C1-C2 segments. (A) Long dissection with critical stenosis (between the arrows) before the procedure. (B) Navigating through the lesion to the distal part of artery, balloon of the Mo.Ma system in the external carotid artery. (C) Result after implantation of 2 RoadSaver stents (between the arrows). (D) Control CT angiography at 12-month follow-up. CT, computed tomography.
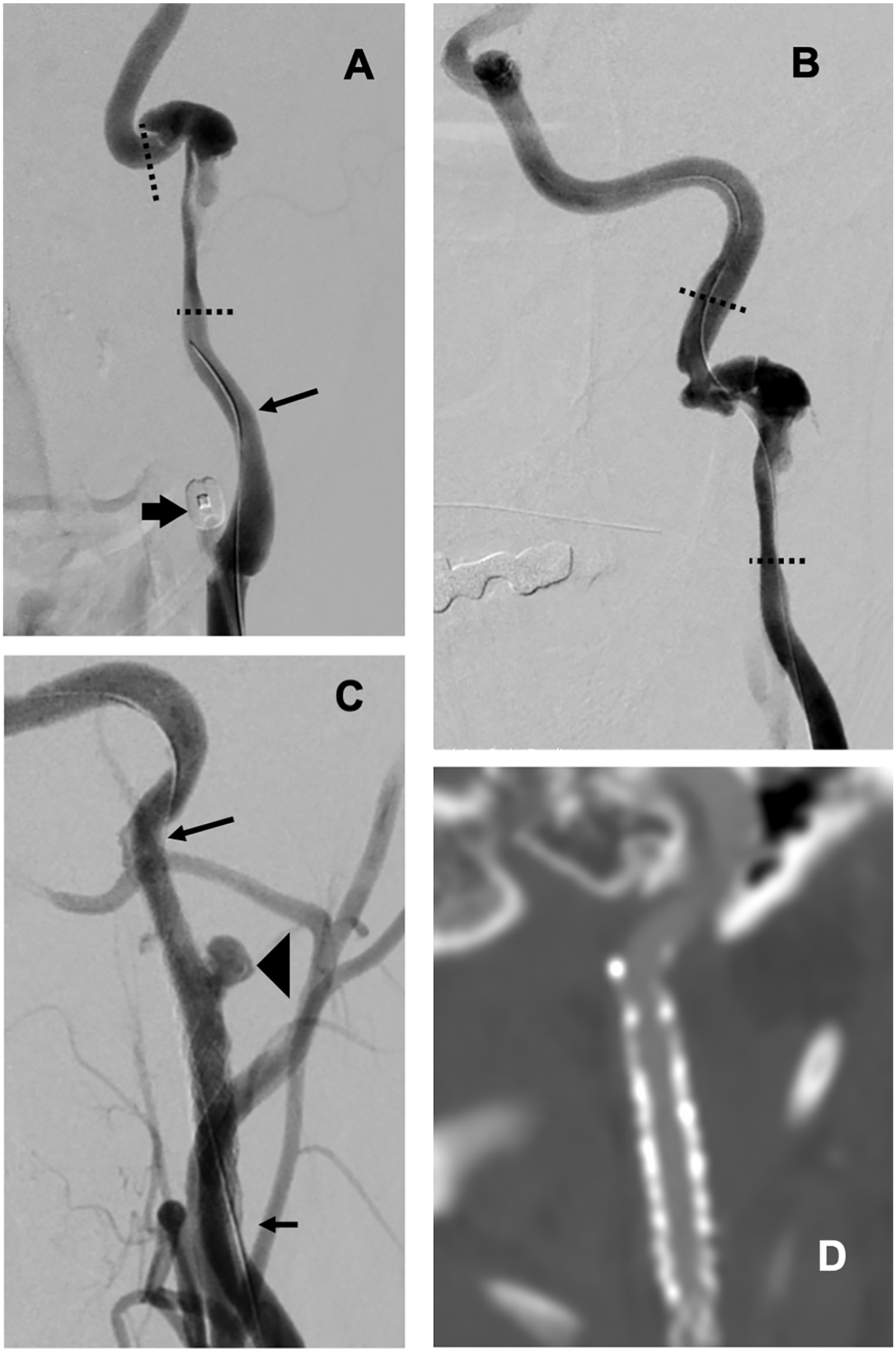
Patient with symptomatic dissection and pseudoaneurysm of the left internal carotid artery in C1/C2 segments. (A) Dissection with pseudoaneurysm between the dotted lines, arrow: beginning of the guide wire; thick arrow: balloon of the Mo.Ma system in the external carotid artery. (B) Successful navigating with guidewire to the distal part of the artery, dissection between the dotted lines. (C) Result after implantation of 2 RoadSaver stents (between the arrows), with normal flow to the intracranial part of the artery and a residual pseudoaneurysm (thick arrow). (D) Control CT angiography at 12-month follow-up, full coverage of the dissection and no pseudoaneurysm. CT, computed tomography.
For the assessment of midterm and late efficacy and safety of these endovascular procedures, follow-ups were scheduled 1, 3, 6, and then every 6 months. During these follow-ups, current neurological status was evaluated, as well as the history of any neurological event that occurred between them. Control CT or digital subtraction angiography (DSA) arteriographies were performed 1–6 months and about 12 months after endovascular repair. After hospital discharge, patients were recommended to take dual antiplatelet therapy (aspirin + clopidogrel or ticagrelor) at least for 3 months, optimally 6 months or longer. In patients presenting with long dissections, over 60 mm, they were recommended to take these agents for 12 months.
The study protocol has been approved by the Bioethical Committee of the Jagiellonian University in Krakow (approval no. 1072.6120.297.2018).
Results
Twenty-two patients presented with dissections of the internal carotid artery and 3 patients with the dissected vertebral artery. In 3 patients, dissection coexisted with an occlusion of the contralateral artery (the internal carotid artery in 2 patients and the vertebral artery in 1 patient). Degree of stenosis at the site of dissection ranged from 40% to 99% (mean ±SD 76.1±25.8%). Length of lesions varied from 13 to 106 mm (mean 47.1±30 mm). In 23 patients, the dissection was associated with aneurysmatic dilatation of the artery, with maximal diameter of such an aneurysm 3–18 mm (mean 8±3.8 mm). Eighteen patients (72%) were initially managed conservatively and the decision on endovascular repair was taken because of deteriorating clinical status. In 7 patients (28%), considering morphology of the lesion and overall clinical picture, endovascular repair was performed urgently, without previous pharmacological management. Details regarding localization and characteristics of dissections, degree of stenosis, as well as regarding endovascular armamentarium used, the duration of postprocedural antiplatelet therapy, and the duration of follow-up are given in Table 3. In all patients endovascular repair underwent uneventfully. There were no technical failures associated with these procedures. There were neither in-hospital deaths, new neurological deficits, nor other serious morbidities, except for neck pain that was seen in 2 patients (8%), in whom the stents were advanced to the C2 segment of the internal carotid artery. Of note, these pains were transient and had no further clinical consequences. Patients presenting with neurological deficits prior to the intervention improved after endovascular repair and this improvement was maintained at hospital discharge.
Localization and Characteristics of Dissections, Presence of Pseudoaneurysm (PsA), Endovascular Armamentarium Used, and Dual Antiplatelet Therapy (DAPT).
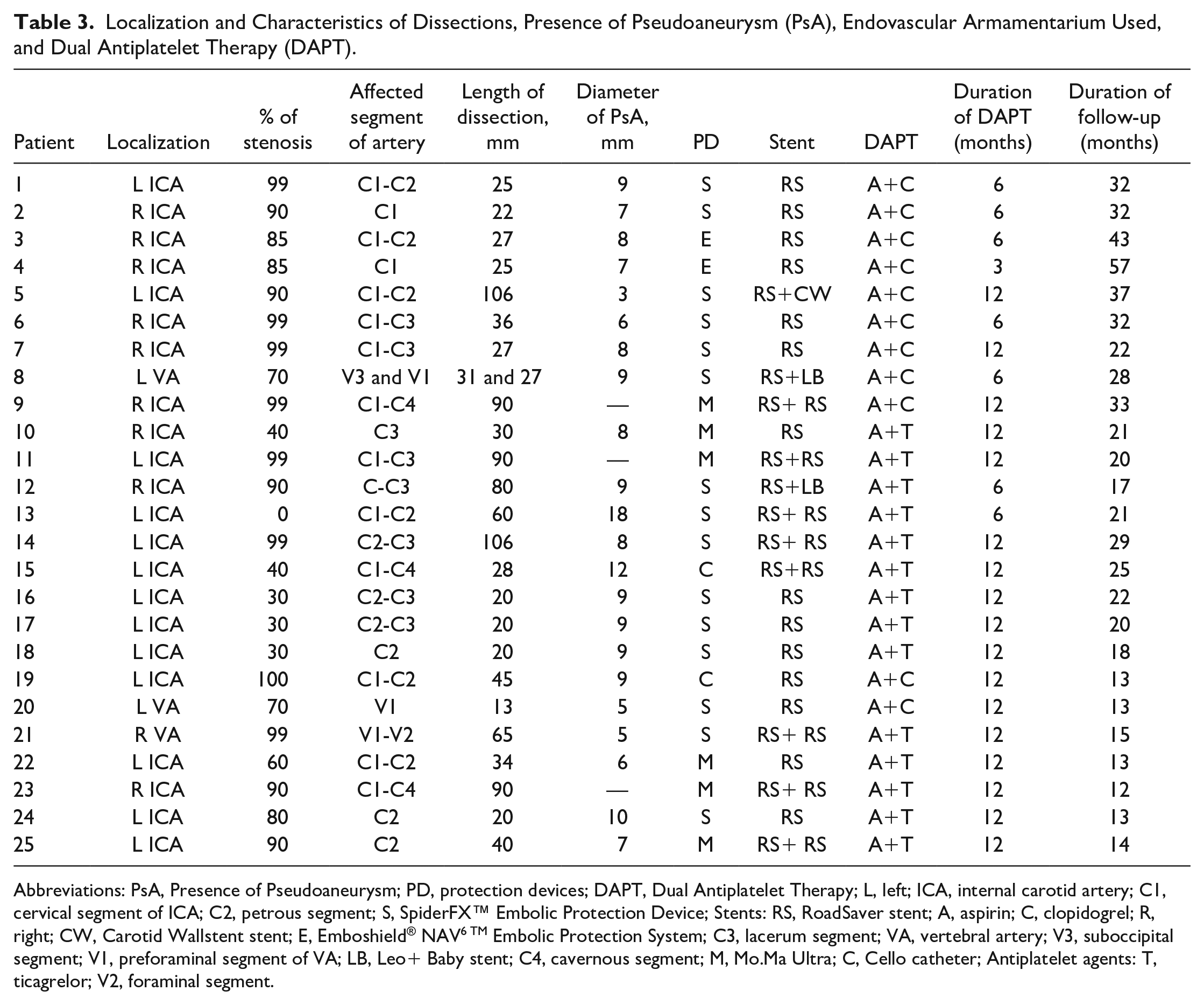
Abbreviations: PsA, Presence of Pseudoaneurysm; PD, protection devices; DAPT, Dual Antiplatelet Therapy; L, left; ICA, internal carotid artery; C1, cervical segment of ICA; C2, petrous segment; S, SpiderFX™ Embolic Protection Device; Stents: RS, RoadSaver stent; A, aspirin; C, clopidogrel; R, right; CW, Carotid Wallstent stent; E, Emboshield® NAV6 TM Embolic Protection System; C3, lacerum segment; VA, vertebral artery; V3, suboccipital segment; V1, preforaminal segment of VA; LB, Leo+ Baby stent; C4, cavernous segment; M, Mo.Ma Ultra; C, Cello catheter; Antiplatelet agents: T, ticagrelor; V2, foraminal segment.
All patients completed the 12-month follow-up. Duration of the long-term follow-up ranged from 12 to 56 months (median 22 months), as given in Table 3. There were no new neurological events at the 30-day follow-up (incidence rate = 0%). There were neither fatalities nor new neurologic adverse events during long-term follow-up. In all patients, control angiographies revealed patent stents, without significant stenosis (1 patient presented with mild degree 30%–40% stenosis) and without relevant pathology regarding cerebral arteries. In addition, in all cases, these angiographies demonstrated a full coverage of the lesions by stents and complete thrombotic closure of the pseudoaneurysm (effect of the flow-diverter stent). In 2 patients, who were managed with 2 stents, control angiographies demonstrated that the segment, in which the stents overlapped, has shortened, still without clinical consequences.
Discussion
It should be emphasized that this study was performed in the tertiary vascular center, dedicated to the management of highly selected patients presenting with pathologies of the cerebral blood vessels, thus the results of our study should not be extrapolated to typical patients with cervical arteries dissections. The results of this survey confirm that in selected group of patients (see Table 2), an endovascular repair of dissections of the carotid and vertebral arteries under protection, which is tailored to the regional angioarchitecture, with the use of new-generation stents and with a long-term postprocedural antiplatelet therapy is safe, also in the long run. Of note, in our survey, there were no patients presenting with the common carotid artery dissection, although such dissections are more prevalent than those of the internal carotid and vertebral arteries. Still, a majority of the common carotid artery dissections are clinically mild and require conservative treatment only. Similarly, in the recently published German multicenter trial, there were no patients requiring intravascular intervention if a dissection affected the common carotid artery. 14
Yet, it should be emphasized that conservative management of patients suffering from cervical artery dissections with antiplatelet and antithrombotic agents still remains the first-line modality of the treatment, and that invasive procedures should be performed in selected cases only, when pharmacological therapy is ineffective.15–17 It should be acknowledged, however, that recommendations on the management of cervical arteries dissection were published several years ago. 18 At that time stents and medications that currently can be used by interventionalists were not available. A more recent meta-analysis suggests a higher efficacy of the endovascular management in comparison with conservative treatment, although safety of these procedures still remains the issue. 19
In the CADISS study, which was a randomized clinical trial comparing conservative treatment for cervical artery dissections with the use of either antiplatelet agents or anticoagulants, the risk of recurrent stroke at 1 year was low: 2.5%. 9 Yet, this study did not include patients presenting with intracranial dissection, where the risk of serious neurological events is thought to be much higher in comparison with the lesions localized extracranially. In our survey, 10 patients (40%) presented with intracranial dissections (i.e., affecting the lacerum or more distal segments of the internal carotid artery). Thus, the results of the CADISS study cannot be easily extrapolated to our patient cohort.
Periprocedural cerebral embolism and reocclusion of implanted stents represent 2 main problems associated with endovascular procedures for dissections of the carotid and vertebral arteries. The use of protection devices during the procedure and implantation of a new-generation stents can theoretically minimize the rate of these serious adverse events, and our study was aimed at addressing this issue. Currently, available evidence regarding endovascular management for the dissections of cervical arteries is highly heterogeneous.10,12,20 Published studies reported the use of very different stent types; they were characterized by different stent designs, profile of the delivery system, size of the stent cells, radial force, and stiffness. Also frequency of the use of flow-diverter stents varied between the studies. Importantly, reocclusion rates of implanted stents were high, in some studies even as high as 12%.8,21–23 In addition, the use of protection systems during these endovascular procedures was reported by a minority of papers and almost always the filters were used. 23 However, in these studies the use of distal protection systems was not associated with clinically overt periprocedural cerebral embolism. 23 Besides, duration of postprocedural antiplatelet therapy varied between the studies.
By contrast to the above-discussed studies, all our patients were managed under protection and in all of them new-generation flow-diverter stents were implanted. There was no periprocedural cerebral embolism in our patient cohort, which contrasts with the published studies.8,21,23 We believe that good results concerning this clinically relevant complication were related to the mandatory, still tailored, use of protection system during the endovascular repair. Although in a majority of our patients, the diagnostics for cerebral embolism comprised clinical assessment and periprocedural angiography, and in some patients it was augmented by DW-MRI, which further confirmed safety of the procedure performed with the use of protection system. In our center, proximal protection is preferred. Proximal protection devices, such as the Mo.Ma or the Cello, allow for a shielding of the brain before navigating through the dissected artery with the wires and catheters.24–26 This is very important, considering the fact that endovascular repair of the dissection is performed in patients who are at a high risk of additional cerebral ischemia during the procedure. In addition, through the Mo.Ma or the Cello system it is possible to perform aspiration thrombectomy from the most distal segments of the internal carotid artery, which was actually done in one of our patients. Yet, proximal protection cannot be used in every patient and in this series it was possible in 8 cases (32%).
There are 2 main technical issues associated with the stenting of distally located cervical dissections (C2-C4 and V2-V3). The first one is related to the tortuosity of these segments of cervical arteries, which makes introduction of many types of stents challenging. The second issue regards a common presence of aneurysmatic dilatation at the site of dissection. In such a case the stent should exclude the aneurysm from circulation. Old-generation closed-cell stents, with small stent cells, can potentially play a role of flow-diverter stents, yet they are stiff, which usually makes their implantation impossible. On the contrary, open-cell stents are easier to navigate and deploy, but because of the large stent cells they cannot exclude the outer aneurysmatic part of the dissected artery from the circulation. Besides, thrombotic material from the pseudoaneurysm can migrate through the struts of these stents and evoke cerebral embolization. Stents that are dedicated to the intracranial lesions (such as the Leo+ Baby stents) are safe and efficient in a case of pseudoaneurysm, but because of a low radial force cannot be used in dissections accompanied by local stenosis. In our material, such stents were used in 2 patients only. One of these patients presented with the dissection of the suboccipital segment of the vertebral artery (V3), which was not accompanied by stenosis. Another patient had the dissection in the petrous segment of the internal carotid artery (C2) and the decision on the use of such a stent was related to the very tortuous course of the extracranial part of the artery. Yet, considering our current expertise, it would be possible to manage this patient exclusively with the double-layer mesh stents, if special intracranial catheters were used.
It seems that the so-called double-layer mesh stents can address both challenging technical problems. These stents are low-profile and highly elastic devices, therefore can be navigated to the distal segments of the vertebral and internal carotid arteries. 27 Also, thanks to the special design of stent cells, these stents behave as the flow-diverter devices and can exclude aneurysmatic dilatations of the dissected artery from circulation. Besides, these stents are characterized by a quite high radial force, hence can be implanted in a case of stenosis. Theoretically, this property should be associated with low reocclusion rates of such stents and this has been confirmed in our survey.
There is, however, a unique property of the RoadSaver double-layer mesh stents that makes their implantation challenging. The final length of this stent depends on caliber of the target artery; the wider the blood vessel, the shorter the stent. In 2 of our patients presenting with carotid dissection coexisting with a significant stenosis, who had implanted 2 overlapping RoadSaver stents, control angiography revealed dilatation of the target artery and shortening of the overlapping segment, which initially had about 1 cm. Therefore, in such patients, a possible shortening of the overlap should be taken into account while planning the proper positioning and length of the stents.
A long duration of postprocedural antiplatelet therapy is potentially another source of our success. We recommended long-term administration of antiplatelet agents in such patients: 6 months in the case of short dissections and 12 months if dissections were longer than 60 mm. Also, currently we prefer ticagrelor over clopidogrel (Table 3), which possibly accounts for a lower risk of in-stent stenosis. Except for 2 patients, in whom ticagrelor caused mild bleeding and needed to be changed to clopidogrel, this new-generation antiplatelet agent was well tolerated.
We acknowledge that there are some weak points in our study. It was a retrospective analysis of patient cohort and not a prospective randomized trial. Moreover, the number of treated patients was relatively small. Still, for ethical reasons, it would be impossible to perform a typical randomized clinical trial in this particular group of patients, especially because cervical artery dissections requiring invasive treatment are rare. A majority of patients suffering from such dissections should be managed conservatively and the results of pharmacological treatment are good. Therefore, in order to assess results of the treatment for such an uncommon clinical entity as dissection of the carotid or vertebral artery requiring stenting, evaluation of patient cohort and comparing the results of such a retrospective evaluation to the already published studies that have utilized different endovascular strategies 7,9,10,14,16–19,23 seems reasonable. In our group of patients, endovascular treatment for cervical dissections in all cases underwent uneventfully. Also, there were no serious mid- and long-term events, such as strokes or in-stent occlusions.
Conclusions
The results of our survey indicate that selected patients with cervical artery dissection, especially those presenting with symptomatic intracranial dissections coexisting with pseudoaneurysms, can be safely managed endovascularly, on condition that the procedure is performed under protection, double-layer mesh flow-diverter stents are implanted, and there is a long postprocedural antiplatelet therapy.
Footnotes
Author Note
Bartlomiej Lasocha is now affiliated to Diagnostic Imaging Unit, University Hospital, Krakow, Poland.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.