
Abstract
Purpose:
The current study sought to investigate the impact of cardiac condition on loss of patency after endovascular therapy (EVT) using new-generation devices for femoropopliteal (FP) lesions.
Materials and Methods:
We retrospectively studied 547 lesions (chronic limb-threatening ischemia: 44%, TASC II C/D lesion: 61%, chronic total occlusion: 37%, in-stent restenosis: 13%, involving popliteal arterial lesion: 45%) belonging to 416 patients (average age: 75±9 years, male: 69%, diabetes mellitus: 62%, hemodialysis: 33%) who underwent EVT with new-generation FP-specific devices (polymer-free paclitaxel-eluting stent, n=186; stent graft, n=119; fluoropolymer-based paclitaxel-eluting stent, n=29; interwoven stent, n=17; drug-coated balloon, n=196) from June 2012 to May 2019. Cardiac function was evaluated using echocardiography. The primary outcome measure was primary patency, which was defined as free from peak systolic velocity ratio (PSVR) >2.5 assessed by duplex ultrasound. Predictors for loss of patency were evaluated using Cox proportional hazards regression analysis.
Results:
Overall 12 primary patency were 80.0±1.8%. After the multivariate analysis, reduced stroke volume evaluated by echocardiography (hazard ratio [HR]=0.99, 95% confidence interval [CI]=0.97-0.99, p=0.03), chronic heart failure (HR=1.76, 95% CI=1.05-2.97, p=0.03), and a smaller distal reference vessel diameter (HR=0.73, 95% CI=0.55-0.97, p=0.03) were significantly associated with loss of 12-month primary patency, whereas lesion length (HR=1.01, 95% CI=0.99–1.03, p=0.33) and presence of chronic total occlusion (CTO; HR=0.92, 95% CI=0.61-1.40, p=0.70) were not statistically significant.
Conclusion:
The current study revealed that cardiac function represented by reduced stroke volume and presence of chronic heart failure as well as a smaller distal reference vessel diameter were significantly associated with loss of 12-month primary patency in patients with peripheral artery disease (PAD) presenting FP lesions endovascularly treated with new-generation devices.
Introduction
Patients with peripheral artery disease (PAD) have poor prognosis in general due to a high cardiovascular morbidity and mortality rate.1,2 Cardiac conditions, whether symptomatic or asymptomatic, adversely affect systemic and lower limb clinical outcomes. The presence of impaired cardiac function (CF) has also been reported as a significant risk factor for diminished patency after femoropopliteal (FP) revascularization in patients with PAD,3,4 speculated to be due to hemodynamic and physiological alterations that include a low-flow state, endothelial cell dysfunction, and vascular smooth muscle cell dysfunction.5–7
Currently, new-generation FP-specific devices, including drug-coated balloon (DCB), drug-coated stent (DES), drug-eluting stent, interwoven bare nitinol stent, and stent graft, have emerged and these have shown better durability than conventional therapy using plain balloon angioplasty or bare nitinol stent and have been widely applied to clinical FP practice.8–10 However, the correlation of CF to loss of patency after endovascular therapy (EVT) using these devices has not been systematically studied. We hypothesized that parameters representing a low-flow CF state would be associated with an increased risk for reduced patency after EVT. The aim of the current study was to reveal the impact of CF on loss of patency in PAD patients with FP lesions treated with new-generation FP-specific devices.
Materials and Methods
Study Participants
The current study was a single center, retrospective analysis including patients presenting FP lesions who primarily underwent EVT with new-generation FP-specific devices from June 2012 to May 2019. During this study period, 2453 lesions in 1658 patients were successfully treated with EVT. Patients treated without new-generation devices (noncoated balloon angioplasty, n=617; bare metal stent, n=397) were excluded from study population. Of these remaining treated with new-generation FP-specific devices, patients complicated with the common femoral artery (n=26) or anastomosis of FP bypass (n=3), having a distal reference vessel diameter smaller than 4 cm because of no indication for new-generation FP-specific devices under instruction for use (n=13), having severe mitral or aortic valve disease because valve disease potentially leads to the overestimation of cardiac function (n=18), or having incomplete data regarding cardiac function (n=168) were excluded from current analysis. We finally analyzed a total of 547 lesions in 416 patients (Figure 1). Polymer-free paclitaxel-eluting stent, stent graft, fluoropolymer-based paclitaxel-eluting stent, interwoven bare nitinol stent, and drug-coated balloon were used in 186, 119, 29, 17, and 196 lesions, respectively. Demographic data and medical comorbidities were obtained. The CF status was assessed using transthoracic echocardiography. Each parameter, including left ventricular ejection fraction (LVEF) and stroke volume (SV) for measures, was assessed prior to the index procedure and all FP-EVT was conducted before completion of any cardiac intervention based on our hospital manner. The current study was performed in accordance with the Declaration of Helsinki and was approved by the ethics committee of the hospital. The current analysis involved observational research without intervention or invasiveness and did not use human biological specimens, and the study was therefore considered exempt from the need for written informed consent from patients in accordance with the Ethical Guidelines for Medical and Health Research Involving Human Subjects in Japan. Instead, relevant information regarding the study was made available to the public and opportunities for individuals to refuse inclusion of their data were ensured.
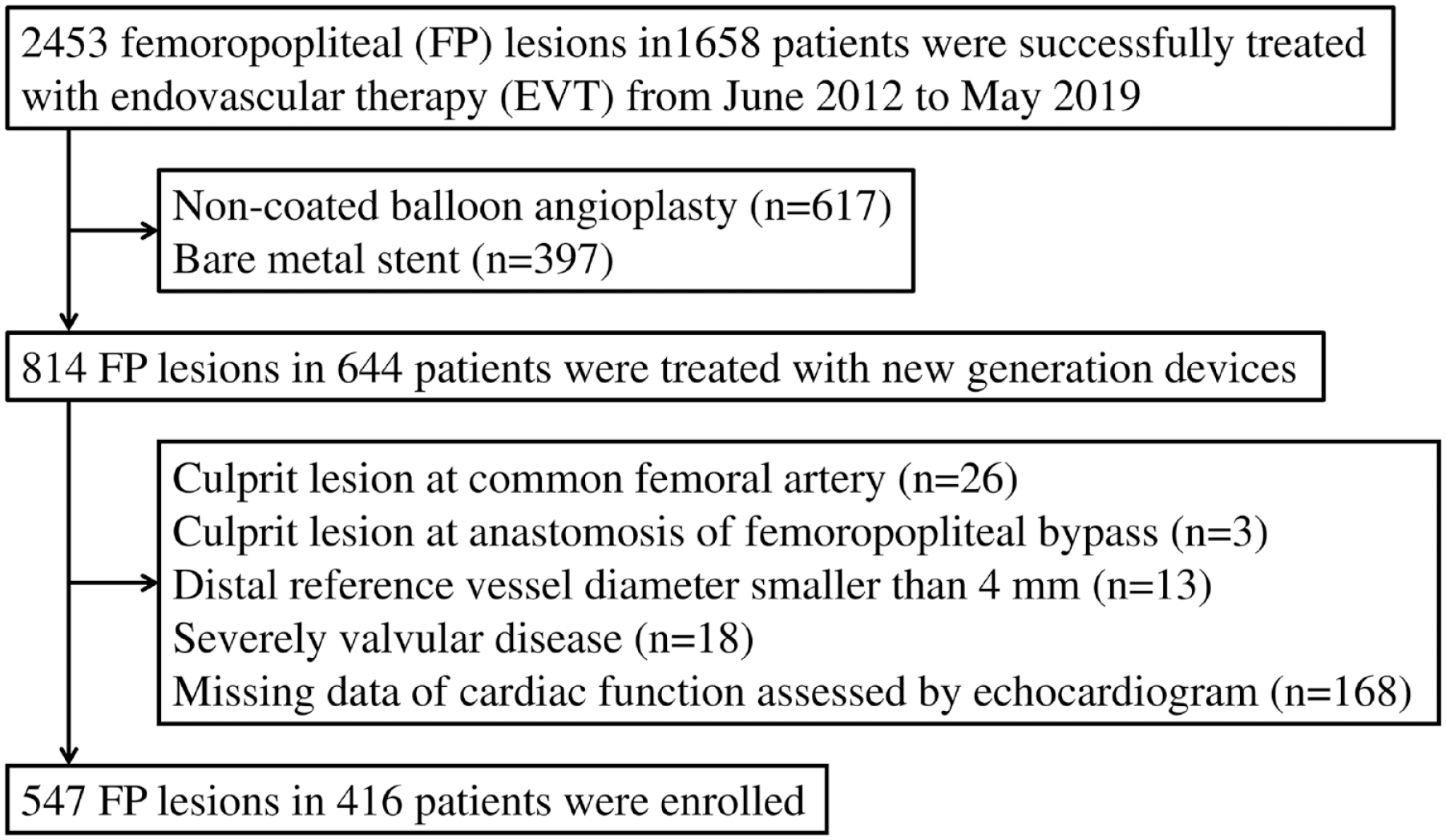
Study profile. A total of 547 lesions in 416 patients who primarily underwent EVT with new-generation FP-specific devices from June 2012 to May 2019 were analyzed. EVT, endovascular therapy; FP, femoropopliteal.
Intervention Procedure
The severity of ischemia in the index limb was routinely evaluated using the ankle-brachial index (ABI). Lesion location and severity were generally evaluated using duplex ultrasound and the presence of significant arterial lesions was diagnosed using digital subtraction angiography (DSA) before EVT. Revascularization was indicated for lesions with stenosis angiographically measuring 75% or greater of the vessel diameter, which was hemodynamically significant. The EVT strategy was determined according to generally accepted principles. The EVT was performed under local anesthesia via a contralateral or ipsilateral antegrade common femoral artery approach using 6Fr or 7Fr sheaths. After successful wire crossing, intravascular ultrasound (IVUS) was used at the operator’s discretion and preballoon dilation was generally performed. Selection of treatment modality (polymer-free paclitaxel-eluting stent, stent graft, fluoropolymer-based paclitaxel-eluting stent, interwoven bare nitinol stent, or drug-coated balloon) was based on clinical examination, anatomic evaluation, and physician’s discretion. Drug-coated balloons were used with inflation times with at least 3 minutes. In case treated with stent implantation, postballoon dilation was routinely performed according to the same size to the vessel diameter after stent implantation. After the procedure, patients continued to receive 75 mg of clopidogrel or 3.75 mg of prasugrel daily. Patients also received aspirin (100 mg) or another equivalent anticoagulation drug. Duration and type of dual antiplatelet therapy were kept by the instructions for use. Duration of dual antiplatelet therapy was as follows: Drug-coated balloon was for at least a month, polymer-free paclitaxel-eluting stent and fluoropolymer-based paclitaxel-eluting stent were for at least 2 to 3 months, and stent graft were for at least 6 months. Prolonged duration of dual antiplatelet therapy in each case was determined by physician’s discretion.
Follow-Up Protocol
Ankle-brachial indexes (ABIs), duplex ultrasound, or both were obtained before intervention. All patients were followed at 1, 3, and 6 months after revascularization, and thereafter every 3 months. Loss of primary patency was determined using established guidelines and as previously reported.11,12 Duplex criteria for patency loss included a peak systolic velocity ratio elevation >2.5 in the treated segment relative to the immediately proximal arterial segment, or evidence of occlusion. Patients were also determined to have patency loss by angiography following recurrence of clinical symptoms or reduction in ABI or duplex ultrasound according to established guidelines. 11 Hemodynamic and clinical success was defined in accordance with accepted reporting criteria. 11
Evaluation for Cardiac Functions
Transthoracic echocardiography examinations were performed routinely before revascularization. Examinations for cardiac function (CF) evaluated by echocardiogram were performed using EPIQ 7 (Philips North America Co, Cambridge, MA) or Vivid E9 (General Electric Co, Boston, MA) ultrasound system. Echocardiographic studies were performed in accordance with American Society of Echocardiography (ASE) guidelines. 12 The LVEF and SV were measured by either the Teichholz or modified Simpson method. Data on cardiac chamber size and function, including left atrial diameter, left ventricular end-diastolic diameter, and left ventricular end-systolic diameter, were also evaluated.
Outcome Measure
The primary outcome measure was primary patency. The secondary outcome measure was (1) all-cause death; (2) major adverse cardiovascular events (MACEs) defined as acute myocardial infarction, stroke, and cardiovascular death; (3) major adverse limb events (MALEs) defined as major amputation and any reintervention; and (4) hospitalization due to heart failure.
Definitions
Chronic heart failure (CHF) was defined as the past history of hospitalization due to heart failure or previously diagnosed as CHF according to the Framingham criteria. 13 Severity of lesion calcification was assessed by Peripheral Arterial Calcium Scoring System (PACSS) and classified into 5 groups as follows: no visible calcium at the target lesion site (PACSS grade 0), unilateral calcification<5 cm (PACSS grade 1), unilateral calcification≥5 cm (PACSS grade 2), bilateral calcification<5 cm (PACSS grade 3), and bilateral calcification≥5 cm (PACSS grade 4). 14
Statistical Analysis
Unless mentioned otherwise, data were presented as mean ± standard deviation (SD) for continuous variables and as frequency (percentage) for discrete variables. Prognostic outcomes were assessed with the Kaplan-Meier method and the differences between groups were assessed with the log-rank test when necessary. Cox proportional hazard regression analysis was used to determine the association of clinical characteristics, including CF with 1-year loss of patency. Clinically specified predictors achieving p<0.05 in univariate analysis were entered the multivariate Cox regression analysis. The hazard ratio (HR) and 95% confidence interval (CI) were reported. A p value<0.05 was considered statistically significant.
Statistical analyses were performed using SPSS Version 24.0J (SPSS Inc, Chicago, Illinois).
Results
Baseline Characteristics
The baseline characteristics are summarized in Table 1. Two hundred eighty-four (69%) patients were male. The mean age was 75 ± 9 years old. Notable comorbidities included diabetes mellitus (62%, n=254), dialysis (33%, n=134), coronary artery disease (62%, n=257), and CHF (14%, n=58). Chronic limb-threatening ischemia (CLTI) was observed in 44% (n=182). Regarding baseline CF characteristics evaluated by echocardiography, average LVEF and average SV were 62±12 % and 60±19 mL, respectively. Baseline lesion characteristics and intervention procedure are shown in Table 2. Of 547 lesions undergoing EVT, TASC II C/D lesion in 61% (n=333) and lesion involving a popliteal lesion in 45% (n=243). Mean lesion length and distal reference vessel diameter were 19±11 cm and 5.9±1.0 mm, respectively. The PACSS classification grade 4 was noted in 23% (n=123) of the study population. Regarding device use, paclitaxel-based devices were mainly used in three-fourths of the population. The remaining 25% of population were treated with stent graft use (22%, n=119) and interwoven stent (3%, n=17).
Baseline Patient Characteristics.
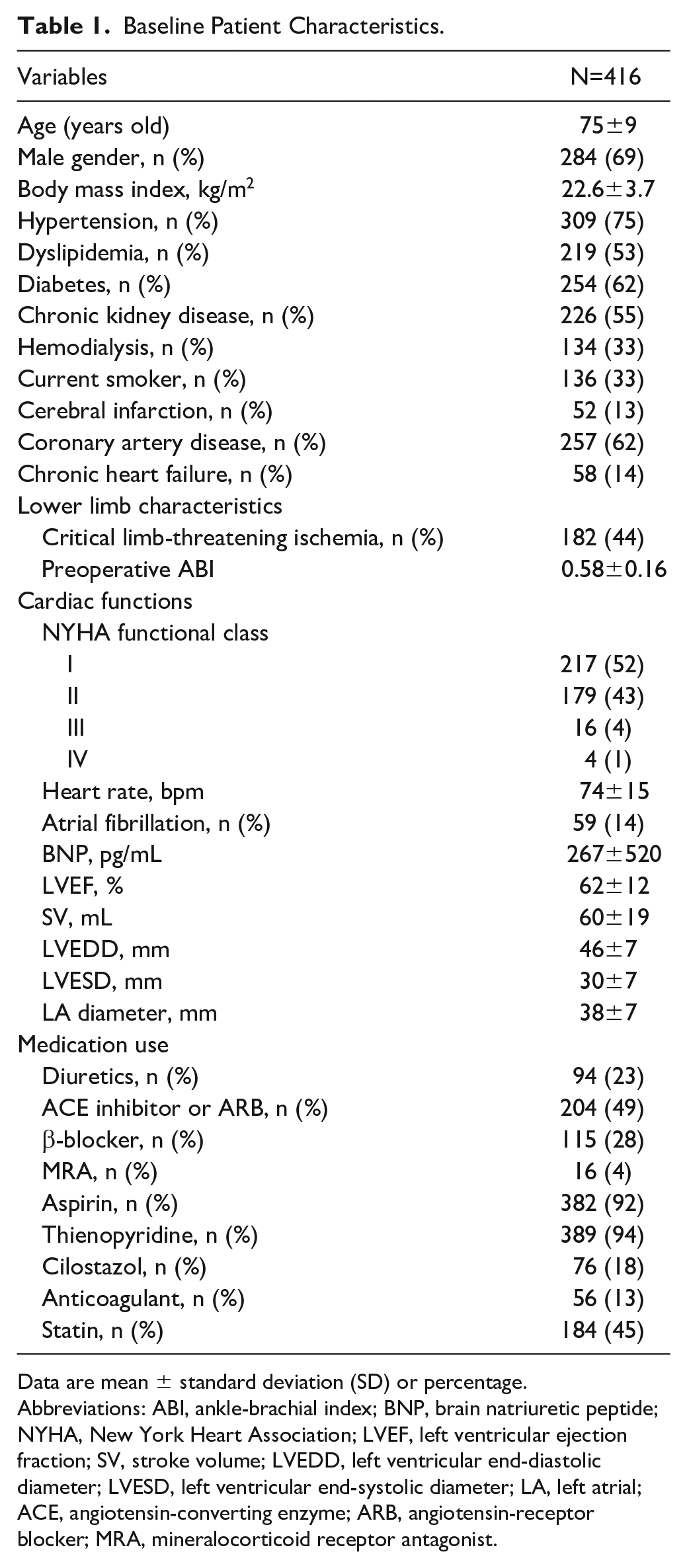
Data are mean ± standard deviation (SD) or percentage.
Abbreviations: ABI, ankle-brachial index; BNP, brain natriuretic peptide; NYHA, New York Heart Association; LVEF, left ventricular ejection fraction; SV, stroke volume; LVEDD, left ventricular end-diastolic diameter; LVESD, left ventricular end-systolic diameter; LA, left atrial; ACE, angiotensin-converting enzyme; ARB, angiotensin-receptor blocker; MRA, mineralocorticoid receptor antagonist.
Baseline Lesion and Procedural Characteristics.
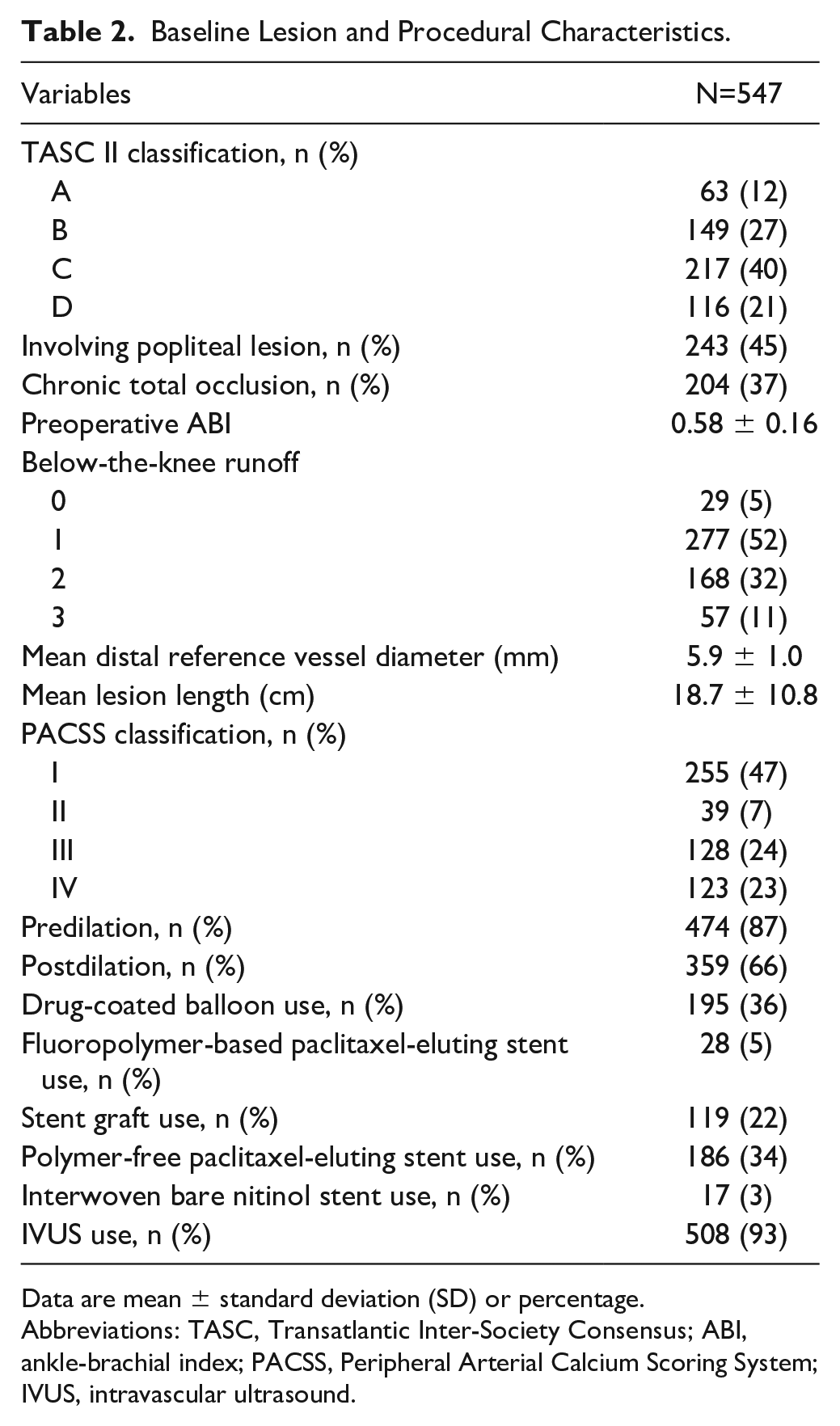
Data are mean ± standard deviation (SD) or percentage.
Abbreviations: TASC, Transatlantic Inter-Society Consensus; ABI, ankle-brachial index; PACSS, Peripheral Arterial Calcium Scoring System; IVUS, intravascular ultrasound.
Predictors for Loss of 12-Month Primary Patency
Data of overall primary patency at 12±2 and 24±2 months were available for 441 (81%) and 395 lesions (72%). Overall primary patency at 12 and 24 months was estimated to have occurred in 80.0±1.8% and 69.0±2.2 %, respectively (Figure 2, Supplemental Figure 1). Univariate analysis revealed that female gender (HR=1.77, 95% CI=1.18-2.64, p<0.01), CLTI (HR=2.02, 95% CI=1.35-3.02, p<0.01), CHF (HR=1.73, 95% CI=1.06-2.82, p=0.03), involving a popliteal lesion (HR=1.81, 95% CI=1.21-2.70, p<0.01), distal reference vessel diameter (HR=0.62, 95% CI=0.47-0.83, p<0.01), stent graft use (HR=0.51, 95% CI=0.29-0.92, p=0.03), polymer-free paclitaxel-eluting stent use (HR=1.53, 95% CI=1.03-2.29, p=0.04), and SV (HR=0.98, 95% CI=0.97-0.99, p<0.01) were significantly associated with a loss of 12-month primary patency. After multivariate analysis, reduced SV evaluated by echocardiography (HR=0.99, 95% CI=0.97-0.99, p=0.03) and CHF (HR=1.76, 95% CI=1.05–2.97, p=0.03) and a smaller distal reference vessel diameter (HR=0.73, 95% CI=0.55–0.97, p=0.03) remained as a significantly independent predictor associated with loss of primary patency as shown in Table 3. The 12-month primary patency stratified by its median value of SV was higher in the SV≥58.1 cm/s group than in the SV<58.1 cm/s group (86.6±2.2% vs 73.4±2.9%, p<0.01, Figure 3). Supplemental Figure 1 shows that 2-year primary patency was also higher in the SV>58.1 cm/s group than in the SV<58.1 cm/s group (75.7±2.8% versus 62.3±3.3%, p<0.01).
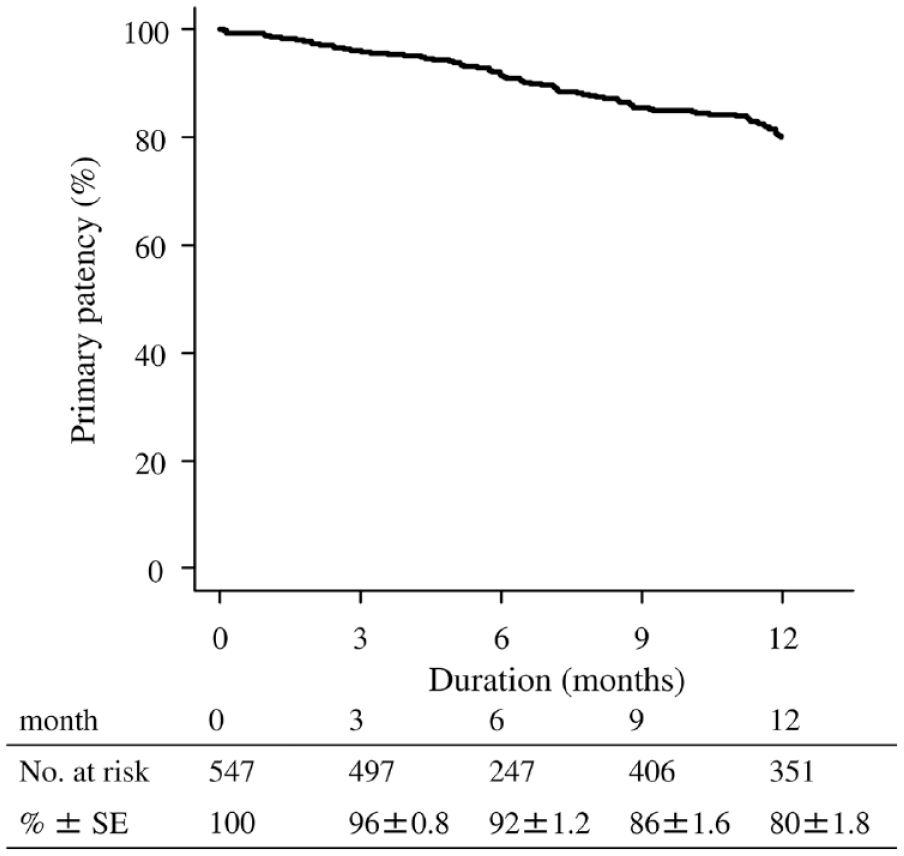
Overall 12-month primary patency after new-generation FP-specific devices implantation. Overall 12-month primary patency after new-generation FP-specific devices implantation was 80.0 ± 1.8%. FP, femoropopliteal.
Univariate and Multivariate Analysis for Loss of Patency.
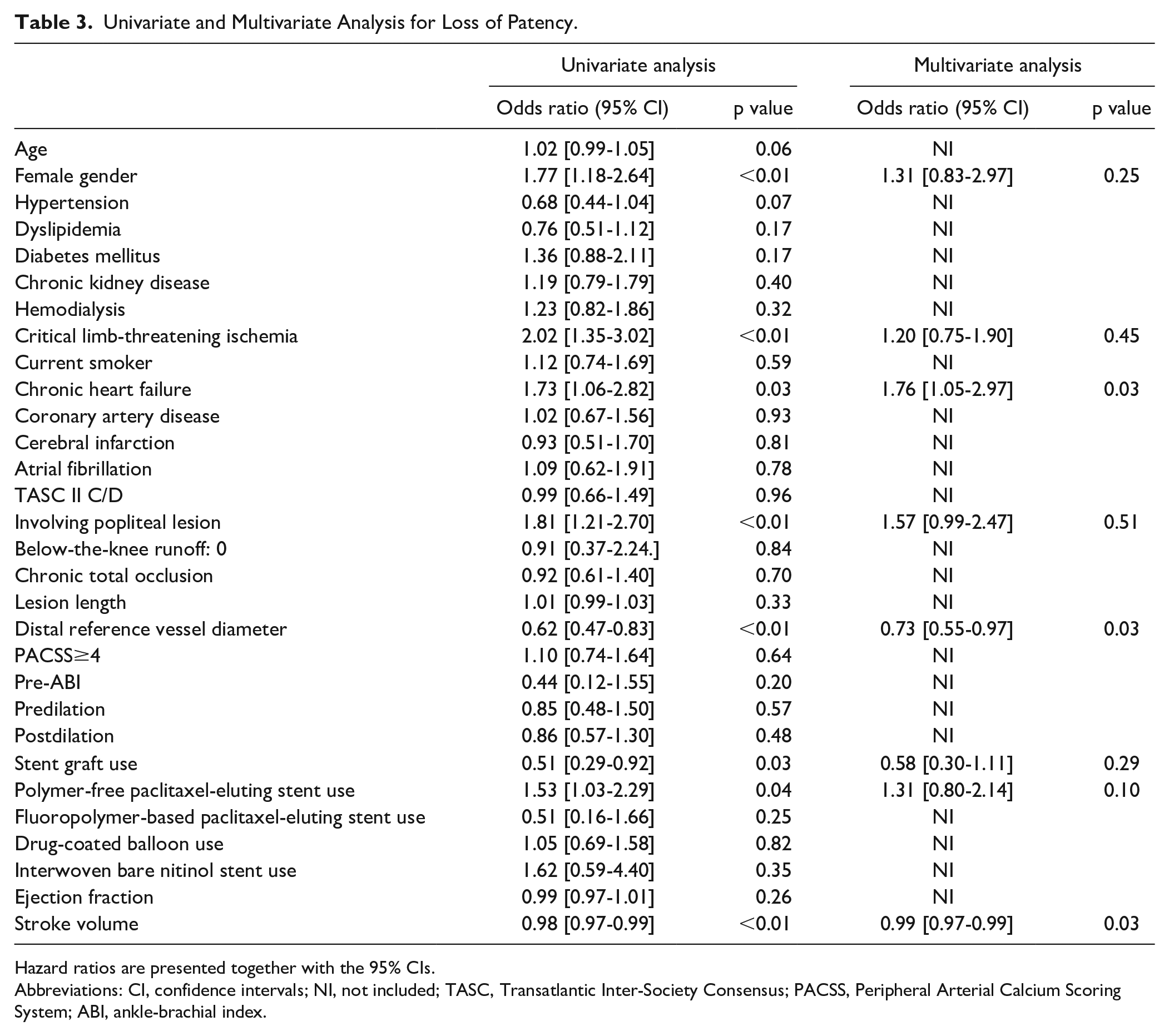
Hazard ratios are presented together with the 95% CIs.
Abbreviations: CI, confidence intervals; NI, not included; TASC, Transatlantic Inter-Society Consensus; PACSS, Peripheral Arterial Calcium Scoring System; ABI, ankle-brachial index.
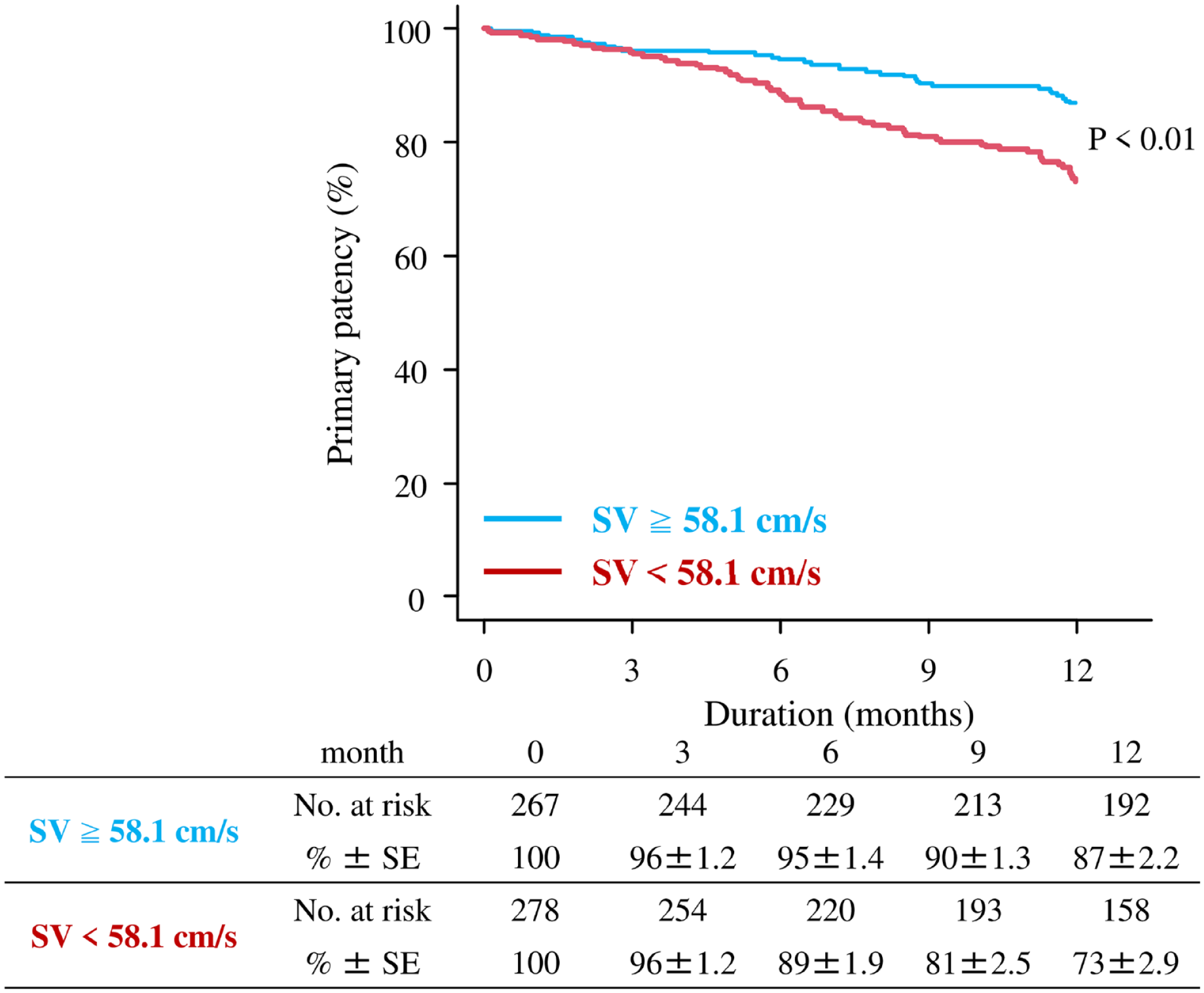
Twelve-month primary patency stratified by its median value of SV. Twelve-month primary patency was significantly lower in the SV<58.1 cm/s group than in the SV≥58.1 cm/s group (p<0.01). SV, stroke volume.
Secondary Outcome Measure
Twelve-month MALE occurred in 25 patients in the SV<58.1 cm/s group and in 17 patients in the SV≥58.1 cm/s group; the Kaplan-Meier estimates of the incidence at 12 months were numerically higher in the SV<58.1 cm/s group, although not statistically different (14.5±2.7% vs 8.9±2.1%, p=0.10). Twelve-month all-cause mortality was significantly higher in the SV<58.1 cm/s group (10.8±2.3% vs 4.7±1.5%, p=0.03), whereas the incidences of cardiovascular death, myocardial infarction, ischemic stroke, and major amputation were not significantly different between the 2 groups (Table 4).
Outcome Measure.
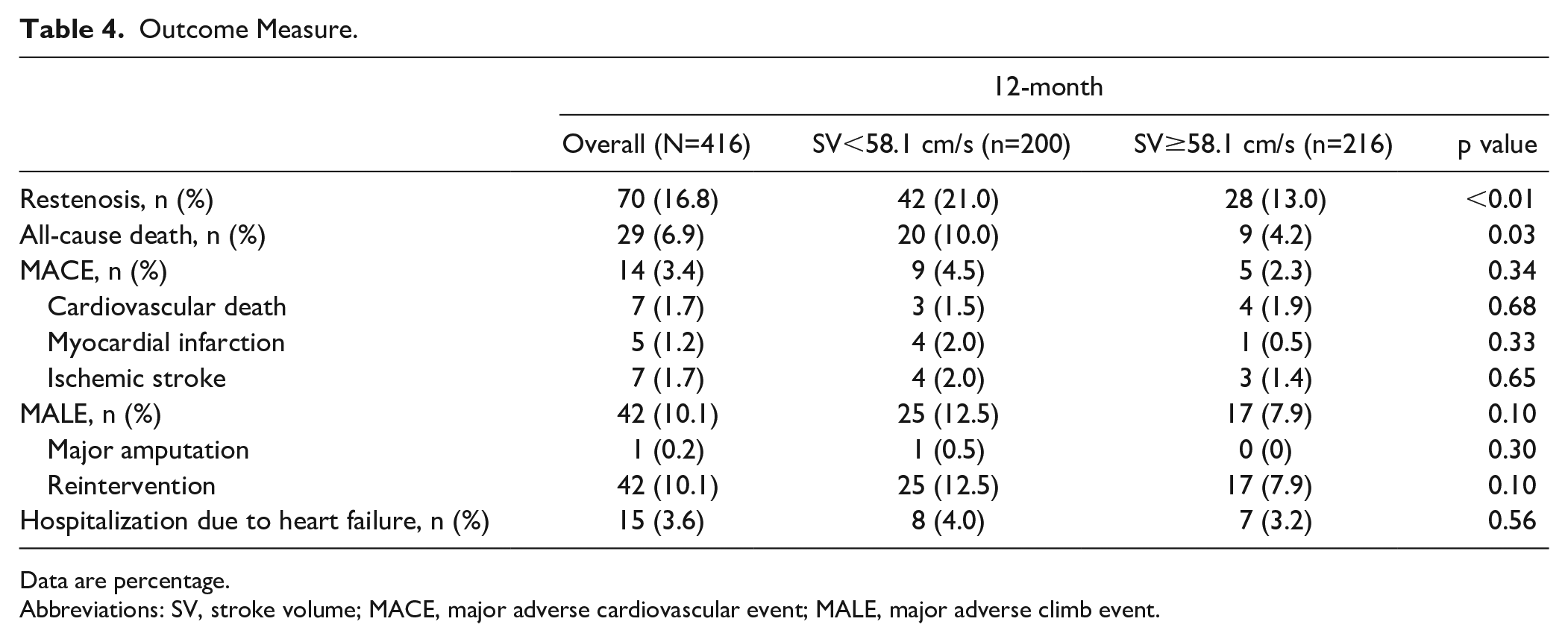
Data are percentage.
Abbreviations: SV, stroke volume; MACE, major adverse cardiovascular event; MALE, major adverse climb event.
Discussion
The current study analyzed 547 lesions in 416 patients with PAD presenting FP lesions endovascularly treated with new-generation FP-specific devices to assess the relationship between cardiac function and 12-month primary patency. Multivariate analysis showed that reduced SV assessed by echocardiography, CHF, and a smaller distal reference vessel diameter were significantly associated with 12-month loss of primary patency.
In PAD patients, the annual mortality rate has been reported to be as high as 12% per year.1,2 The PAD is also associated with increased risk for incident heart failure. The prevalence of CHF among patients with PAD is estimated at 5% to 15% and PAD is associated with a twofold increase in relative risk for CHF. 15 In several recent series of patients undergoing endovascular interventions, the prevalence of CHF actually approached 30%.3,4 Observational studies and meta-analyses have consistently shown that the presence of PAD in CHF patients is an independent predictor of hospitalization, mortality, and poor limb prognosis.16–18 In the Heart Failure: A Controlled Trial Investigating Outcomes of Exercise Training (HFACTION) study, PAD was reported in 7% of patients with heart failure and an LV ejection fraction of <35% and was associated with an increased risk of all-cause hospitalization and mortality (HR=1.31, p=0.011). 16 Bakken et al 19 also showed that CHF was associated with an increased risk of amputation. In addition to the high prevalence and adverse event of PAD in CHF patients, patency after EVT for this group has been also very limited.
Several recent studies have reported diminished patency after EVT in CHF patients. Conrad et al 3 found that CHF was an independent predictor of reduced primary patency, assisted patency, and limb salvage after superficial femoral artery intervention with traditional therapy using plain balloon angioplasty or bare nitinol stent use. O’Brien-Irr et al 4 reported an increased failure rate of FP and tibial endovascular interventions with plain balloon angioplasty or bare nitinol stent use in patients with CLTI and CHF. Meltzer et al 20 showed that CHF, and specifically, heart failure with reduced EF were independent risk factors for loss of patency after endovascular intervention for symptomatic PAD.
Although those are important data because CF has received minimal attention as a risk factor for reduced patency post-EVT in PAD patients, those are in the era of conventional therapy using plain balloon angioplasty or bare nitinol stents. Currently, new-generation FP-specific devices, including pharmacologically suppressing neointimal hyperplasia using biological therapies and mechanically blocking neointimal proliferation via stent struts, are clinically emerging for the treatment of FP lesions and these devices showed better long-term patency than conventional balloons and bare nitinol stent.8–10 The current study revealed that a reduced stroke volume as well as CHF and a smaller distal reference vessel diameter were significantly and independently associated with the loss of primary patency in PAD patients with FP lesions post-EVT with new-generation FP-specific devices.
Consistent with the current study, CHF is previously reported to be an independent predictor for primary patency.3,4,20 The current study showed that CHF was a still strong predictor for restenosis even if we used new-generation FP-specific devices. Vessel diameter was also previously reported to be an independent predictor for primary patency. In analysis without IVUS data, a smaller angiography-evaluated reference vessel diameter was significantly associated with a higher risk of restenosis. 21 Interestingly, the current study also showed that female gender, diabetes mellitus, and chronic total occlusion (CTO) lesions were not associated with any elevated risk for loss of patency after EVT. From latest experience and evidence in FP EVT, these factors are described as a critical risk factor for refractory restenosis. 22 The current finding was in contrast to these previous experiences, implying that the new-generation devices might overcome these risk factors influencing restenosis occurrence.
In this current study, we focused on SV in CF. Pathologically, restenosis or occlusion begins with the formation of thrombosis, which leads to the activation of vascular endothelial growth factor (VEGF). The classical mechanism of thrombus formation is represented by Virchow triad of blood stasis, endothelial injury, and hypercoagulability. The SV directly reflects blood flow and this mechanism strongly supports the relationship between SV and patency. Although LVEF is the traditionally representative parameter that reflects cardiac condition, once cardiac function is impaired, LVEF reduces first as the left ventricular end-diastolic volume (LVEDV) compensatory gets larger to preserve SV. Therefore, LVEF does not exactly reflect blood flow and may not be associated with loss of patency after EVT.
In addition, 24-month primary patency was significantly lower in patients with reduced SV as shown in Supplemental Figure 1. However, 12-month difference was neither spread nor attenuated, meaning SV might not be a predictive factor for loss of primary patency after 12 months. Although reduced SV was reported to be significantly associated with cardiac death and hospitalizations due to worsening heart failure at the mean follow-up period of 991 days on the Kaplan-Meier analysis, 23 the current study revealed the incidences of MACE, including cardiac death, and hospitalizations were not significantly different between the 2 groups at 12 months. The impact of SV on prognostic outcome in PAD patients might be established by performing a longer follow-up. In this study, reduced SV was related to loss of patency, and once SV has been reduced, it is difficult to recover. In PAD patients, it is important to evaluate CF and try to preserve SV by the use of medication or intervention in early stages. Also, the usage of anticoagulant drug after EVT is shown to improve the mortality. 24 It may be more beneficial to use anticoagulant drugs in patients with reduced SV because the anticoagulant drugs more effectively prevent thrombosis formation in low-flow state.
This study has several limitations. As a retrospective review, the analysis was based on electronic medical record documentation and was subject to misclassification error. Moreover, although an effort was made to analyze all established risk factors for patency loss, the list of dependent variables was inherently incomplete. Other limitations include practical issues with follow-up of CF, echocardiography taken only once, inability to obtain follow-up CF results, and not classifying the cause of the reduced SV.
Conclusion
The current study revealed that cardiac function represented by reduced stroke volume and presence of CHF as well as a smaller distal reference vessel diameter were significantly associated with a loss of 12-month primary patency in patients with PAD presenting with FP lesions endovascularly treated with the new-generation FP-specific devices.
Supplemental Material
sj-tiff-1-jet-10.1177_15266028211070963 – Supplemental material for Impact of Cardiac Function on Loss of Patency in Patients With Peripheral Artery Disease Presenting the Femoropopliteal Lesions Endovascularly Treated With New-Generation Devices
Supplemental material, sj-tiff-1-jet-10.1177_15266028211070963 for Impact of Cardiac Function on Loss of Patency in Patients With Peripheral Artery Disease Presenting the Femoropopliteal Lesions Endovascularly Treated With New-Generation Devices by Sho Nakao, Osamu Iida, Yosuke Hata, Shin Okamoto, Takayuki Ishihara, Kiyonori Nanto, Takuya Tsujimura, Mitsuyoshi Takahara and Toshiaki Mano in Journal of Endovascular Therapy
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.