
Abstract
Background:
The Trans-Atlantic Inter-Society Consensus Document (TASC II) aims to comprehensively describe the case scenarios of aortoiliac and femoropopliteal lesions to suggest an endovascular or a surgical approach. Over time, it has become a guide for describing the gravity of arterial lesions.
Purpose:
To assess the revised TASC II system for classifying arterial lesions in a large database of patients presenting with claudication.
Materials and Methods:
This study was a retrospective review of the arteriograms of patients with intermittent claudication. Aortoiliac and femoropopliteal lesions were classified according to the TASC II. When no consensus was reached, the lesion was rated as unTASCable.
Results:
In total, 1454 patients were included (male: 62.1%, 66.8±9.3 years). There were 39% aortoiliac lesions (n=960/2462) and 61% femoropopliteal lesions (n=1502/2462); 33.6% of the patients (n=489/1454) were associated with aortoiliac and femoropopliteal lesions. In addition, 20% of the lesions (n=493/2462) were unTASCable, and 26.7% of the patients (n=388/1454) had at least 1 unTASCable lesion. There were 4 categories of unTASCable lesions: (1) association with a common femoral artery lesion in 53.1% (n=262/493); (2) iliac artery lesions in 23.1% (n=114/493); (3) femoropopliteal lesions whose lengths did not fit into any category in 16.6% (n=82/493); and (4) association with an aortic lesion in 7.1% (n=35/493). The interobserver agreement was 0.97 for anatomically describing the infrarenal arterial tree and 0.85 for TASCing, with the lesions lowering to 0.69 for aortoiliac lesions.
Conclusion:
Using the revised TASC II case scenario, 26.7% of the patients had at least 1 unTASCable lesion. Reporting peripheral artery disease using a comprehensive anatomical description of the infrarenal arterial tree showed better interobserver reproducibility.
Introduction
With more than 8000 citations, the revised Trans-Atlantic Inter-Society Consensus Document on Management of Peripheral Arterial Disease (TASC II) is 1 of the essential references in the vascular scientific and clinical community. 1 This multidisciplinary consensus aimed to standardize the reporting of aortoiliac and femoropopliteal lesions based on anatomical location and morphological complexity to reflect their suitability for endovascular, surgical, or hybrid interventions. Over time, the “endovascular first” approach has become preeminent, lowering its clinical interest in defining the “best treatment.” 2 Nevertheless, its capability in grading the severity of the lesions has proven to be useful in characterizing clinical trial populations, allowing some comparison across studies. 3 The Trans-Atlantic Inter-Society Consensus Document has recently been updated. 4 Nevertheless, most of the aortoiliac and femoropopliteal case scenarios defining the TASC categories have remained unchanged, with the same constrained length limits for classifying the lesions and with no additional recommendation regarding the common iliac and common femoral artery (CFA) bifurcations. 5
A comprehensive classification of the lesions of the patients treated at our institution from 2008 to 2018 was performed. During the first evaluations, despite thorough training of all the readers and daily collegial agreement meetings, several case scenarios remained unTASCable. To obtain reliable reporting of arterial lesions to allow proper comparisons, we comprehensively described infrarenal arterial trees along the TASCing of lesions.
This study’s main goal was to assess the capability and reliability of the TASC case scenario approach for describing aortoiliac and femoropopliteal lesions in patients presenting with intermittent claudication. The secondary purposes were to categorize the different unTASCable case scenarios, calculate their frequency, and analyze the reason for their unTASCability.
Materials and Methods
Study Endpoints
The primary endpoint of this study was to determine the applicability of the TASC II lesion grading system to properly rate a large database of aortoiliac and femoropopliteal lesions in patients presenting with intermittent claudication.
The secondary endpoints were to categorize and analyze the different unTASCable case scenarios, as well as to calculate their respective frequencies.
Patient Population
The study was approved by the local institutional ethics committee of the Centre Intégré Universitaire de Santé et de Services Sociaux de l’Estrie—Centre Hospitalier Universitaire de Sherbrooke (CIUSSS de l’Estrie-CHUS). This study was a single-center observational retrospective review of the angiograms of consecutive patients presenting with intermittent claudication and referred for endovascular revascularization after well-conducted medical management at the University Hospital of Sherbrooke from January 2008 to December 2018. Written consent to participate in the study was waived because of the study’s retrospective character. Following the institutional and local regulatory policies, all the patients signed written informed consent before undergoing the procedure.
The inclusion criteria were as follows: (1) patients older than 18 years; (2) patients presenting with intermittent claudication (Rutherford 2–3); and (3) patients referred for endovascular revascularization after well-conducted medical therapy. The exclusion criteria were as follows: (1) repeat arteriogram during the 2008 to 2018 period of the study and (2) nonatherosclerotic disease (trauma, aneurysm).
Detailed demographic, clinical, and procedural information was collected for each patient from their digital file.
Digital Subtraction Angiography Angiograms
Routinely, an anteroposterior abdominal aortogram and 30° right and left anterior oblique arteriograms of the aortoiliac arteries and lower limb arteriogram(s) were obtained using a moving table protocol.
Descriptive Lesion Analysis
The angiograms were reviewed using a Synapse 5.1 PACS system (Fujifilm Medical Systems, Stamford). The images were analyzed by 6 readers (6 medical students) supervised by a senior interventional radiologist (GG, 15 years of experience) during an 8 week medical research rotation. One week of training was provided to the medical students before beginning the classification of the arterial lesions. The training included the reading of arteriograms using a training data set of 50 digital subtraction angiographies (DSAs).
The database was split into 6 equal parts, and each reader analyzed the corresponding arteriograms. The entire infrarenal vascular tree of each patient was comprehensively analyzed, and every arterial lesion was located, measured, and reported on a web app developed for this study (Figure. 1) connected to a secured database server (Filemaker Server 17; Claris International Inc, Santa Clara, California). Following this analysis, the aortoiliac and femoropopliteal lesions were rated using the TASC II criteria. During the entire database analysis, a daily collegial meeting was held to review the ratings. When no consensus was reached for the TASC classification of an aortoiliac or a femoropopliteal lesion, the lesion was rated as unTASCable. The different reasons for inconclusive lesion ratings were analyzed and reported. A randomly chosen data set of 40 DSAs was analyzed to calculate the interobserver agreement for anatomically describing the infrarenal arterial tree and for TASCing aortoiliac and femoropopliteal lesions. The interobserver agreement was performed by 1 senior reader (GG) and 2 medical students (AB, MB), 2 months after the end of the medical research rotation.
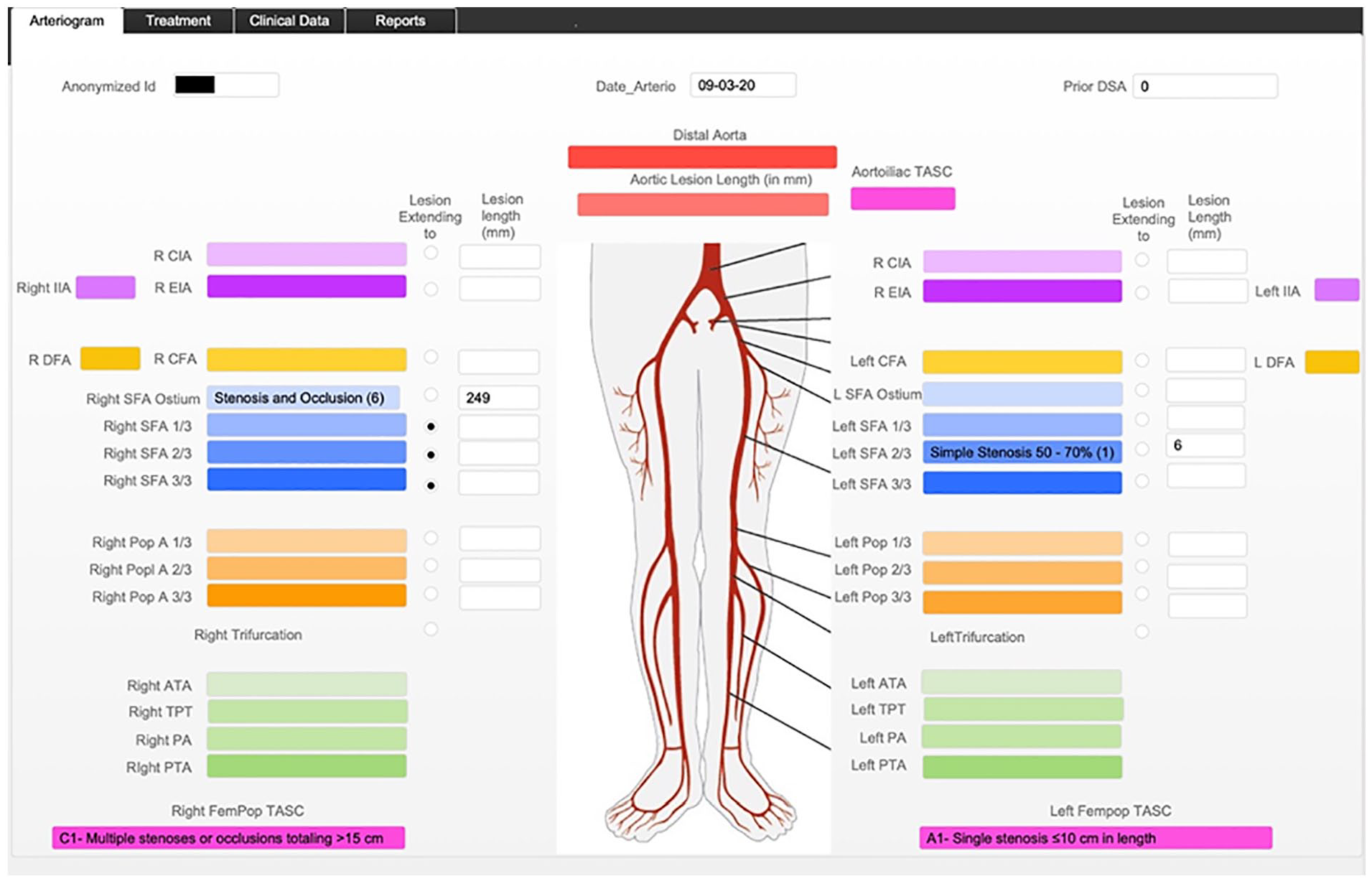
Web app designed for the study, allowing a comprehensive description of lower limb peripheral artery disease, including the severity, location, length of steno-occlusive disease, and corresponding TASC grading. TASC, Trans-Atlantic Inter-Society Consensus Document; ATA, anterior tibial artery; CFA, common femoral artery; CIA, common iliac artery; DFA, deep femoral artery; EIA, external iliac artery; IIA, internal iliac artery; SFA, superficial femoral artery; PA, peroneal artery; PTA, posterior tibial artery; TPT, tibioperoneal trunk.
Statistical Analysis
Continuous variables were expressed as mean±standard deviation. Dichotomous and categorical variables were expressed as counts and percentages. Continuous variables were compared using the Mann-Whitney test or Student’s t test. Categorical data were compared using chi-squared or Fisher’s exact test. Interobserver agreements were calculated using Cohen’s and Fleiss’ kappa. The level of statistical significance was set at p<0.05.
Results
Patients
From 2008 to 2018, 5219 consecutive lower limb arteriograms were performed. After the initial revision of the files, the 1454 first arteriograms performed in 1454 patients with intermittent claudication (Rutherford 2 and 3) were analyzed. The cohort included 62.1% men (n=903) and 37.9% women (n=551) with a mean age of 66.8±9.2 years. The baseline clinical characteristics are summarized in Table 1. The cardiovascular risk factors were highly prevalent, including arterial hypertension in 62.4%, hyperlipidemia in 59.8%, active smoking in 22.8%, and diabetes in 28.3% of patients.
Clinical Characteristics of the Entire Cohort and According to the Arterial Lesion Type of the Patients Included in the TASCability study.
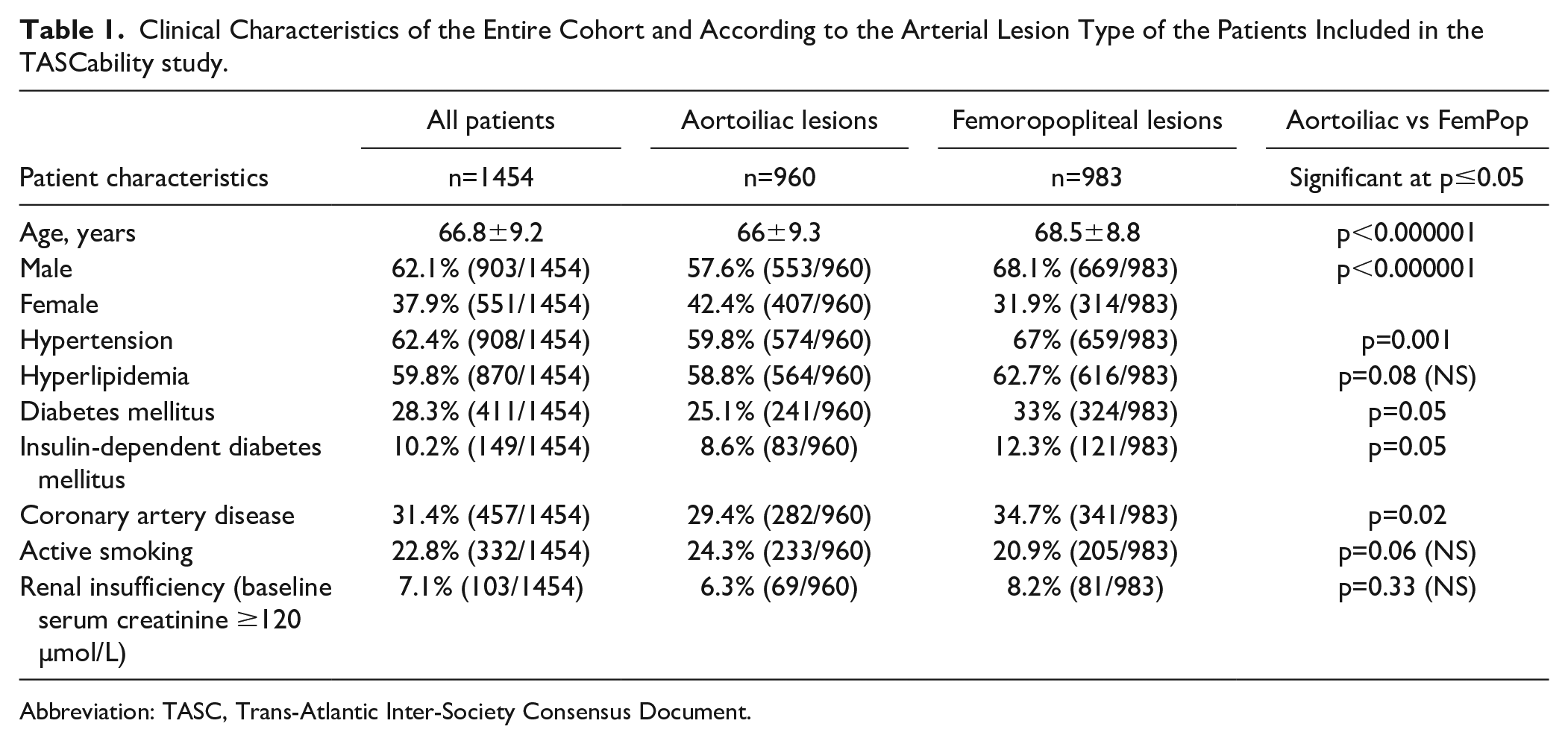
Abbreviation: TASC, Trans-Atlantic Inter-Society Consensus Document.
Several baseline characteristic differences were statistically significant between the aortoiliac and femoropopliteal lesion groups: mean age (66±9.3 years vs 68.5±8.8 [p<0.00001]); sex ratio (57.6% of men vs 68.1%, respectively [p<0.00001]); arterial hypertension (59.8% vs 67% [p=0.001]); diabetes mellitus (25.1% vs 33% [p=0.05]); type 1 diabetes (8.6 and 12.3%, [p=0.05]); and coronary artery disease (29.4 and 34.7% [p=0.02]). However, hyperlipidemia, tobacco use, and renal insufficiency were not significantly different between the groups.
Image Analysis/TASC Rating
Among the 1454 patients, 2462 significant lesions were identified, corresponding to 39% (n=960/2462) aortoiliac lesions, 30.1% (n=742/2462) left femoropopliteal lesions, and 30.9% (n=760) right femoropopliteal lesions. The different associations of the lesions are reported in Table 2. Most aortoiliac lesions were rated as TASC A (40.8%, n=392) (Table 3), whereas femoropopliteal lesions were more evenly distributed among TASC A, B, and C (18.8%, 28% and 28%, respectively) (Table 4).
Aortoiliac and Femoropopliteal Artery Lesion Associations Encountered in the Patients Included in the TASCability Study.
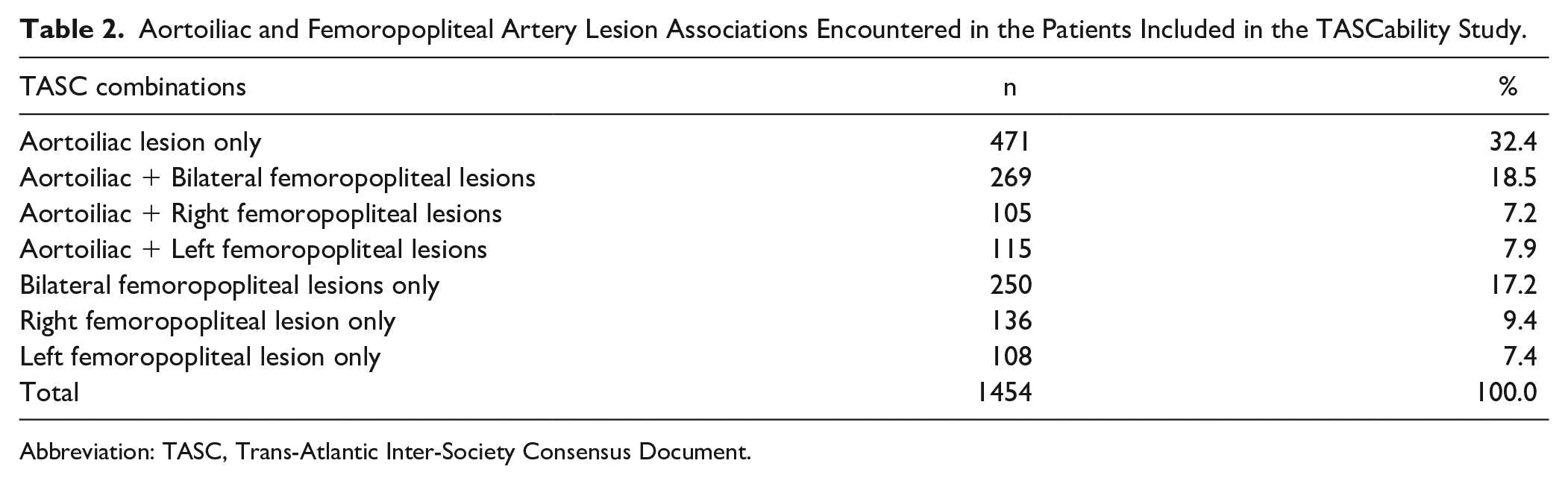
Abbreviation: TASC, Trans-Atlantic Inter-Society Consensus Document.
Classification of Aortoiliac Artery Lesions According to the TASC II Grading Consensus.
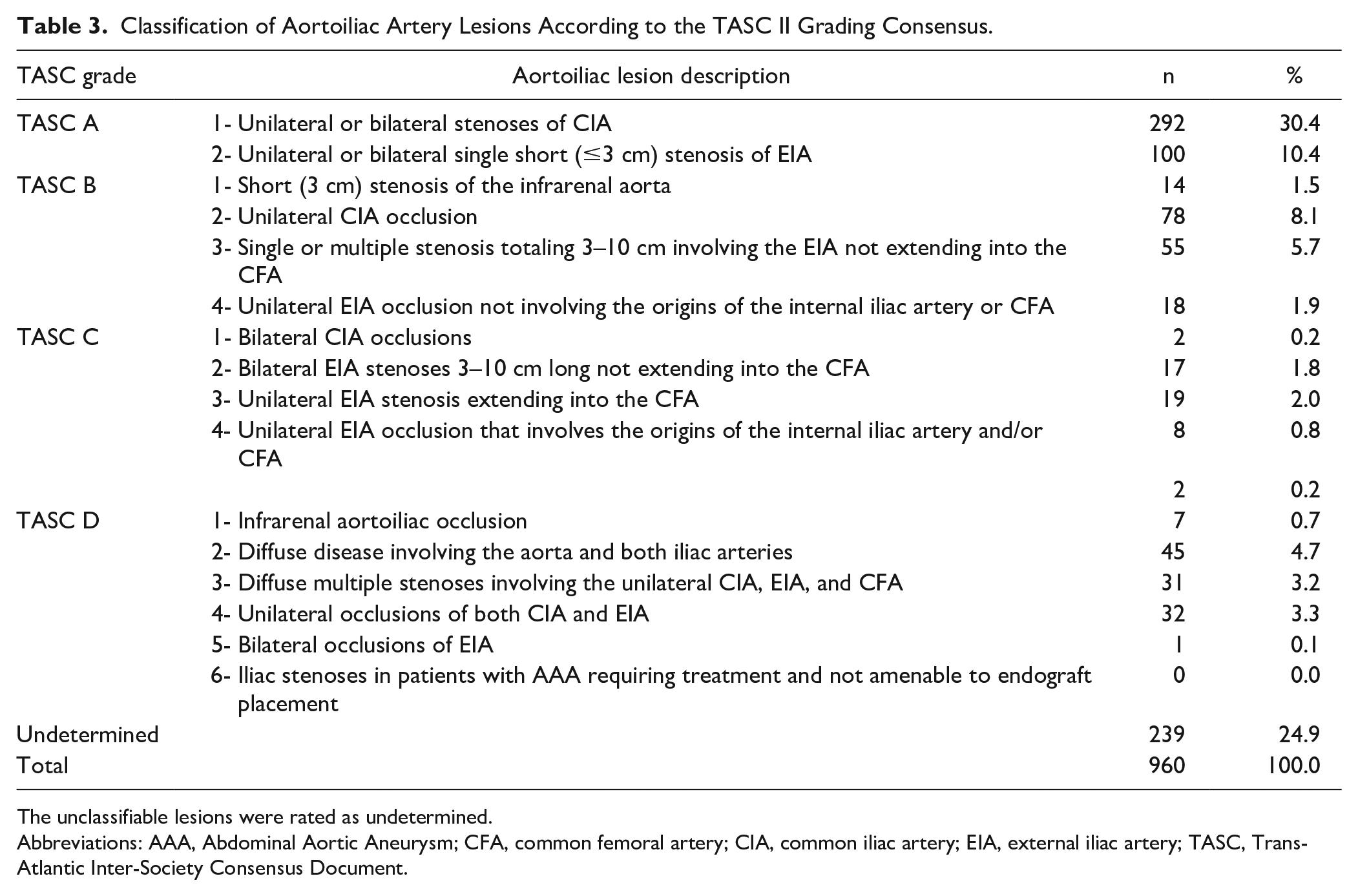
The unclassifiable lesions were rated as undetermined.
Abbreviations: AAA, Abdominal Aortic Aneurysm; CFA, common femoral artery; CIA, common iliac artery; EIA, external iliac artery; TASC, Trans-Atlantic Inter-Society Consensus Document.
Classification of Femoropopliteal Artery Lesions According to the TASC II Grading Consensus.
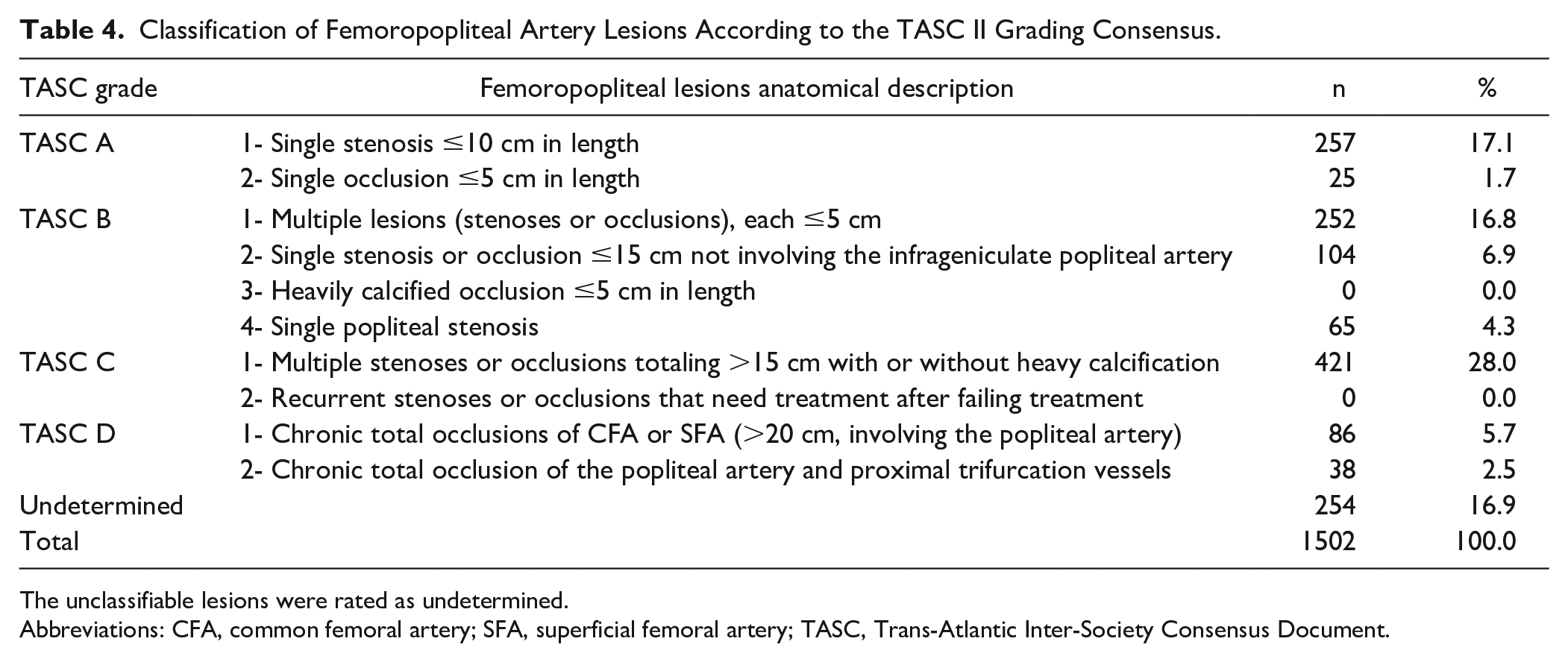
The unclassifiable lesions were rated as undetermined.
Abbreviations: CFA, common femoral artery; SFA, superficial femoral artery; TASC, Trans-Atlantic Inter-Society Consensus Document.
Twenty percent of the vascular lesions (n=493/2462) were classified as unTASCable, corresponding to 24.9% (n=239/960) of the aortoiliac and 16.9% (n=254/1502) of the femoropopliteal lesions. At least 1 unTASCable lesion was encountered in 26.7% of the patients (n=388/1454). Significantly more unTASCable lesions were found in the aortoiliac group than in the femoropopliteal group (p=0.05). A comprehensive description of the lesions classified as undetermined is reported in Table 5 with the corresponding drawings in Figures 2 and 3. Overall, 23 types of lesions were considered unTASCable using the TASC II convention: 15 categories for aortoiliac lesions and 8 for femoropopliteal lesions. Among the 23 unTASCable case scenarios, the 5 most common lesions represented 57.8% (n=285/493) of the unTASCable lesions as follows: (1) CFA stenosis with ipsilateral femoropopliteal stenosis in 16.4% of cases (n=81/493); (2) CFA stenosis with ipsilateral femoropopliteal occlusion in 13.4% of cases (n=66/493); (3) bilateral common iliac artery (CIA) and/or external iliac artery (EIA) and unilateral or bilateral CFA stenoses in 11.8% (n=58/493); (4) unilateral CIA and EIA stenoses and contralateral CIA or EIA lesions in 8.3% of cases (n=41/493); and (5) unilateral CIA and EIA stenoses in 7.9% of cases (n=39/493). The general interobserver agreement for TASCing arterial lesions was 0.85 (good agreement), with 0.93 (excellent agreement) for femoropopliteal lesions and 0.69 (moderate agreement) for aortoiliac lesions. The interobserver agreement for anatomically describing infrarenal arterial trees was 0.97 (excellent agreement).
Classification and Repartition of the Unclassifiable Aortoiliac and Femoropopliteal Artery Lesions.
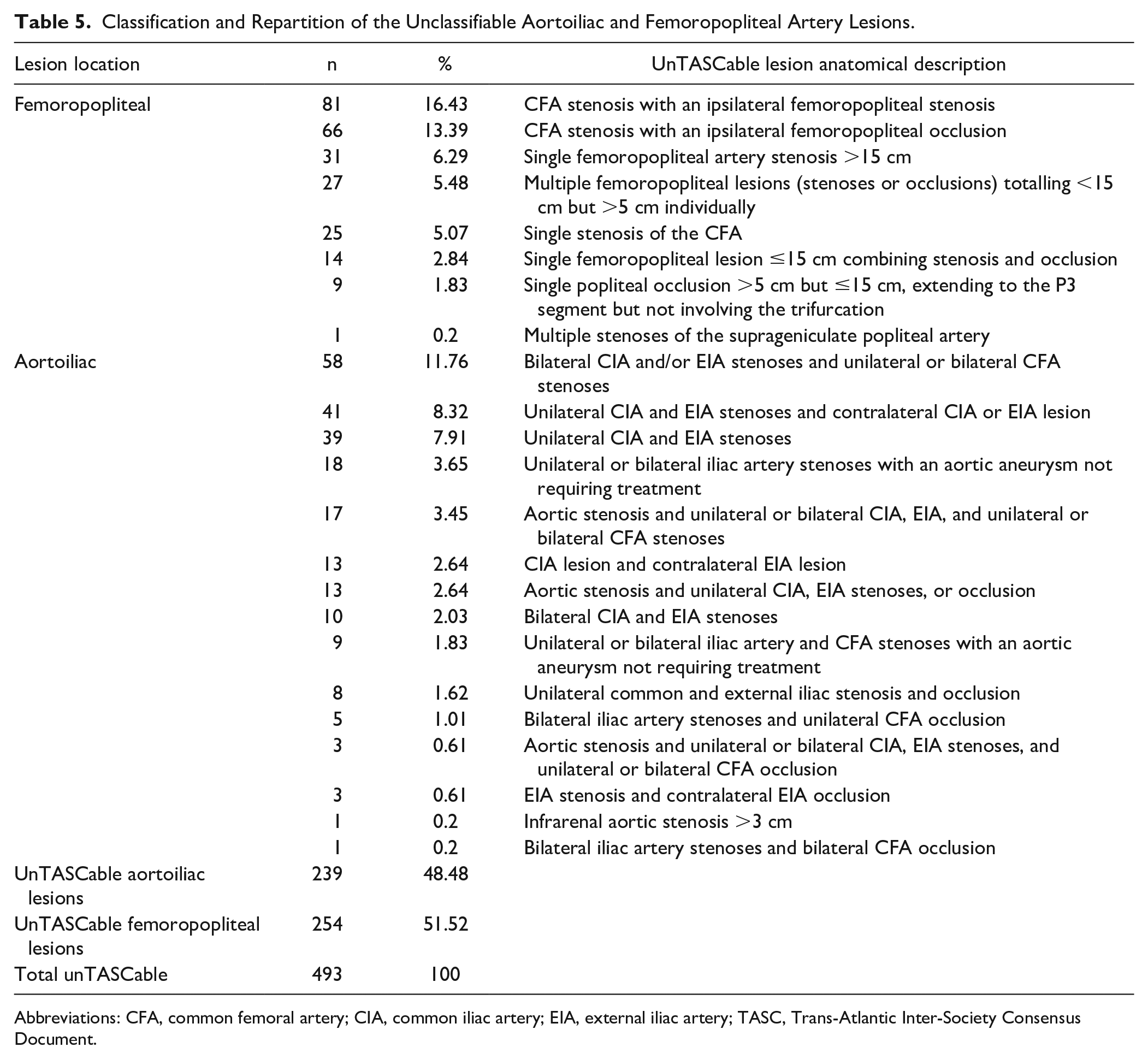
Abbreviations: CFA, common femoral artery; CIA, common iliac artery; EIA, external iliac artery; TASC, Trans-Atlantic Inter-Society Consensus Document.
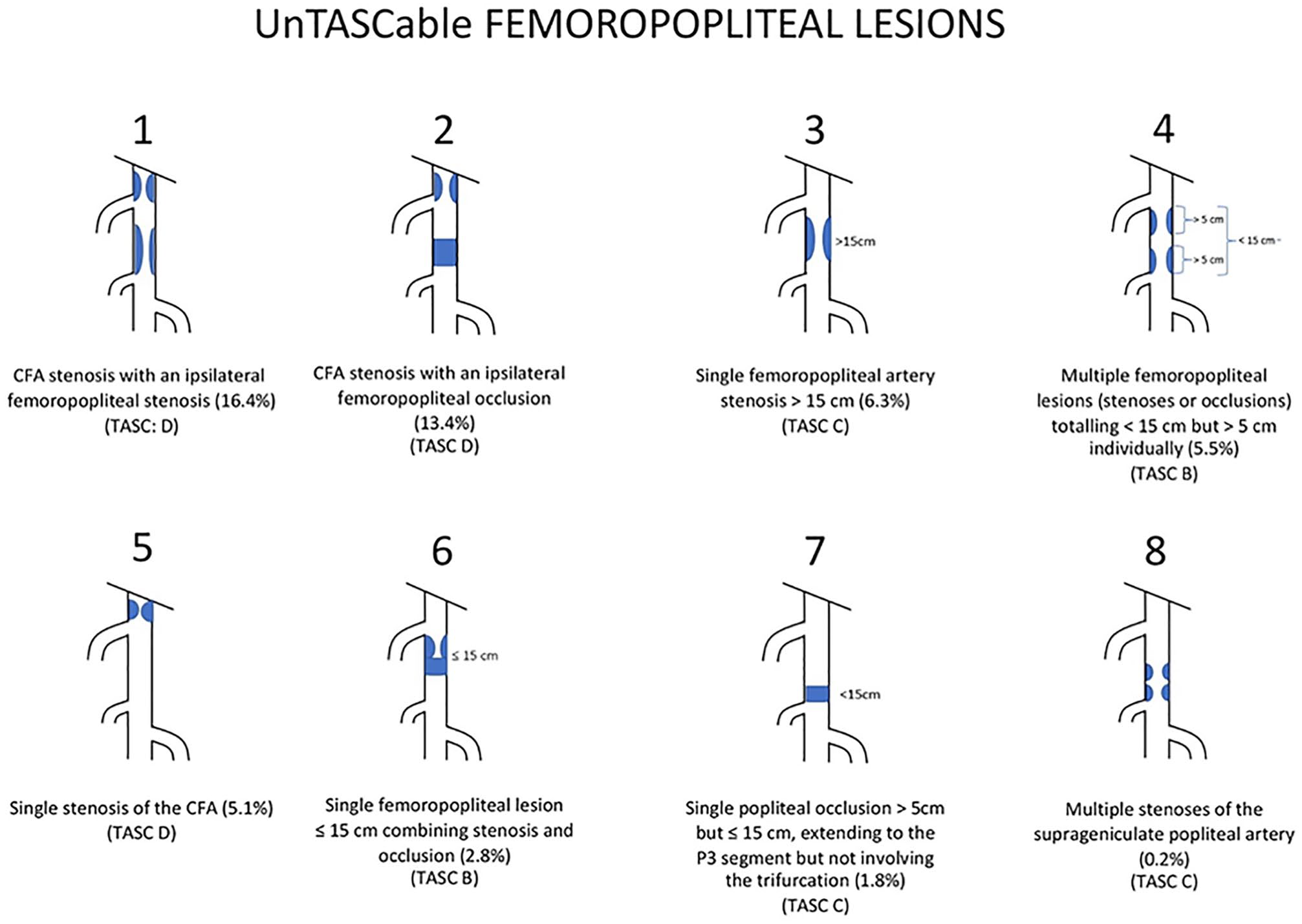
Femoropopliteal unTASCable case scenarios encountered in the TASCability study ordered from the most to the least frequently encountered cases for each group. A suggested TASC categorization has been mentioned. TASC, Trans-Atlantic Inter-Society Consensus Document; CFA, common femoral artery.
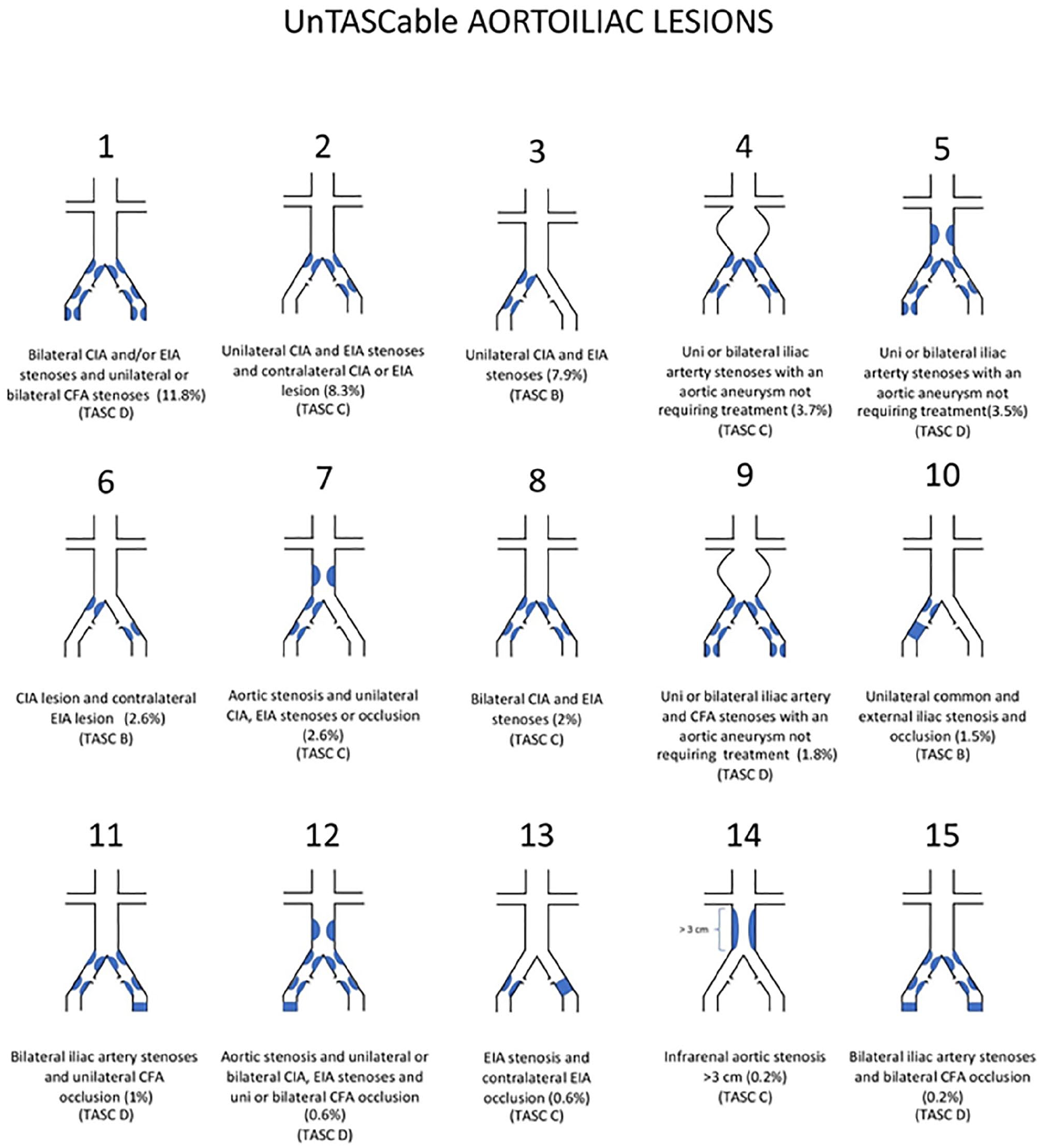
Aortoiliac unTASCable case scenarios encountered in the TASCability study ordered from the most to the least frequently encountered cases for each group. A suggested TASC categorization has been mentioned. CFA, common femoral artery; CIA, common iliac artery; EIA, external iliac artery; TASC, Trans-Atlantic Inter-Society Consensus Document.
Discussion
Classifying peripheral artery disease is a difficult challenge because of its many variations. The authors of the TASC system chose to use a case scenario approach. As shown in our study, this approach has significant limitations, with 20% of the aortoiliac and femoropopliteal lesions identified in clinical practice being unTASCable. This leaves 26.7% of our patients with no treatment recommendation and no classification as a severity marker.
During the first round of lesion analysis, which led to the TASCability study, several lesions were difficult to classify. Given the worldwide acceptance of the TASC classification, an attempt was made to fit the lesions into 1 of the 4 categories. In doing so, a few problems were observed. Several TASC case scenarios had subjective interpretability (apparently contradictory or deemed imprecise definitions), as previously reported by Kukkonen et al. 6 For example, the TASC II D1 definition (chronic total occlusions of CFA or superficial femoral artery (SFA) >20 cm, involving the popliteal artery) may be confusing. It is unclear whether SFA occlusions must both be >20 cm in length and have popliteal involvement or whether either is sufficient to justify D1 classification . This finding was 1 reason for the reported poor interreader agreement of the TASC II classification.6,7 Our initial solution to this problem was to rate the lesions following a clear consensus between readers, developed throughout the reading of the first arteriograms. This local agreement concerning TASC definitions was based on subjective interpretation, dramatically lowering the TASC value for severity grading. Another critical issue was that the word “stenosis” was not defined. In the Consensus for Vascular Registries published in 2018, vascular surgeons agreed upon stenosis as being a narrowing >50% of the arterial lumen. 8 This definition is used as a cut-off for treatment in the “Global vascular guidelines on the management of chronic limb-threatening ischemia.” 9 However, the 2016 American College of Cardiology/American Heart Association guidelines for managing peripheral artery disease indicated that a reduction in the diameter by 50% to 75% might not be hemodynamically significant. 10
A staging system should be based on clearly defined and objective criteria that allow an efficient and adequate classification of the lesions. Such a well-designed algorithm should enable software to classify the lesions. To perform an objective classification of the encountered lesions, the inconclusive lesions were rated as unTASCable. The analysis of those lesions demonstrated that, in addition to the subjective interpretability of some case scenarios, there was also an important lack of case scenarios.
Approximately half of the unTASCable lesions were related to the presence of CFA lesions, which represented 10.6% (n=262/2462) of the vascular lesions and 53.1% (n=262/493) of the unTASCable lesions. The lack of case scenarios regarding the involvement of the CFA is likely due to CFA being regarded as a surgical territory in 2007 and its description deemed unnecessary. 11 This dogma has now been challenged with several clinical trials, such as the TECCO study, 12 which prospectively compared endovascular and surgical techniques. An up-to-date classification should include a description of the CFA and its bifurcation.
The second most frequent unTASCable case scenarios were related to iliac-only lesions. Together, those cases represented 23.1% (n=114/493) of the unTASCable lesions or 11.9% of the aortoiliac lesions (114/960). As acknowledged by the Society for Vascular Surgery guidelines, iliac artery lesions are usually primarily treated endovascularly with good long-term patency results. 13 Nevertheless, a proper comparison of iliac lesions is required to allow management improvement.
The third category of missing case scenarios regarded femoropopliteal artery lesions whose lengths did not fit in any of the TASC II categories. Those cases represented 16.6% (n=82/493) of the unTASCable lesions. The most frequent unTASCable lesion was single femoropopliteal artery stenosis >15 cm, representing 2.1% of femoropopliteal lesions (n=31/1502). This case scenario fell exactly between the TASC B2 and TASC C1 recommendations (Table 4). Whether the chosen cut-offs (5 and 15 cm) are still relevant currently remains unknown.
The fourth group corresponded to aortic lesions, which represented 7.1% (n=35/493) of the unTASCable lesions (when omitting associated CFA lesions). One important case scenario was the association of unilateral or bilateral iliac lesions with an aortic aneurysm, which does not require treatment. Properly treating those patients without preventing the opportunity for a future endovascular graft is of utmost importance.
To help with the TASC classification of the unTASCable lesions, a TASC categorization has been suggested (Figure 2 and 3). Those suggestions were made trying to respect the spirit of the TASC II classification. Nevertheless, since its publication in 2007, many innovations have been made in the endovascular therapy field and those categories should be revisited.
Reporting Peripheral Artery Disease: Building the Future
The initial objective of the TASC classification to define the best treatment approach by comparing endovascular and surgical techniques side by side is debatable. This “silver bullet” approach aimed at determining the treatment that would supersede another for each case scenario. Because atherosclerosis is part of normal artery aging, accelerated by well-known risk factors, recurrence is more a rule than an exception.14,15 In practice, both techniques have strengths and weaknesses and may be used subsequently in the long-time course of peripheral artery disease. Data are required to predict technical success, patency rates, complications, and patient survival for each technique.
Although the TASC II classification has not been updated since 2015, many operators still refer to it worldwide. 16 The reason is simple—there is a dire need for a classification that allows the comparison of studies and practices for patients with claudication. The TASC system has become a marker of severity of arterial lesions. Although the system allows some comparisons, reporting the many case scenarios as 1 of the 4 TASC categories leads to destructive sampling, reducing the potential for subsequent analyses and refinement of the classification. As demonstrated in our study, 33.6% of the patients (n=388/1454) had a combination of aortoiliac and femoropopliteal lesions. These patients are not properly considered by the current TASC approach, which divides the vascular tree into different anatomical areas. Given the importance of both inflow and outflow on arterial patency, it is questionable whether such a system should be used instead of a more comprehensive system. A simple solution could be to systematically describe the entire infrarenal arterial tree for every patient reported in clinical trials and registries. 17 As shown in our study, the reporting of peripheral artery disease using a purely anatomical description has an excellent interobserver reproducibility of 0.97, compared with 0.85 when using the TASC classification, even lowering to 0.69 for TASCing aortoiliac lesions.
This finding advocated for the movement from the current lesion-based “patchwork” system that juxtaposes the different anatomical level type knowledge to a more comprehensive patient-based approach. Infinite computations and comparisons would be enabled that are independent of any constrained staging system. The limitation of not having registries that include thorough arterial bed descriptions is exemplified by the brand-new limb-based anatomic staging GLASS system designed to manage critical limb ischemia. As acknowledged by their authors, the GLASS system still requires prospective validation because no large patient-level anatomical database exists. A similar approach has been successfully used by the International Association for the Study of Lung Cancer to design and revise the tumor, node, and metastasis staging system of lung cancer recommendations. 18 They have progressively developed an international database with anatomical and nonanatomical elements, now accounting for more than 90 000 patients. This database allows the precise definition of anatomical criteria to predict the outcomes and propose the right treatments. Moving from a lesion-level to patient-level data reporting has already been promoted following the paclitaxel controversy and difficulties in adequately demonstrating whether paclitaxel has a significant impact on patient mortality.19,20
With the advent of big data analysis and artificial intelligence, there would be no better moment for scientific societies to develop a standard tool for reporting and analyzing lower limb arterial lesions in patients with claudication. A well-designed registry relying on a comprehensive anatomical description could help improve management practices. 21 Recently, the American College of Cardiology and the Society for Vascular Surgery announced their intention of uniting forces through a common registry. 22 This is a huge step forward for patient care. The question is how will the lesions be reported?
Conclusion
As envisioned by Robert Rutherford, the TASC classification has been a successful attempt to create a universally accepted system to describe arterial lesions. 23 Nevertheless, in its current version, the TASC II has several drawbacks: subjectivity of some definitions, lack of important definitions, and a lack of case scenarios, allowing only the proper classification of 80% of aortoiliac or femoropopliteal lesions in patients with claudication. A new classification is needed. To build more comprehensive and reliable evidence for peripheral artery disease management, our community should consider moving from the current lesion-based to a patient-based description of arterial lesions.
Study Limitations
Our study did not consider CIA or CFA bifurcations and infrapopliteal arteries.
A bias may have lowered the proportion of CFA lesions because most of those lesions are primarily treated surgically without DSA at our institution.
Patients referred for an intervention may have more extensive multilevel atherosclerotic disease.
Clinical Perspectives
Our study advocate for moving from the current “patchwork” lesion approach to a patient-level approach for being able to properly compute the large variability of arterial lesions encountered in clinical practice. This could eventually help to better define the anatomical criteria responsible for the outcomes and propose the right treatments.
Footnotes
Acknowledgements
We thank Mrs Sylvie Roy and Ju-Hong Lee, for their help in building up and reviewing the database. We thank Mr Daniel Robillard for his help in implementing the database server.
Author’s Note
Jean-Francois Vendrell is now affiliated to Université de Sherbrooke, Sherbrooke, QC, Canada.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Mach-Gaensslen Foundation of Canada. The Mach-Gaensslen Foundation of Canada had no involvement in the study design, collection, analysis, interpretation of data, writing of the article, or decision to submit the article for publication. The authors certify that they have no involvement in any organization, or nonfinancial interest in the subject matter or materials discussed in this article other than those disclosed thereafter: Gérald Gahide is a medical consultant for Boston Scientific.