
Abstract
Purpose:
Currently there is no robust evidence which type of bridging stent graft provides better outcomes after branched endovascular aortic repair (BEVAR). Self-expanding (SESG) and balloon-expandable (BESG) stent grafts are both commonly used to connect branches to their respective target vessels (TV). The aim of the current review was to evaluate the impact of the type of bridging stent grafts on TV outcomes during the mid-term follow-up after BEVAR.
Materials and Methods:
The study protocol was registered to the PROSPERO (CRD42021274766). A search of the English literature was conducted, using PubMed and EMBASE databases via Ovid and Cochrane database via CENTRAL, from inception to June 30, 2021, using the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines. Only comparative studies on BEVAR reporting TV outcomes related to BESG vs SESG were considered eligible. Individual studies were assessed for risk of bias using the Newcastle Ottawa Scale. The Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach was used to evaluate the quality of evidence. The primary outcomes were primary patency, freedom from endoleak, TV instability, and re-intervention between BESG and SESG, used as bridging stents in branches. The outcomes were summarized as odds ratio along with their 95% confidence intervals (CI), through a paired meta-analysis.
Results:
Five out of 609 articles published from 2016 to 2020 were included in the analysis. In total, 1406 TV were revascularized, 547 (38.9 %) with BESGs and 859 with SESGs. The overall pooled primary patency (odds ratio [OR], 0.40; 95% confidence interval [CI], 0.29–1.09; p=.256, I2=4.24%) and freedom from branch-related endoleak (OR, 0.65; 95% CI, 0.17–1.48; p<.122, I2=0.18%) did not differ between the stent types during the available follow-up (17 months, range = 12–35 months). In 4 studies (619 TV), SESG required fewer secondary interventions (OR, 1.04; 95% CI, 0.23–1.83; p=.009, I2=0%) and TV instability rate was lower (OR, 0.99; 95% CI, 0.33–1.65; p=.003, I2=0%) compared with BESG during the available follow-up.
Conclusion:
BESG and SESG seem to perform similarly in terms of primary patency and branch-related endoleak during the mid-term follow-up. Current data from retrospective studies suggest that overall TV instability and re-intervention rates are favorable for SESG as bridging stent grafts in BEVAR.
Introduction
Endovascular aortic repair of complex aortic pathologies with branched endografts (BEVAR) has been extensively used for the management of urgent and elective cases. Previous studies reported up to 97% technical success rate. 1 Off-the-shelf BEVAR devices are eligible for >50% of patients with thoracoabdominal aortic aneurysms (TAAA) with an estimated early mortality at 5%, ranging from 8.5% in elective to 30% in ruptured aneurysms, while the increased experience affects positively the associated safety and efficacy of the method.1 –5 In terms of perioperative morbidity, data retrieved from retrospective analyses presented an estimated spinal cord ischemia rate at 12.2% and acute renal failure at 18.7%. 5 Different factors may affect BEVAR outcomes including older age, obesity, history of coronary artery disease, and renal failure. 1
Along these lines, target vessels’ (TVs) complications have been under evaluation and their impact on BEVAR outcomes has also been under investigation. 6 No valid guideline recommendation nor high-level comparative effectiveness evidence has been available to guide physicians’ decisions on TV management regarding the type of bridging stent grafts that should be used for complex endovascular aortic repair. In the recent literature, the reported branch-related endoleak was >5% while patency and freedom from target vessel (TV) instability was reported to be more than 99% and 85%, respectively.1,7 Renal branch occlusion was the most common complication (8%), among all other visceral TVs.8,9 Different factors may have affect TV occlusion such as vessel morphology, stent-graft characteristics, and patients’ medical history.7,8 Due to the aforementioned findings, the impact of stent graft on TV adverse events has been a factor under investigation while to date, both self-expanding (SESG) and balloon-expandable (BESG) stent grafts have been used as bridging stents in branched devices.9 –11
The aim of this meta-analysis was to evaluate the impact of stent-graft type, as bridging stent, on TV outcomes in patients undergoing BEVAR.
Materials and Methods
Eligibility Criteria
Study protocol enrollment of this systematic review and meta-analysis were pre-specified and registered to the PROSPERO registry (CRD42021274766). The Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines were followed. 12 Ethical approval was not required. Eligible studies were considered any randomized controlled trial or observational, prospective, or retrospective study comparing TV-associated outcomes, including primary patency, branch-related endoleak, TV instability, and re-intervention between BESG and SESG in BEVAR. Studies reporting on TV outcomes without defining the associated stent type or including only one stent type—BESG or SESG—as well as studies including less than 20 patients were excluded. When studies reported on branch and fenestrated devices or when a composite of fenestrations and branches were present in the same main device, only data reporting on branches were included. Furthermore, in case of potential overlap between studies, the most recently published analysis was chosen to be included. Data extraction and methodological assessment were performed by two independent investigators (P.N, K.S.). Discrepancies were resolved after discussion with a third author (T.K.).
Search Strategy
A data search of the English medical literature was conducted, using PubMed, EMBASE, and CENTRAL databases, until 30 June 2021. The P.I.C.O. (patient; intervention; comparison; outcome) model was used to define the clinical questions and select relevant articles (Supplementary Table 1). 13 The following search terms, including Expanded Medical Subject Headings (MeSH), were used in various combinations: “stent,” “branch,” “thoracoabdominal,” “aneurysm,” “self-expandable,” “balloon.” The primary selection was based on title and abstract. A secondary scrutiny was performed according to the full text.
Data Extraction and Quality Assessment
Microsoft Excel was used to develop a standardized data extraction file. Extracted data included study characteristics such as author, date of publication, journal, center(s) performing the analysis, study period, and type of study. Clinical and technical information included type of intervention (branched endovascular aortic repair [BEVAR] or fenestrated endovascular aortic repair [FEVAR] which also included branches for TV catheterization), type of aneurysm and TAAA classification according to modified Crawford’s criteria, type of device used (platform), baseline demographics (age, gender), number of TVs, and type of stent graft (BESG or SESG). The application of relining was also recorded. In terms of outcomes, primary patency, freedom from branch-related endoleak, TV instability, and re-intervention were recorded during the available follow-up of each study.
Individual studies were assessed for clarity of reporting using the Newcastle-Ottawa Scale (NOS). 14 NOS evaluates 3 main methodological domains of cohort studies: selection methods, comparability of cohorts on the design or analysis, and assessment of outcomes. The scale uses a star system, with a maximum of 9 stars. Studies achieving at least 7 stars were considered of higher quality. 14 The Grading of Recommendations, Assessment, Development and Evaluations (GRADE) methodology was used to evaluate the quality of evidence and summary of findings for each of the included outcomes, to ensure that the effectuated judgments are systematic and transparent. 15 Supplementary Table 2 summarizes the results of the GRADE approach and Supplementary Τable 3 represents the summary of evidence.
Definitions
Branch-related endoleak was defined as any endoleak including type IC and IIIC endoleaks, due to distal bridging stent sealing zone or inter-attachment, respectively. 6 TV instability was defined a composite outcome used to define any death or rupture related to side branch complication, including occlusion, device migration affecting any branch, branch-related sac growth or any secondary intervention indicated to treat a branch-related complication, including endoleak, disconnection, kink, stenosis, occlusion, or rupture.16 -18 Re-intervention was considered any secondary intervention after the completion of the main intervention that was related to TV complications.
Outcomes
The comparative primary patency, freedom from endoleak, TV instability, and re-intervention between BESG and SESG, used as bridging stents in branches, were analyzed.
Statistical Analysis
The outcomes were summarized as odds ratio along with their 95% confidence intervals (CI), through a paired meta-analysis. The inter-study heterogeneity was evaluated using the significance of the Cochran’s Q-metric (pQ) and quantified by the Higgins I2 statistics. Significance was set at p<0.05, and we used continuity correction equal to 0.5 for metrics associated with zero events. The pooled estimate was assessed using the random-effects model in the presence of any inter-study heterogeneity (I2>50%). Publication bias was visualized by funnel plots. All statistical analyses were executed using RevMan5 (Copenhagen, Denmark). 19
Results
In total, 609 articles were identified in the initial search while 519 subjects were evaluated after duplicates removal. After the exclusion of 378 articles, 32 full texts were assessed for eligibility. Finally, 5 studies were included in the qualitative and quantitative statistical analysis while the remaining were excluded due to the reasons presented in Figure 1.9
–11,20,21 Four out of 5 included studies reported data on all TV outcomes following BEVAR during follow-up (17 months, range = 12–35 months). The mean age of the patients was 70.8 years (range = 63–81 years) and 49.5% were males (325/656). In total, 2359 vessels were catheterized via fenestrations and branches. From them, 1406 were revascularized using branches and were included in the current analysis. Regarding stent type, 547 (38.9%) TVs were treated with BESG while the remaining (859, 61.1%) using SESG. The specific stent type applied in each case is presented in Supplementary Table 4 (Panel A). The main characteristics of the analyzed studies and the commercial type of stent used, as well as the distribution of relining between the two groups and among TVs, are presented in
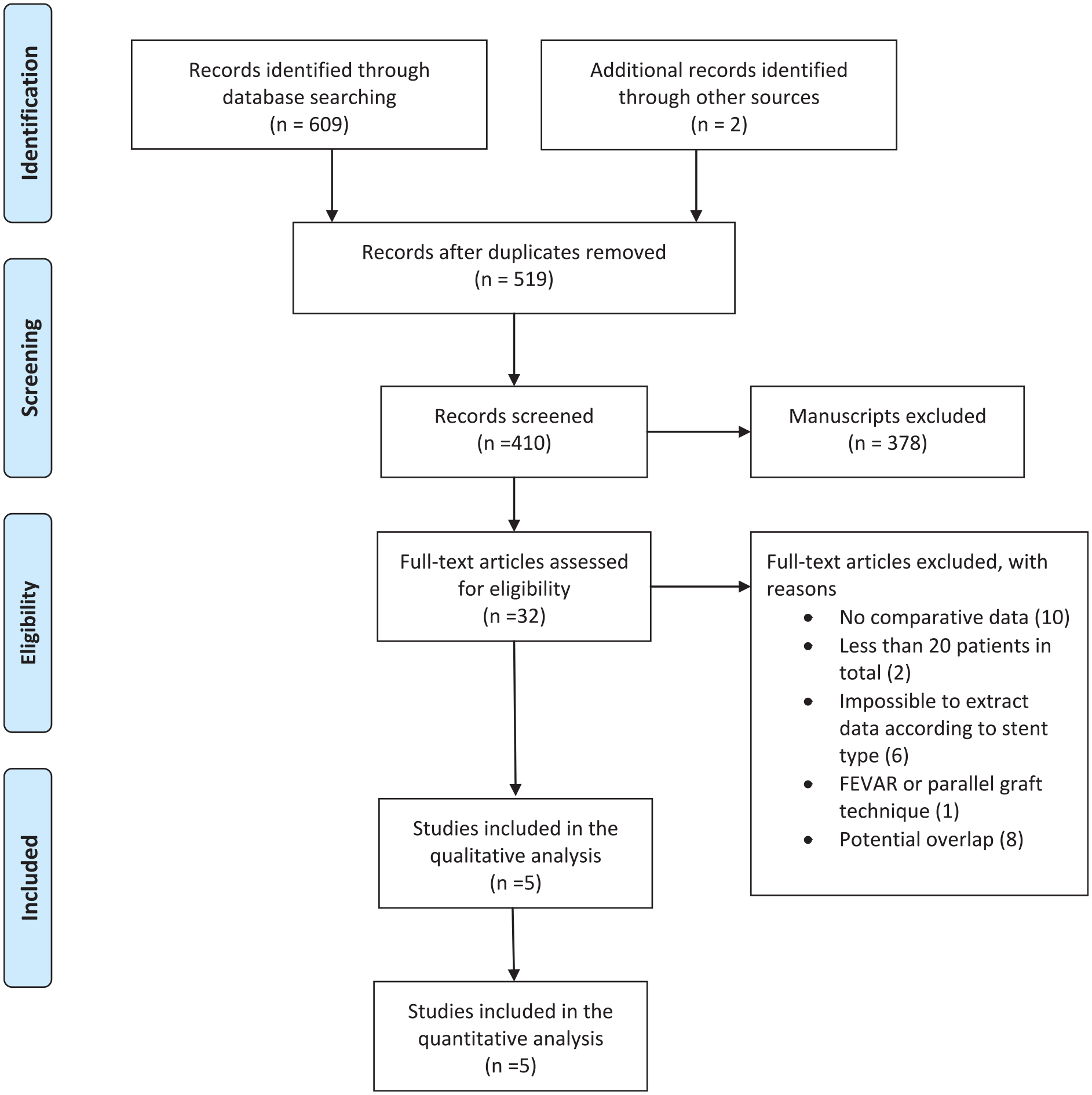
The flow chart of the selection process according to PRISMA statement. Five studies were finally included in the systematic review and meta-analysis.
Included Studies’ Main Characteristics.
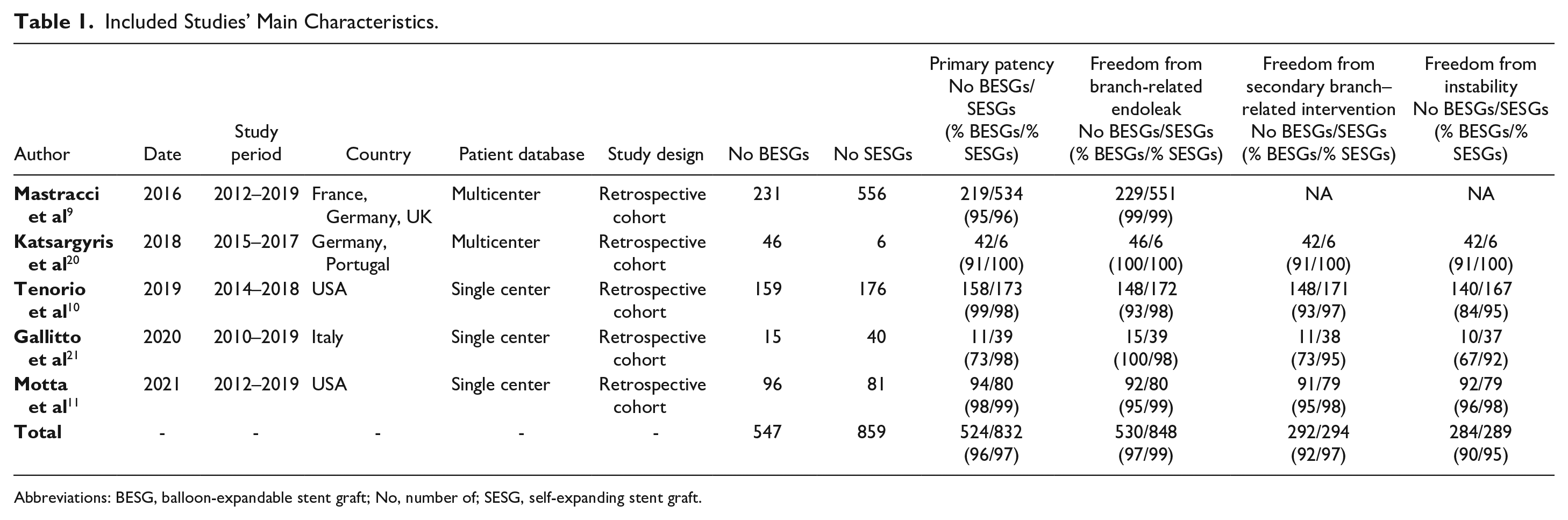
Abbreviations: BESG, balloon-expandable stent graft; No, number of; SESG, self-expanding stent graft.
Material Distribution Among Studies Including Stent Type and Platform Type.
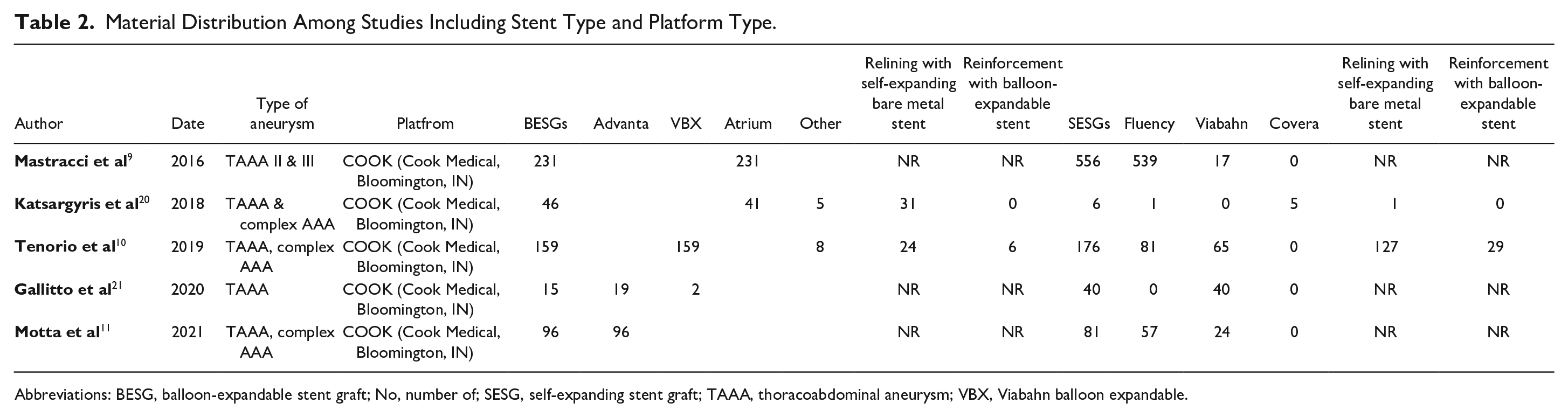
Abbreviations: BESG, balloon-expandable stent graft; No, number of; SESG, self-expanding stent graft; TAAA, thoracoabdominal aneurysm; VBX, Viabahn balloon expandable.
Primary Patency
All 5 studies were included in patency analysis.9 –11,20,21 In total, 524 (96%) TVs remained patent using BESG (95% CI, 0.93–0.99, I2=73.09%, p<.001) and 832 (97%) using SESG (95% CI, 0.96–0.99, I2=35.2%, p<.001). The overall pooled primary patency rate did not differ between groups (odds ratio [OR], 0.40; 95% CI, 0.29–1.09; p=0.256, Figure 2A). A low heterogeneity across studies was evident (I2=4.24%, p=0.259, Figure 2B).
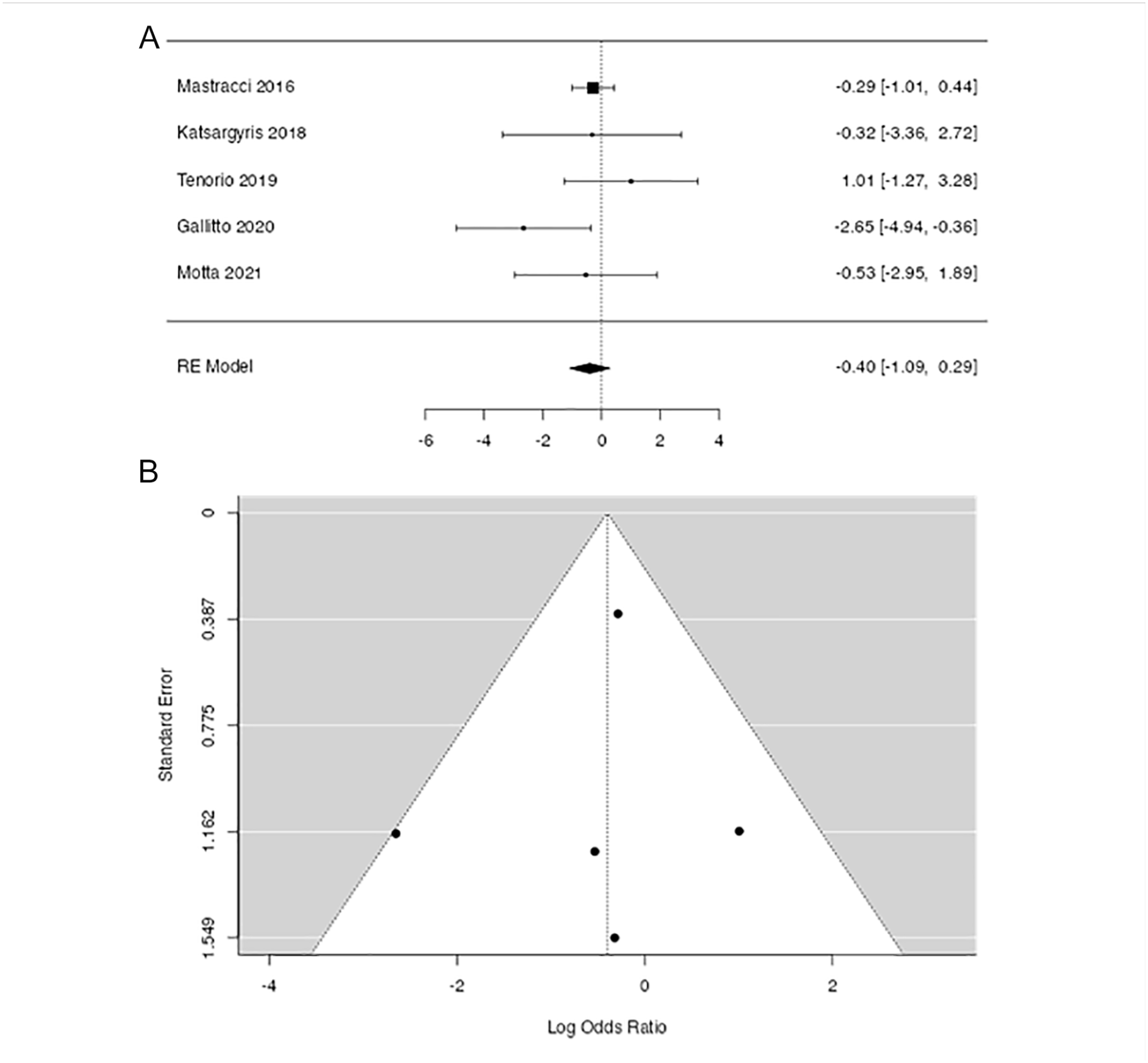
Forest plot of the primary patency between self-expanding (SESGs) and balloon-expandable (BESGs) stent grafts (Panel A) and the associated heterogeneity observed among studies (Panel B).
Freedom From Endoleak
All 5 studies were included in this subanalysis.9 –11,20,21 From 547 TVs that were revascularized using BESG, 530 (97%) presented freedom from endoleak (95% CI 0.95–1.00, I2=64.58, p<.001) while in the SESG (859 stents), 848 (99%) presented freedom form endoleak (95% CI 0.98–1.00, I2=0%, p<.001), without presenting a significant difference between the two groups (OR, 0.65; 95% CI, 0.17–1.48; p< .122, Figure 3A). There was a low heterogeneity among studies (I2=0.18%, p=0.467, Figure 3B).
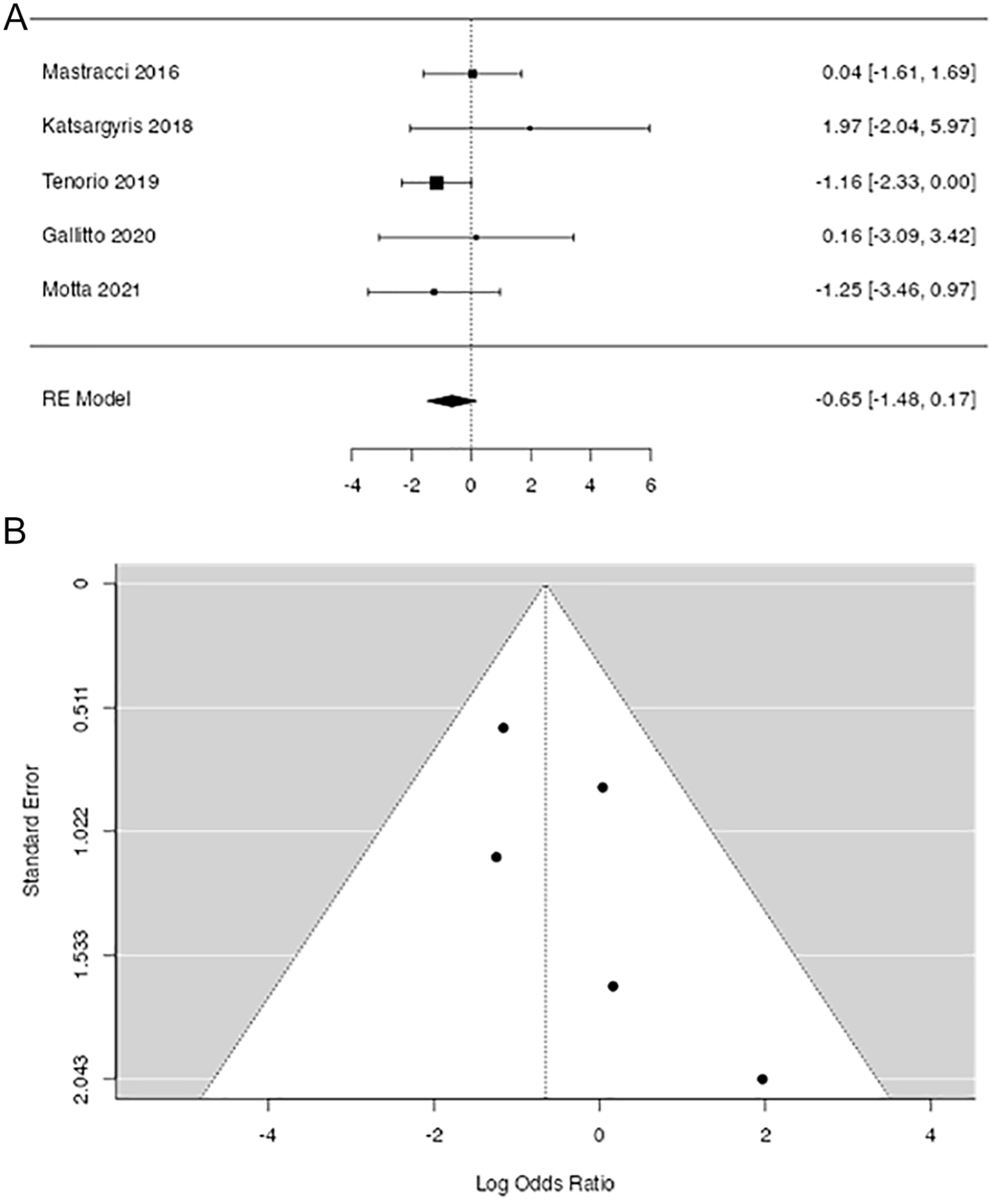
Forest plot of branch-related endoleak between self-expanding (SESGs) and balloon-expandable (BESGs) stent grafts (Panel A) and the associated heterogeneity observed among studies (Panel B).
Freedom From TV Instability
The subgroup analysis for TV instability between BESGs and SESGs included 619 TVs (316 BESG and 303 SESG) in which 573 vessels remained free from instability (284 BESG and 289 SESG).10,11,20,21 In the BESG group, the estimated freedom from instability was 91% (95% CI, 0.85–0.96; I2=64.44%, p<.001) and in the SESG group, 96% (95% CI, 0.93–0.98; I2=3.54%, p<.001). TVs being revascularized using SESG stents presented lower risk for instability in comparison with BESG (OR, 0.99; 95% CI, 0.33–1.65, p=.003, Figure 4A), with no heterogeneity observed among studies (I2=0%, p=0.679, Figure 4B).
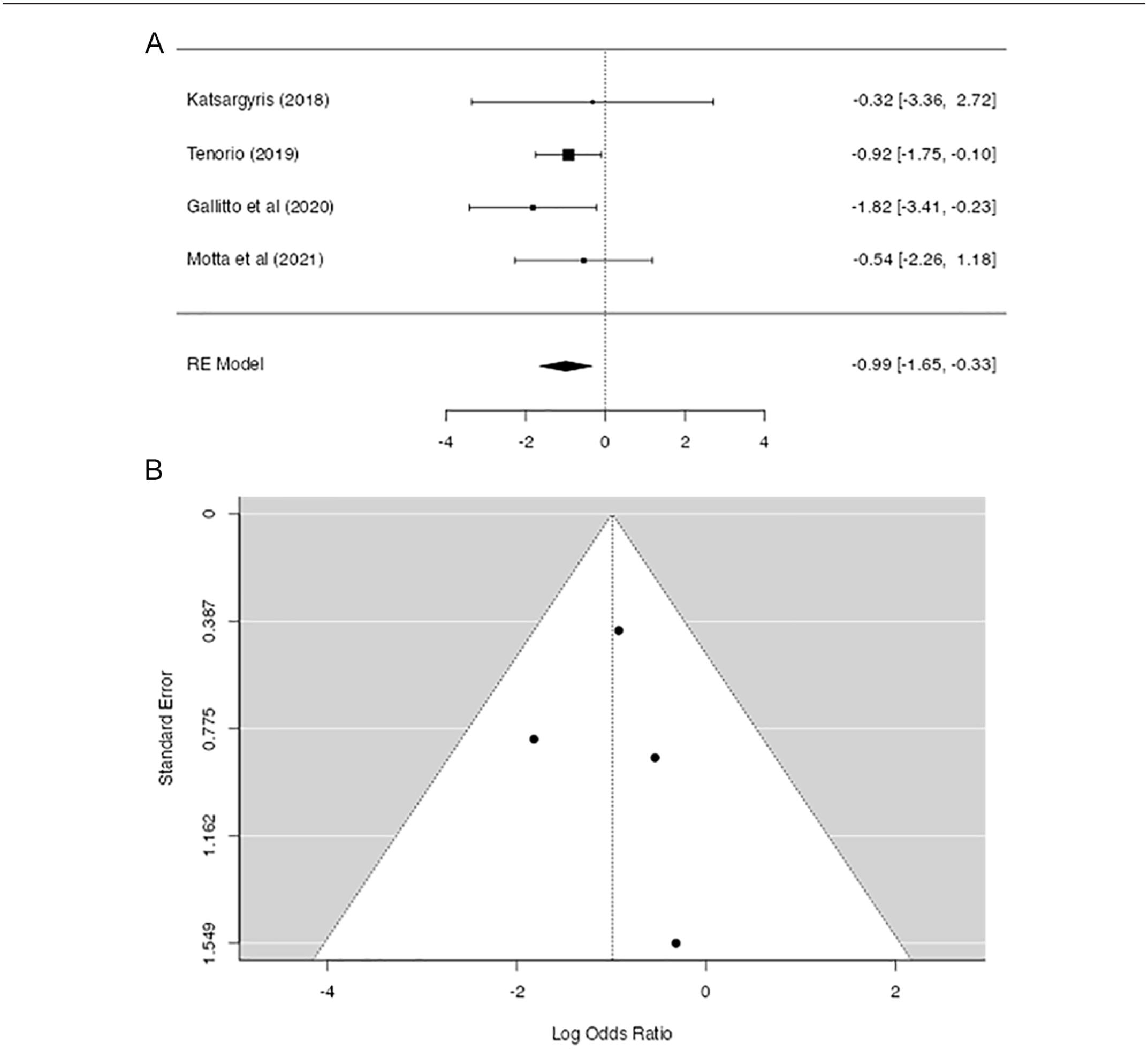
Forest plot of freedom from target vessel (TV) instability of bridging stents according to stent graft type (Panel A) and the heterogeneity across studies (Panel B).
Freedom From Secondary Intervention
Among 4 studies, including 619 TVs (316 BESG and 303 SESG), 586 did not require a secondary intervention (292 BESG and 294 SESG).10,11,20,21 In the BESG group, the estimated freedom from re-intervention was 95% (95% CI, 0.90–0.99; I2=0.19%, p<.001) and in the SESG, 97% (95% CI, 0.95–0.99, I2=0%, p<.001). The comparative analysis showed that SESG required fewer secondary interventions (OR, 1.04; 95% CI, 0.23–1.83; p=.009, Supplementary Figure 1A). A low heterogeneity among studies was noted (I2=0%, p=0.736, Supplementary Figure 1B).
Risk of Bias
Three studies were found to be at a “high” risk of bias11,20,21 with less than 7 stars while 2 studies were found to be at “low” risk of bias according to NOS.9,10 Individual studies were attributed a higher risk of bias in cases of inadequate representative study population, lack of additional important factors, and not reported loss to follow-up or inadequate surveillance period (Supplementary Table 5).
Discussion
BEVAR has been widely used for the treatment of complex aortic pathologies with acceptable technical and clinical outcomes.1,2,22,23 Currently available stent grafts, self-expanding or balloon-expandable, are not originally designed as bridging stents for complex aortic repair with fenestrated or branched devices. 24 Bridging stent selection is usually based on the discretion of the operator taking into account patient and intraoperative characteristics as well as availability in each department.24,25,26 This choice has many procedural implications including the number of stents needed, access routes, and profile of access sheaths. The technical and clinical success of BEVAR is not only associated to the main endograft, but also to the bridging stent graft, as TV complications affect the post-operative course and mortality rates.7,24,27
In the current analysis, both stent graft types, BESG and SESG, showed good outcomes with a primary patency rate at 95%, while freedom from branch-related endoleak was 97% for both covered stent types. In contrast, TV instability, re-intervention, and intra-operatively relining rates were higher for BESGs, indicating a stent-design impact on procedural outcomes.20,24 The limited data do not permit a safe association of the specific BESG to the related adverse event (Supplementary Table 4, Panel B). Design characteristics of BESG may affect TV instability, with renal stents being at higher risk for occlusion.8,9 BESGs and SESGs may differ in rigidity, which may account for an inability to absorb the kinetic forces during respiration, and TV angulation and tortuosity.7,9,10,25 In this analysis, only covered stents were used as bridging stents, while bare metal stents were used only for relining due to stenosis or important angulation remarked intra-operatively. The use of bare metal stents does not seem ideal in case of branched device as the risk for endoleak and intimal proliferation may drive to a higher need for re-intervention during follow-up. 26 New designs may differ from early generations and offer more flexibility with a less frequent need for relining. 27
Relining of a bridging stent graft with an uncovered stent may provide additional biomechanical characteristics to the branch, affecting the outcome. In this analysis, 14% of the BESGs and 10% of the SESGs were relined using bare metal self-expanding stents, while 3.4% of the SESGs were re-enforced with a balloon-expandable stent.10,20 Conflicting data exist regarding the role of relining.10,27 Combining both stent graft types represents another option and has been proposed to offer advantages. 28 It is of note that in the current meta-analysis, more than 30% of BESGs were Viabahn Balloon-Expandable stents (W. L. Gore and Associates, Flagstaff, AZ), a newer generation BESGs with high primary patency and freedom from re-intervention and instability rates (Supplementary Table 4).11,29 –32 However, even with the application of these newer BESGs and despite the promising results, the available data in the literature remain conflicting when compared with SESGs. 10
SESGs were used as bridging stents since the initial reports and the estimated patency was >95%. 33 However, it should be noted that they were re-inforced using balloon-expandable stents and the role of each stent type on TV patency cannot be clarified. 33 Later data on SESGs supported these findings by reporting a primary patency at 95%. 34 Regarding BESGs, the available experience has shown high primary patency rate achieving 100% with low endoleak and re-intervention rate.18,35 Currently available literature has shown that both stent types can be safely and effectively applied during BEVAR, and this meta-analysis is in accordance with the primary patency and endoleak rates of the literature in both stent types. However, the role of relining and its impact on patency need further investigation. SESGs, in previous reports, have all been relined using bare metal stents and provided a high patency rate. 34 The continuous inner forces of a self-expanding bare metal stent in any bridging stent may augment the total force to the vessel wall and increase patency. However, a stent into stent may eliminate TVs’ lumen diameter. A diameter and angulation threshold for relining, to achieve the optimal benefit, could clarify the questions arising regarding its role.
Limitations
This systematic review and meta-analysis included data across retrospective observational studies reporting on TVs’ outcomes, using BESG and SESG as bridging stents in BEVAR. The methodological quality of the included studies varied considerably. Studies including less than 20 cases were excluded as they would potentially depict the initial experience or a low volume center. This may have affected the outcomes of the current analysis. Furthermore, the different commercial stent types, the increasing use of inner branches instead of standard branches may have affected the outcomes. The lack of information regarding the use of relining as well as the anatomic characteristics of the revascularized TVs and distribution of the events among the different TVs may also have affected the outcomes. Furthermore, long-term data were not available while a subanalysis regarding the brand of stent graft was not mendable in this study.
Conclusion
BESG and SESG seem to perform similarly in terms of primary patency and branch-related endoleak during the mid-term follow-up. Current data from retrospective studies suggest that overall TV instability and re-intervention rates are favorable for SESG as bridging stent grafts in BEVAR.
Supplemental Material
sj-docx-1-jet-10.1177_15266028221083458 – Supplemental material for Meta-analysis of Comparative Studies Between Self- and Balloon-Expandable Bridging Stent Grafts in Branched Endovascular Aneurysm Repair
Supplemental material, sj-docx-1-jet-10.1177_15266028221083458 for Meta-analysis of Comparative Studies Between Self- and Balloon-Expandable Bridging Stent Grafts in Branched Endovascular Aneurysm Repair by Petroula Nana, Konstantinos Spanos, Alexandros Brodis, Giuseppe Panuccio, George Kouvelos, Christian-Alexander Behrendt, Athanasios Giannoukas and Tilo Kölbel in Journal of Endovascular Therapy
Supplemental Material
sj-docx-2-jet-10.1177_15266028221083458 – Supplemental material for Meta-analysis of Comparative Studies Between Self- and Balloon-Expandable Bridging Stent Grafts in Branched Endovascular Aneurysm Repair
Supplemental material, sj-docx-2-jet-10.1177_15266028221083458 for Meta-analysis of Comparative Studies Between Self- and Balloon-Expandable Bridging Stent Grafts in Branched Endovascular Aneurysm Repair by Petroula Nana, Konstantinos Spanos, Alexandros Brodis, Giuseppe Panuccio, George Kouvelos, Christian-Alexander Behrendt, Athanasios Giannoukas and Tilo Kölbel in Journal of Endovascular Therapy
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Tilo Kölbel has intellectual property with Cook Medical. Christian-Alexander Behrendt is chairman of the German Chapter of the Medical Device Epidemiology Network (mdepinet.de). All remaining authors declare no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.