
Abstract
Purpose:
To report 24 month safety and efficacy of the Tack Endovascular System for treatment of post-percutaneous transluminal angioplasty (PTA) infrapopliteal dissections in patients with critical limb-threatening ischemia (CLTI).
Materials and Methods:
The Tack-Optimized Balloon Angioplasty (TOBA) II below-the-knee (BTK) study was a prospective, multicenter, single-arm evaluation of the Tack Endovascular system for post-PTA infrapopliteal dissection repair. Patients with Rutherford Clinical Category (RC) 3 to 5 and a post-PTA dissection(s) of the BTK arteries were enrolled. The 30 day primary safety endpoint was a composite of major adverse limb events (MALE) and all-cause perioperative death (POD). The primary effectiveness endpoint was a composite of MALE at 6 months and 30 day POD. Outcomes were assessed as observational endpoints at 24 months.
Results:
Tack-Optimized Balloon Angioplasty II BTK enrolled 233 patients; all patients had a post-PTA dissection(s) and received ≥1 Tack implant (range, 1–16). Mean age was 74.4±10.0 years and 67.4% were men. Most patients had CLTI (RC 3: 16.3%; RC 4/5: 83.7%). Mean target lesion length was 80±49 mm. Moderate to severe calcium was present in 89 (35.8%) lesions and total occlusions were present in 118 (47.6%) lesions. Kaplan-Meier freedom from MALE at 24 months + POD at 30 days was 92.2% and 24 month freedom from clinically-driven target lesions revascularization was 73.6%. Kaplan-Meier target limb salvage was 95.7% and amputation-free survival was 75.4%. Improvements in functional status and quality of life were observed through 24 months.
Conclusion:
The TOBA II BTK study demonstrated sustained safety and efficacy through 24 months in patients treated for post-PTA dissection(s) of BTK lesions.
Clinical Trial Registration:
ClinicalTrials.gov identifier NCT02942966.
Keywords
Introduction
Peripheral artery disease (PAD) affects >200 million patients worldwide. 1 Critical limb-threatening ischemia (CLTI) is the most severe manifestation of PAD and is characterized by lower extremity rest pain, ulceration, gangrene, and a marked decrease in quality of life (QoL).2,3 Critical limb-threatening ischemia is a complex disease state that is associated with a myriad of comorbidities such as hypertension, diabetes mellitus, chronic kidney disease, and dyslipidemia. Given the complexity of CLTI, the prognosis is poor with an increased risk of cardiovascular events and amputation and a 5 year mortality rate of 50%. 3
Although CLTI is characterized by multisegment disease, a landmark study of CLTI lesion distribution in patients with ischemic foot ulcers demonstrated that the infrapopliteal vessels contained 74% of the hemodynamically significant lesions. 4 Below-the-knee (BTK) lesions are challenging from a treatment perspective as they often present with poor outflow, diffuse disease, chronic total occlusions, and/or with medial calcification. 5 Percutaneous transluminal angioplasty (PTA) remains the standard of care for patients undergoing infrapopliteal endovascular revascularization. 6
The mechanism of PTA relies on mechanical dilatation of the artery which results in controlled dissections in up to 30.7% of infrapopliteal lesions. 7 However, it is expected that the incidence of postangioplasty dissections in the BTK arteries may be even higher, as their detection is hindered by the small vessel diameters and the inherent limitations of angiographic imaging. Although dissections are thought to contribute to acute luminal gain following balloon angioplasty, 8 their occurrence has also been shown to predict procedural complications and restenosis, with more severe dissections associated with worse outcomes.9 –11 Treatment of post-PTA dissections in the infrapopliteal arteries typically involves prolonged secondary balloon inflations and/or placement of a coronary stent, the latter of which remains off-label in the United States and is subject to fracture.12 –14
The Tack Endovascular System was purpose-built for focal repair of post-PTA dissections with the goal of optimizing outcomes following PTA. The self-expanding implants are designed to exert a low outward radial force to create focal tissue apposition with a reduction in metal burden relative to stents due to their short longitudinal length and open-cell design. The 6 and 12 month results from the Tack-Optimized Balloon Angioplasty (TOBA) II BTK study demonstrated that the Tack Endovascular System is safe and effective for treatment of BTK dissection(s) with reasonable rates of major adverse limb events (MALE) + perioperative death (POD), patency, clinically-driven target lesions revascularization (CD-TLR), limb salvage, and wound healing.15,16
In this study, we report the 24 month results of the prospective, multicenter, single-arm TOBA II BTK study which was designed to assess the safety and efficacy of the Tack Endovascular System for localized treatment of post-PTA dissection(s) of the infrapopliteal arteries.
Materials and Methods
The TOBA II BTK study was an early-phase prospective, single-arm, multicenter, open-label, nonrandomized study. The study was performed at 41 clinical centers across the United States, Europe, and New Zealand and was conducted in compliance with the Declaration of Helsinki, International Conference on Harmonization E6—Good Clinical Practice, and ISO 14155. The trial was approved by all relevant Institutional Review Boards or Ethics Committees, and all patients provided informed consent. The study is listed at ClinicalTrials.gov as NCT02942966. The objective of this study was to investigate the safety and effectiveness of the Tack Endovascular System in patients with post-PTA dissection(s) in the mid/distal popliteal, tibial, and peroneal arteries ranging in diameter from 1.5 to 4.5 mm.
Eligibility
Clinical and angiographic inclusion and exclusion criteria were detailed previously. 15 Briefly, patients were eligible for potential enrollment if they received PTA in the mid/distal popliteal, tibial, and/or peroneal arteries. Patients underwent balloon angioplasty with a nondrug coated balloon, inflated to nominal pressure or higher if required to expand any residual waist on the balloon. Post-PTA angiograms were performed and reviewed against the angiographic inclusion/exclusion criteria; if there was significant (>30%) residual stenosis, the lesion was treated with repeat PTA at longer inflation times or increased pressure in accordance with the investigator’s decision. If post-PTA angiography demonstrated a resulting dissection(s) that the investigator evaluated as requiring repair and would otherwise have treated by some other means (such as, but not limited to, additional angioplasty with extended inflation time, or stenting), the patient was then considered eligible for enrollment.
Study Procedure
The Tack Endovascular System consists of self-expanding nitinol implants, each measuring 6 mm in length. The short longitudinal length in combination with an open-cell design functions to minimize the amount of metal in contact with the artery. The Tack implant (Figure 1) is designed to treat dissections by exerting a low outward radial force upon the vessel wall to create focal tissue apposition across the range of reference vessel diameters from 1.5 to 4.5 mm.
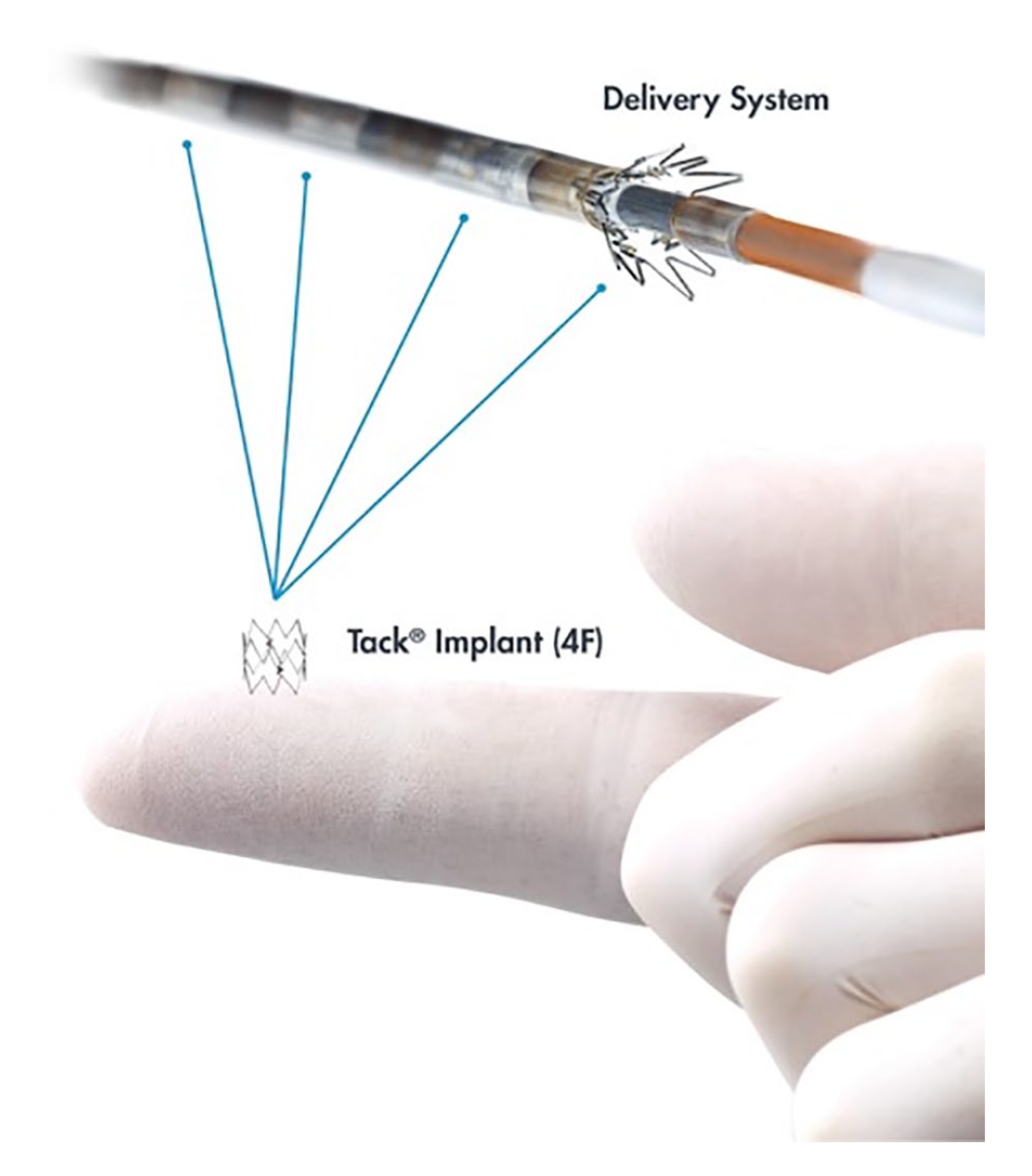
Tack implant and Tack Endovascular System (4F).
Four independent Tack implants were provided preloaded onto a 4F delivery catheter with an outer diameter of 1.33 mm. Following angiographic identification of a dissection, the delivery catheter was loaded onto the 0.014″ guidewire used during the PTA procedure. Utilizing fluoroscopic guidance with magnification, the device was advanced to the treatment site. Tacks were then deployed along the dissected segment(s), moving in a distal-to-proximal direction. Postdilation of each Tack was required, and angiography was utilized to confirm acute vessel patency. In the event of a suboptimal result, bailout stenting was permitted (or as otherwise required for the safety of the patient).
Follow-up
Clinical follow-up was performed at 30 days and 6, 12, and 24 months with planned follow-up through 36 months.
Study Endpoints and Definitions
The primary safety endpoint was defined as MALE at 30 days + POD at 30 days. Major adverse limb event was defined as any above-ankle target limb amputation, and/or major reintervention to the target lesion(s) (defined as placement of a new bypass graft, jump/interposition graft revision, or performance of thrombectomy/thrombolysis). Perioperative death was defined as all-cause death occurring during or within 30 days after the index procedure. The primary effectiveness endpoint was defined as freedom from MALE at 6 months + POD at 30 days. Safety and efficacy were assessed at 12 and 24 months as observational endpoints.
Additional observational endpoints included target limb salvage, amputation-free survival, CD-TLR, changes in Rutherford Clinical Category (RC), ankle-brachial index (ABI), toe-brachial index (TBI), and QoL metrics.
Safety outcomes were adjudicated by an independent Clinical Events Committee (CEC), while a Data Safety Monitoring Board provided periodic review and oversight of patient safety and scientific integrity of the trial. Independent core laboratories reviewed all angiograms, X-rays (Yale Cardiovascular Research Group; New Haven, Connecticut), and duplex ultrasounds (VasCore, Massachusetts General Hospital; Boston, Massachusetts) performed during the study.
Statistical Analyses
All patients who had the Tack Endovascular System advanced through the introducer sheath were assigned to the intent-to-treat population. Intent-to-treat patients were included in all endpoint analyses. Endpoints were analyzed using descriptive statistics. Mean, standard deviation, and sample size are provided for continuous variables; when the mean was not an appropriate measure of central tendency, alternative statistics such as median were considered. For categorical variables, the percentage of patients having or experiencing the event is presented along with the actual number of patients experiencing the event and sample size. Kaplan-Meier estimates were used to evaluate time to event data for freedom from MALE + POD, freedom from CD-TLR, target limb salvage, and amputation-free survival. Statistical analyses were performed using SAS software (version 9.4; SAS Institute, Cary, North Carolina).
Results
Patient and Lesion Characteristics
Tack-Optimized Balloon Angioplasty II BTK enrolled 233 patients at 41 sites in the United States, Europe, and New Zealand. Patient enrollment and follow-up through 24 months are illustrated in Figure 2. Baseline patient and clinical characteristics were published previously 16 and are summarized in Supplemental Table 1. Briefly, mean age was 74.4±10.0 years and 67.4% were men. Critical limb-threatening ischemia patients comprised 83.7% (195/233) of the study population, with 50.2% (117/233) classified as RC 5, 33.5% (78/233) as RC 4, and 16.3% (38/233) as RC 3. High rates of diabetes (153/233, 65.7%), smoking (145/233, 62.2% current or former), and chronic kidney disease (57/232, 24.6%) were present.
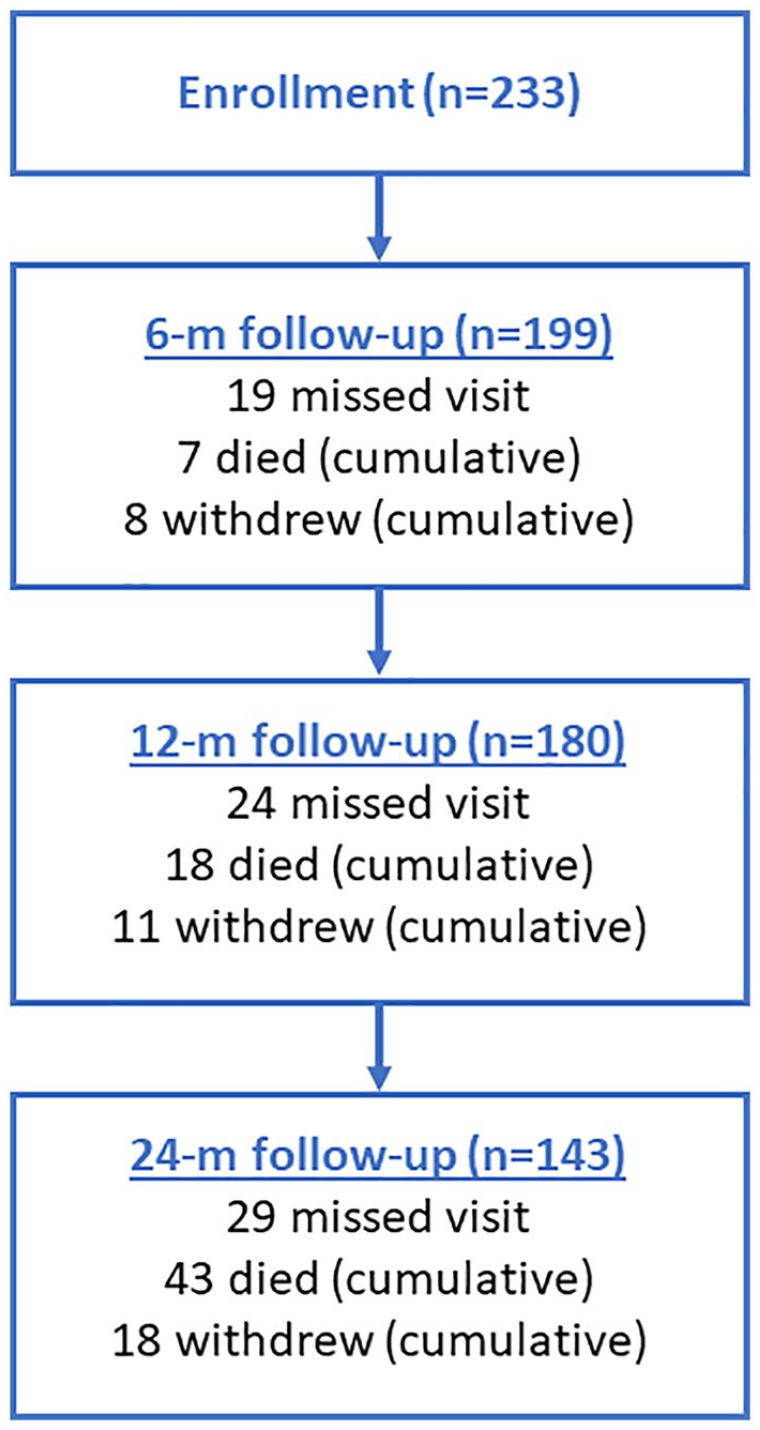
Patient enrollment and follow-up. M, month.
Angiographic and procedural characteristics as adjudicated by the core laboratory were published previously 16 and are summarized in Supplemental Table 2. In brief, moderate to severe calcium was present in 35.8% (89/248) lesions and total occlusions comprised 47.6% (118/248) of lesions. Percutaneous transluminal angioplasty-treated length was 154±110 mm. Reference vessel diameter was 3.5±1.0 mm proximally and tapered to 2.6±0.7 mm distally. Standard PTA was performed in 248 target lesions, resulting in 341 post-PTA dissections requiring repair. Lesions were located in the mid/distal popliteal and tibial arteries with the majority in the anterior tibial (41.5%, 103/248), posterior tibial (22.2%, 55/248), and peroneal arteries (21.4%, 53/248). The worst dissection per patient was grade A in 21.4%, grade B in 39.3%, grade C in 11.8%, grade D in 26.6%, and grade E in 0.9%. The mean number of Tacks deployed to treat the dissections was 4.0±2.8 implants per patient.
The 6 and 12 month safety, efficacy, and observational endpoints have been reported previously.15,16 Here, we present the results through 24 months. Select patient results have been stratified according to baseline RC to observe the differences in outcome between claudicants and patients with CLTI.
Freedom From MALE + POD
As shown in Figure 3A, Kaplan-Meier freedom from MALE at 24 months + POD at 30 days was 92.2% overall, and 100% and 90.5% for baseline RC 3 and RC 4/5 patients, respectively.
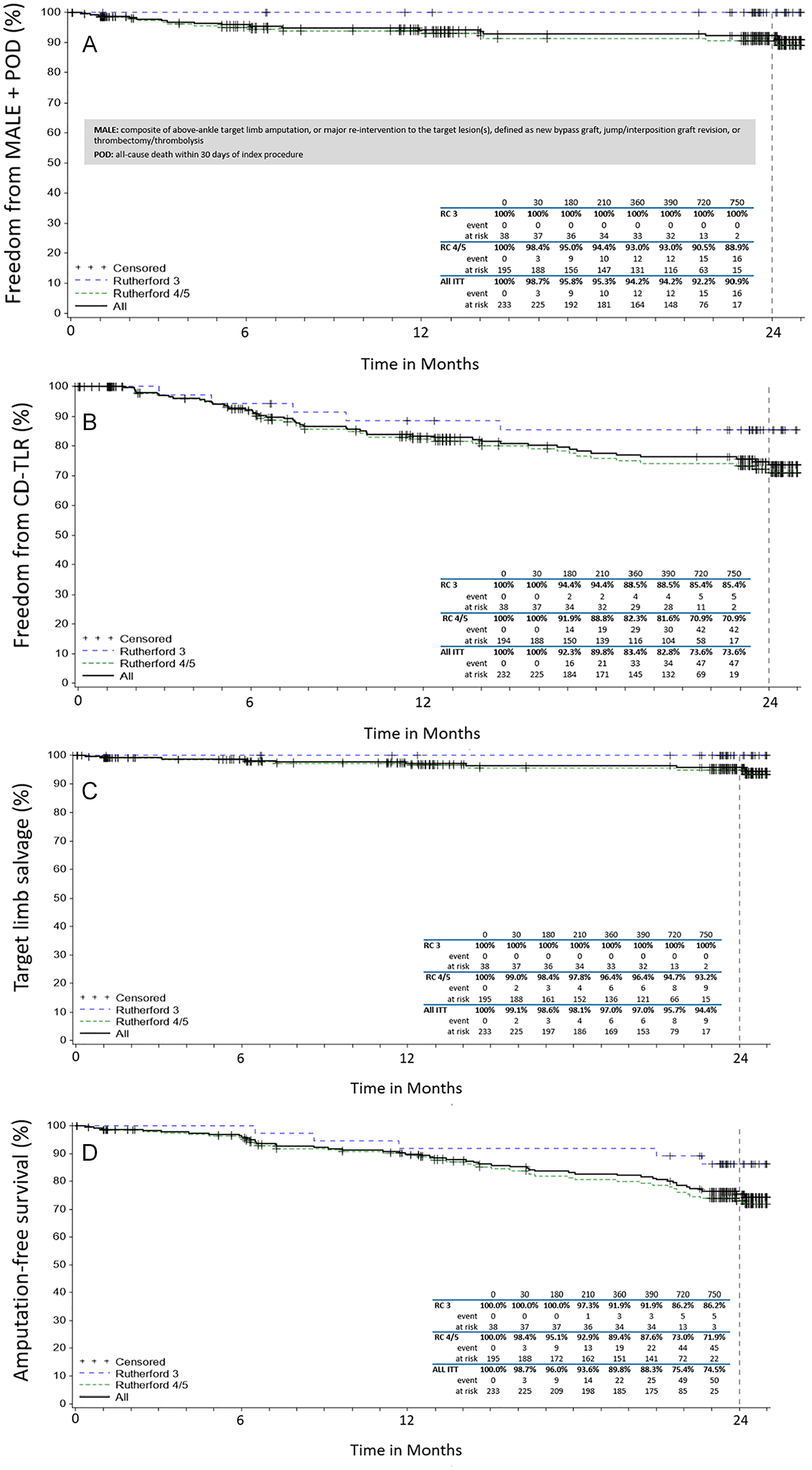
Kaplan-Meier curves for (A) freedom from major adverse limb events (MALE) + perioperative death (POD), (B) freedom from clinically-driven target lesion revascularization (CD-TLR), (C) target limb salvage (TLS), and (D) amputation-free survival (AFS) in intent-to-treat (ITT) individuals through 24 months. RC, Rutherford Category.
Freedom From CD-TLR and CD-TVR
Twenty-four month Kaplan-Meier freedom from CD-TLR was 73.6% in all patients, 85.4% for baseline RC 3, and 70.9% for baseline RC 4/5 patients (Figure 3B). Kaplan-Meier freedom from CD-TVR at 24 months was 73.1% in all patients.
Target Limb Salvage
At 24 months, Kaplan-Meier target limb salvage (Figure 3C) was 95.7% overall, and 100% for baseline RC 3 and 94.7% for baseline RC 4/5 patients, respectively.
All-Cause Mortality and Amputation-Free Survival
At 24 months, Kaplan-Meier survival in all patients was 78.0%. There were 43 patient deaths through 24 months, all reviewed by the CEC. No deaths were determined to be attributable to the Tack Endovascular System. Amputation-free survival (Figure 3D) was 75.4% overall, 86.2% in RC 3 and 73.0% in RC 4/5 patients. A total of 9 major amputations were reported through 24 months, and none occurred in the baseline claudicant population.
Changes in Functional Status
Significant and sustained hemodynamic improvement was seen in ABI and TBI from baseline through 24 months (Figure 4). The average TBI at 24 months was 0.65±0.39, compared with the baseline mean of 0.43±0.23 (p<0.0001), with similar improvement in ABI (0.90±0.19 at 24 months and 0.74±0.27 at baseline [p<0.0001]) (Figure 4). Sustained improvement in RC was reported in 86.9% (126/145) of patients, with 66.2% (96/145) improving ≥3 classes (p<0.0001).
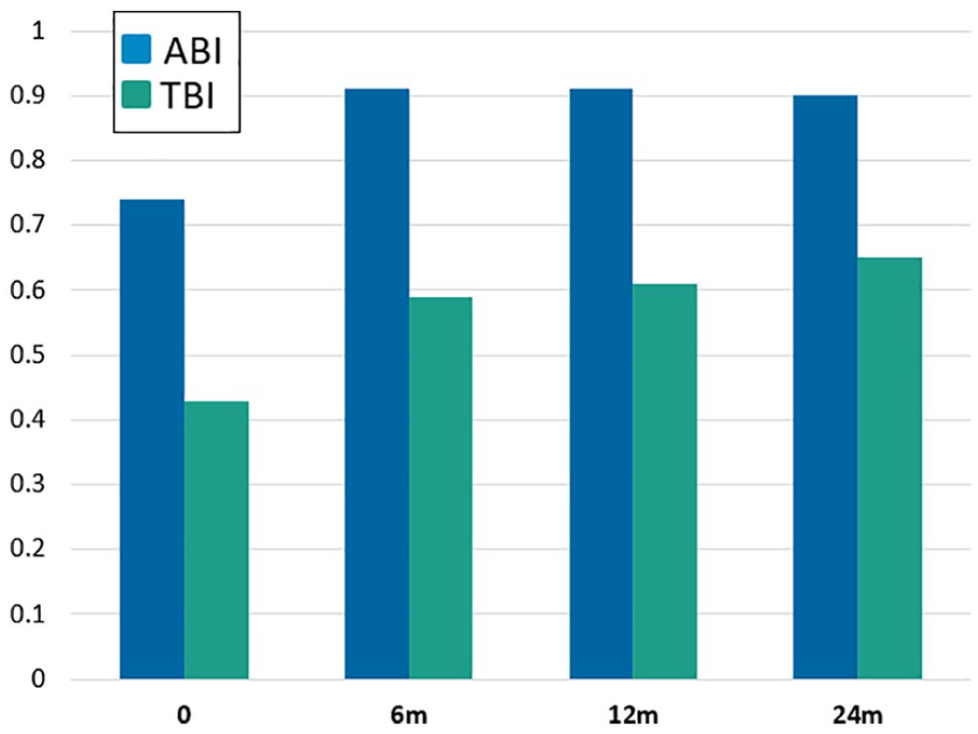
Sustained improvement in ankle-brachial index (ABI) and toe-brachial index (TBI) through 24 months. M, month.
Changes in Patient-Reported QoL Measures
Patients reported improvement in QoL through 24 months in the EQ-5D-3L assessment, with decreased limitations in pain/discomfort (p<0.0001) and increased overall health in the EQ-visual analogue scale scores (p=0.0035). Significant and sustained improvement in Walking Impairment Questionnaire (WIQ) was seen across all categories: distance, speed, stair, and overall (p<0.0001).
Discussion
The 24 month results of the TOBA II BTK study demonstrated durable safety and efficacy of the Tack Endovascular System for treating post-PTA dissections in CLTI patients with BTK lesions. Twenty-four month freedom from MALE + 30 day POD was 92.2% overall, while it was 90.5% for patients with CLTI (RC 4/5). Freedom from CD-TLR through 24 months was 73.6% for all BTK patients and 70.9% in those with CLTI. Target limb salvage was 95.7% overall and 94.7% in the CLTI population. Freedom from all-cause mortality was 78.0% overall, and a total of 9 major amputations were reported through 24 months. These robust outcomes were also associated with increased patient-reported overall health and WIQ QoL scores. These data demonstrate an important role for the Tack Endovascular System in post-PTA dissection repair of the infrapopliteal arteries, particularly in patients with CLTI.
Currently, PTA remains the gold standard for minimally invasive treatment of infrapopliteal arterial disease. However, long-term efficacy with PTA has been shown to be variable with most studies reporting 1 year patency and repeat revascularization rates ranging from around 50% to 80%. 17 It has been shown that post-PTA dissections are known to contribute to suboptimal results.9,10 The Tack Endovascular System technology was intended to help optimize and potentially improve the long-term outcomes of PTA. Tacks exert a low radial force and combined with an open-cell design and smaller longitudinal length, they are designed to overcome many of the limitations of bare metal and drug-eluting stents. Tack was originally shown to be safe and effective for post-PTA dissection repair above the knee18 –20 and was later expanded for evaluation in the infrapopliteal arteries.15,16,21 The 4F Tack Endovascular system was approved for post-PTA dissection repair in the mid/distal popliteal, tibial, and peroneal arteries ranging in diameter from 1.5 to 4.5 mm in April 2020.
Regulatory approval of the Tack Endovascular System for the treatment of BTK lesions was based on the 6 month results of the pivotal TOBA II BTK study, which met primary safety and effectiveness objective performance goals. 15 The 6 month results showed favorable rates of MALE + POD, patency, CD-TLR, and limb salvage, 15 all of which were sustained through 12 months. 16 Improvements in RC and wound status were also observed at both 6 and 12 months.15,16 The updated 24 month analyses presented herein continue to build on the safety and efficacy of the TOBA II BTK clinical study, demonstrating sustained MALE + POD, freedom from CD-TLR, high amputation-free survival and target limb salvage, and sustained improvements in RC, ABI, and TBI. Per study design, follow-up will continue through 36 months.
The results of the TOBA II BTK study are substantiated by additional studies which evaluated Tack performance in the infrapopliteal arteries. In the prospective, single-arm TOBA BTK pilot study (N=35) published by Brodmann et al, 21 procedural success was achieved in 97.1% and there were no MALEs reported through 30 days. The patency (by lesion) and freedom from CD-TLR rates at 12 months were 78.4% and 93.5%, respectively. Significant improvements in RC were also observed and 75% of patients improved 4 or 5 categories. In a single-center, real-world study (N=51) by Lichtenberg and colleagues, 22 the Tack Endovascular System was utilized to repair dissection following above-the-knee or BTK revascularization with balloon angioplasty (plain or drug-coated), atherectomy, and/or lithotripsy. Technical success was reported in 98.3% of the 60 dissections in which Tack was deployed and no major adverse events or device-related complications occurred during the procedure. Collectively, these studies support the safety and efficacy of the Tack Endovascular System for focal dissection repair in the infrapopliteal arteries.
Recent studies have been launched in the United States to evaluate the safety and efficacy of purpose-built stents for the treatment of BTK disease in CLTI patients. The SAVAL Pivotal trial is a randomized study that is enrolling CLTI patients with infrapopliteal lesions to compare the nitinol self-expanding, paclitaxel-coated SAVAL BTK Vascular Stent System with PTA. 23 A single-arm study will begin after completion of enrollment in the RCT and will aim to assess additional safety and efficacy data following implantation of the SAVAL Stent. In addition, the safety and efficacy of the self-expanding nitinol MicroStent System compared with PTA is being assessed in CLTI patients with infrapopliteal disease. 24 Finally, the LIFE-BTK randomized controlled trial is a premarket clinical safety and efficacy evaluation of the everolimus-eluting resorbable Esprit BTK System compared with PTA for the treatment of CLTI patients with BTK lesions. 25 It is the first investigational device exemption trial in the United States to assess a fully resorbable device in the infrapopliteal arteries. Forthcoming data from each trial will be important in determining the future role of these BTK devices in treating patients with infrapopliteal lesions in the United States. Currently, the purpose-built 4F Tack Endovascular System remains the only scaffold approved by the Food and Drug Administration for use in the infrapopliteal arteries.
Limitations
Limitations of the TOBA II BTK study include the nonrandomized and single-arm design which was necessary due to the lack of a device that could serve as a direct comparator. Furthermore, the TOBA II BTK study enrolled patients who were RC 3 to 5 and excluded patients who were RC 6; therefore, the results of this study may not be directly generalizable to CLTI patients with major tissue loss.
Conclusion
The purpose-built Tack Endovascular System demonstrated sustained safety and efficacy through 24 months for treatment of post-PTA dissection in CLTI patients with infrapopliteal lesions. Outcomes were also associated with improvements in Rutherford classification and patient-reported QoL. These data demonstrate an important role for the Tack Endovascular System in post-PTA dissection repair of the infrapopliteal arteries, particularly in the setting of CLTI.
Supplemental Material
sj-docx-1-jet-10.1177_15266028221083462 – Supplemental material for Twenty-Four Month Results of Tack-Optimized Balloon Angioplasty Using the Tack Endovascular System in Below-the-Knee Arteries
Supplemental material, sj-docx-1-jet-10.1177_15266028221083462 for Twenty-Four Month Results of Tack-Optimized Balloon Angioplasty Using the Tack Endovascular System in Below-the-Knee Arteries by George L. Adams, Michael Lichtenberg, Christian Wissgott, Andrej Schmidt, Trisha Tarra, Shannon Matricardi and Patrick J. Geraghty in Journal of Endovascular Therapy
Supplemental Material
sj-docx-2-jet-10.1177_15266028221083462 – Supplemental material for Twenty-Four Month Results of Tack-Optimized Balloon Angioplasty Using the Tack Endovascular System in Below-the-Knee Arteries
Supplemental material, sj-docx-2-jet-10.1177_15266028221083462 for Twenty-Four Month Results of Tack-Optimized Balloon Angioplasty Using the Tack Endovascular System in Below-the-Knee Arteries by George L. Adams, Michael Lichtenberg, Christian Wissgott, Andrej Schmidt, Trisha Tarra, Shannon Matricardi and Patrick J. Geraghty in Journal of Endovascular Therapy
Footnotes
Acknowledgements
The authors wish to thank the following investigators who participated in Tack-Optimized Balloon Angioplasty II below-the-knee study: Patrick J. Geraghty, MD, St. Louis, MO; Joseph Cardenas, MD, Yuma, AZ; Michael Lichtenberg, MD, Arnsberg, Germany; Christian Wissgott, MD, Heide, Germany; Klaus Hertting, Buchholz, Germany; Ehrin Armstrong, MD, Aurora, CO; Marcus Thieme, MD, Sonneberg, Germany; Zoltan Ruzsa, MD, Kecskemet, Hungary; Robert Staffa, MD, Brno, Czech Republic; Jaafer Golzar, MD, Oak Lawn, IL; Marianne Brodmann, MD, Graz, Austria; Andrew Holden MD, Auckland, New Zealand; Nicolas Shammas, MD, Davenport, IA; Vaqar Ali, MD, Jacksonville, FL; George Adams, MD, Raleigh, NC; Jeffrey Carr, MD, Tyler, TX; Nelson Bernardo, MD, Washington, DC; Jon George, MD, Philadelphia, PA; Ashit Jain, MD, Fremont, CA; John Rundback, MD, Teaneck, NJ; Andrew Klein, MD, Atlanta, GA; Muhammad Khan, MD, McKinney, TX; Gary Ansel, MD, Columbus, OH; Sundeep Das, MD, St. Louis, MO; Peter Soukas, MD, Providence, RI; Craig Walker, MD, Houma, LA; Gaurav Aggarwala, MD, Huntsville, TX; Rahul Bose, MD, New Braunfels, TX; Klaus Brechtel, MD, Berlin, Germany, Bryan Fisher, MD, Nashville, TN; Sashi Kilaru, MD, Cincinnati, OH; Bela Merkley, MD, Budapest, Hungary; Robert Attaran, MD, New Haven, CT; Jack Chamberlin, MD, Elk Grove Village, IL; Thomas Davis, MD, Detroit, MI; Gabriel Delgado, MD, Matthews, NC; David Dexter, MD, Norfolk, VA; Richard Kovach, MD, Browns Mills, NJ; Siddhartha Rao, MD, Cary, NC; Andrej Schmidt, MD, Leipzig, Germany; Michael Silva, MD, Galveston, TX; and Neil Strickman, MD, Houston, TX
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: G.L.A. is a consultant for Philips. M.L. is a consultant, received grant support for scientific support, and speaker honorarium from Philips. C.W. is a consultant for Intact Vascular/Philips. A.S. is a consultant for Abbott, BD, Boston Scientific, Cook, Cordis, Cryolife, Philips, Reflow Medical, and Upstream Peripheral. T.T. is an employee of Philips. S.M. is an employee of Philips. P.J.G. is a consultant for Becton Dickinson/Bard Peripheral Vascular, and Boston Scientific and Equity/Ownership in Pulse Therapeutics, MedAlliance SA, and Aveera.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Intact Vascular/Philips.
Prior Presentations
These data were previously presented at New Cardiovascular Horizons in New Orleans, LA, on June 3, 2021, AMP in Orlando, FL, on August 12, 2021, and VIVA in Las Vegas, NV, on October 4, 2021.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.