
Abstract
Purpose:
The widespread adoption of endovascular aneurysm repair (EVAR) as preferred treatment modality for abdominal aortic aneurysm (AAA) has enlarged the number of patients needing open surgical conversion (OSC). The relationship between adherence to Instructions For Use (IFU) and EVAR long-term outcomes remains controversial. The aim of this study is to compare preoperative differences and postoperative outcomes between EVAR patients not adjusted to IFU and adjusted to IFU who underwent OSC.
Methods:
This multicenter retrospective study reviewed 33 explanted EVARs between January 2003 and December 2019 at 14 Vascular Units. Patients were included if OSC occurred >30 days after implantation and excluded if explantation was performed to treat an endograft infection, aortic dissection, or traumatic transections. Variables analyzed included baseline characteristics, adherence to IFU, implant and explant procedural details, secondary reinterventions, and postoperative outcomes.
Results:
Fifteen explanted patients (15/33, 45.5%) were identified not accomplished to IFU (out-IFU) at initial EVAR vs 18 explanted patients adjusted (in-IFU). During follow-up, a mean of 1.73±1.2 secondary reinterventions were performed, with more type I endoleaks treated in the subgroup out-IFU: 16.7% vs 6.3% in-IFU patients and more type III endoleaks (8.3% vs 0%). Patients out-IFU had shorter mean interval from implant to explant: 47.60±28.8 months vs 71.17±48. Type II endoleak was the most frequent indication for explantation. Low-flow endoleaks (types II, IV, V) account for 44% of indications for OSC in subgroup of patients in-IFU, compared with 13.3% in patients out-IFU and high-flow endoleaks (types I and III) were the main indication for patients out-IFU (33.3% vs 16.7% in-IFU). Total endograft explantation was performed in 57.5% of cases (19/33) and more suprarenal clamping was required in the subgroup out-IFU. Overall, 30-day mortality rate was 12.1% (4/33): 20% for patients out-IFU and 5.6% in-IFU.
Conclusions:
In our experience, type II endoleak is the most common indication for conversion and differences have been found between patients treated outside IFU with explantation taking place earlier during follow-up, mainly due to high-flow endoleaks and with higher mortality in comparison with patients adjusted to IFU. Ongoing research is required to delve into these differences.
Keywords
Introduction
Endovascular aneurysm repair (EVAR) has become the treatment of choice during the last 2 decades with acceptable short- and long-term results. 1 Despite this, secondary endovascular interventions are needed, between 9% and 15% of these patients,2,3 to maintain its durability. Imaging surveillance along the patient life is required to identify complications as endoleaks, migrations, limb graft thrombosis, or aneurysm sac expansions. When salvage endovascular procedures fail, explantation of the graft and open surgical conversion (OSC) is performed with a significant morbidity and mortality risk. Recent published series on surgical conversion report an average mortality rate of 10% in an elective setting and more than 50% in urgent cases.4,5 The incidence of OSC is increasing over the time with rates varying between 0.67% and 22.8% in some series. 6
Plenty literature 4 in recent years has described technical outcomes after open conversion: surgical approach (transperitoneal or retroperitoneal), clamp location, type of explantation (partial or complete), and postoperative complications. However, there is sparse information about the preoperative factors that might lead to OSC, specifically the relationship between devices Instructions For Use (IFU) compliance, endovascular reintervention, device degenerative phenomena, 7 and their influence to the final OSC indication. Some studies have found IFU nonadherence to be associated with higher rates of early and late endoleaks, aortic sac growth, early reinterventions, and worse long-term survival. 8
The objective of the present retrospective multicenter study is to compare preoperative variables such as implant procedure characteristics, detailed endovascular reinterventions during the surveillance program, and postoperative outcomes between EVAR patients not adjusted to IFU with patients adjusted to IFU who underwent late open conversion.
Materials and Methods
Study Design
A multicenter retrospective national study was designed to identify patients requiring open conversion of previous EVAR, between January 1, 2003 and December 31, 2019. Review Board approval was obtained from all participants’ institution before starting the study. A chart review was designed from previous published protocols and shared between centers that agreed to participate. The project was promoted and disseminated among the members of the CCEV (Spanish Endovascular Surgery Chapter) of the SEACV (Spanish Vascular Surgery Society) with representatives from most of the Vascular Surgery Units of the Spanish territory.
Data and Eligibility Criteria
Open surgical conversion was defined as any transperitoneal or retroperitoneal intervention for aneurysm-related or graft-related complications, with or without endograft explantation. 9 Patients were only included, if the conversion occurred >30 days after implantation. Patients were excluded if the explantation was performed to treat a diagnosed endograft infection, an aortic dissection, or traumatic transections. Based on previous studies,10,11 the 30-day cutoff was selected to exclude early complications of EVARs. The conversion rate is the proportion of explants of the total EVAR performed during the entire inclusion period per hospital. Time to OSC is the time that elapses between implant and explant procedure and was calculated as mean±standard deviation.
Data were collected in 7 categories (Supplemental Table 1). Demographic information included sex, age, duration of implant, conversion rate and comorbidities such as hypertension, diabetes, cerebral ischemia, chronic obstructive pulmonary disease, coronary artery disease, and chronic renal failure. 12 Detailed EVAR implantation procedure information was retrieved from operation notes as aneurysm diameter, device brand, indication of initial EVAR (elective vs urgent repair), EVAR configuration (bifurcated, aorto-uni-iliac), intraoperative device adjuncts (femoro-femoral bypass, ilio-femoral bypass, Palmaz stent, proximal cuffs, etc), and intraoperative endoleaks and before 1 month, treated with or without success. Reviewing pre-implant computed tomographic (CT) images assessed adherence to endograft IFU. The IFU parameters were adjusted to each device brand at the time of deployment as (1) infrarenal neck angulation, (2) neck length, (3) neck calcification, (4) neck thrombus, (5) iliac tortuosity, and (6) iliac diameter. Each patient may have one or more than one criteria of IFU nonadherence to be considered as such. 10
All patients included underwent ultrasound or CT as part of the EVAR surveillance program at 1, 6, 12, 24 months, and then, annually thereafter. The follow-up was considered “partial,” if the patient failed to present at any time during the surveillance program and “complete,” if the patient attended all the scheduled appointments. Detailed information of interventions before referral for conversion was compiled in a fifth category as number of secondary reinterventions, indication, type of endoleaks, technique details of the procedure performed to sort it out, and certitude of success. Widespread endoleaks classification was used13,14 and joined up into 2 categories: high-flow endoleaks (types I and III) and low-flow endoleaks (types II, IV, and V). 15
After secondary endovascular interventions failed, the indication to proceed to conversion was based on the risks of OSC weighed against the risks of rupture, depending on the size of the aneurysm and the type of endoleak. 9 Indication for explantation was classified as endoleak by type, graft migration, aneurysm expansion without endoleak, limb thrombosis, rupture, and combinations of more than one; all concepts based on the definitions stated by the Society for Vascular Surgery reporting standards. 16 Operative technique details for explant procedure were included in a sixth category as aneurysm diameter, surgical approach, clamp position, intraoperative death, and surgical conversion technique. The type of surgical reconstruction varied between 3 options: complete explantation, partial endograft explantation, and those were the endograft itself was not explanted, but open surgical modifications were performed as cerclage of the aortic sac around the main body to treat type I endoleaks, or ligation/clipping of lumbar vessels to treat type II endoleaks. Urgent conversions (<24 hours from presentation) comprised those performed for symptomatic aneurysms, ruptured aneurysm, or stent graft thrombosis.
Postoperative outcomes were recorded with specific attention to those occurring within 30 days: length of hospital stay, 30-day mortality, major complications (myocardial infarction, renal failure, prolonged ventilation, stroke, limb or visceral ischemia, and graft infection), and reinterventions postoperatively.
Statistical Analysis
Data were collected and analyzed using SPSS version 24 software (IBM, Inc., Chicago, Illinois). Continuous data are detailed using descriptive statistics (mean±standard deviation). Other continuous variables were reported as medians with their corresponding interquartile ranges and percentages. Categorical variables were presented as values with percentages. Baseline characteristics were compared by t test (for continuous variables) or Fisher exact test (for categorical variables) or their nonparametric equivalents as appropriate. Analysis of association with 30-day mortality was performed using Pearson χ2 test and Fisher exact test for categorical factors and Wilcoxon rank sum tests for continuous measures. Statistical significance was identified for a p value <.05.
Results
Baseline Patient Characteristics and EVAR Implant Procedure
Fourteen Vascular Surgery Units in Spain agreed voluntarily to participate, representing 70% that perform complex endovascular procedures. From January 2003 to December 2019, 33 patients out of 6.247 EVAR cases required endograft explantation. Thus, the incidence of OSC within these Units ranges from 0.004 to 2.9 with a mean rate of 0.95±0.88.
Endograft adjustment to IFU was independently assessed, with not missing CT of the implant procedure and reviewed in all of the 33 cases. Two subgroups of patients were identified: 15/33 patients (45.5%) not fulfilling the requirements for their specific device instructions to deployment (out-IFU) and 18/33 patients adjusted to the IFU in the primary EVAR (in-IFU). In the out-IFU group, 6 cases had excessive neck angulation and short neck length, 2 cases had neck thrombus or neck calcification that exceeded 50% of the aortic circumference and 15.1% had iliac access problems and 46.6% (7/15) had more than one criteria not adjusted to IFU. No differences in patients’ demographics and comorbidities between both groups were found (Table 1).
Baseline Demographics Characteristics of 33 Patients Who Underwent OSC.
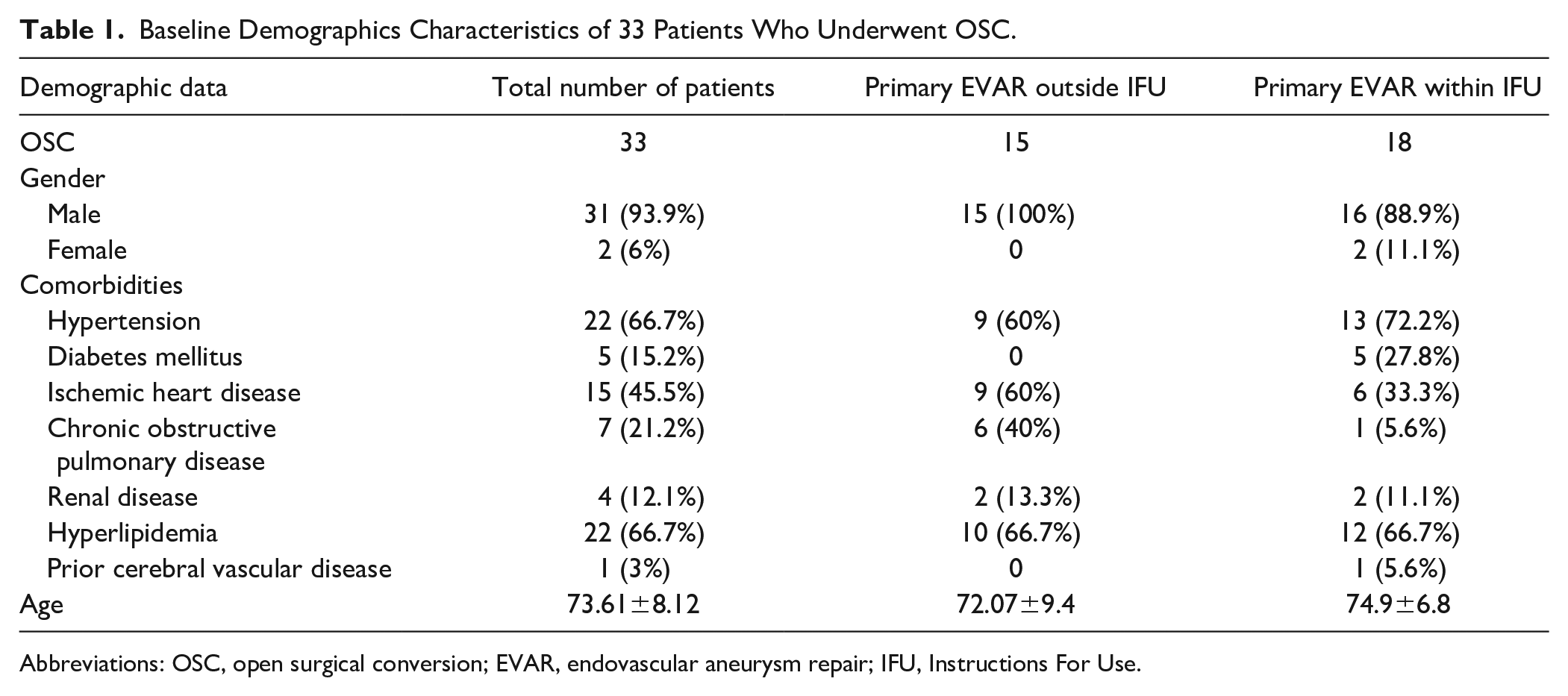
Abbreviations: OSC, open surgical conversion; EVAR, endovascular aneurysm repair; IFU, Instructions For Use.
The majority of patients (n=31, 93.9%) underwent an elective implant procedure, only 2 (6%) was nonelective, being bifurcated stent grafts in 29 (87.9%) of the cases and 4 aortouniliac devices with femoral crossover graft. More stent grafts with suprarenal fixation were deployed in patients outside IFU (93% vs 50% suprarenal fixation in-IFU patients). See type of device brand in Table 2. At implant, intraoperative endoleaks were detected in 9 (27.7%) of the 33 patients, 7 (77.7%) of those were type II endoleaks.
Implant Endograft Procedure Characteristics of 33 Patients Who Underwent OSC.
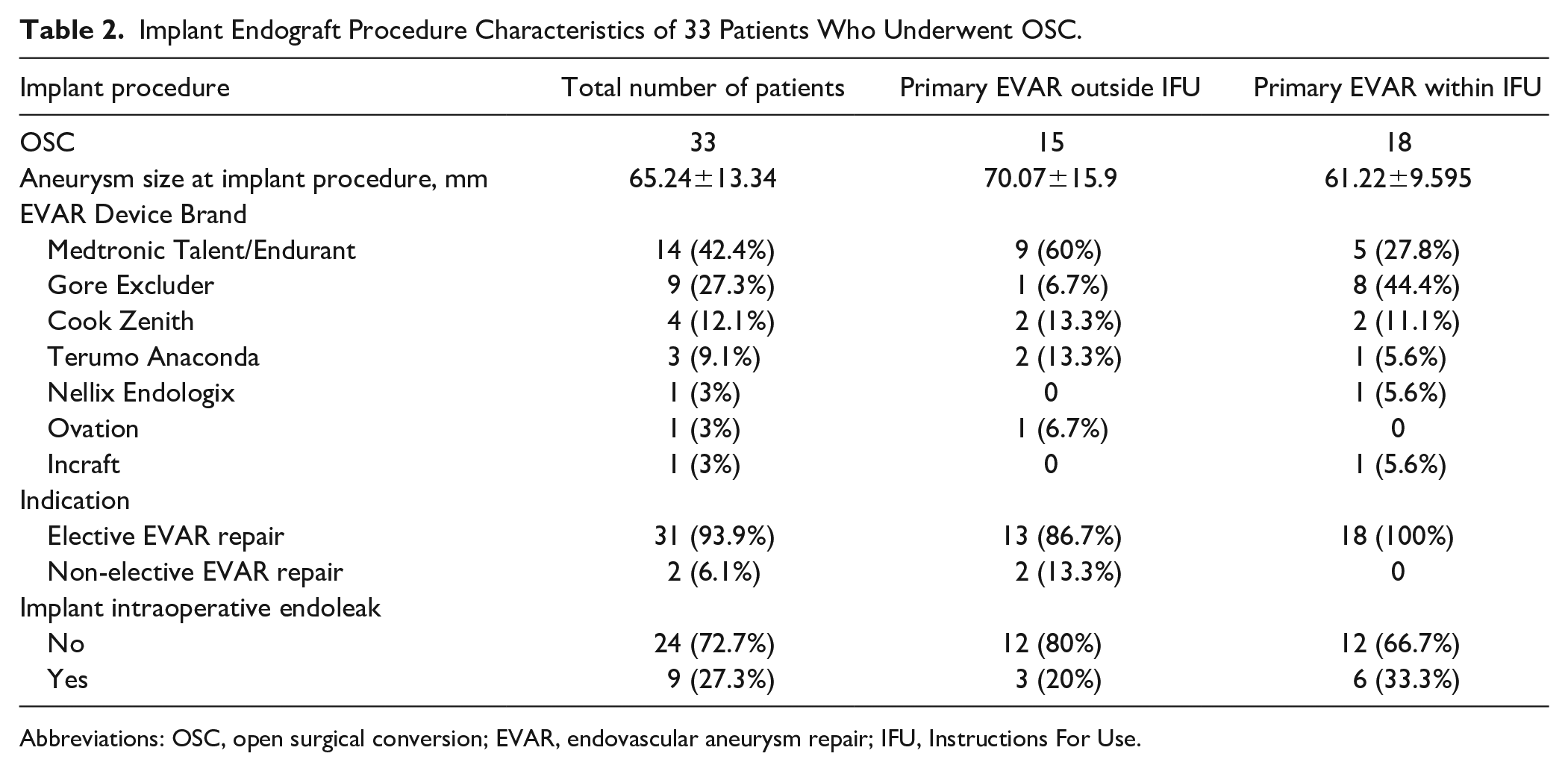
Abbreviations: OSC, open surgical conversion; EVAR, endovascular aneurysm repair; IFU, Instructions For Use.
Surveillance Program and Secondary Reinterventions Before OSC
From implant to explant, complete follow-up was accomplished by 60.6% of the patients (20/33) and partial in 39.4% (13/33), being slightly higher in patients in-IFU group. A mean of 1.73±1.2 secondary interventions during follow-up were performed: 1.53±1.2 in patients with primary EVARs outside IFU vs 1.89±1.2 in the groups within IFU. Nearly all of the patients (84.8%, 28/33) required one reintervention before OSC. Of note, 9.1% (3 patients) suffered ≥ 4 endovascular reinterventions. The time from implant to explant was shorter in not-IFU patients: 47.60 ±28.8 months (median 50 months) vs 71.17±48.1 months in-IFU patients (median 66.5 months), with no statistical difference between groups (see Table 3 and Figure 1, for details).
Follow-Up Characteristics of 33 Explanted Patients From EVAR Implant Procedure to EVAR Explant Procedure.
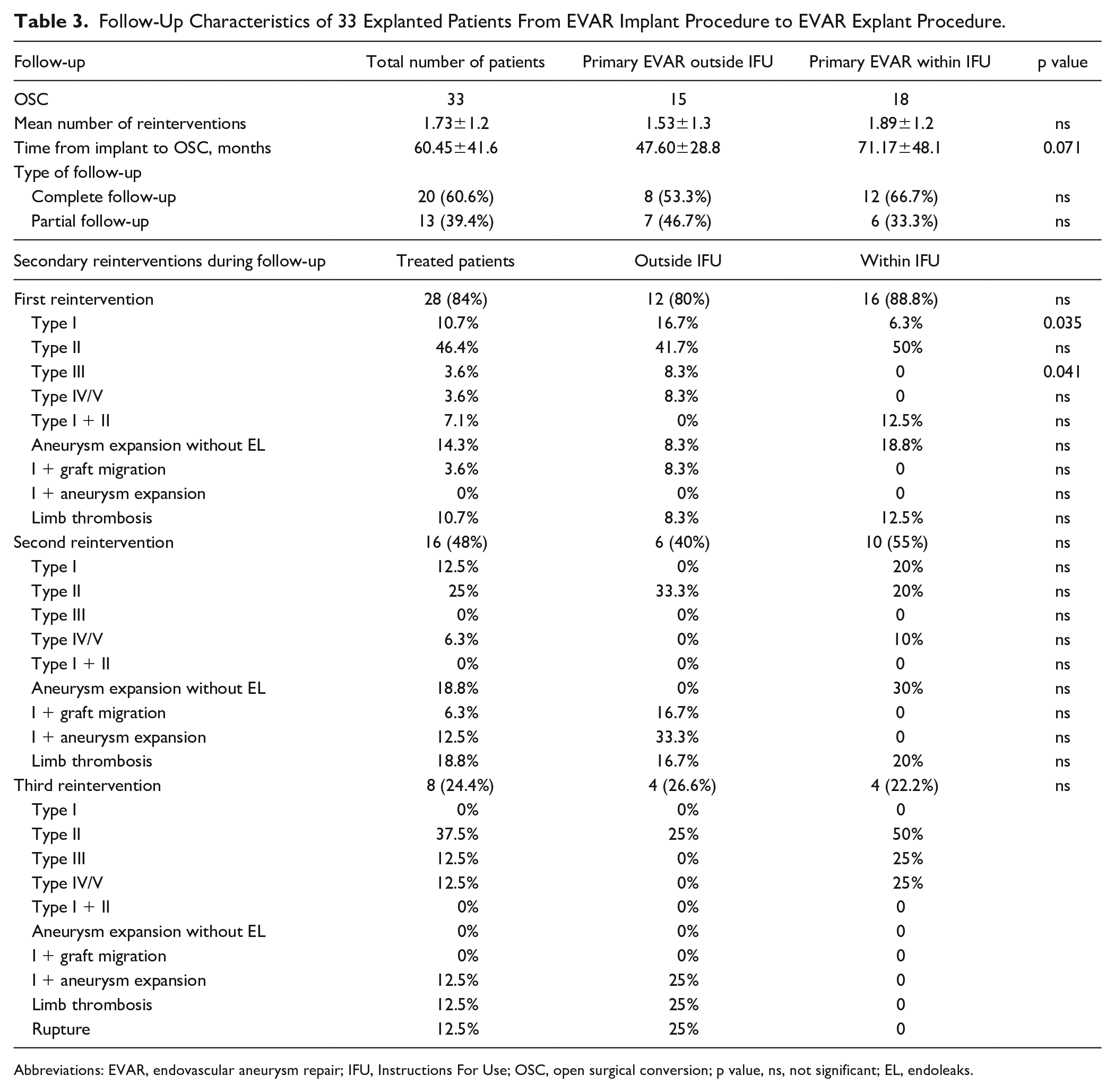
Abbreviations: EVAR, endovascular aneurysm repair; IFU, Instructions For Use; OSC, open surgical conversion; p value, ns, not significant; EL, endoleaks.
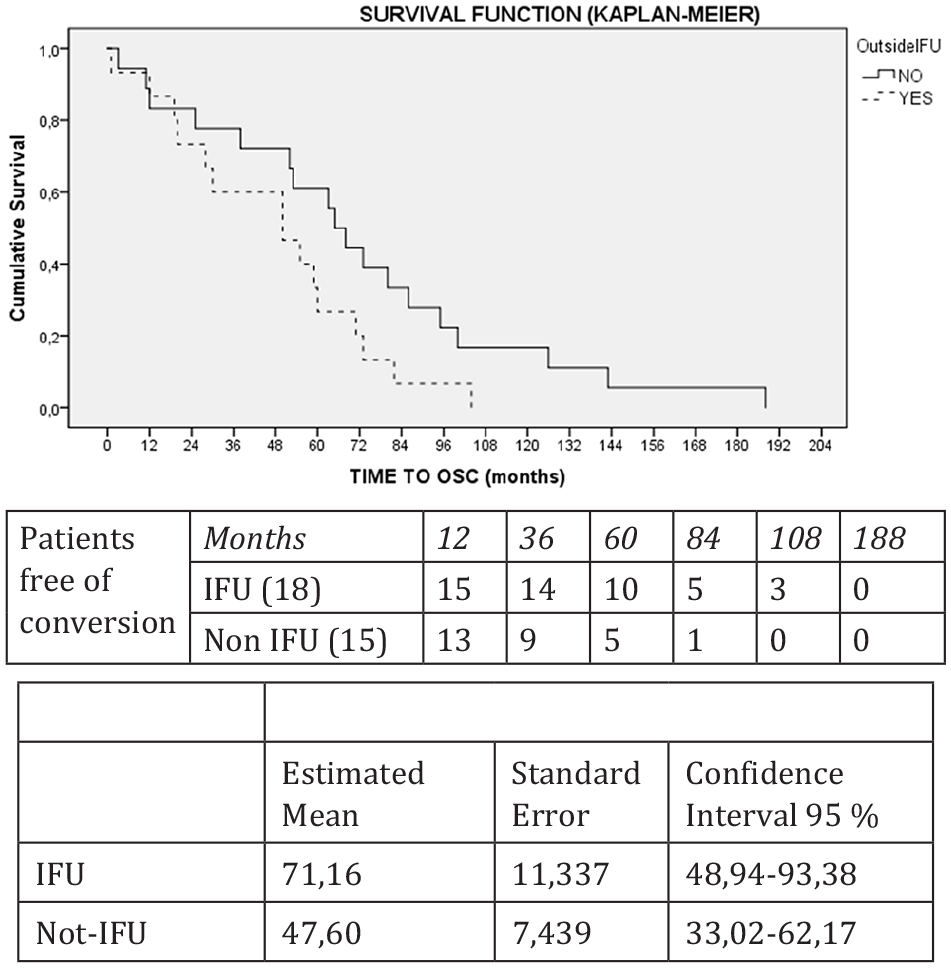
A log rank test was carried out to compare the estimation of the means of time with conversion using the Mantel-Cox method. A X2 of 3.25 was obtained for 1 degree of freedom, with no statistically significant difference (p=0.071). IFU, Instructions For Use; OSC, open surgical conversion.
Type II endoleaks were the most common leak treated during follow-up, representing 46.4% of total endoleaks treated at first reintervention. Differences were found, especially at first reintervention, with more type I endoleaks (16.7% vs 6.3%) and type III endoleaks (8.3% vs 0%) in the subgroup of patients not adjusted to IFU with significant statistical differences. See Table 3 with the distribution of endoleaks treated according to the number of reinterventions.
Indications for OSC After EVAR
Significant value should be given to the subgroup’s differences in the final indication to OSC (see Table 4). Type II endoleak was the most frequent contributing factor to the indication for explantation in all groups, but especially among patients who had repair within IFU criteria 38.9% vs 6.7% in out-IFU patients. Low-flow endoleaks (type II, type IV, and type V) account for 44% of late conversions in the subgroup of patients of EVARs within IFU, compared with 13.3% in patients out-IFU. On the contrary, OSC was indicated due to a type I endoleak in only 16.7% of the patients in-IFU vs 26.7% in patients out-IFU with no statistically significant differences. So that, high-flow endoleaks (type I and type III) were the main indication for OSC especially in the subgroup of patients out-IFU (33.3% of indications vs 16.7% in-IFU patients). Indication for aneurysm expansion without endoleaks (24.2%) had a similar distribution in both subgroups. See indications in Figure 2.
Classification and Frequency of Final Indications to Open Surgical Conversion After EVAR.
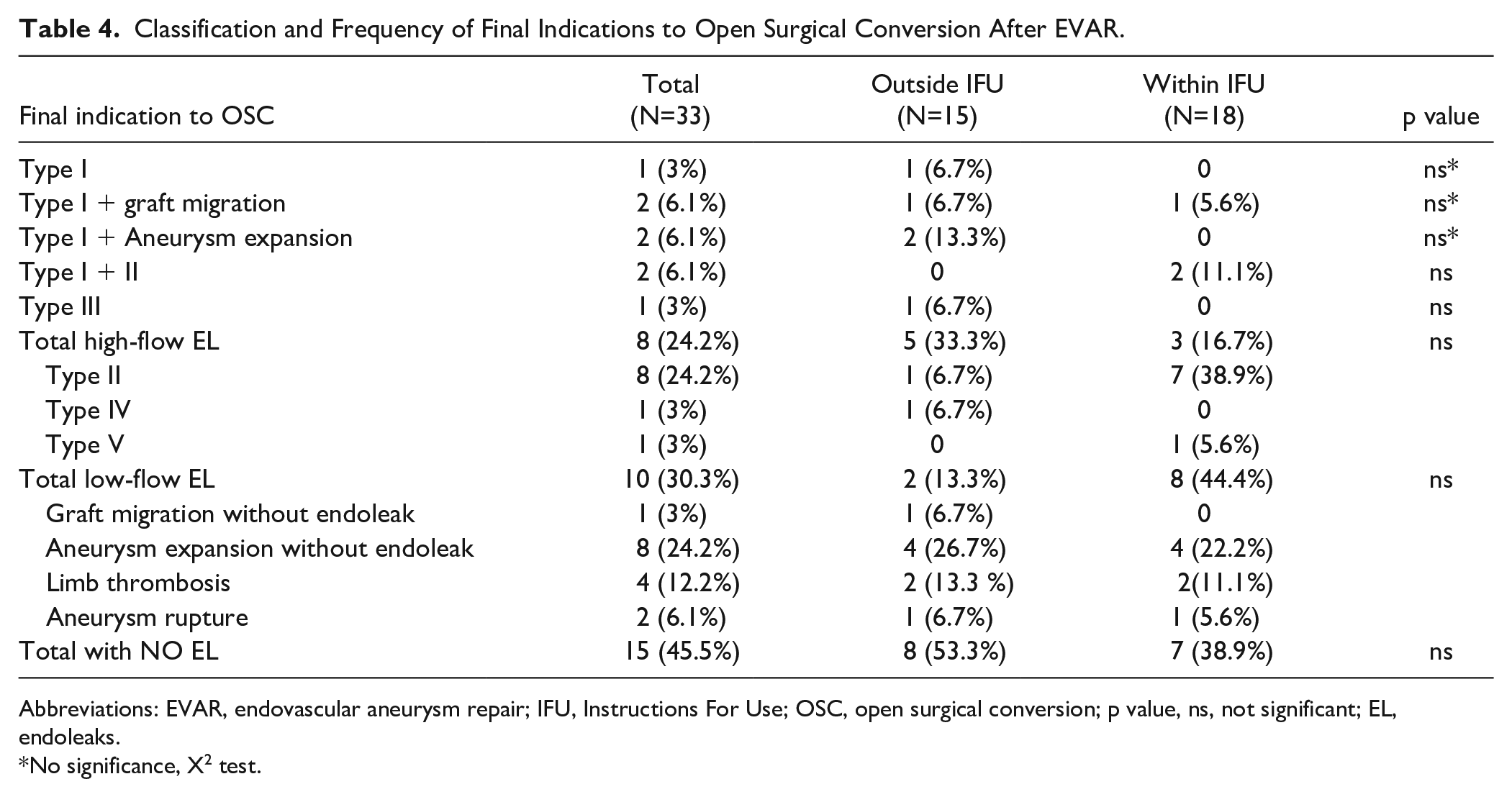
Abbreviations: EVAR, endovascular aneurysm repair; IFU, Instructions For Use; OSC, open surgical conversion; p value, ns, not significant; EL, endoleaks.
No significance, X2 test.
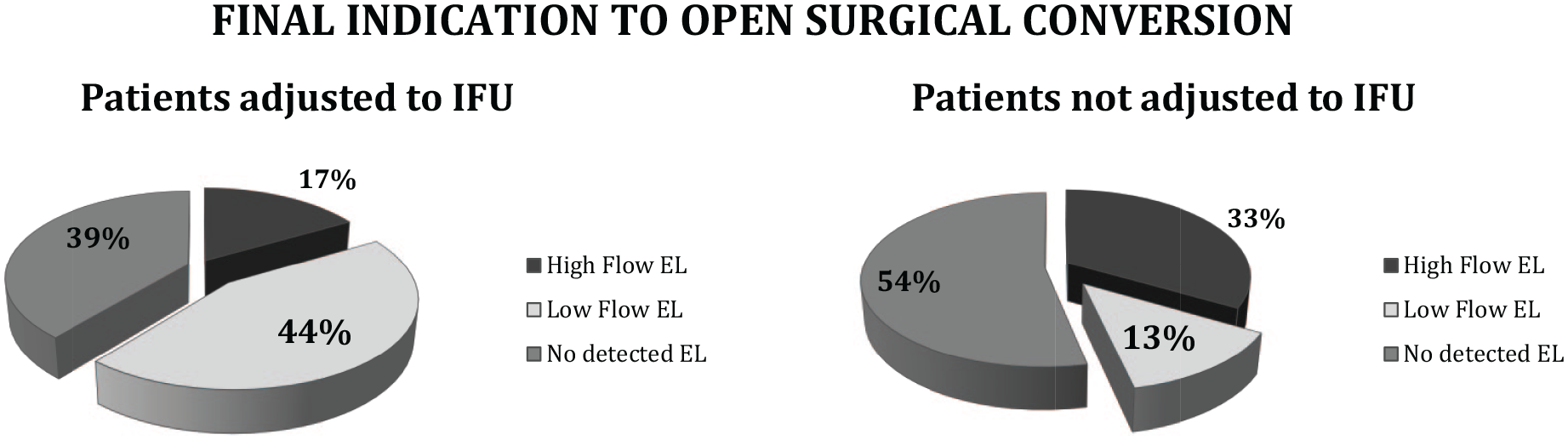
Comparison of final indication with open surgical conversion between patients adjusted to IFU criteria and not adjusted to IFU. X2 test, no significance difference between groups. IFU, Instructions For Use; EL, Endoleak.
Explant Procedure and Postoperative Outcomes
The majority of the patients (n=28, 84.8%) underwent an elective procedure, whereas 5 (15.15%) patients had emergent explantation. Operative characteristics were determined by surgeon preference and clinical factors (see Table 5). Total endograft explantation was performed in 57.5% of the cases (19/33), slightly higher in out-IFU explanted patients (66.7%) and partial explantation in 30.3% (10/33). Abdominal laparotomy, endograft preserving, and lumbar vessels ligation were necessary in 12.1% of the patients (4/33). More suprarenal clamping was required in the subgroup of patients out-IFU. Postoperative complications occurred in 42.4% (n=14) of the patients, 64% of them due to acute postoperative renal failure. Clamping above renal arteries was related to more complications as renal failure, and higher 30-day mortality rate (19% above vs 0% in patients with clamping below renal arteries). The intraoperative death rate was 6% (2/33). The mean length of stay was 16.24 days with a median of 10 days. Overall, the 30-day mortality rate was 12.1% (4/33), 20% mortality rate for patients out-IFU, and 5.6% for patients in-IFU with no statistical differences. For patients operated urgently, the 30-day mortality was significantly higher than elective patients (40% vs 7.1%, p=0.038).
Surgical Approach, Explantation Technique, and Postoperative Outcomes of the Conversion Procedure and Group Comparisons.
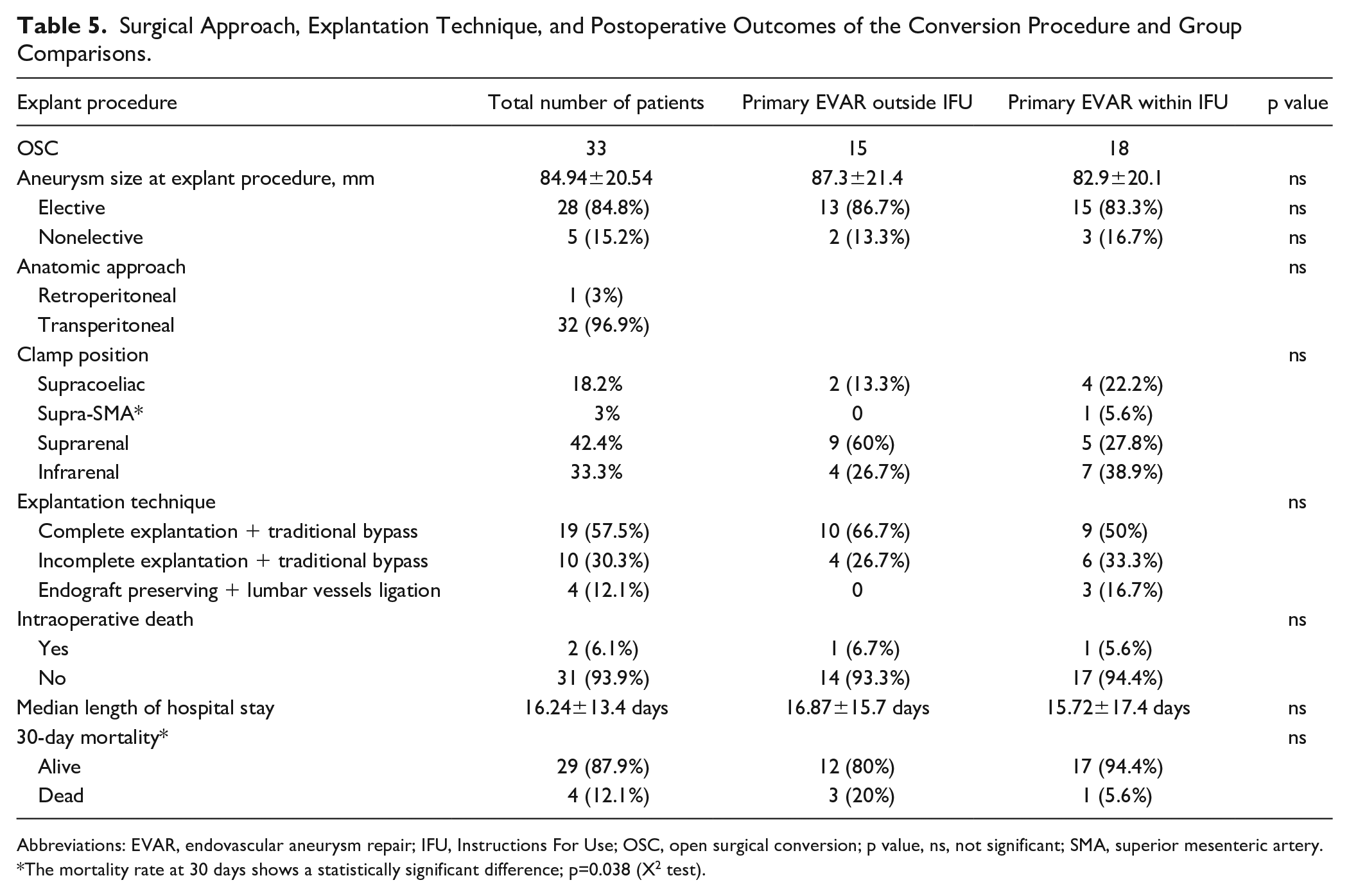
Abbreviations: EVAR, endovascular aneurysm repair; IFU, Instructions For Use; OSC, open surgical conversion; p value, ns, not significant; SMA, superior mesenteric artery.
The mortality rate at 30 days shows a statistically significant difference; p=0.038 (X2 test).
Discussion
Due to the growing number of patients having EVAR, the need for open conversion of failing endografts is increasing over time with rates varying between 0.67% and 22.8% in some series5,6 (0.95%±0.88% in the present study). According to the literature, 17 IFU nonadherence is associated with worse long-term EVAR outcomes. In our multicenter retrospective study, comparing OSC for abdominal aortic aneurysm treated with EVAR outside IFU and EVAR adjusted to IFU, we found that late open conversion in not-IFU patients is indicated mainly for high-flow endoleaks (type I and type III). This finding had its influence on the interval from implant to explant making it shorter (47.60±28.8 months vs 71.17±48.1 months in IFU patients) and had also less secondary endovascular reinterventions during follow-up (1.53±1.2 vs 1.89±1.2 in the group in IFU), probably with the aim to reduce the risk of aneurysm rupture during surveillance. Each stent graft device has its own manufacturers outline IFU to increase long-term durability. According to the literature, IFU nonadherence is high ranging from 38% to 68.9% 18 and the relationship between adherence to IFU and EVAR outcomes remains controversial. Herman et al 19 demonstrated higher rates of graft-related complications after elective EVAR in patients with nonadherence to IFU after elective EVAR (16.3% vs 10%). In a similar-sized study, AbuRahma et al 8 found IFU nonadherence to be associated with higher rates of early and late type IA endoleaks and worse long-term survival. In contrast, Antoniou et al 20 conducted a systematic review of the literature and meta-analysis of 4498 patients’ outcomes with standard EVAR performed outside vs within IFU and found no significant association between nonadherence to IFU and most of the defined outcomes as technical failure, requirement for adjunctive procedures, type I–related reintervention, or aneurysm sac expansion. Type I endoleaks represent a failure of the proximal/distal sealing and may be the liberal use or EVAR over the recent years has lead to an increase of the incidence of EVAR failure. In our study, patients not adjusted to IFU with high-flow endoleaks during follow-up (see Figure 1) might be recognized at a high risk for a sooner OSC compared with patients adjusted to IFU, and to our best knowledge, there are no references in the literature to this fact.
On the contrary, type II endoleaks were the most frequent contributing factor to the indication for explantation in both groups of our study, a finding well confirmed from prior reports. 21 So type II endoleaks do not seem the benign condition that it is generally accepted, which it is still a subject of much debate, 22 and set the patient at a significantly higher rates of conversion to open repair.
Surgical conversion of failed EVAR presents unique technical challenges, especially the difficulties to stent removal. In our study, total endograft explantation was performed in 57.5% of the cases (19/33), being slightly higher for out-IFU explanted patients (66.7%). In total, 93% of patients out-IFU had initial endograft with suprarenal fixation, probably being more necessary to clamp above the renal arteries to explant the graft in this subgroup. Aortic cross-clamping above the renal arteries increases the risk of visceral ischemia, acute kidney injury, and cardiac complications.23,24 In the present report, postoperative complications occurred in 42.4% (n=14) of the patients, 64% of them due to acute postoperative renal failure. Some authors have proposed partial grafts removal and to create a “neo-neck” preserving the first covered stent and “neo-limbs,” 25 maintaining distal endoprosthesis as an alternative option to avoid complex complete explantations. 26 Factors such as suprarenal fixation, active endoleaks, periaortic inflammation and secondary endovascular salvage devices such as embolization coils, proximal cuffs, and endoanchors contribute to increase the mortality and complexity of stent removal. 11 Overall, in our study, the 30-day mortality rate was 12.1% (4/33). The 30-day mortality rate was higher in patients out-IFU than in-IFU patients (20% vs 5.6%) without statistical significance. For patients operated urgently, our 30-day mortality rate was significantly higher than elective patients (40% vs 7.1%, p=0.038). The significantly increased mortality associated with nonelective conversions highlights the need for active surveillance 27 and management at high-volume aortic referral centers. 28
Long-term results of the EVAR 1 trial have shown worse mortality in the EVAR group beyond 8 years, primarily the result of increased rates of secondary aneurysm sac rupture. 29 All patients in the EVAR 1 had anatomy considered appropriate for EVAR and one would assume that the effects of nonadherence to IFU would only increase these risks of long-term EVAR failure and OSC would be required in some instances adding significant higher morbidity and mortality risk. In fact, Xodo et al 30 studied 144 patients with OSC after failed EVAR and found decreased 5-year survival in patients with advanced age and emergency treatment. In the present report, performing OSC after failed EVAR in out-IFU patients was associated with higher rates of mortality. Physicians are committed to adhere to follow the IFU as much as feasible not only to allow maximal benefit to the patient, but also to keep the patient’s best interest in mind. 31 Selected patients with adverse anatomic features who are deemed high risk for complex open or endovascular procedures might likely be safely treated with conventional EVAR, although the long-term durability is exposed to criticism.
Limitations of This Study
As most of the studies available in literature, the analysis is retrospective thus including inherent selection bias. Many patients may not have been captured in this data set because they were lost after several years of follow-up or those with expanding aneurysm sacs who did not go OSC because of the comorbid status.
Another potential confounding factor is the proportion of patients who underwent EVAR outside of device IFU over time with no complications and that could not be ascertained. Finally, as the final indication to OSC is not established from recommendations based on international practical guidelines, centers participating in this study may have been heterogeneous in terms of indications or surgical techniques and contribute to small and heterogeneous groups of patients with multiple mechanisms of endograft failure, making statistical analysis difficult. Despite the sample size is small to derive meaningful conclusions, this study sheds some light reporting real-world features of OSC of failed EVARs and their relationship to device IFU compliance adjustment, secondary reinterventions, and endoleaks.
Conclusions
Notwithstanding the technologic advancement and the increasing experience of endovascular surgeons, some EVAR patients will definitely need open conversion. In our study, differences have been found between patients outside IFU who need conversion and patients within IFU, with more high-flow endoleaks during follow-up, shorter interval from implant to explant, and higher mortality. This study reinforces the trend that EVAR patients treated outside IFU have worse long-term outcomes mainly due to high-flow endoleaks and also special technical features when come to explantation. Further studies and international network investigation need to be done to broad and deepen these initial results.
Supplemental Material
sj-docx-1-jet-10.1177_15266028221102658 – Supplemental material for Multicenter Comparative Analysis of Late Open Conversion in Patients With Adherence and Nonadherence to Instructions for Use Endovascular Aneurysm Repair
Supplemental material, sj-docx-1-jet-10.1177_15266028221102658 for Multicenter Comparative Analysis of Late Open Conversion in Patients With Adherence and Nonadherence to Instructions for Use Endovascular Aneurysm Repair by Cristina Lopez-Espada, Jose Linares-Palomino, Mercedes Guerra Requena, Francisco Javier Serrano Hernando, Elena Iborra Ortega, Rafael Fernández-Samos, Amer Zanabili Al-Sibbai, Elena González Cañas, Jose Mª Rodriguez Sánchez, Jose Miguel Zaragozá García, Andrés García León, Soledad Manzano Grossi, Luis de Benito, Daniel Gil Sala and Livia Revuelta Mariño in Journal of Endovascular Therapy
Footnotes
Acknowledgements
To the Spanish Endovascular Surgery Chapter (CCEV) for its technical support to this project promote initiatives to improve the quality of care in our specialty.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.