
Abstract
Purpose:
To investigate the safety and efficacy of fast-track management of concurrent percutaneous coronary intervention (PCI) in patients with abdominal aortic aneurysm scheduled for endovascular aortic aneurysm repair (EVAR).
Materials and Methods:
Eligible patients with abdominal aortic aneurysm who received EVAR from January 2011 to December 2019 were included in this retrospective cohort study. Propensity score (PS)–matched analysis was used to balance the baseline between the fast-track and standard control (EVAR without significant coronary artery disease) groups. Effects of fast-track management on short-term and midterm outcomes were evaluated via Cox proportional hazard regression and logistic regression analyses with corresponding hazard ratio (HR) or odds ratio (OR) and associated 95% confidence intervals (95% CIs), respectively.
Results:
The study included 669 patients (73 fast-track and 596 standard control). Compared with the standard control group, no significant difference was found regarding major adverse cardiac events (HR 0.78, 95% CI [0.36, 1.68], p=0.519), overall mortality (HR 0.63, 95% CI [0.25, 1.55], p=0.315), and 30-day major hemorrhage events (OR 1.01, 95% CI [0.99, 1.03], p=0.514). The results were consistent in the PS-matched cohorts regarding major adverse cardiac events (HR 0.57, 95% CI [0.25, 1.29], p=0.176), overall mortality (HR 0.43, 95% CI [0.17, 1.11], p=0.820), and 30-day major hemorrhage events (OR 1.00, 95% CI [0.05, 10.61], p=0.999). Similar results were found in the subgroup analyses concerning fast-track management of 2-week intervals and patients with high age-adjusted Charlson comorbidity index.
Conclusions:
Under appropriate perioperative care, shortening the time interval between PCI and EVAR to 1 month, or even 2 weeks, seemed to be safe and effective. Short-term and midterm cardiovascular and survival outcomes were comparable with patients who underwent standard EVAR without significant coronary artery disease.
Keywords
Introduction
Abdominal aortic aneurysm (AAA) is a life-threatening disease that mainly affects elderly males. Given the shared risk factors, 1 current evidence suggests a high prevalence of concomitant coronary artery disease (CAD) in the AAA population, reaching approximately 30% to 65%. 2 Cardiovascular adverse events rather than aneurysm-related adverse events remain one of the leading causes of long-term mortality after endovascular AAA repair (EVAR). 3 According to the European Society for Vascular Surgery (ESVS) and the Society for Vascular Surgery (SVS),4,5 prophylactic coronary revascularization, mostly by percutaneous coronary intervention (PCI) in clinical practice, was recommended in patients with unstable CAD or considered to be at high risk of cardiac events before EVAR.
Regarding the optimal time interval between PCI and EVAR, the 2019 ESVS guideline recommended deferring repair of aneurysms until mono-antiplatelet therapy (MAPT) was available, 4 usually requiring 6 to 12 months according to the American College of Cardiology/American Heart Association. 6 The recent guidelines from SVS also recommended that the repair of aneurysms should be delayed for at least 30 days after coronary stenting, if cessation of dual antiplatelet therapy (DAPT) was need for surgery. These recommendations were based on the fact that DAPT was necessary to reduce the risk of coronary-stent thrombosis, while DAPT could also confer incremental risk for major hemorrhage events. 7 However, the sources of evidence supporting postponing AAA intervention mainly came from various open procedures, 8 which were deemed to have a higher bleeding risk than endovascular procedures. Recently, some studies reported acceptable outcomes in patients underwent aneurysm repair 2 to 8 weeks after PCI, which suggested the feasibility of a shorter interval between PCI and aortic aneurysm repair.9–11 However, these studies were limited by the inclusion of various aortic diseases that might face different cardiac risks, and few comorbidity confounding factors were addressed in these studies, which might influence the results.
In the past decade, our center has developed a fast-track strategy for managing patients who need to receive concurrent PCI before EVAR, which gradually shortened the time interval to within 1 month. To further investigate the safety and efficacy of our fast-track management of concurrent PCI and EVAR, we conducted a retrospective propensity score (PS)–matched cohort study in our center. We hypothesized that a short time interval within 1 month between PCI and EVAR with appropriate perioperative care would not increase the risk of major adverse cardiac events (MACE) and overall mortality after surgery.
Materials and Methods
Study Design
This retrospective cohort study was performed in a tertiary academic hospital in China. The study was reported following the standard of Reporting of Observational Studies in Epidemiology Statement of cohort studies. De-identified data were used for analysis and the study was approved by the institutional review board of West China Hospital. Informed consent was absent because of the retrospective nature of this study.
Study Cohort
Consecutive patients with infrarenal AAA (ICD-10 codes I71.3 and I71.4) or iliac aneurysm (ICD-10 codes I72.3) from January 2011 to December 2019 were reviewed in the hospital information system. The inclusion criteria were patients with AAA (with or without iliac aneurysm) who received EVAR using a bifurcated stent graft. EVAR would be performed in following situation if anatomically eligible: (1) patients with AAA who have reached the diameter threshold for surgery as guidelines4,5; (2) patients with iliac aneurysm (>3.5 cm) and small AAA (>3.0 cm). And PCI would be performed in patients with at least 1 coronary stenosis ≥70% or in patients with coronary stenosis ≥50% who had angina. The exclusion criteria were as follows: (1) history of coronary artery bypass grafting (CABG) or PCI at least 1 month before EVAR; (2) laboratory examination indicating potential myocardial injury 12 (high-sensitivity troponin-T [c-TnT] > 70 ng/L) or heart failure (pro-brain natriuretic peptide [pro-BNP]) using age-adjusted cut-offs 13 without further assessment by percutaneous coronary angiography (PCA) or coronary computed tomography angiography (CCTA); (3) high cardiac risk patients (Revised Cardiac Risk Index [RCRI] > 2) or significant CAD (with coronary stenosis ≥70%) while no coronary revascularization was performed before EVAR; (4) reintervention of previous EVAR.
The primary independent variable was whether the patient received PCI with coronary stenting before EVAR. Patients included in the study who underwent PCI within 1 month before EVAR were grouped into the fast-track group, and those without evidence of significant CAD were grouped into the standard control group. In our center, routine cardiac assessment was performed in patients planed for EVAR older than 60 years, either by coronary CTA or angiogram, dependent on patients’ history and symptoms.
Fast-Track Protocols of Perioperative Management
All perioperative management and treatment strategies followed a standard protocol. Patients received electrocardiograms and cardiac biomarker evaluations at admission as routine assessments. Echocardiography was performed for the elective patient. Coronary artery assessment either by CCTA or PCA was recommended for patients if they had at least 1 risk factor from the RCRI. Coronary artery lesions were evaluated by cardiologists who decided whether the lesions required treatment or which revascularization procedure should be used. All patients with PCI received DAPT during the whole perioperative period of EVAR and received cardiac biomarker evaluations on the first day and third day after PCI. The time interval between PCI and EVAR was determined by the levels of cardiac biomarkers, and EVAR would be performed as soon as the patient was asymptomatic with post-PCI elevations of CK-MB < 3×upper reference limit (URL) and the post-PCI elevations of troponin < 35×URL. 14 Emergency surgery would be performed once aneurysm-related symptoms were exacerbating. Most of the other patients who did not receive PCI were prescribed MAPT in addition to those who refused PCI or needed DAPT for other indications. Endurant II or IIs Stent Graft (Medtronic, Minneapolis, MN, USA) was used in all patients in this study.
Follow-Up Protocols
Patients received EVAR were followed up via ultrasound at 1 month, 3 months, 12 months, and annually thereafter as previously described.15,16 Computed tomography angiography was performed if adverse aneurysm-specific complications including type I or III endoleaks, persistent type II endoleak with or without increased diameter of the aneurysm, limb occlusion, or other related symptoms were observed.5,4 Furthermore, follow-up by telephone calls or online consultations was also used to identify the status of the patients if patients could not visit our clinics.
Covariables of Interest
Demographic variables included were age, gender, and smoking status. Comorbidities were identified using clinical diagnosis records and medical insurance records. The age-adjusted Charlson comorbidity index (ACCI) was used to estimate the severity of comorbidity, 17 and preoperative cardiac risk was evaluated via the RCRI. Anatomical parameters were recorded as follows: maximum diameter of the aneurysm sac, maximum diameter of the iliac arteries, and whether there was concomitant iliac aneurysm. All the diameter parameters were measured from the minor axis of axial sections or from normal planes of the centerline in the reconstructed image. A maximum diameter of the AAA of >70 mm was defined as a large aneurysm sac. 16 Diagnosis of concomitant iliac aneurysm followed the criteria of ESVS. Mode of anesthesia (general or regional) was also recorded.
Outcomes of Interest
The primary outcome was MACE involving death, myocardial infarction (ICD-10 codes I21,I22), congestive heart failure (ICD-10 codes I20-I25, I11,I13), and the need for cardiac revascularization. Secondary outcomes included the risk of major hemorrhage events (occurrence of type 3 or 5 hemorrhage events according to Bleeding Academic Research Consortium), 18 and total hemorrhage events, cardiac death, overall mortality, and aneurysm-related adverse events (aneurysm-related reintervention and death).
Statistical Analysis
Categorical variables were described as frequencies and percentages. Normally distributed continuous variables were present as mean with standard deviation (SD) and nonparametric variables were present as median with interquartile ranges (IQR). The differences between groups were tested by Fisher’s exact or chi-square tests for categorical variables. Student’s t-test or Mann–Whitney U test was used to compare differences between groups for continuous variables. Standardized mean differences (SMDs) were calculated to further evaluate the balance between groups. A baseline variable was considered imbalanced if the SMD > 10%.
PS matching analysis was used to minimize baseline differences between groups. The propensity for receiving PCI was estimated by a logistic regression model based on age, gender, smoking status, hypertension, diabetes, chronic obstructive pulmonary disease, chronic kidney disease, cerebrovascular disease, cancer, peripheral artery disease, anesthesia, urgency of surgery, large aneurysm sac, and coexisting iliac artery aneurysms. Matching ratios of 1:2 and an optimal approach 19 with minimal average distance were used to create a matched cohort. Multiple imputation was used to address the missing values. Survival curves were generated via Kaplan–Meier method. The effects of fast-track management on midterm and short-term outcomes were evaluated via Cox proportional hazard regression analysis and logistic regression analysis, and the results were reported as hazard ratio (HR) or odds ratio (OR) with associated 95% confident intervals (95% CI), respectively. Subgroup analyses were conducted in patients who received EVAR within 2 weeks after PCI and in patients with a high ACCI (ACCI > 2) to further test the safety of the fast-track strategy. 17
Sensitivity analyses were conducted using inverse probability of treatment weighting (IPTW)–adjusted analyses with marginal structural model and another via covariate adjustment using propensity score (CAPS).20,21 In addition, sensitivity analysis with follow-up time included in the estimation of PS (time-adjusted PS) was performed to further assess the robustness of the results, as the median follow-up time for the fast-track group was shorter than that for the standard control group. 22 Considering that multiple imputation was adopted to address missing values, stabilized weights were used to generate the weighted cohort, and standard errors were obtained using a robust variance estimator for regression models. 20 All statistical analyses were performed using R Studio Version 3.6.0 (http://www.R-project.org). A significance level of 0.05 was used for all analyses.
Results
Baseline Characteristics
A total of 842 patients were reviewed according to the inclusion and exclusion criteria and 669 patients were finally enrolled in the study (Figure 1). Of the 669 patients eligible for study, 73 (10.9%) patients received PCI within 1 month before EVAR. Of the 73 patients in the fast-track group, 54 (74.0%) patients had single-vessel lesions and 18 (24.6%) had multi-vessel lesions. Most patients (63/73, 86.3%) in our center were treated via drug-eluting stents. The median follow-up time (IQR) was 23 (13–47) months for the fast-track group and 34 (15–64) months for the standard control group (p=0.010). A total of 18 (2.7%) patients were unavailable for follow-up after discharge. Other baseline characteristics were present in Tables 1 and 2. In brief, patients who received PCI before EVAR were more likely to be older, male gender, have a smoking history, and have a higher prevalence of hypertension, diabetes, concomitant iliac aneurysm, and so on. After propensity score matching, balances were achieved for most propensity score variables. The median follow-up time was 23 (13–47) months for the fast-track group and 35 (12–70) months for the standard control group (p=0.054).
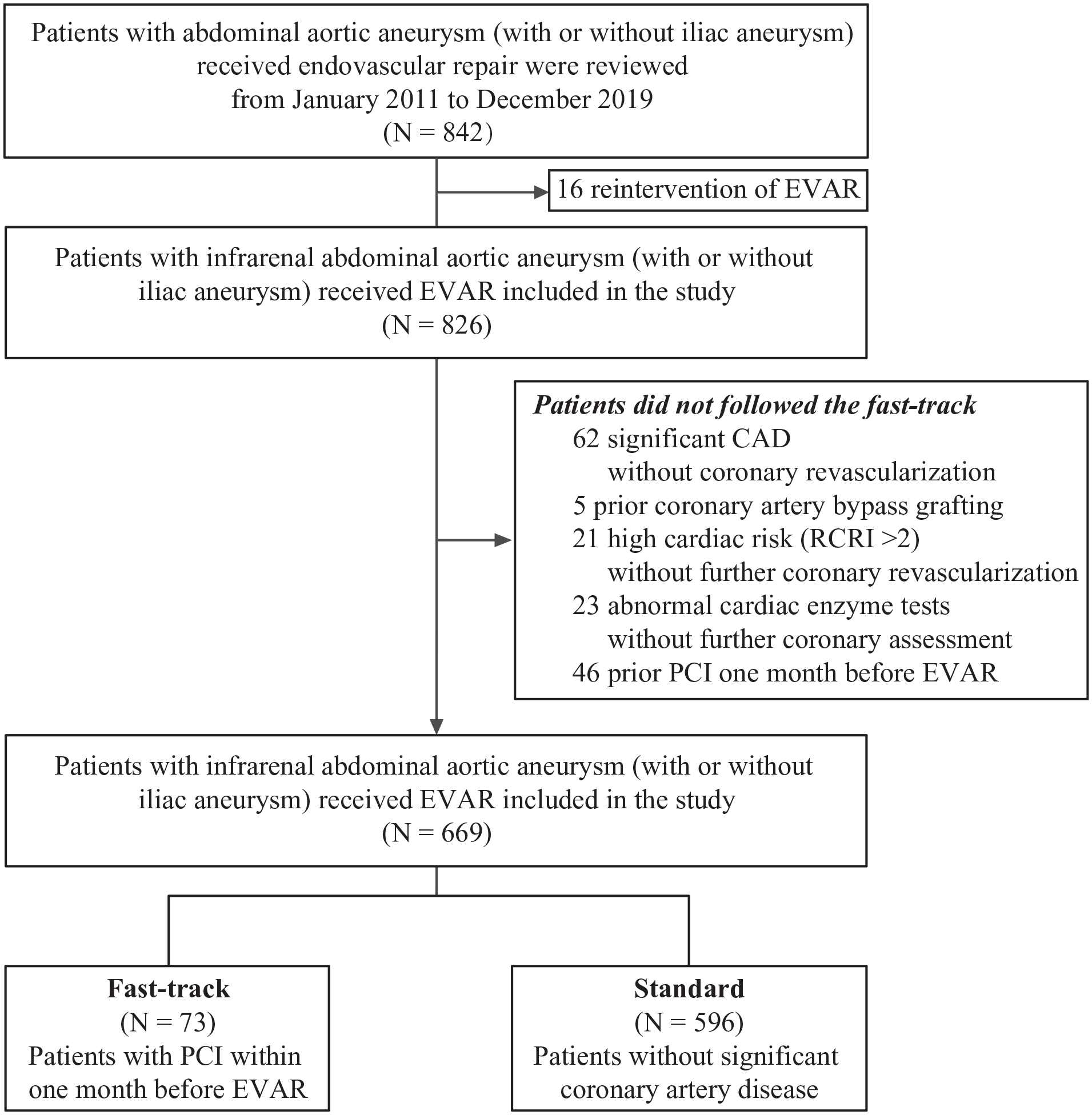
Study flowchart. EVAR, endovascular abdominal aortic aneurysm repair; CAD, coronary artery disease; RCRI, Revised Cardiac Risk Index; PCI, percutaneous coronary intervention.
Baseline Characteristics of the Crude Cohort.
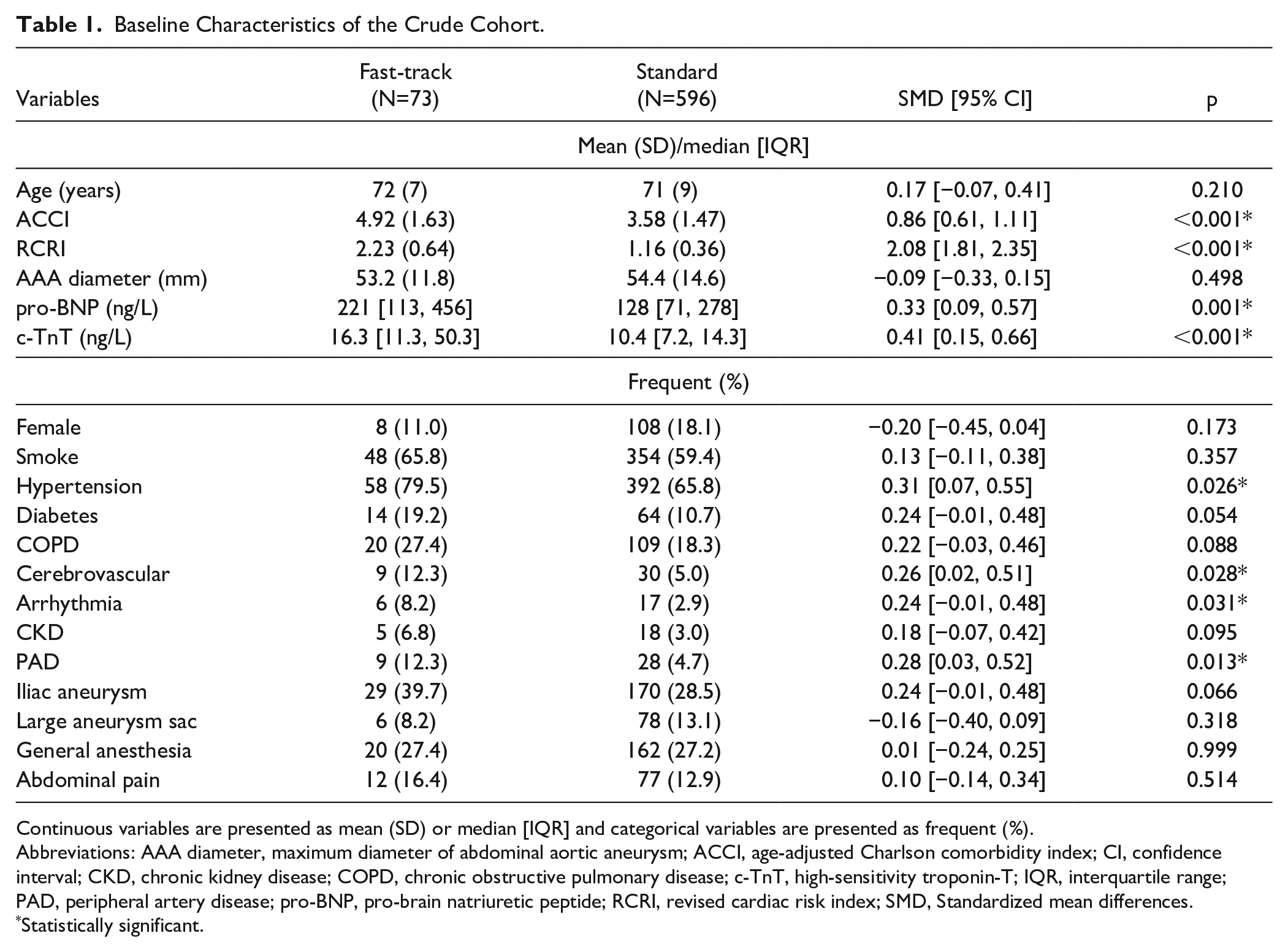
Continuous variables are presented as mean (SD) or median [IQR] and categorical variables are presented as frequent (%).
Abbreviations: AAA diameter, maximum diameter of abdominal aortic aneurysm; ACCI, age-adjusted Charlson comorbidity index; CI, confidence interval; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; c-TnT, high-sensitivity troponin-T; IQR, interquartile range; PAD, peripheral artery disease; pro-BNP, pro-brain natriuretic peptide; RCRI, revised cardiac risk index; SMD, Standardized mean differences.
Statistically significant.
Baseline Characteristics of the Propensity Score–Matched Cohort.
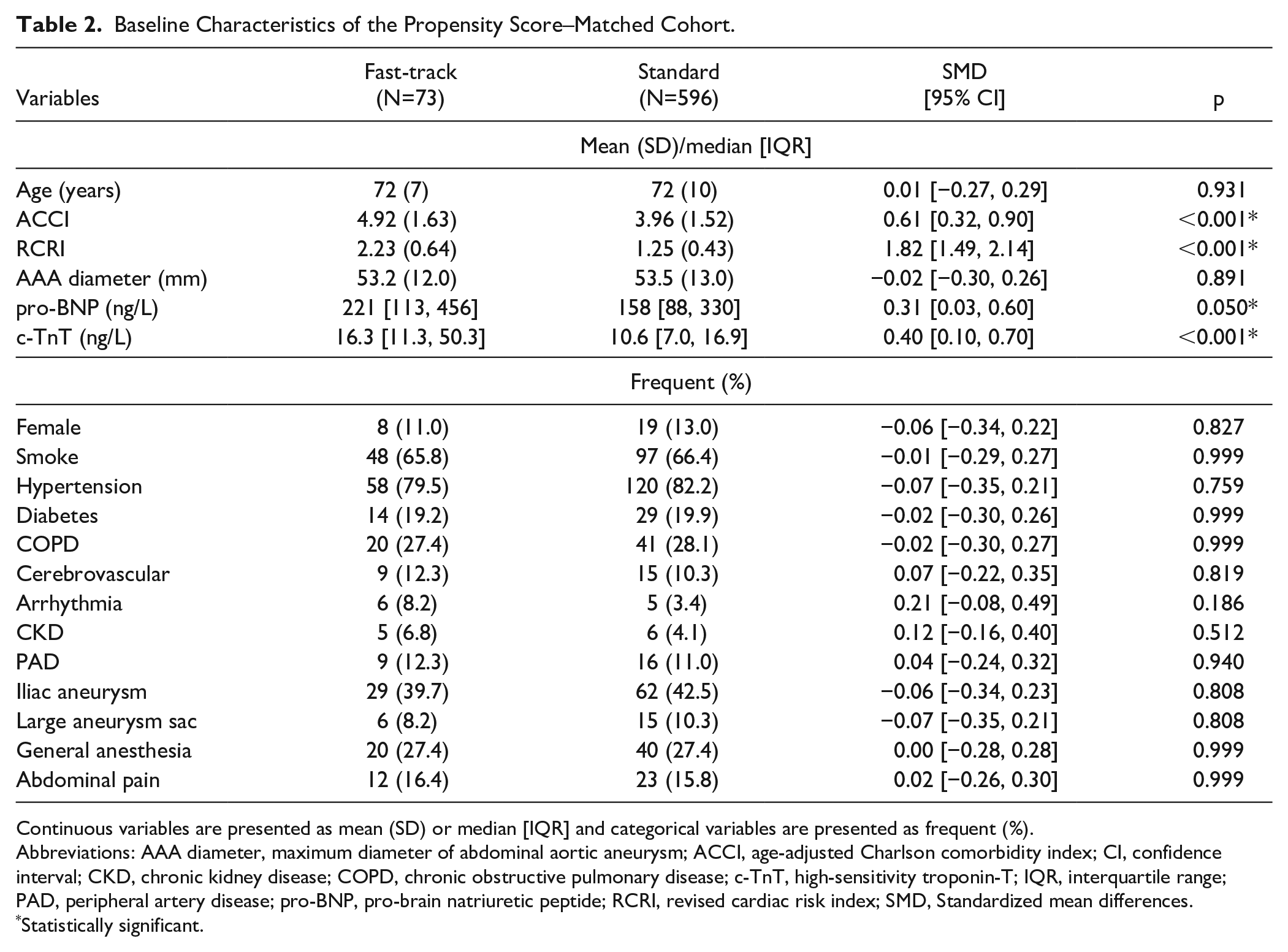
Continuous variables are presented as mean (SD) or median [IQR] and categorical variables are presented as frequent (%).
Abbreviations: AAA diameter, maximum diameter of abdominal aortic aneurysm; ACCI, age-adjusted Charlson comorbidity index; CI, confidence interval; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; c-TnT, high-sensitivity troponin-T; IQR, interquartile range; PAD, peripheral artery disease; pro-BNP, pro-brain natriuretic peptide; RCRI, revised cardiac risk index; SMD, Standardized mean differences.
Statistically significant.
30-Day MACE
There were eleven 30-day MACE occurred, with 1 (1.4%) in the fast-track group and 10 (1.7%) in the standard control group. After propensity score matching, a total of 6 patients suffered from 30-day MACE, with 1 (1.4%) in the fast-track group and 5 (3.6%) in the standard control group. Both crude (OR 1.00, 95% CI [0.97, 1.03], p=0.843) and matched (OR 0.39, 95% CI [0.02, 2.49], p=0.396) analyses suggested no significant difference between groups. Sensitivity analyses also indicated similar results.
In the subgroup analysis of patients with a 2-week interval between PCI and EVAR, crude analysis suggested no significant difference regarding 30-day MACE (OR 1.00, 95% CI [0.97, 1.03], p=0.886). Similarly, in PS-matched analysis, no increased risk was found in terms of 30-day MACE (OR 0.39, 95% CI [0.02, 2.49], p=0.396). Sensitivity analyses were consistent with the above results (Table 3, Supplementary Table 1). Similar results were found in subgroup analysis for patients with a high ACCI (Supplementary Table 2).
Comparison of Outcomes Between Fast-Track and Standard Control Groups.
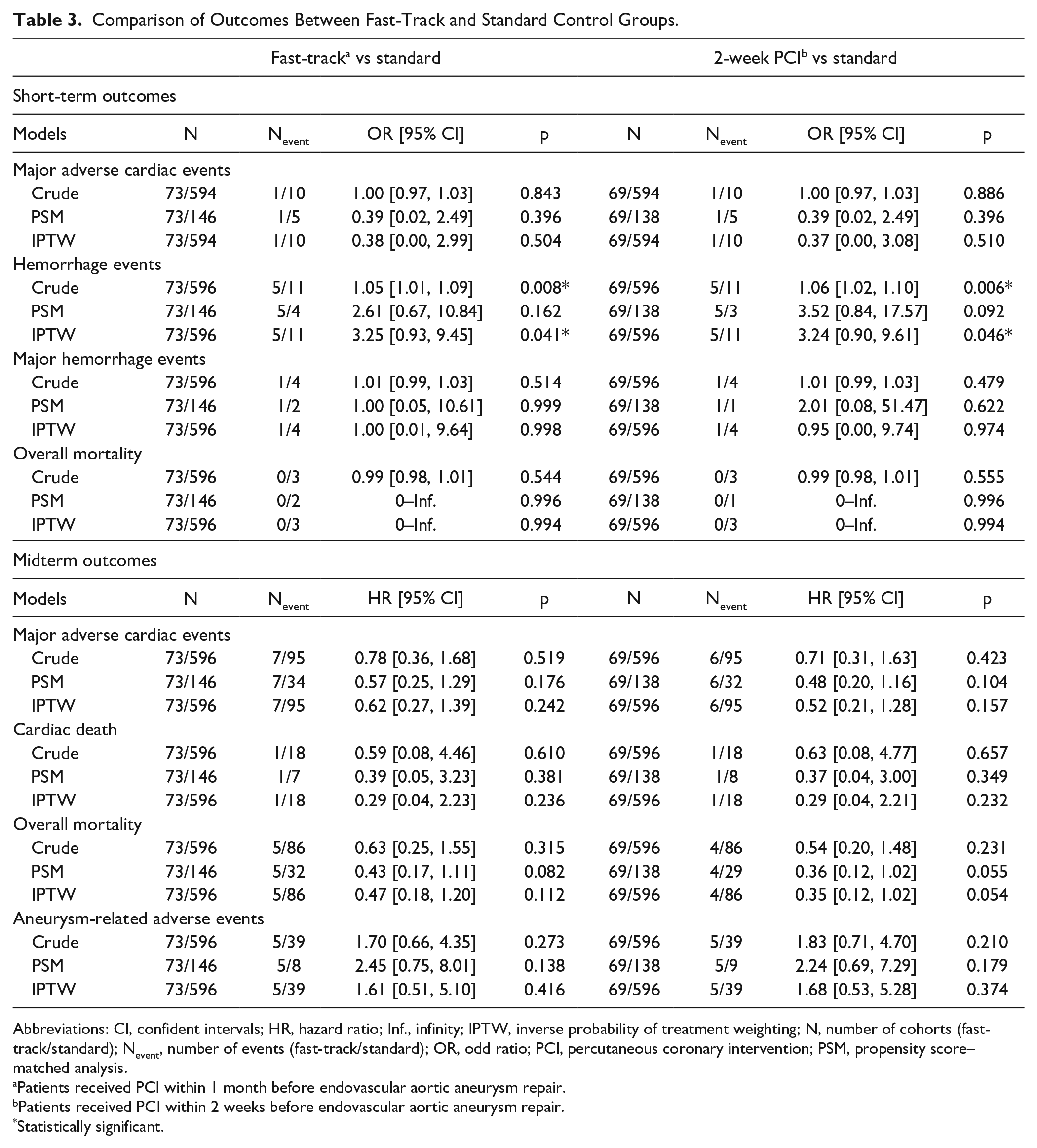
Abbreviations: CI, confident intervals; HR, hazard ratio; Inf., infinity; IPTW, inverse probability of treatment weighting; N, number of cohorts (fast-track/standard); Nevent, number of events (fast-track/standard); OR, odd ratio; PCI, percutaneous coronary intervention; PSM, propensity score–matched analysis.
Patients received PCI within 1 month before endovascular aortic aneurysm repair.
Patients received PCI within 2 weeks before endovascular aortic aneurysm repair.
Statistically significant.
30-Day Major Hemorrhage Events
A total of 5 major hemorrhage events occurred, with 1 (1.4%) in the fast-track group and 4 (0.7%) in the standard control group. After matching, 1 (1.4%) major hemorrhage event occurred in the fast-track group and 2 (1.4%) in the standard control group. No increased risk of major hemorrhage events was found in crude analysis (OR 1.01, 95% CI [0.99, 1.03], p=0.514) and PS-matched analysis (OR 1.00, 95% CI [0.05, 10.61], p=0.999), which was further confirmed in sensitivity analyses.
In the subgroup analysis of patients with PCI within 2 weeks before EVAR, no significant difference was found between the groups regarding major hemorrhage events in crude (OR 1.01, 95% CI [0.99, 1.03], p=0.479) and matched (OR 2.01, 95% CI [0.08, 51.47], p=0.622) analyses (Table 3). Similar results were found in patients with a high ACCI in terms of major hemorrhage events (Supplementary Table 2). Other details for hemorrhage events were record in Supplementary Table 3.
MACE and Cardiac Death in Midterm Follow-Up
A total of 102 (15.2%) patients suffered from MACE during follow-up, with 7 (9.6%) in the fast-track group and 95 (15.9%) in the standard control group (Figure 2A). The MACE included 1 cardiac-cause death and 1 heart failure, and 2 cardiac revascularizations in the fast-track group; and 18 cardiac deaths, 14 myocardial infarctions, 9 heart failures, and 2 cardiac revascularizations in the standard control group.
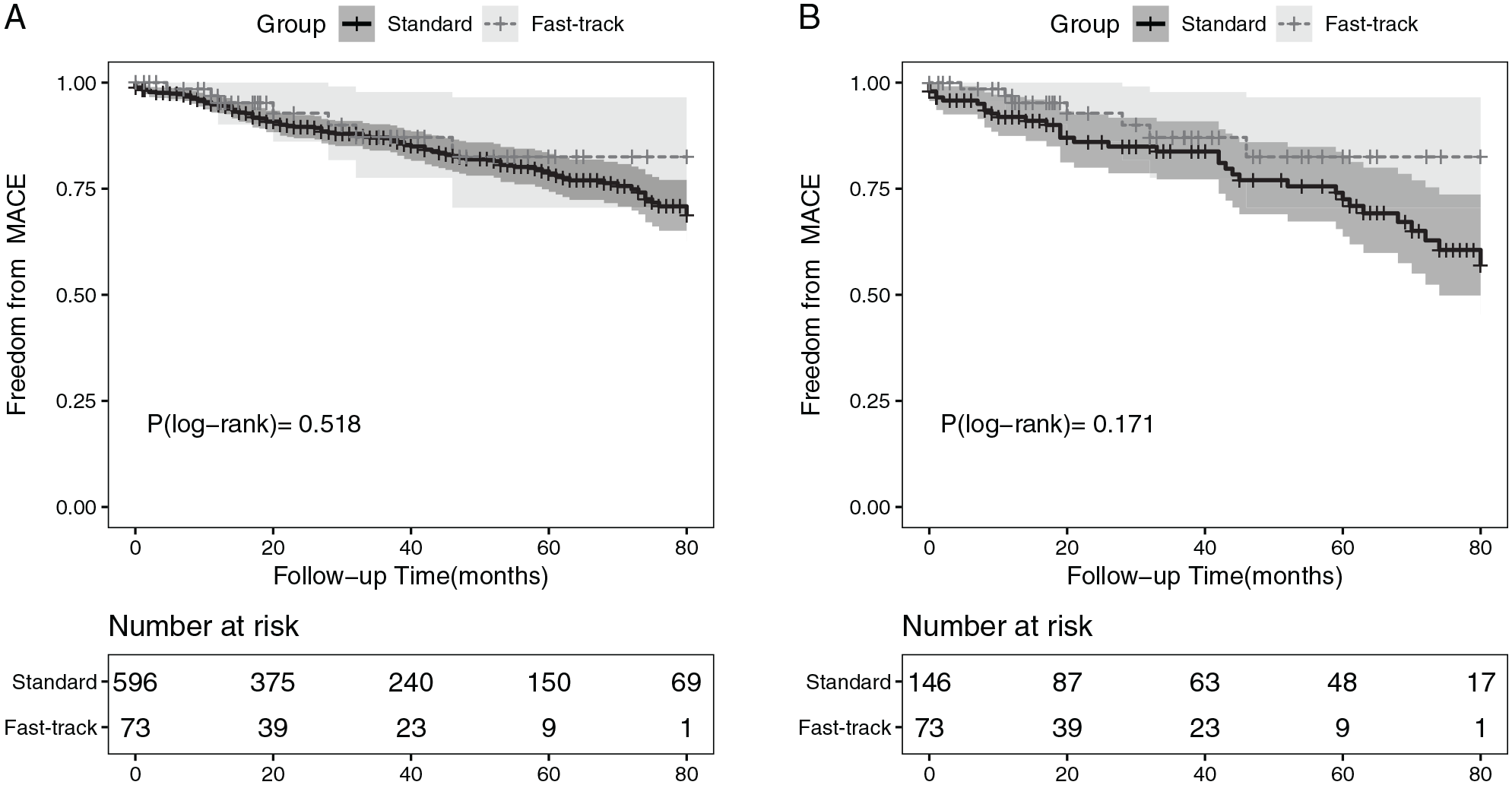
Kaplan–Meier curves of freedom from major adverse cardiac events in crude (A) and propensity score–matched (B) cohorts. MACE, major adverse cardiac events.
In the crude analysis, no significant difference was found between groups in terms of MACE (HR 0.78, 95% CI [0.36, 1.68], p=0.519) and cardiac death (HR 0.59, 95% CI [0.08, 4.46], p=0.610). In the PS-matched analysis, MACE occurred in 41 (18.7%) patients, with 7 (9.6%) in fast-track group and 34 (23.3%) in the standard control group (Figure 2B). No significant difference was found between the group regarding MACE (HR 0.57, 95% CI [0.25, 1.29], p=0.176) and cardiac death (HR 0.39, 95% CI [0.05, 3.23], p=0.381). Similar results of MACE and cardiac death were found in sensitivity analyses (Table 3, Supplementary Table 4).
In the subgroup of patients with shorter time interval within 2 weeks, no increasing risk of MACE was found in crude analysis (HR 0.71, 95% CI [0.31, 1.63], p=0.423) and in PS-matched analysis (HR 0.48, 95% CI [0.20, 1.16], p=0.104). No difference was found in terms of cardiac death between groups in either crude analysis (HR 0.63, 95% CI [0.08, 4.77], p=0.657) or PS-matched analysis (HR 0.37, 95% CI [0.04, 3.00], p=0.349). As for patients with high ACCI, both crude (HR 0.71, 95% CI [0.33, 1.54], p=0.382) and matched (HR 0.73, 95% CI [0.31, 1.71], p=0.466) analyses suggested no significant difference regarding MACE. No significant difference was found in terms of cardiac death in either crude analysis or PS-matched analysis. The results of the sensitivity analyses were consistent with previous results (Table 3, Supplementary Table 5).
Overall Mortality in Midterm Follow-Up
Regarding overall mortality, a total of 91(13.6%) patients died during follow-up. Death of all causes occurred in 86 (14.4%) patients in the standard control group as compared with 5 (6.8%) patients in the fast-track group. No significant difference was found in crude analysis (HR 0.63, 95% CI [0.25, 1.55], p=0.315, Figure 3A) or PS-matched analysis (HR 0.43, 95% CI [0.17, 1.11], p=0.820, Figure 3B). Similarly, no significantly decreased risk of overall mortality was found in sensitivity analyses (Table 3, Supplementary Table 4).
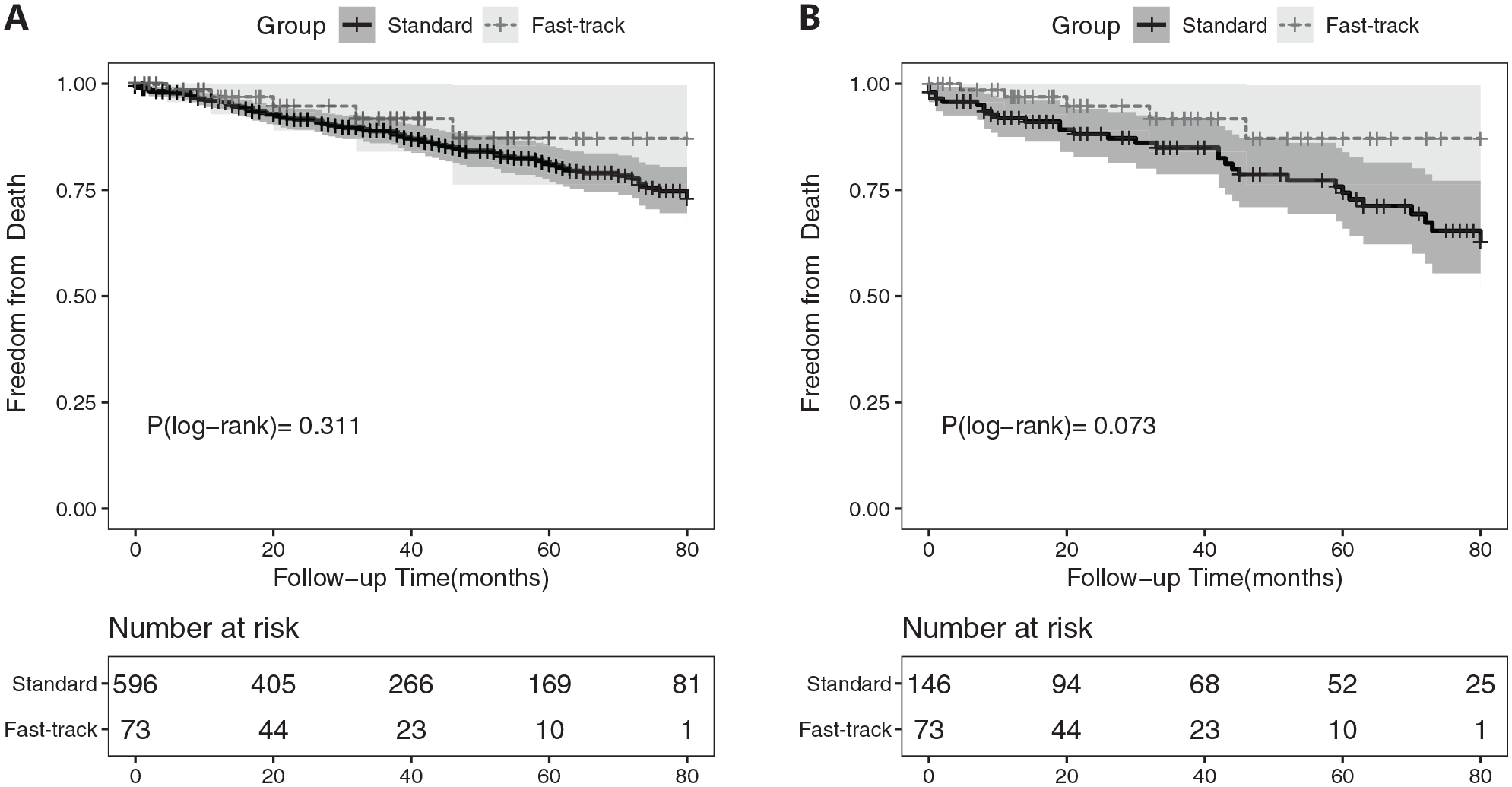
Kaplan–Meier curves of freedom from overall mortality in crude (A) and propensity score–matched (B) cohorts.
In the subgroup analysis in patients who received EVAR within 2 weeks after PCI, crude analysis suggested no difference regarding overall mortality (HR 0.54, 95% CI [0.20, 1.48], p=0.231). In PS-matched analysis, no increasing risk of overall mortality was found between groups (HR 0.36, 95% CI [0.12, 1.02], p=0.055). Notably, reduced risk of overall mortality was found in the CAPS (HR 0.34, 95% CI [0.12, 0.98], p=0.045) and time-adjusted PS analyses (HR 0.33, 95% CI [0.11, 0.96], p=0.042, Supplementary Table 4).
After stratification by ACCI, no significant difference was found in crude and PS-matched analyses in terms of overall mortality. Improved of overall mortality was associated with PCI in time-adjusted PS analysis (Supplementary Table 5).
Aneurysm-Related Adverse Events in Midterm Follow-Up
For aneurysm-related outcomes, a total of 44 (6.6%) patients suffered from aneurysm-related adverse events, with 5 (6.8%) aneurysm-related reinterventions in the fast-track group and 11 (1.8%) aneurysm-related death and 33 (5.5%) aneurysm-related reinterventions in the standard control group. No significant difference was found in either crude analysis (HR 1.70, 95% CI [0.66, 4.35], p=0.273) or PS-matched analysis (HR 2.45, 95% CI [0.75, 8.01], p=0.138) regarding aneurysm-related adverse events. No significant difference was found in the sensitivity analyses.
For aneurysm-related reintervention, no significant difference was found between groups regarding the aneurysm-related reintervention (HR 1.95, 95% CI [0.75, 5.07], p=0.168) in crude and PS-matched analysis (HR 2.59, 95% CI [0.78, 8.63], p=0.122), which were consistent in sensitivity analyses and subgroup analyses (Table 3, Supplementary Tables 4 and 5).
Discussion
Specific recommendations for the optimal interim between EVAR and PCI were still controversial due to limited and conflicting evidence. Compared with previously related outcomes, our study presented short-term and midterm outcomes of fast-track management of concurrent PCI in patients scheduled for EVAR.
Upon a series of PS analyses, our study suggested that EVAR for patients with a short time interval within 1 month or even shorter after PCI compared with those without CAD (normal cardiac risk) was comparable regarding the risk of MACE, overall mortality, major hemorrhage events, and aneurysm-related outcomes. However, it should be noted that more hemorrhage events occurred in the fast-track population.
Coronary artery revascularizations, mostly by PCI, prior to EVAR were more frequenting patients with high risk for the purpose of reducing the cardiac risk of surgery in our center. Compared with the standard control group, patients in the fast-track group showed poorer baseline characteristics, with more males, smoke history, and higher prevalence of comorbidities. To address this problem, PS analyses accounting for demographics, comorbidities, operation, and aortic anatomic factors were performed to achieve a balanced baseline, which provided several important implications for clinical practice.
First, our study provided evidence that a short time interval between PCI and EVAR might not increase the risk of MACE and overall mortality. Traditionally, coronary stent thrombosis, a catastrophic cardiac complication, was believed to be associated with surgically induced proinflammatory and prothrombotic effects. 23 The highest risk of in-stent thrombosis was found in the first 4 to 6 weeks after PCI in older observation studies. 6 However, most of the patients with indications for coronary artery revascularization in our study received EVAR within 2 weeks after PCI showing similar outcomes as those without significant CAD, showing a numerical but nonsignificant decrease in overall mortality, and the results were consistent in subgroup analyses of patients with high ACCI, which further indicated the feasibility of the fast-track management of concurrent PCI in AAA. The prothrombotic context, which was also associated with untreated AAA, might be normalized 12 months after EVAR, although it might be enhanced at an early stage after aneurysm repair. 24 However, this result should be considered carefully, as those patients with severe CAD who were unsuitable for fast-track management were excluded in our study.
Second, EVAR could be safely performed without cessation of DAPT regarding major hemorrhage events. Previous studies have been based mainly on noncardiac surgery, including not only endovascular procedures, but also open procedures. The hemorrhage risk of those surgeries might outweigh the increased thrombotic risk caused by cessation of dual antiplatelet therapy. 25 Balance between thrombosis and hemorrhage was difficult to achieve in most noncardiac surgeries, so a recommendation of delaying the surgery after PCI was given. However, EVAR, a minimally invasive procedure, was physically associated with less hemorrhage risk and trauma. To date, the relationship between the presence of DAPT during endovascular procedures and hemorrhagic complications was unclear, but hemorrhage complications were common after endovascular procedures and were believed to be associated with a significant increase in mortality.26,27 Our study suggested that patients who received EVAR without cessation of DAPT preoperatively for 1 month, even 2 weeks after PCI, had a similar risk of major hemorrhage events, which was consistent with a previous study, 11 in which repair of aortic aneurysms was performed within 8 weeks after PCI. Femoral access was mostly obtained via surgical cut down. Access analysis was limited by the small sample size of our study. However, a recent meta-analysis found that the rate of would complications was similar in surgical cut down and percutaneous procedures based on the results of randomized clinical trials (RCTs). 28 Notably, total hemorrhage events occurred more frequently in patients with PCI in crude analysis and IPTW analysis, although the PS-matched analysis and CAPS analysis suggested no significant difference between groups. Thus, the risk of hemorrhage should also be carefully considered even in endovascular procedures.
Third, any delay in AAA repair, a time-sensitive operation, might pose patients at a risk of rupture. A previously study indicated that patients who underwent AAA repair more than 2 weeks after coronary revascularization had higher mortality (33%), and all of those died because of rupture of AAA. 29 The guideline of American College of Cardiology 30 recommends that noncardiac surgery in patients treated with drug-eluting stents should be delayed 6 months, while a suggested upper limit interval from referral to treatment was 8 weeks according to ESVS. 4 It was reported that combined CABG and AAA repair had a 30-day mortality of approximately 7.8%. 31 PCI with EVAR was considered a less-invasive procedure that could have a lower mortality. 9 The rupture risk of aneurysms increased with increasing of aneurysm diameter. About 3.5% of untreated AAA with diameter of 5.5-5.9cm ruptured in 6 months, and about 12.8% of untreated AAA ruptured in 6 months if the diameter reached 7 cm. The 1-year risk of rupture wound increase to 9.4% for aneurysms of 5.5 to 5.9 cm, and 34% for aneurysms of more than 7 cm.30,32,33 While in fast-track group, the short-term rate of MACE was about 1.3% and the rate of midterm MACE was about 10%. Thus, the advantage of fast-track management of PCI before EVAR may exceed the risk of potential MACE in patients with AAA larger than 5.5 cm. In addition, patients with an AAA diagnosis might face a risk of psychological problems. Preoperative anxiety and depression occurred in about 40% of patients scheduled for AAA repair in our center, as noted in a previous study, 34 and psychological well-being and mental illness were found to be associated with worse outcomes in recent studies, 7 which stressed the importance of keeping waiting time at a minimum.
Limitation
The findings of this study should be considered carefully in the context of limitations. First, our study was a retrospective observational study; inevitably, selection and recall bias may exist in our study. But we performed PS-matched analysis to address potential bias of the cohort, and the consistent results with the crude analysis suggested the reliability of our results. Second, it would be ideal if we could include patients that have a prior cardiac intervention over 2 weeks before EVAR as another “custom-track” group, but unfortunately, such patients are few in our center. Therefore, we selected a stricter “coronary healthy” population without significant CAD as the standard control group, which could provide a general perspective of the MACE risk after EVAR. Third, we did not collect the detailed values of the cardiac biomarkers, thus we could not fully exclude subclinical cardiac events in the standard control group, and analysis of femoral access was limited by the small sample size of our study, so we did not collect the detailed numbers of percutaneous and cutdown procedures that may have played on bleeding complications. Fourth, the median follow-up time for fast-track group was shorter than the standard control group, and the sample size for fast-track group was small. To address this problem, we also performed sensitivity analyses with follow-up time as an additional factor for estimating the PS, and the results were similar as other analyses, which further confirmed the robustness of our results. We are also conducting a prospective cohort study enrolling more patients with fast-track management, hoping to provide higher levels of evidence with larger sample sizes.
Conclusions
After accounting for demographic, operative, and anatomical confounders, our PS-matched results provide new evidence regarding the safety and efficacy of fast-track management of concurrent PCI in patients scheduled for EVAR. Under appropriate perioperative cardiovascular care, those patients who need both PCI and EVAR could be safely treated with a fast-track approach, with EVAR after PCI in 1 month or even 2 weeks. Further prospective studies in larger samples are needed to validate the robustness of our findings.
Supplemental Material
sj-docx-1-jet-10.1177_15266028221105179 – Supplemental material for Fast-Track Management of Concurrent Percutaneous Coronary Intervention in Patients Scheduled for Endovascular Abdominal Aortic Aneurysm Repair
Supplemental material, sj-docx-1-jet-10.1177_15266028221105179 for Fast-Track Management of Concurrent Percutaneous Coronary Intervention in Patients Scheduled for Endovascular Abdominal Aortic Aneurysm Repair by Chengxin Weng, Jiarong Wang, Jichun Zhao, Yukui Ma, Bin Huang, Yi Yang, Ding Yuan, Tiehao Wang and Xiyang Chen in Journal of Endovascular Therapy
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Sichuan Foundation of Science and Technology (grant number: 2020YFS0247).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.