
Abstract
Purpose:
Ruptured abdominal aortic aneurysm (AAA) is almost always considered fatal without open surgical or endovascular repair. We report a case that has defied this norm and explore the possible factors involved in this exceedingly rare outcome.
Case Report:
An 87 year old gentleman presented with an acute ruptured AAA with left retroperitoneal hematoma. He was counseled for emergent repair, but opted for conservative management instead. He has remained well at the time of writing, 13 months from the rupture, with clinical resolution of symptoms along with radiological resolution of the hematoma.
Conclusion:
Timely repair remains the mainstay of management for ruptured AAA, although this rare case highlights that it is possible for ruptured AAA to seal spontaneously with patient surviving up to 13 months. We have sought to hypothesize the factors in this case that may have contributed to prolonged survival following untreated ruptured AAA.
Clinical Impact Statement
While the overwhelming evidence is that a ruptured AAA left unrepaired is fatal, our case report illustrates a rare case that shows it is possible for ruptured AAA to seal spontaneously, with patient surviving up to 13 months. We seek to hypothesize the factors that may contribute to such prolonged survival.
Introduction
We report a case of a gentleman who survived an unrepaired ruptured abdominal aortic aneurysm (AAA) for 13 months, at the time of writing.
Case Report
The patient is an 87 year old gentleman with good premorbid functional status and independent in activities of daily living, and past medical history of hypertension, hyperlipidemia, and previous heroin addiction. He presented to the Emergency Department (ED) in April 2021 for acute left-sided abdominal pain of 1 day duration and giddiness. There was no chest pain, back pain, or syncope. On arrival, he had a borderline low blood pressure of 87/60 mm Hg, heart rate 70 bpm, and was saturating well on room air. On examination, he was alert, conversant, and comfortable. He had an expansile abdominal mass and differential upper limb systolic blood pressure: 60 mm Hg on the left and 121 mm Hg on the right. Bilateral foot pulses were present with no trash feet.
There was no previous abdominal or vascular imaging. A point of care ultrasound scan in the ED revealed an AAA of 7 cm diameter with no pericardial effusion. An emergent computed tomography (CT) aortogram revealed a ruptured fusiform infrarenal AAA measuring 7.5 × 7.4 × 6.0 cm3 (anterior-posterior diameter × width × cranio-caudal length) (Figure 1). There was an associated left retroperitoneal hematoma measuring 4 × 6 × 11 cm3, without active contrast opacification. Proximal neck length of the AAA was 4.4 mm, neck diameter 17.3 mm, and neck angle 21.5° (Figure 2).
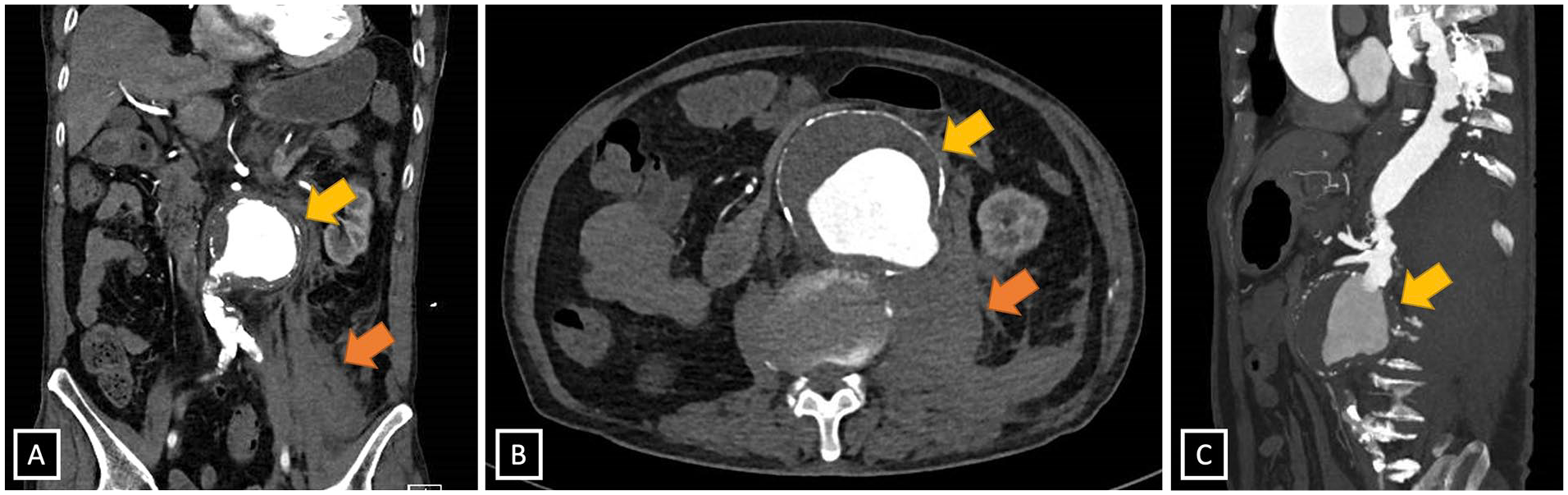
Computed tomography (CT) aortogram images showing acute ruptured infrarenal abdominal aortic aneurysm (AAA): (A) coronal, (B) axial, and (C) sagittal. Yellow arrows indicate the aneurysm, with likely site of rupture being the posterolateral aspect. Orange arrows indicate the left retroperitoneal hematoma.
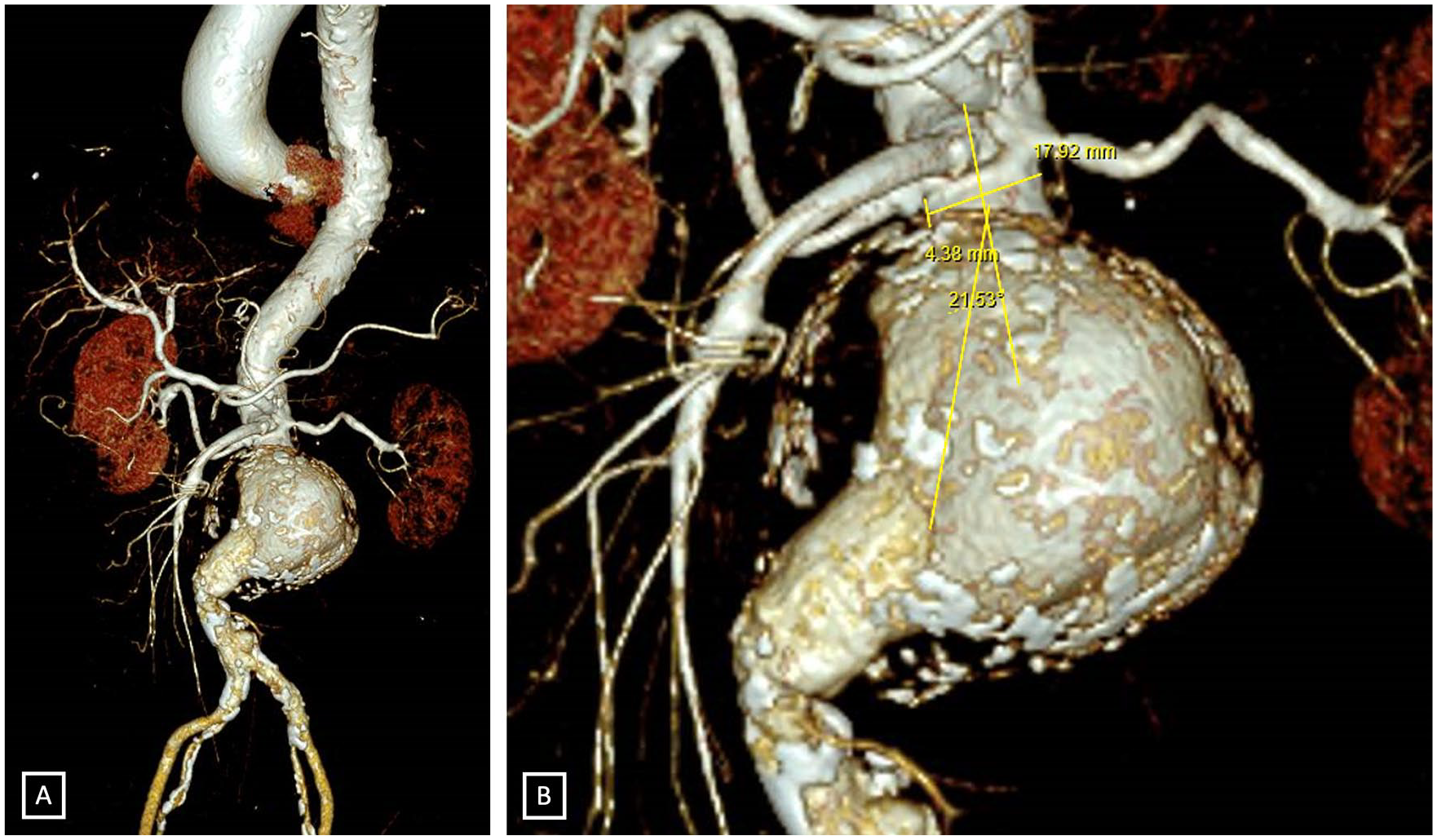
(A) A 3-dimensional reconstruction showing the morphology of the aneurysm. (B) The short proximal neck length of the abdominal aortic aneurysm (AAA) made emergent endovascular aneurysm repair (EVAR) technically challenging.
Laboratory investigations revealed hemoglobin drop from a baseline of 15 to 11.7 g/dL on arrival. Hematocrit was slightly decreased at 36.3%. The patient had a high anion gap metabolic acidosis, with a bicarbonate of 14.2 mmol/L, pH 7.181, base excess –10.0 mmol/L, and lactate 10.4 mmol/L on arrival. The patient also had acute kidney injury with a creatinine of 258 umol/L, on a background of chronic kidney disease (baseline creatinine 110 umol/L). The patient was fluid resuscitated with crystalloids, and 1 pint of packed red blood cells transfusion was pre-emptively started in the ED. The electrocardiogram did not show any ischemic changes.
The surgical on call team was urgently activated and the patient was reviewed by a vascular senior consultant within 30 minutes of activation. The patient had been duly prepared for emergency operation; however, the patient himself was adamant not to undergo surgery. An urgent family conference was held between the vascular team, patient, and family. The team counseled that the patient had a ruptured AAA which was immediately life-threatening, and without intervention, the patient would die through exsanguination in a matter of hours to days. Open surgical repair of the AAA was recommended. The alternative of an endovascular aneurysm repair (EVAR) was also discussed, but in view of the short proximal neck and atherosclerotic aorta which would negatively affect the proximal seal, EVAR would have a high chance of technical failure. Complex EVAR such as chimney EVAR was considered, but the patient remained resistant toward all types of surgery. While the family was keen for surgery, the patient communicated clearly that he did not want surgery and wished for palliation. He understood the information and the consequences of rejecting surgery (counseled on certain death), could retain the information, weigh the benefits and risks of the options provided, and was deemed to be mentally competent.
The palliative medicine team was consulted for end-of-life management and titration of opioid analgesia, and the patient was subsequently transferred to an inpatient hospice. The patient was hydrated appropriately until resolution of acute kidney injury. Serial hemoglobin checks remained stable at 11 to 12 g/dL without further transfusions. Systolic blood pressure was controlled at 100 to 120 mm Hg.
A CT aortogram was repeated 2 months later for prognostication, which showed interval increase in size of the aneurysm, measuring 7.6 cm × 10.0 cm × 8.0 cm, and with reduction in size of the left retroperitoneal hematoma (Figure 3). As the patient remained stable and comfortable throughout his hospice stay, he was discharged in the third month.
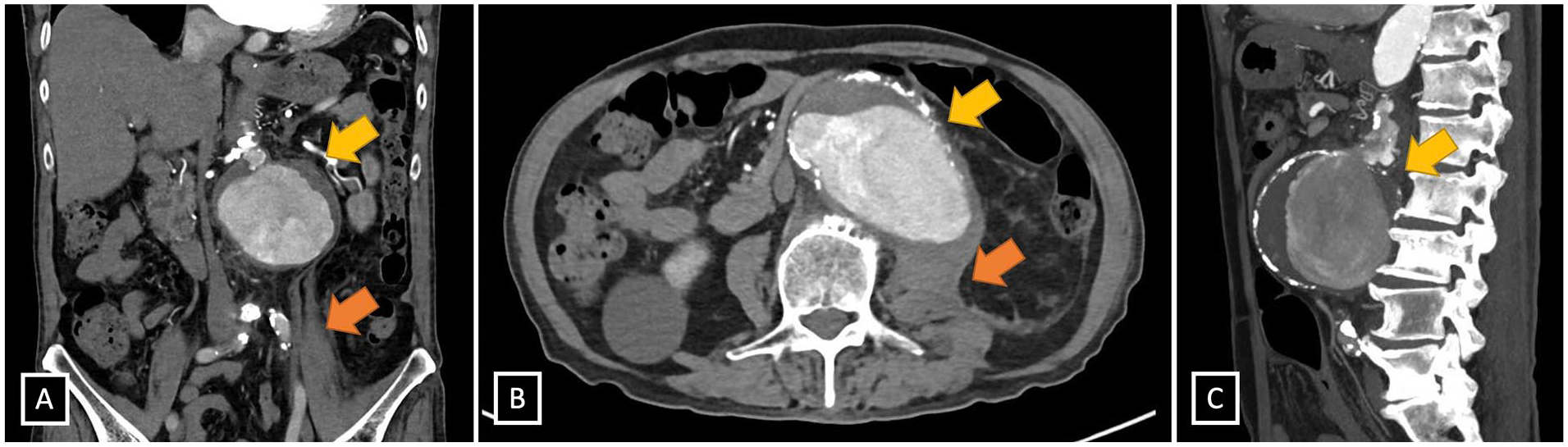
Computed tomography (CT) aortogram images 2 months post rupture: (A) coronal, (B) axial, and (C) sagittal. Yellow arrows indicate the aneurysm. Image B shows the “draped aorta” sign pathognomonic of contained rupture of abdominal aortic aneurysm (AAA)—the posterior wall of the AAA molds and drapes over the anterior surface of the vertebra. Orange arrows indicate the left retroperitoneal hematoma, which has reduced in size.
The patient has subsequently been seen twice in the vascular clinic, and continues to follow-up every 2 monthly with his family doctor. He has remained well with no abdominal pain, is off analgesia, and is fully independent in activities of daily living. Interval elective aneurysm repair (both open surgical and endovascular techniques) has been discussed with the patient in clinic, and he has been counseled on the continued high risk of free rupture, but he remains keen for conservative management. The latest CT aortogram in November 2021 (7 months post rupture) showed that the aneurysm has remained approximately stable in size, now 8.4 cm × 11.5 cm × 8.3 cm (Figure 4). The left retroperitoneal hematoma has resolved.
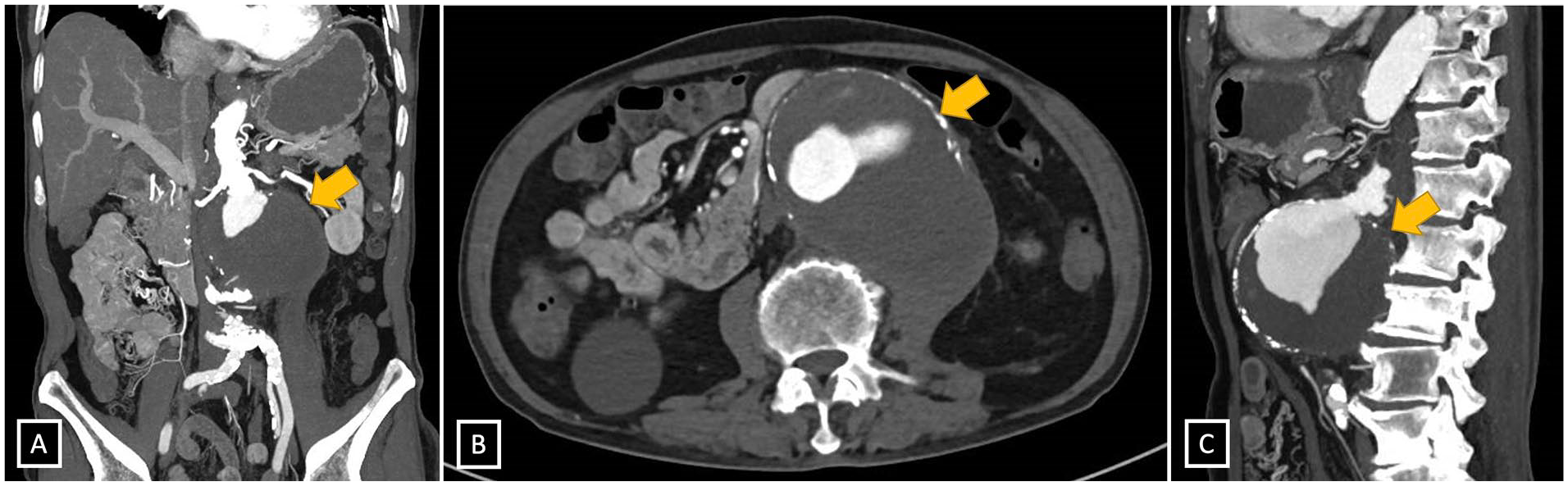
Computed tomography (CT) aortogram images 7 months post rupture: (A) coronal, (B) axial, and (C) sagittal. Yellow arrows indicate the aneurysm sac, which has remained stable in size. The left retroperitoneal hematoma has resolved.
Discussion
It is widely accepted that a ruptured AAA, without any form of surgical intervention, is almost uniformly fatal, with death usually occurring within hours to a week of rupture. 1 The mortality associated with ruptured AAA (with or without treatment) has been reported to be as high as 81%.2,3 Even if the patient is able to survive through a surgery, mortality following open repair of ruptured AAA remains 30% to 50%.4,5 EVAR for ruptured AAA is associated with less perioperative morbidity, but not all patients are candidates for EVAR due to limitations with vascular anatomy and the time-sensitive nature of ruptured AAA repair.
There is a dearth of studies and reports regarding survival from unrepaired ruptured AAAs in literature. We have collated the available literature in Table 1. For patients with ruptured AAA who decided not to be operated on, average time to death was 7 hours in 1 study of 21 patients, with the longest survival being 6 days. 6 Median survival was 16.5 hours in a retrospective study of 56 patients, 7 and 2.2 hours in another study of 57 patients. 8 In the latter study, a subgroup analysis of 26 hemodynamically-stable patients revealed that survival after 2 hours was 96%, showing that this group can have longer survival than patients who are hemodynamically unstable. However, death remained the invariable outcome among this group of patients. 8 This makes a case like ours exceedingly rare. Still, it is worth noting that it may not be unique—in one case report, there was a patient who survived up to 5 months after an unrepaired ruptured AAA. 9
Tabulated Studies and Case Reports of Patients With Unrepaired Ruptured AAAs in the English Literature, and the Recorded Time to Death.
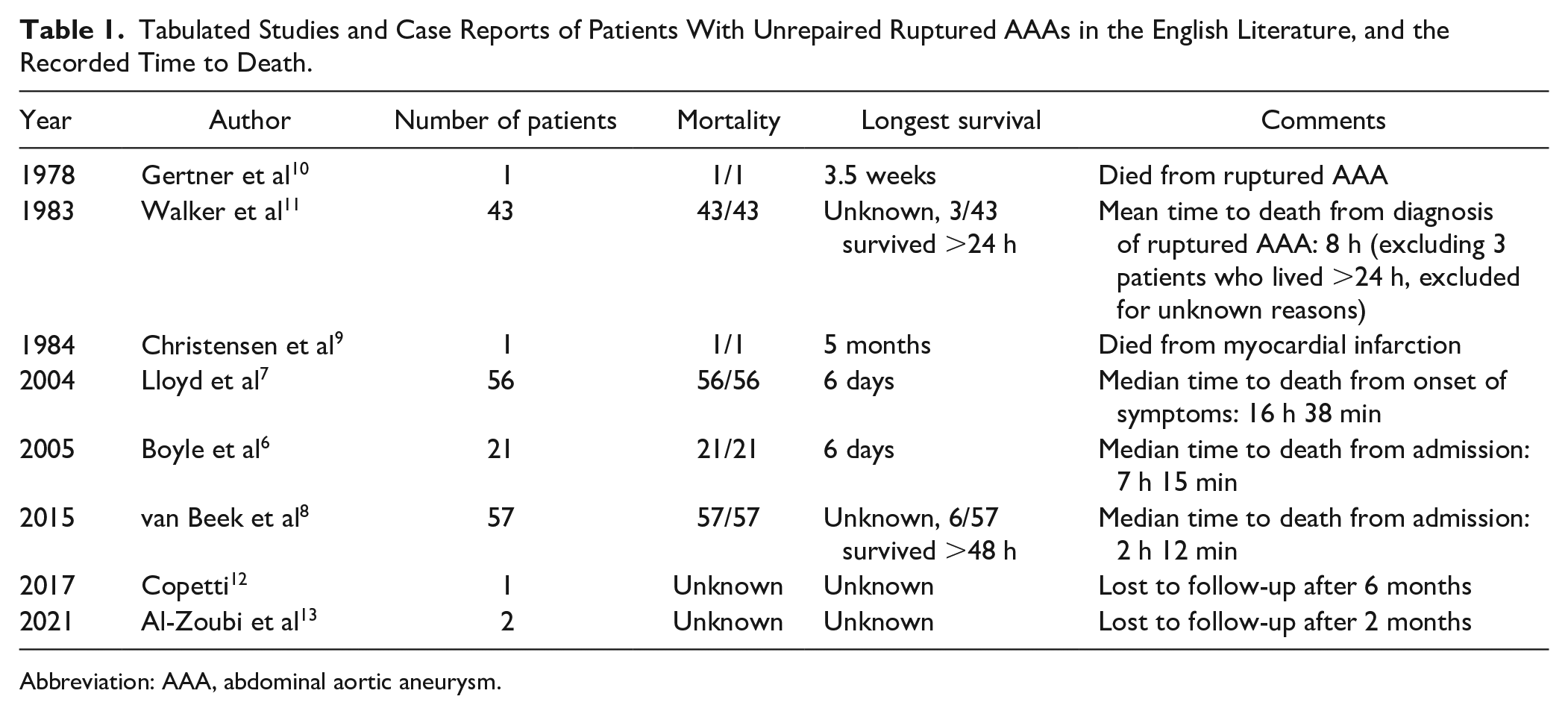
Abbreviation: AAA, abdominal aortic aneurysm.
We can postulate possible reasons that this patient may have survived a ruptured AAA. A case series of chronic sealed AAAs determined that for a perforation to be sealed off, it requires 2 events—slow hemorrhage and high resistance of surrounding structures. 14 The initial CT aortogram did not show any contrast blush, with the tear in the aortic wall not obviously seen on imaging, suggesting that any tear in the wall was likely to be minor. The patient was relatively stable with a borderline blood pressure which suggested that hemorrhage was likely to be slow. In fact, permissive hypotension (keeping systolic blood pressure 80–100 mm Hg) prevents further shearing of the aortic wall and helps limit blood loss. 15
Second, the bleeding was likely tamponaded by surrounding structures. The aneurysm ruptured posterolaterally into the retroperitoneal space, which is bounded by tough fascia that limits blood loss. A contained hematoma developed in the left infrarenal space, which is a “high resistance” space bounded by the anterior renal fascia, which fuses with preaortic fascia and the posterior renal fascia, which fuses with the fascia of the psoas major—This would have effectively encapsulated the hemorrhage. It has also been hypothesized that for large aneurysms, the chronic process of enlargement results in increased adherence to the surrounding structures, which results in a stronger perianeurysmal reaction that can more effectively contain a rupture. 14
There is still a risk that the rupture will reopen and result in catastrophic massive hemorrhage. 14 Therefore, interval elective surgical repair of the AAA is still recommended, as long as the patient consents. But we remain hopeful for the outcome of this patient and are glad to know that he has regained independence in his activities of daily living, with a meaningful quality of life.
Conclusion
Ruptured AAA remains almost invariably fatal in patients who are untreated, and immediate repair is still the mainstay of management. This report describes a rare case of medium-term survival following unrepaired ruptured AAA.
Footnotes
Acknowledgements
The authors would like to acknowledge the support of the Department of General Surgery in Sengkang General Hospital.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.