
Abstract
Introduction:
Women are generally underrepresented in trials focusing on aortic aneurysm. Nevertheless, sex-related differences have recently emerged from several studies and registries. The aim of this research was to assess whether sex-related anatomical disparities existed in fenestrated and branched aortic repair candidates and whether these discrepancies could influence endovascular repair outcomes.
Methods:
Data from all consecutive patients treated during the 2008–2019 period within the Italian Multicenter fenestrated or branched endovascular aortic repair (F/BEVAR) Registry were included in the present study. Propensity matching was performed using a logistic regression model adjusted for demographic data and comorbidities to obtain comparable male and female samples. The selection model led to a final study population of 176 patients (88 women and 88 men) among the total initial cohort of 596. Study endpoints were technical and clinical success, overall survival, aneurysm-related death, and reintervention rates evaluated at 30 days and during follow-up.
Results:
Twenty-eight patients (15.9%) received urgent/emergent repair. In most of the cases (71.6%), women received treatment for extensive thoracoabdominal pathology (Crawford type I, II, or III aneurysm rather than type IV or juxta-pararenal) versus 46.6% of men (p=0.001). Female patients presented with more challenging iliac accesses with at least one side considered hostile in 27.3% of the cases (vs 13.6% in male patients, p=0.039). Finally, women had significantly smaller visceral vessels. Women had significantly worse operative outcomes, with an 86.2% technical success rate versus 96.6% in the male population (p=0.016). No differences were recorded in terms of 30-day reinterventions between men and women. The 5-year estimate of freedom from late reintervention, according to Kaplan-Meier analysis, was 85.6% in men versus 81.6% in women (p=ns). No aneurysm-related death was recorded during follow-up (median observational time, 23 months [interquartile range, 7–45 months]).
Conclusion:
Women presented a significantly higher incidence of thoracoabdominal aneurysms, smaller visceral vessels, and more complex iliofemoral accesses, resulting in a significantly lower technical success after F/BEVAR. Further studies assessing sex-related differences are needed to properly determine the impact on outcomes and stratify procedural risks.
Clinical Impact
Women are generally underrepresented in trials focusing on aortic aneurysms. Aiming to assess whether sex may affect outcomes after a complex endovascular aortic repair, a propensity score selection was applied to a total population of 596 patients receiving F/BEVAR aortic repair with the Cook platform, matching each treated female patient with a corresponding male patient. Women presented more frequently a thoracoabdominal aneurysm extent, smaller visceral vessels, and complex iliofemoral accesses, resulting in significantly worse operative outcomes, with an 86.2% technical success versus 96.6% (p=0.016). No differences were recorded in terms of short-term and mid-term reinterventions. According to these results, careful and critical assessment should be posed in case of female patients receiving complex aortic repair, especially regarding preoperative anatomical evaluation and clinical selection with appropriate surgical risk stratification.
Keywords
Introduction
Aortic aneurysms are more common in men than in women, with increased risk of late diagnosis and rupture in female patients. 1
The impact of sex differences regarding abdominal aortic aneurysm (AAA) treatment has been deeply investigated2–8; indeed, the most recent European Society for Vascular Surgery guidelines indicate different thresholds for AAA correction in women and men. 9
Nevertheless, mainly due to different rates of prevalence, women were generally underrepresented in most of the trials aiming to assess clinical outcomes after surgical or endovascular AAA repair.10–14
Recent technological advancement and dedicated material availability have led to an increased number of patients receiving endovascular aortic repair, for both infrarenal and thoracoabdominal aneurysms, the latter with fenestrated or branched endovascular aortic repair (F/BEVAR).
Despite all the implications deriving from sex divergence within cardiovascular diseases not being fully understood yet, they may play a role in outcome differences between men and women after F/BEVAR, which appear to be even more significant than those in patients treated for infrarenal aneurysms.
The aim of the present study was to assess whether sex may affect outcomes after a complex endovascular aortic repair in a broad cohort of patients from a national multicenter F/BEVAR registry.
Materials and Methods
Italian Multicenter Fenestrated and Branched Study Registry
Data from all consecutive patients intended to be treated in 4 Italian Academic centers (Bologna S. Orsola-Malpighi hospital, Perugia Santa Maria della Misericordia hospital, Florence Azienda Ospedaliero-Universitaria Careggi hospital, and Milan Università Vita-Salute S. Raffaele hospital) with F/BEVAR using the Zenith Cook platform during the 2008–2019 period were included in a prospective electronic database. All the data were shared once anonymized according to the European General Data Protection Regulation so that each patient was deidentified with a coding number. It was a voluntary, observational, multicenter, and retrospective registry (Italian Multicenter F/BEVAR Registry [IMFB Registry]). The study was approved by the local institutional review boards.
Each patient signed a written consent form for anonymous use of data regarding surgery and follow-up for scientific purposes. No funding was obtained from companies or other institutions for this research. 15
Registry Cohort
Patients with thoracoabdominal aortic (TAAA), pararenal, or juxtarenal aneurysms were enrolled in the registry, and visceral arteries were revascularized using either fenestrations or antegrade branches depending on the anatomy. Both patients presenting with a degenerative and post-dissecting aortic aneurysm were included in the study cohort. When using custom-made endografts, the configuration was designed in co-operation with the Cook planning center and the performing physician, while in the case of an off-the-shelf device such as T-branch, case planning and feasibility were left to the surgeon’s discretion. A detailed evaluation of the aortoiliac and visceral vessels was performed analyzing each preoperative computed tomography angiography scan and measuring arterial diameters, calcification, tortuosity, and eventual stenosis, using dedicated workstations allowing multiplanar, 3-dimensional reconstructions and central lumen line analysis.
As several patients received a staged procedure, the enrollment for each case was decided as per intention to treat, with the patients being included in the data set at the first procedural step. Patient demographics and preoperative clinical data were collected, including comorbidities and indication for treatment, according to the Society for Vascular Surgery reporting standards.16–18
A comprehensive analysis focusing on clinical outcome predictors from the IMFB Study registry was already published, providing detailed data on the entire registry cohort. 15
Endpoints: Statistical Analysis
As the entire cohort was highly unbalanced regarding sex distribution, with the aim of obtaining a more homogeneous population for properly comparing sex differences in the outcomes of patients treated with complex endovascular aortic reconstruction, a 1:1 automatic propensity matching was performed using a logistic regression model adjusted for demographic data and comorbidities. The model included all available risk factors listed in the shared electronic data set (age, obesity, hypertension, smoking, diabetes, dyslipidemia, chronic renal failure, chronic obstructive pulmonary disease, coronary artery disease, American Society of Anesthesiologists physical status classification, and peripheral artery disease). The matching method selected 1 man from the entire cohort for every treated woman. Anatomical features were not included in the model, allowing the natural inherent anatomical gender differences to persist. This methodological approach was preferred with the intention to underline proper sex-related characteristics and evaluate their eventual influence on results after complex aortic repair. By including each possible anatomical feature in the selection model, 2 almost-identical populations would have been created. As a result, eventual significant differences in patient’s outcomes after surgery would have been accountable to biohumoral or endocrine parameter rather than to characteristics more directly affecting interventional endovascular maneuvers.
An additional propensity-matched population was, however, selected, including aneurysm extent alongside the already considered variables, aiming to further disaggregate results.
Continuous data are expressed as mean±standard deviation or median and interquartile range (first quartile and third quartile) when appropriate and categorical variables as number of patients and percentages. For the comparison of categorical data, percentages were compared by 2-tailed χ2 test with a Yates correction and Fisher exact test, when appropriate. Continuous variables were compared with the Student t test.
A Kaplan-Meier analysis was performed to estimate long-term results. Estimates were considered reliable in case of standard error <0.10. The log rank test was used to compare survival distributions.
Outcomes of the study consisted of assessing whether there was a sex-related difference in the technical success, clinical success, overall survival, aneurysm-related death, and reintervention rates, at 30 days and during follow-up.
Technical success was defined as correct endograft deployment with target visceral vessel (TVV) patency without evident type I/III endoleak or limb occlusion at final angiography.
Clinical success was defined according to the reporting standards for endovascular aortic repair of aneurysms involving the renal-mesenteric arteries. 19
All statistical analyses, including propensity matching, were performed with SPSS software version 26 (IBM, Armonk, NY, USA). A 2-sided p value of less than 0.05 was considered to indicate a statistically significant difference in each case.
Results
Matching Results
During the study period, a total of 596 consecutive patients were scheduled to receive a treatment with F/BEVAR using the Zenith Cook platform for complex aortic disease.
Propensity matching was applied with the aim of obtaining a homogeneous cohort of male and female patients.
Overall, 85% (n=508) of the included patients were men, while with the 1:1 propensity score adjustment, a male patient was matched with each treated female patient using a binary logistic regression model considering the selected variables.
The selection model led to a final study population of 176 patients (88 women and 88 men).
A plot obtained after automatic propensity matching, showing standardized mean differences in the study cohort before and after matching, for the considered variables, can be found in the Supplementary Material.
The mean age at the time of the index procedure was 73.6±6.8 years, and most of the patients suffered from hypertension (97.2%) and dyslipidemia (70.5%).
Aortic aneurysm etiology was deemed as degenerative in 75.9% of the cases, as post-dissection in 7.4%, and as post-surgical in the remaining 13.1%.
Twenty-eight patients (15.9%) received urgent/emergent repair, 16 (9.1%) because of an aneurysm measuring more than 80 mm in axial diameter in a computed tomography scan, 8 (4.6%) for contained aneurysm rupture, and the remaining 4 patients for aortic pain. No statistical differences were detected between male and female patients on the distribution of urgent or ruptured aneurysm settings at the bivariate analysis.
Detailed baseline characteristics and risk factors in male and female patients before and after propensity matching are reported in Table 1.
Baseline Characteristics in the Study Cohort, Before and After Propensity Matching.
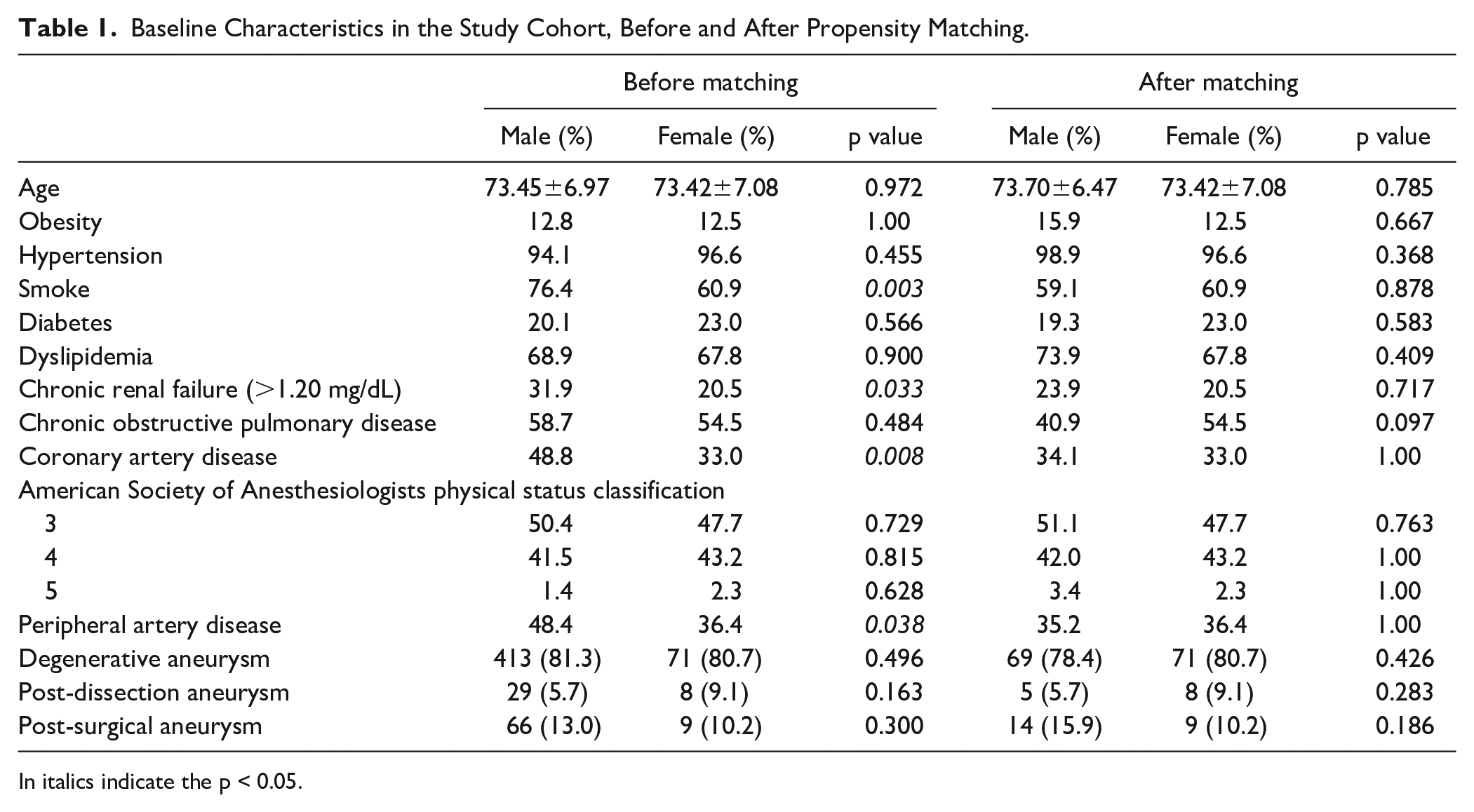
In italics indicate the p < 0.05.
Preoperative Anatomy
A comparison between male and female patients according to aortic aneurysm extent, anatomical complexity, and presence of hostile iliofemoral access was performed.
In the univariate analysis, a TAAA was a more common finding in female patients (86.5% vs 61.4%, p<0.0001), with 71.6% of women receiving treatment for extensive aneurysm disease (Crawford type I, II, or III) when compared with 46.6% for men (p=0.001). Conversely, a significant proportion of male patients were affected by a more localized aortic pathology as pararenal and juxtarenal aneurysms represented indication for treatment in 17.0% of male versus 4.5% of female patients (p=0.013) and 21.6% of male versus 9.1% of female patients (p=0.035), respectively.
Graft design distribution accurately reflected these anatomical differences in the 2 groups. Indeed, female patients received less frequently a fenestrated endograft (50.0% vs 68.2%, p=0.021), while other configurations had a homogeneous distribution (Table 2).
Type of Endograft Received (176 Patients [88 Men vs 88 Women]).

Note. ns = not significant.
With the aim of stratifying according to procedural complexity, patients receiving an aortic repair with at least 3 TVVs to revascularize were compared with others. No differences between male and female patients according to this complexity index were found in the selected population (90.9% complex procedures in women vs 83.0% in men, p=0.179).
Moreover, female patients resulted in having significantly smaller TVVs, as reported in Table 3.
Anatomical Features (176 Patients [88 Men vs 88 Women]).
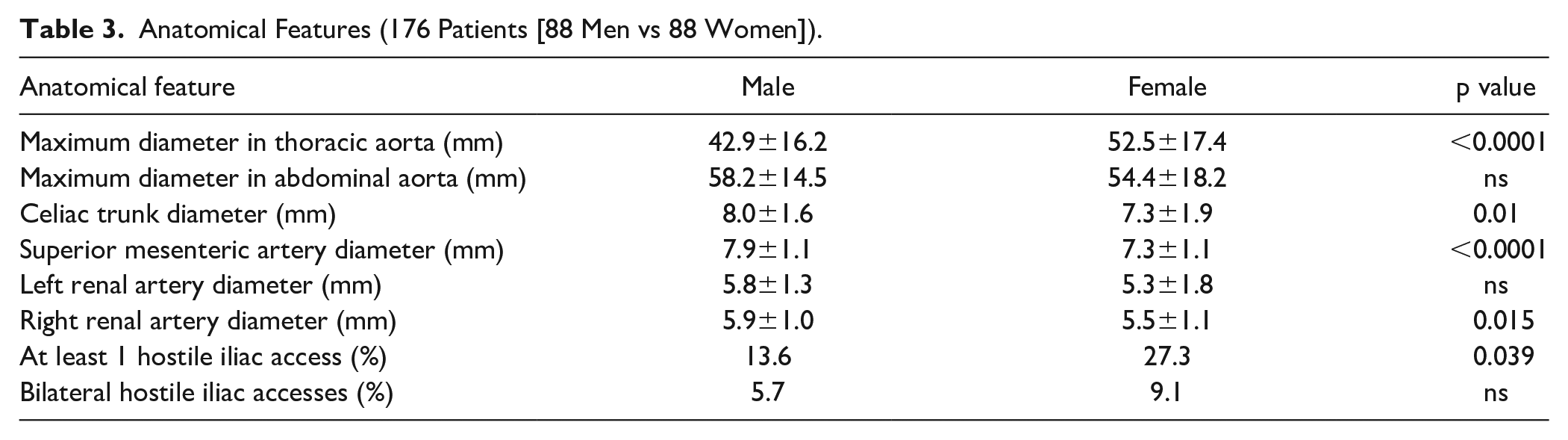
A composite endpoint considering vascular iliofemoral artery accesses was therefore assessed. Arterial access was considered hostile when the external iliac artery measured less than 7 mm in axial diameter 20 or in case of multiple stenosis or occlusion or circumferential calcification (more than 50% of internal lumen or more than 3 cm in length).
Female population presented more frequently with challenging iliac accesses with at least one side considered hostile in 27.3% of the cases (vs 13.6% in male patients, p=0.039).
As a consequence of the more extensive aortic disease in female patients, a staged procedure in 2 or more steps was more frequently applied to women (53.4% vs 30.7%, p=0.004), with the aim of minimizing postoperative onset of spinal cord ischemia.
A percutaneous access to advance the fenestrated/branched endograft was preferred in 23.7% of women and 14.8% of men (p=ns).
Thirty-Day Results
While no need for immediate surgical conversion and no mortality within the first 24 hours were observed, the technical success rate was 86.2% in women versus 96.6% in men (p=0.016).
Reasons for technical failure are detailed in Table 4. Women received a prophylactic cerebrospinal fluid drainage more frequently (51.7% vs 28.7% in men, p=0.003), but despite this, they developed a persistent (>24-hour postprocedural) symptomatic spinal cord ischemia in 15.9% of the cases (vs 5.7% in male patients, p=0.050). No differences were found in terms of perioperative (within 30 days from any aortic procedure) mortality in the 2 groups (6.8% female vs 4.5% in male, p=ns)
Technical Failures and Reasons for Failure.

Abbreviations: CTA, computed tomography angiography; LRA, left renal artery; POD, postoperative day; RRA, right renal artery; SMA, superior mesenteric artery.
Clinical success at 30 days was significantly higher in men than women (85.2% vs 67.0%, p=0.008)
Reinterventions and Follow-up
No differences were recorded in terms of early (within 30 days) reinterventions between male and female patients (10.2% vs 8.0%, respectively, p=ns). At a median follow-up of 23 months (interquartile range, 7–45 months), no differences in terms of 5-year overall survival according to the Kaplan-Meier estimate were recorded (70.3% male vs 60.3% female, p=ns, Figure 1).
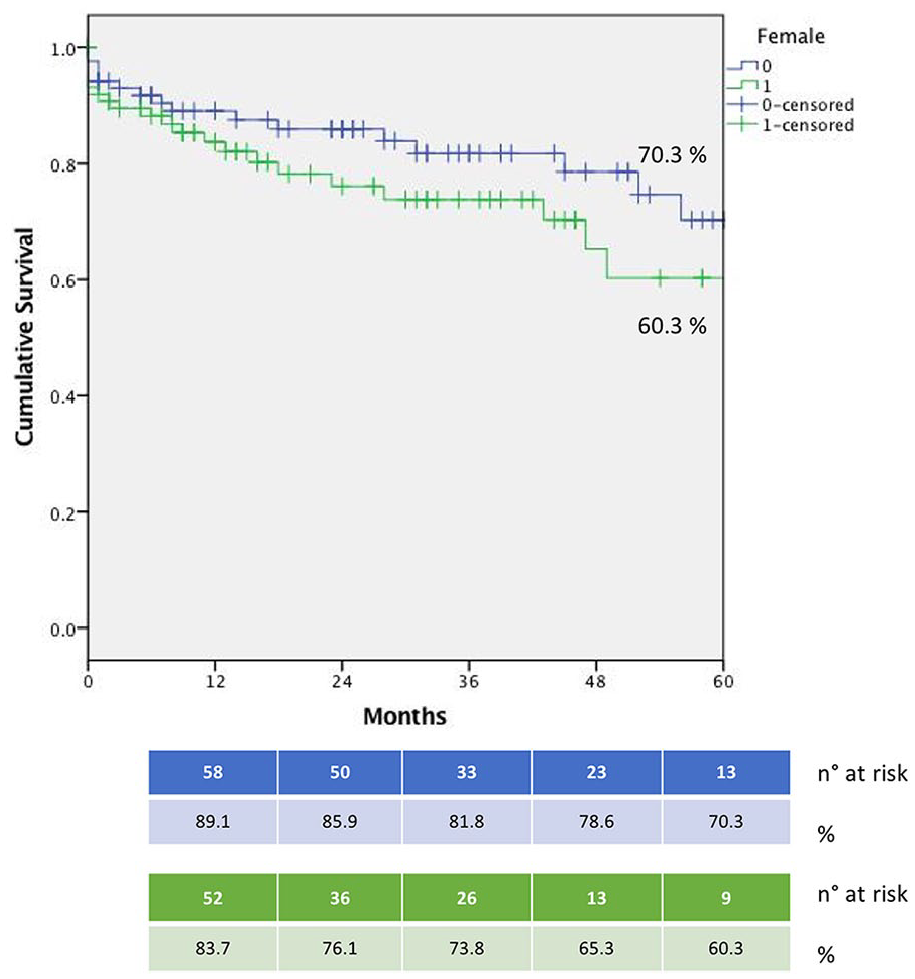
Overall survival for the selected population (males and females).
Besides perioperative period, no late aneurysm-related death was observed during follow-up in the entire study cohort.
One female patient died on postoperative day 75 after receiving a thoracic endograft implant, as the first step of a planned 2-stage procedure which would have been completed using a custom-made device. The death was not considered aneurysm-related because it was caused by acute respiratory failure.
Finally, 5-year freedom from late reintervention, defined as the absence of any secondary surgical or endovascular procedure beyond 30 days after aortic repair, estimated with the Kaplan-Meier analysis, was 87.3% in men and 84.1% in women (p=ns, Figure 2).
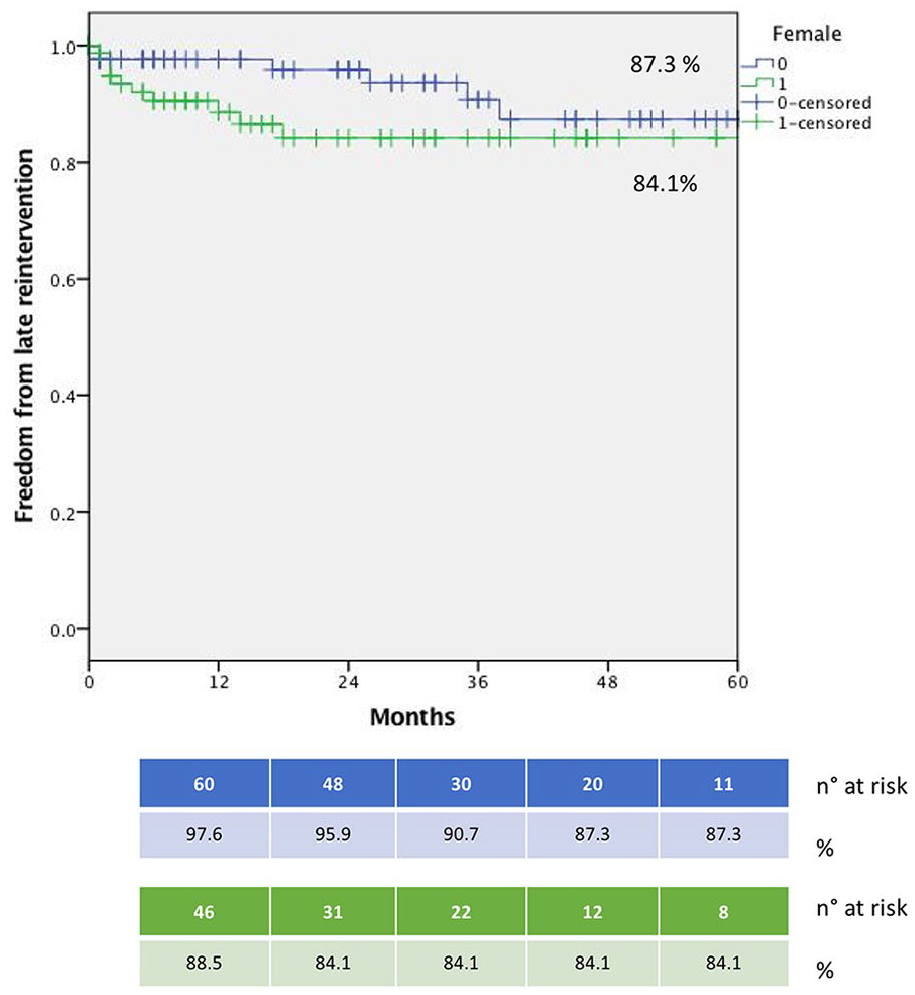
Survival rate free from any late reintervention (males and females).
Additional Assessment According to Pathology Extent
Aiming to further disaggregate results, eliminating other potential confounders, a second propensity matching was run, adjusting population selection also according to aneurysm extent, in addition to all variables included in the first model.
Even in this case, women reported worse outcomes with a technical success rate of 82.4% versus 92.9% in men (p=0.03)
Discussion
It is generally established how female patients undergoing infrarenal aortic aneurysm repair, whether open or endovascular, mostly report worse outcomes.21–23
Several studies investigated gender differences in open thoracoabdominal aortic repair, confirming how women are more prone to develop complications also in case of more extended aortic treatment.24–26
The present analysis aimed to assess whether sex differences could affect endovascular complex aortic procedures as well.
Few researches are currently available addressing this specific issue, leaving gender impact on the outcome of complex minimally invasive aortic procedures seriously underrated.
According to the high male predominance in aortic aneurysm incidence, most of the available devices are primarily designed for male patients, not taking into account, for instance, the smaller size of female access arteries. 27
Our understanding of complex aortic endovascular reconstruction and factors influencing its outcomes currently relies mostly on single-center experiences or registries with relatively limited numbers when compared with the evidence in the infrarenal segment.28–30
Recently, however, more robust data have been published, in some cases also specifically focusing on sex-related differences after F/BEVAR. Edman et al 31 compared 288 women with 598 men treated in 8 American facilities for TAAA. Despite lower technical success rates, women demonstrated 30-day outcomes and 1-year survival rates comparable to those of men.
Rieß et al investigated a large German health insurance claims database and compared outcomes in men and women receiving fenestrated/branched endografts for aneurysms correction. Female patients resulted in having significantly higher rates of in-hospital (relative risk [RR]: 2.86, 95% confidence interval [CI]: 1.61–5.08), 30-day (RR: 2.27, 95% CI: 1.37–3.76), and 90-day (RR: 1.97, 95% CI: 1.25–3.10) mortality. 27
The initial study cohort for the present research belongs to a national Italian multicentric registry specifically designed to obtain a broad experience in complex endovascular aortic repair using a single brand endograft.
With the goal of reducing concurrent variables and having a homogeneous population, starting from a total registry cohort of 596 treated patients, we narrowed the study sample down to 176, using propensity matching with a logistic regression model adjusted for demographic data and comorbidities.
As women frequently receive a delayed aortic aneurysm treatment1,32,33 and are more likely to present with undertreated and underdiagnosed cardiovascular comorbidities, the propensity matching applied in this study was built considering age and all available risk factors to isolate only sex-related differences in outcomes.
The most important research findings probably come with the demonstration that in the selected population, women presented a more hostile vascular anatomy and a more extensive aneurysmal disease.
In fact, women turned out having significantly higher incidence of TAAA (Crawford type I, II, and III), smaller visceral vessels, and more complex iliofemoral accesses.
These results confirm previous assessment from Grandi et al, 34 who, in an anatomical feasibility study published in 2021, identified a higher proportion of type II TAAA (p=0.012) in women among a population of 268 patients treated for TAAA in a single center during the 2007–2019 period.
Same evidence derives from the study by Edman et al 31 in the aforementioned paper, confirming a significantly higher ratio of women having a type I–III TAAA extent (p<0.0001).
Moreover, both studies pointed out the existing significant sex differences in vascular iliofemoral accesses.31–34
The aforementioned findings could explain the dissimilar perioperative outcomes between men and women after F/BEVAR reported in the present study.
Hostile iliac anatomy role during complex aortic repair was previously investigated by Gallitto et al. 20 Over a 5-year experience, the authors demonstrated how procedures were significantly more demanding in patients with complex iliofemoral accesses, with more frequent difficult target vessel cannulations, endograft twisting, and intraoperative adjunctive maneuvers needed in the hostile iliac access group. 20
Coselli et al 35 proved in their milestone 2016 paper, collecting 3 decades of surgical thoracoabdominal repair experience, how proximal aneurysm extent worsens procedure results. During the 1986–2014 period, the authors treated 3309 thoracoabdominal aneurysms with open surgery. Patients treated for type II TAAA developed a much higher adverse event rate than those who received type IV TAAA treatment (19.0% vs 10.2%, p>0.0001).
Similar findings were outlined about the endovascular approach, with the number of fenestrations being predictive of perioperative mortality and severe morbidity. 36
The results of the WINDOWS study, a French multicenter, prospective single-arm trial for F/BEVAR in complex aortic aneurysms, underline once again the impact of pathology extension on perioperative mortality and major complications. Patients treated via endovascular approach for juxtarenal or pararenal aneurysms (group 1) performed significantly better than patients with a more proximally extended dilatation (group 2). In a univariate analysis, in-hospital/30-day mortality and major complications risks were 3.25 (95% CI: 1.51–7.00) and 2.02 (95% CI: 1.21–3.37) times higher, respectively, for patients in group 2. These results were further confirmed as positive independent predictors of outcomes at the multivariate analysis. 37
Finally, even if strong evidence about the importance of the size of arteries in operative success is lacking, it is common experience that a large TVV makes cannulation and overstenting smoother and easier than smaller ones.
Thus, each of the aforementioned features found more frequently in female patients could affect perioperative results during endovascular complex aortic repair.
These findings reflect the present study outcomes, as both technical and 30-day clinical success rates ended up being significantly lower in female patients.
Study Limitations
The present analysis is the result of a selection performed over a broad multicenter national experience collected over the years in 4 academic centers. The first limitation to be disclosed is the retrospective nature of the registry. Although enrolled patients could be deemed as a real-world national sample, a selection bias should be considered as individual institutional different criteria exist between participating centers.
As already discussed, women are underrepresented in most of the studies investigating aneurysmal aortic pathology, including the present one. Aiming to assess sex-related differences, the authors opted for propensity matching using a logistic regression model adjusted for demographic data and comorbidities, trying to reduce the bias related to different sex-related distributions.
Procedural results in terms of success and complications may have been affected by the different distribution of extensive thoracoabdominal aneurysms in women and men. This reflects, however, the different real-world pathology incidence, and the study findings are likely to express an existing sex disparity. Moreover, as Crawford extension does not necessarily match with treatment broadening or with its difficulty, the authors divided procedural complexity into 2 groups, comparing patients receiving revascularization of at least 3 TVVs with those whose reconstruction included 2 or just 1 visceral vessel. No differences in terms of this parameter were found in the selected study cohort.
Conclusions
In the selected study population, women presented a more hostile vascular anatomy as well as a more extensive aneurysmal disease. Indeed, they showed a significantly higher incidence of thoracoabdominal aneurysms, smaller visceral vessels, and more complex iliofemoral accesses. The technical success rate was significantly lower in women, most probably due to anatomical complexity.
Despite the objective limits of the present analysis, our data suggest how a more careful and critical assessment should be posed in case of female patient preoperative evaluation and selection with appropriate surgical risk stratification when planning an endovascular complex aortic procedure.
Further studies specifically aiming to reveal sex-related differences in extensive aortic pathology are needed to confirm these preliminary data.
Supplemental Material
sj-jpg-1-jet-10.1177_15266028221137498 – Supplemental material for Sex Influence on Fenestrated and Branched Endovascular Aortic Aneurysm Repair: Outcomes From a National Multicenter Registry
Supplemental material, sj-jpg-1-jet-10.1177_15266028221137498 for Sex Influence on Fenestrated and Branched Endovascular Aortic Aneurysm Repair: Outcomes From a National Multicenter Registry by Giacomo Isernia, Gioele Simonte, Enrico Gallitto, Luca Bertoglio, Aaron Fargion, Germano Melissano, Roberto Chiesa, Massimo Lenti, Carlo Pratesi, Gianluca Faggioli and Mauro Gargiulo in Journal of Endovascular Therapy
Footnotes
Authors’ Note
The abstract was accepted for fast-track presentation at the ESVS 2021 annual meeting held in Rotterdam.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EG, LB, GM, MG and GF are proctors and consultants for Cook medical.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.