
Abstract
Objective:
Poor ergonomic posture during interventional procedures might lead to increased physical discomfort and work-related musculoskeletal disorders. Adjunctive equipment such as lead aprons (LAs) has been shown to increase ergonomic posture risk (EPR). The objective of this study was to evaluate the effectiveness of StemRad MD (StemRad Ltd., Tel Aviv, Israel), a weightless exoskeleton-based radiation protective ensemble, in reducing EPR on the operator using wearable inertial measurement unit (IMU) sensors.
Methods:
A prospective, observational study was conducted at an academic hospital. Inertial measurement unit sensors were affixed to the upper back of 9 interventionalists to assess ergonomic risk posture during endovascular procedures while wearing a traditional LA or the StemRad MD radiation protection system. Total fluoroscopy time, procedure type, and ergonomic risk postures were recorded and analyzed.
Results:
Twenty-one cases were performed with StemRad MD and 30 with LAs. Mean procedure time for the StemRad MD procedures was 48.4±23.3 minutes (range: 24–106 min), and for LA procedures, it was 34.66±25.83 minutes (range: 6–100 min) (p=.060). The operators assumed low-risk ergonomic positions in 96.1% of StemRad MD cases and in 62.9% of LA cases (p=.001), and high-risk ergonomic positions in 0% and 6.2%, respectively (p=.80). Mean EPR score for StemRad MD was 1.16, and for the LA, it was 1.49 (p=.001).
Conclusions:
StemRad MD significantly reduces the EPR to the torso compared with a LA-based radiation protection system.
Clinical Impact
Poor ergonomic posture during interventional procedures might leas to work-related musculoskeletal disorders for healthcare workers. StemRad MD, a weightless, exoskeleton-based radiation protection system was shown to significantly reduce ergonomic posture risk to the torso compared to conventional lead aprons. This might lead to reduced physical discomfort for procedure-based specialists.
Keywords
Introduction
Work-related musculoskeletal disorders (WMSDs), such as chronic neck and back pain, among procedure-based specialists have been gaining increasing attention in recent years.1–5 Even though physicians tend to minimize the impact of WMSDs, several studies have shown that up to 85% of surgeons have musculoskeletal symptoms.6,7 Physical discomfort might lead to increased psychological stress, loss of focus, and overall burnout which might impact patient outcomes and increase medical errors. 1
The presence of personal adjunctive equipment, such as surgical loupes or LAs, has been associated with increased physical discomfort and poor ergonomic postures.1,8 Lead aprons can weigh between 5 and 8 kg and increase ergonomic strain on the operator’s neck, shoulders, and lower back, especially for longer procedures. For example, endovascular procedures require delicate manipulation of guidewires and catheters to navigate within vessels. This requires the operator to maintain a fixed posture for long periods, which aggravates physical stress on axial, weight-bearing muscles. In addition to physical symptoms, physicians wearing LAs have also reported increased levels of distraction during procedures, 3 as well as decreased range of motion.
Physical discomfort and WMSDs stem from poor intraprocedural ergonomics. The aim of this study was to evaluate the effectiveness of a novel, exoskeleton-based, radiation protection system named StemRad MD (StemRad Ltd., Tel Aviv, Israel), in reducing EPR on the operator’s torso as compared with conventional LAs.
Materials and Methods
Setting and Participants
This was a single-center, prospective, observational study conducted at a large academic hospital. A total of 9 subjects (8 males and 1 female, n=9) participated in the study, including interventional radiologists (n=8) and a vascular surgeon (n=1). Age, years of experience, and relevant medical history data were collected. Recruitment was by word of mouth, and participants were informed that they could opt out of the study at any moment. The study was conducted according to the principles defined by the Declaration of Helsinki, and the need for written informed consent was waived by the Institutional Review Board. However, oral informed consent was obtained before measurement sessions.
StemRad MD Radiation Protection System
The StemRad MD radiation protection device consists of 4 parts: a customized protective apron made up of bismuth-antimony bilayer (Kemmetech, Kent, UK, 0.5 mm lead equivalent), a visor (face shield made of transparent material) made of transparent lead-acrylic attenuation material (Kuraray Co. Ltd., Nigata, Japan, 0.34 mm lead equivalent), a thyroid collar (Kemmetech, Kent, UK, 0.5 mm lead equivalent), and a proprietary exoskeletal system to channel the weight of all components away from the user and onto the floor (Figure 1). The LA and thyroid protector used for the study were 0.5 mm lead equivalent thickness (Attenutech, Lutz, FL, USA).

StemRad MD Exoskeleton Radiation Protection System is composed of a lead-free material apron (A), a proprietary exoskeleton (B), a dedicated hanger (C), and a visor (D). The exoskeleton channels all the weight to the floor while enabling full range of movement. The hanger allows easy access (E–G) and exit of the system. The StemRad MD is worn from the bottom up, and once the operator has donned the system, they can put on sterile gowns and gloves.
The exoskeletal system is based on an external, weight-bearing rod with articulating joints at hip and knee level. The components of the radiation attenuation product are suspended by the exoskeleton so that it is not in contact with the operator’s shoulders or upper back. In this way, the radiation protection system’s weight is removed from the operator whilst allowing full range of motion, both for standing and sitting positions. The exoskeletal system is fitted for each operator based on hip, knee, and height measurements. The exoskeletal system is not fixed, and the operator is able to move independently around the operating table and room. During endovascular, interventional, and hybrid procedures, the system allows for complete range of motion in all directions owing to its weightless properties.
Protocol Overview
For the purposes of quantifying EPR, previously validated 9 inertial measurement unit (IMU) sensors were used (Opal sensor, RIT Inc, Portland, OR, USA). The IMU sensor is wireless and measures 5.49 cm × 4.0 cm × 1.43 cm. Before the surgical procedure, member(s) of the StemRad MD team affixed the IMU sensor behind the physician’s upper torso, at the level of the T1 vertebra. The IMU sensor was placed in a manner that the x-axis of its orientation was aligned with the torso of the physician. Before each procedure, a calibration was done with each participant to measure their natural posture. During the calibration procedure, the physicians were standing upright with both arms outstretched and pointing downward. If the calibration procedure was unsatisfactory, the data were eliminated from the study. The objective was to compute the rotation variation in the torso during the procedure (Figure 2). During the procedure, data were stored in the IMU and were later extracted by the study team. In addition to IMU measurements, the study team collected data regarding the procedure including procedure type, use of ancillary shielding, time of procedure, and radiation dose.
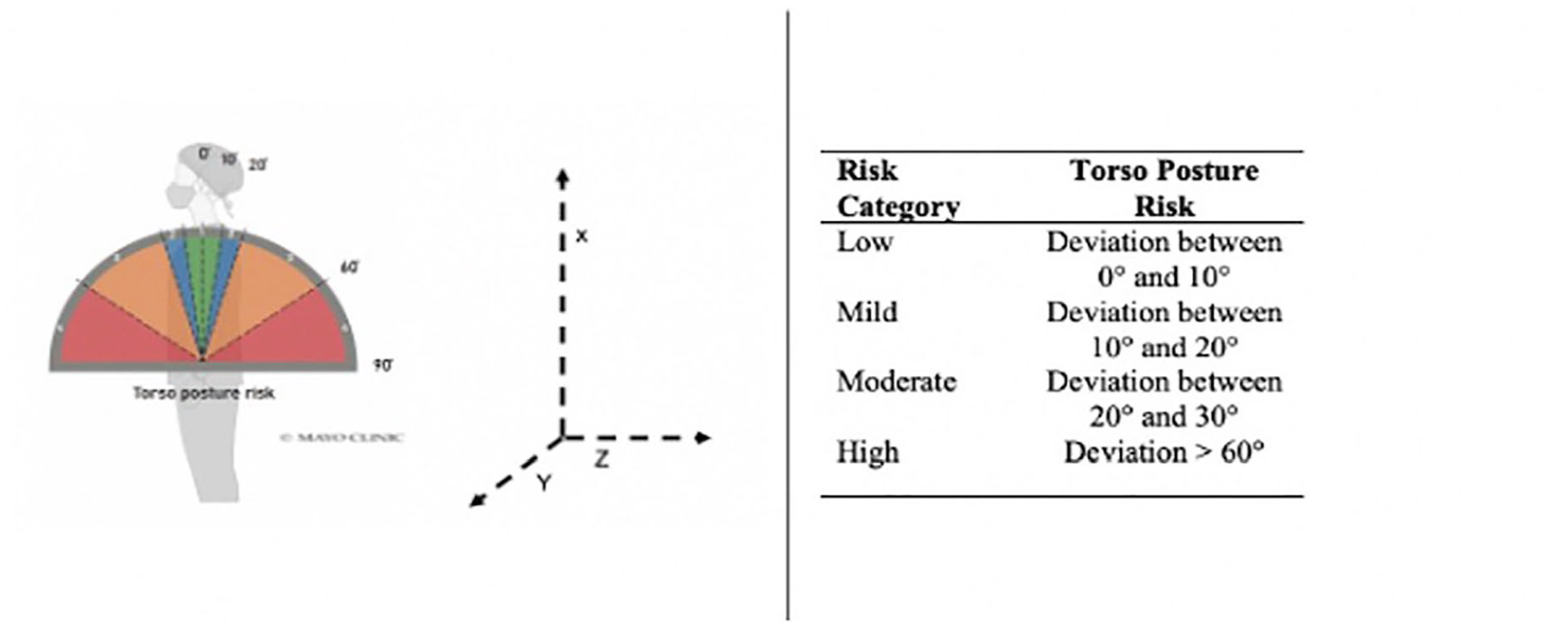
Various posture angles and corresponding EPR risks: low (green), mild (blue), moderate (orange), and high (red). Reproduced with permission from Elsevier.
In addition to procedures with the StemRad MD, the same protocol was followed for procedures with traditional LA, to compare the ergonomic advantages of the 2. Measurements were taken for 51 consecutive cases. The use of StemRad MD or traditional LA was randomly assigned to each procedure.
EPR Calculation
During the procedure, data were stored in the IMU and were later extracted by the study team. For each measurement, the natural posture angle of the physician was subtracted from the total posture angle to calculate the true deviation during the procedure. Body angles were categorized into 4 different risk levels: (1) low (green), (2) mild (blue), (3) moderate (orange), and (4) high (red), depending on torso deviation in the y-axis (Figure 2). Deviation between 0° and 10° is defined as low risk, between 10° and 20° is mild risk, between 20° and 60° as moderate risk, and above 60° as high-risk posture. The scale was derived from previous studies.10,11
The body part specific EPR score was calculated using the following equation:
where Ri is the risk level category associated with different postures (1, 2, 3, or 4), and Pi is the percentage of the time the physicians spent on that particular posture as recorded by the IMUs.
Statistical Analysis
Data collected during the procedure and downloaded from the IMU sensor were analyzed using SPSS Statistics version 27 (IBM, Armonk, NY, USA). Descriptive statistics were calculated. Normality of distributions was calculated with the Shapiro-Wilk test. Continuous variables are expressed as means with standard deviation and compared through 2 sample t-test or Mann-Whitney U test, as appropriate. Median and interquartile range (IQR) are also reported for non-normally distributed variables. Categorical variables are expressed as number and percentages and compared with chi-square test or Fisher’s exact test. Statistical significance was set at a 2-tailed p<.05. A post hoc statistical power analysis was performed.
Results
A total of 9 physicians (8 males and 1 female) were included in the study. In 21 cases, the StemRad MD system was used, while 30 cases were performed with the conventional LA. Of the 21 StemRad MD cases, 17 were performed by interventional radiologists and 4 by a vascular surgeon, while all LA cases were done by an interventional radiologist. Mean age of the physicians was 44.5±9.5 years (range: 32–61). Mean years of experience were 15±9.5 (range: 3–32). Four physicians (44.4%) reported occasional lower back symptoms. Mean procedure time for the StemRad MD procedures was 48.4±23.3 minutes (range: 24–106 min), and for LA procedures, it was 34.66±25.8 minutes (range: 6–100 min) (p=.060).
The procedures performed with the StemRad MD system included a branched thoracic endovascular aortic repair (TEVAR), endovascular aortic repair (EVAR), type 2 endoleak (EL) embolization, celiac artery (CA) stenting, nephro-ureteral stenting, gastrostomy tube placement, left upper extremity fistulogram and intervention (n=2), transjugular intrahepatic portosystemic shunt (TIPS) (n=3), transjugular liver biopsy and arterial embolization (n=3), and arterial embolization (n=5).
The procedures performed with a conventional LA included a nephrostomy tube placement, venous recanalization, ureteral stent exchange, TIPS, gastrostomy tube placement, transjugular liver biopsy, nephro-ureteral stent placement, liver chemoembolization, inferior vena cava (IVC) filter removal (n=2), Mediport removal, central venous catheter (CVC) placement (n=9), upper extremity fistulogram and intervention (n=3), and arterial embolization (n=5).
The type, number, and duration of procedures for StemRad MD and LA are illustrated in Figure 3.
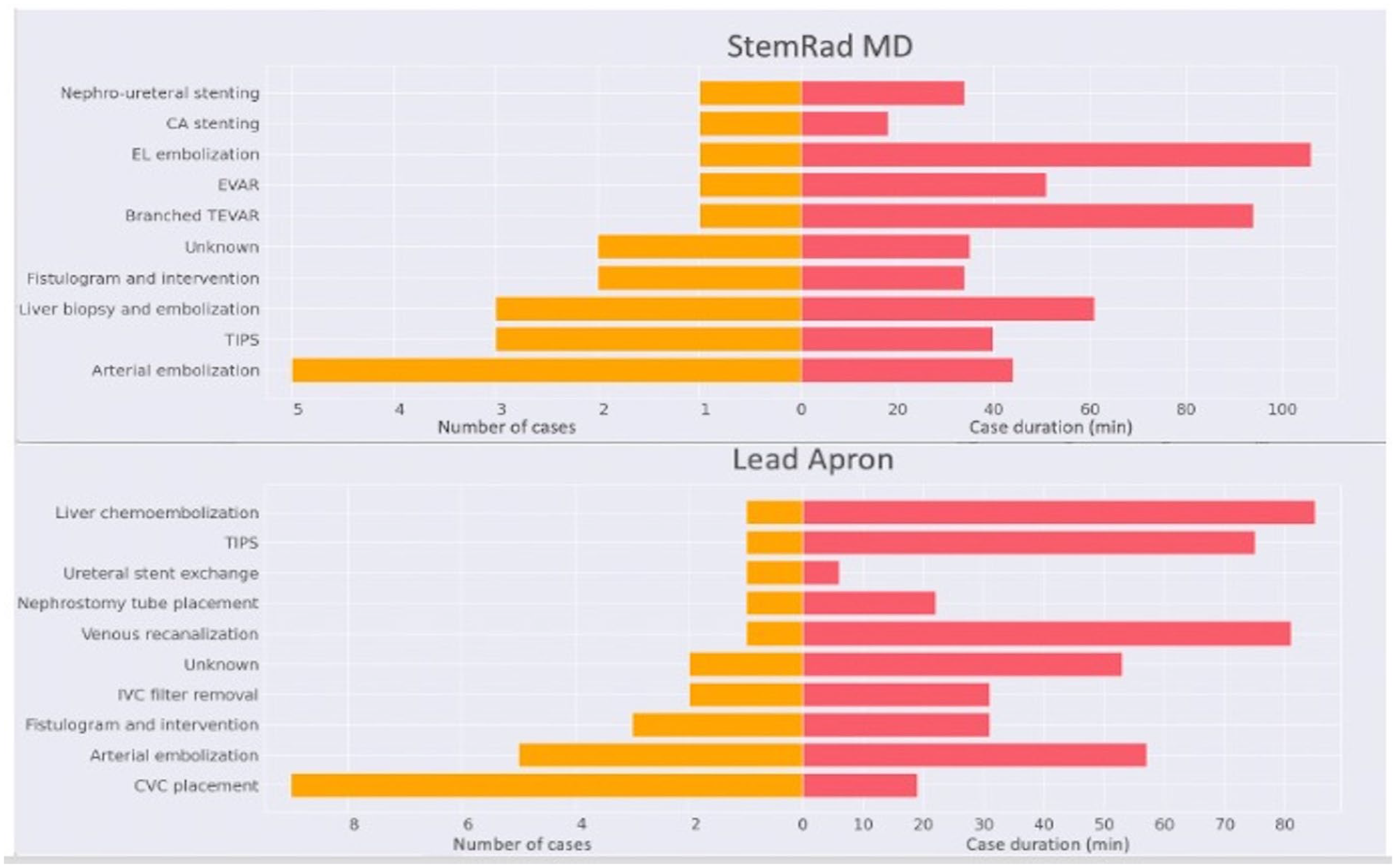
Bar chart illustrating the number (orange, on the left), type and duration (red, on the left) of the different types of procedures with StemRad MD and LA; CA, celiac artery; EL, endoleak; EVAR, endovascular aortic repair; TEVAR, thoracic endovascular aortic repair; TIPS, transjugular intrahepatic portosystemic shunt; IVC, inferior vena cava; CVC, central venous catheter.
Mean EPR values of the StemRad MD and LA are shown in Table 1. Inertial measurement unit data showed that the operators held low EPR positions for 87.4±21.3% (94.32%, IQR: 11.29) of the procedure duration with StemRad MD cases, and for 64.1±24.7% (66.44%, IQR: 33.22) of LA cases (p=.001), mild EPR for 8.3±11.6% (5.44%, IQR: 9.98) and 19.8±11.35% (p=.001), moderate EPR for 4.1±10.3% (.72%, IQR: 1.73) and 14.2±19.2% (6.92, IQR: 16.13) (p=.001), and high-risk EPR for 0.4±0.1% (0%, IQR: 0) and 1.9±9% (0%, IQR: 0) (p=.80), respectively. Mean torso EPR score for StemRad MD was 1.16±0.3% (1.06, IQR: .13) and 1.49±0.6% (1.38, IQR: .47) for the LA (p=.001) (Figure 4).
Ergonomic Posture Risk Category and Mean Risk Score for StemRad MD and Lead Apron.
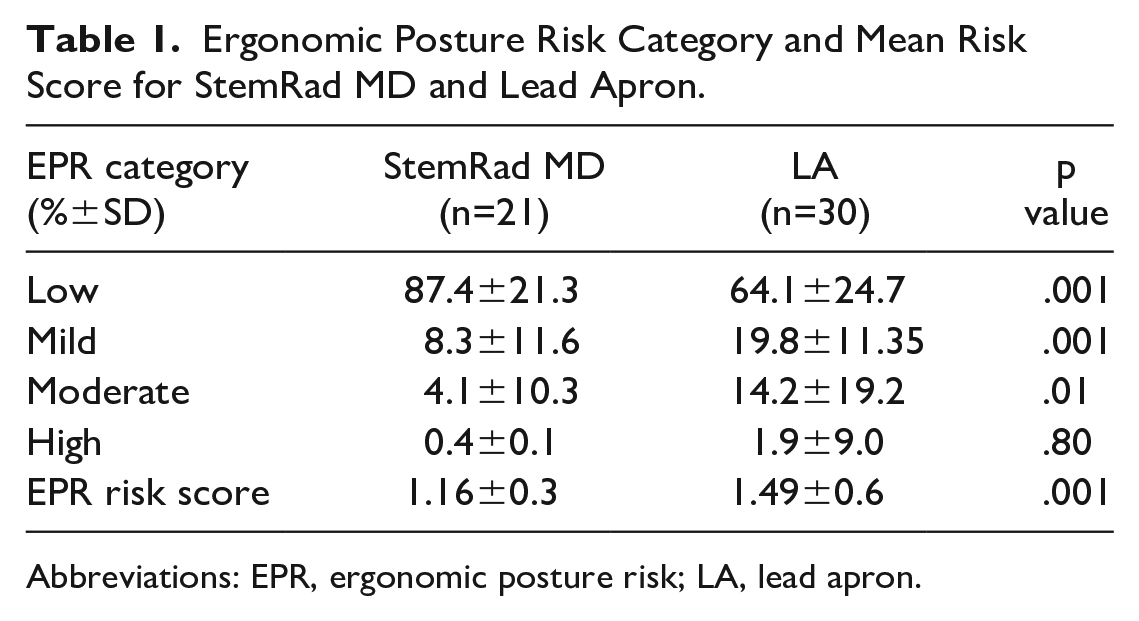
Abbreviations: EPR, ergonomic posture risk; LA, lead apron.
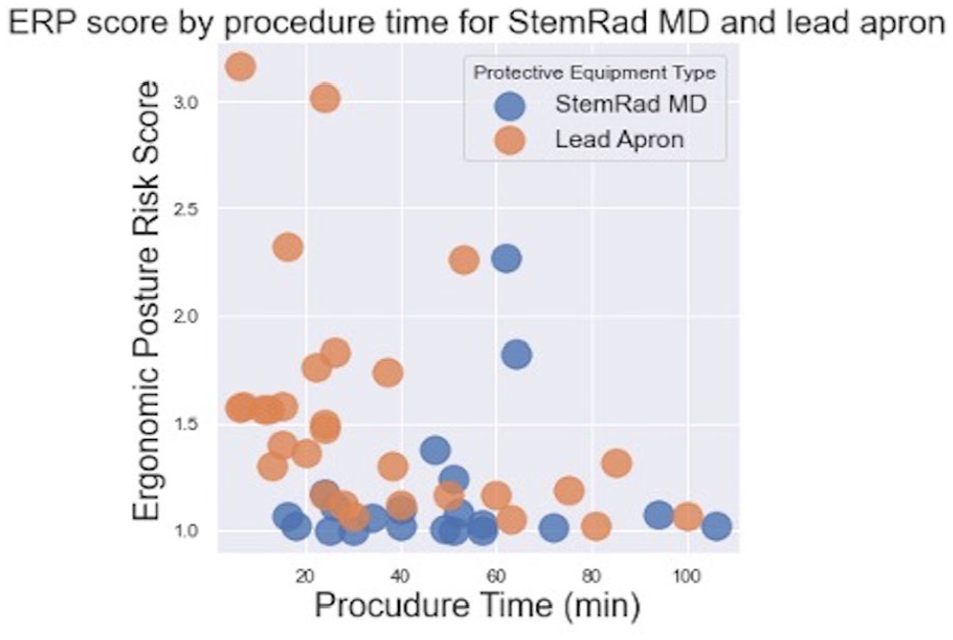
Scatter plot depicting the mean EPR score by procedure for StemRad MD (blue) and LA (orange). Overall, procedures with StemRad MD had lower EPR risks, both for shorter and longer procedures.
The post hoc statistical power was 72%.
Discussion
The main finding of this study suggests that StemRad MD reduces ergonomic strain on the operator as mean torso EPR was significantly less when using StemRad MD as compared with conventional LAs.
The use of traditional radiation protection equipment, such as LAs, has been linked with increased physical strain.12,13 Poor intraprocedural posture, longer procedures, and use of adjunctive equipment have all been linked to this discomfort.2,14,15 The most frequently reported symptoms include neck, shoulder, back, and knee pain.4,16 Davila et al 1 conducted an electronic survey on 263 members of the Society for Clinical Vascular Surgery. The authors reported that lead was worn by 91.4% of the physicians at least once per week and by 48.4% at least once per day. Lead-lined glasses or head covers (scrub caps) were worn by 57.5% at least once per week and 35.3% at least once per day. Up to 92.3% of participants reported pain immediately after interventions, especially for interventions requiring radiation protection with lead attenuating protective equipment.
Objective measurement of physical discomfort presents several challenges. However, several studies have used IMU sensors as a way to quantify muscular activity and strain.3,14 Inertial measurement unit sensors work by detecting linear acceleration using accelerometers and rotational rate using gyroscopes. 17 Data collected from the IMU are translated into EPR. Endovascular procedures have been shown to have an EPR of 2.31 for the neck and 1.75 for the torso. 3 Deviation angles as measured by IMUs are 24.3° and 19.1°for the neck and torso, respectively, with angles above 20° considered highly demanding. 2 Neck muscular strain with interventional procedures is attributed to the position of fluoroscopic monitors. 18 Torso strain can be attributed to the weight of LA, as weight-bearing muscle groups are mostly affected intraoperatively. Torso strain is, therefore, the most relevant parameter when examining the ergonomics of lead radiation protection equipment.
Our study revealed a mean torso EPR score of 1.49 with traditional LA, compared with 1.16 when wearing the StemRad MD radiation protection system. Physicians spent 95.7% of procedure duration in the 2 lowest EPR categories with StemRad MD cases compared with 83.9% with LAs. Only 4.5% of the procedure duration was spent in the 2 highest EPR categories with the StemRad MD, compared with 16.1% with LAs. This increase in the ergonomic risk is quite significant for lead wearers in comparison with the StemRad MD. One of the reasons why the torso EPR risk is lower for the StemRad wearer is its structure which ensures that the physician’s torso remains in the low-risk position by default and is less likely to be in the region of high risk during the procedure.
Work-related musculoskeletal disorders are associated with high costs to employers such as absenteeism, lost productivity, and increased health care, disability, and worker’s compensation costs. 19 Even though surgeons under-report WMSD to their employers, WMSDs might lead to emotional and physical burnout. Grossi et al 20 reported that burnout was predictive of higher pain frequency and greater degree of disability secondary to pain. Ultimately, WMSDs, physical pain, and burnout could lead to increased costs for the hospital. Even though the price for the StemRad MD is higher than a traditional LA, these costs could partially offset economic losses considering the decreased ergonomic risk for physicians.
One limitation of this study was the fact that it was found to be slightly underpowered, but it ultimately succeeded in demonstrating a statistically significant difference in mean torso EPR. Even though the procedures were randomly assigned in the 2 groups, a single operator performed all the procedures with the StemRad MD due to concerns about previous lower back pathology in relation to the increased length of the procedures. Ergonomic posture risk was not directly compared between the 2 groups for the exact same procedure and procedure length. This might introduce some bias for our study. The overall procedure time lengths, however, were equilibrated between the 2 groups. Moreover, female surgeons were under-represented in this study. However, current literature has not been able to identify differences in WMSDs incidence among the 2 genders. 21 Inertial measurement unit sensors have been widely validated for ergonomic posture assessment, but this technology is susceptible to artifacts due to gravity accelerations and incorrect alignment between sensor and anatomical axes. Finally, time of day could have an implication on physician posture, as it tends to be worst later in the day but was not considered for this study.
In conclusion, the exoskeleton-based StemRad MD improves torso ergonomics for the operator in comparison with conventional aprons, which might lead to decreased musculoskeletal strain. Further studies are needed to investigate our finding in reducing the incidence of WMSDs with the StemRad MD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: B.Z. acts as chief medical officer for StemRad Inc., Tampa, Fl, USA. R.P.C. is employed by StemRad Inc., Tampa, FL, USA. All other authors have reported that they have no relationships relevant to the contents of this article to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.