
Abstract
Background:
A recent meta-analysis of randomized control trials demonstrated a significantly higher risk of major amputation in patients treated with drug-coated balloons (DCBs) compared with standard treatment, especially in high-dose paclitaxel-coated DCBs. Distal particulate embolization after DCB use was considered a potential cause of the higher incidence of major amputation. The current study aimed to histologically and biologically compare biologic drug effect and distal particulate embolization in 3 DCBs (a high-dose paclitaxel-coated DCB [IN.PACT Admiral] and 2 low-dose paclitaxel-coated DCBs [Ranger and Lutonix]).
Methods and Results:
The DCBs were inflated in the healthy descending aortas of 18 rabbits, followed by euthanasia 28 days after the procedure. The treated descending aorta and distal skeletal muscles were histopathologically evaluated, and paclitaxel concentrations were measured. The paclitaxel concentration of the treated lesion was highest for Ranger, followed by IN.PACT and Lutonix (Ranger vs IN.PACT vs Lutonix: 1089 [745–2170] pmol/mg vs 638 [160–2075] pmol/mg vs 25 [10–304] pmol/mg, respectively; p<0.0001). In the histopathological evaluation, the angle of severe medial smooth muscle cell loss was largest for Ranger followed by IN.PACT and Lutonix (12.8 [8.0–20.4] degree vs 1.4 [1.2–5.2] degree vs 0.8 [0.5–2.5] degree, respectively), with significant differences for Ranger vs IN.PACT (p=0.007) and Ranger vs Lutonix (p=0.002). However, paclitaxel concentrations of distal skeletal muscles were lowest for Lutonix, followed by Ranger and IN.PACT (12 [1–58] pmol/mg vs 15 [13–21] pmol/mg vs 42 [19–108] pmol/mg, respectively, p<0.0001). The numbers of arteries with downstream DCB effects were highest for IN.PACT, followed by Ranger and Lutonix (Ranger vs IN.PACT vs Lutonix, 3 [3–4] vs 4 [3–7] vs 2 [1–2], respectively), which was consistent with the measured tissue paclitaxel concentrations.
Conclusion:
These findings suggest that Ranger demonstrates the strongest paclitaxel effect, as well as the second-best effect regarding distal particulate embolization, making it a good treatment option for patients with peripheral artery disease among the 3 DCBs evaluated in the current study. Further clinical head-to-head comparisons with larger numbers of patients are needed to explore which DCB is the most effective and safe treatment option.Clinical Impact:
The findings of the current preclinical study suggests that Ranger demonstrates the strongest paclitaxel effect, as well as the second-best effect regarding distal particulate embolization making it a good treatment for patients with intermittent claudication and chronic limb-threatening ischemia.
Keywords
Introduction
The number of patients with peripheral artery disease in the lower extremities who undergo endovascular therapy has been increasing because of the lower risk of periprocedural complications with shorter hospital stays compared with surgery.1,2 The latest guidelines recommend drug devices for short de novo femoropopliteal lesions as class II treatment.3–5 Paclitaxel, one of the main drugs used in peripheral arteries, reduces restenosis by interrupting the cell cycle of smooth muscle cells via stabilization of microtubules, thereby arresting mitosis. 6 Drug-coated balloons (DCBs) would be a better treatment option for shorter, less complicated lesions compared with drug-eluting stents (DESs) as previous studies have shown comparable clinical outcomes with “leaving nothing behind” strategies that enable flexible future treatment options (e.g., bypass or additional stent implantation for restenosis lesion).7,8 However, a recent meta-analysis of 8 randomized control trials (RCTs) with 1420 patients (97% with chronic limb-threatening ischemia [CLTI]) has demonstrated a significantly higher risk of major amputation in CLTI patients treated with DCB compared with those treated with conventional balloon angioplasty (hazard ratio [HR] 1.66, confidence interval [CI] 1.14 to 2.42, p=0.008). 9 The meta-analysis also raised potential concerns for high-dose paclitaxel-coated DCBs, which are characterized by paclitaxel coating doses ≥3.5 µg/mm2, compared with low-dose paclitaxel-coated DCBs. Distal particulate embolization after DCB use was considered one of the potential causes of a higher incidence of major amputation.
Recently, several preclinical studies have examined biologic characteristics of Conformité Européene (CE)-marked DCBs, suggesting significant differences among DCBs.10–16 Not only the drug type and dose but also the excipients and coating integrity of the DCBs can be reasons for the observed differences (Supplementary Table 1). According to these studies, the degree of distal particulate embolization was significantly higher in high-dose paclitaxel-coated DCBs than in low-dose paclitaxel-coated DCBs.10–12 However, the results of the paclitaxel effects, which were evaluated histologically10,11 or biologically, 12 were inconsistent. Kolodgie et al histologically investigated paclitaxel effects and evaluated medial smooth muscle cell (SMC) loss scores in a swine femoral artery model. 10 As a result, the paclitaxel-induced effects 28 days after DCB use were higher in the high-dose paclitaxel-coated DCB (IN.PACT Admiral, paclitaxel dose 3.5 µg/mm2; Medtronic, Galway, Ireland) than in the low-dose paclitaxel-coated DCB (Lutonix, 2.0 µg/mm2; Bard, New Providence, New Jersey, USA). 10 By contrast, Torii et al have demonstrated an opposite effect using the same swine model, showing numerically higher paclitaxel effects for low-dose paclitaxel-coated DCBs (Ranger, 2.0 µg/mm2; Boston Scientific, Marlborough, MA, USA; Stellarex, 2.0 µg/mm2; Phillips, Amsterdam, Netherlands) than for a high-dose paclitaxel-coated DCB (IN.PACT Admiral). 11 Another study by Boitet et al using a rabbit descending artery model found the highest paclitaxel concentration in the treated aorta for Ranger, followed by IN.PACT, Stellarex, the other CE-marked high-dose paclitaxel-coated DCB (Passeo-18 Lux, 3.0 µg/mm2; Biotronik, Berlin, Germany), and Lutonix. 12 Previous preclinical studies suggest that the most important aspect of paclitaxel effects on DCB is not the dose of paclitaxel on the balloon, but the formulation of paclitaxel and excipient/coating on DCB; however, no studies have proven these hypotheses both histologically and biologically. Therefore, the current study aimed to investigate paclitaxel effects and distal particulate embolization in three DCBs (one high-dose paclitaxel-coated DCB [IN.PACT Admiral] and two low-dose paclitaxel-coated DCBs [Ranger and Lutonix]) histologically and biologically.
Methods
Rabbit Model of Descending Aorta Balloon Angioplasty
The study protocol was reviewed and approved by the Education and Research Support Center in the Department of Animal Care at Tokai University (reference number: 211052).
Ranger, IN.PACT, and Lutonix, which represent all available DCBs for femoropopliteal lesions in Japan, were evaluated in the current preclinical study with reference to past preclinical studies.11,12 Eighteen Japanese white rabbits (Tokyo Laboratory Animals Science Co., Tokyo, Japan) were fed with a normal diet and received dual-antiplatelet therapy (aspirin and clopidogrel starting 2 days prior to the procedure, continued until the day of sacrifice). General anesthesia with isoflurane via inhalation mask was performed, and surgical access was obtained via the right carotid artery with a general sterile technique to insert a 5F vascular sheath. After nitroglycerin and heparin injection, angiography of the descending aorta and balloon injury was performed using a 4.0 × 20 mm compliant balloon catheter (Sterling balloon dilatation catheter, Boston Scientific, Marlborough, MA, USA) at a nominal pressure by slipping the inflated balloon from the distal descending artery to induce endothelial denudation following neointimal proliferation. A 4.0 × 40 mm DCB was inflated at a target balloon-to-artery overstretch ratio of 1:1.1 to 1.2 (average inflated pressure: 7.5±0.8 atm, inflated size: 4.1±0.1 mm) following an aortic size measurement using a 5 Fr sheath (2.3 mm) as a control. All DCBs were inflated for 180 s in the descending aorta as recommended by the companies providing the IN.PACT and Ranger DCBs. The recommended inflation time for the Lutonix DCB is 30 s; however, Lutonix DCBs were also inflated for 180 s for a fair comparison of the drug effects. Angiography was performed after DCB inflation to document patency. A total of 6 IN.PACT Admiral DCBs, 6 Ranger DCBs, and 6 Lutonix DCBs were used in this study (Figure 1). The animals recovered in the recovery unit after the procedure. For a month, the animals were carefully examined at least once a day by laboratory technicians. All animals received appropriate care in compliance with Animal Welfare Act and Public Health Services policies.
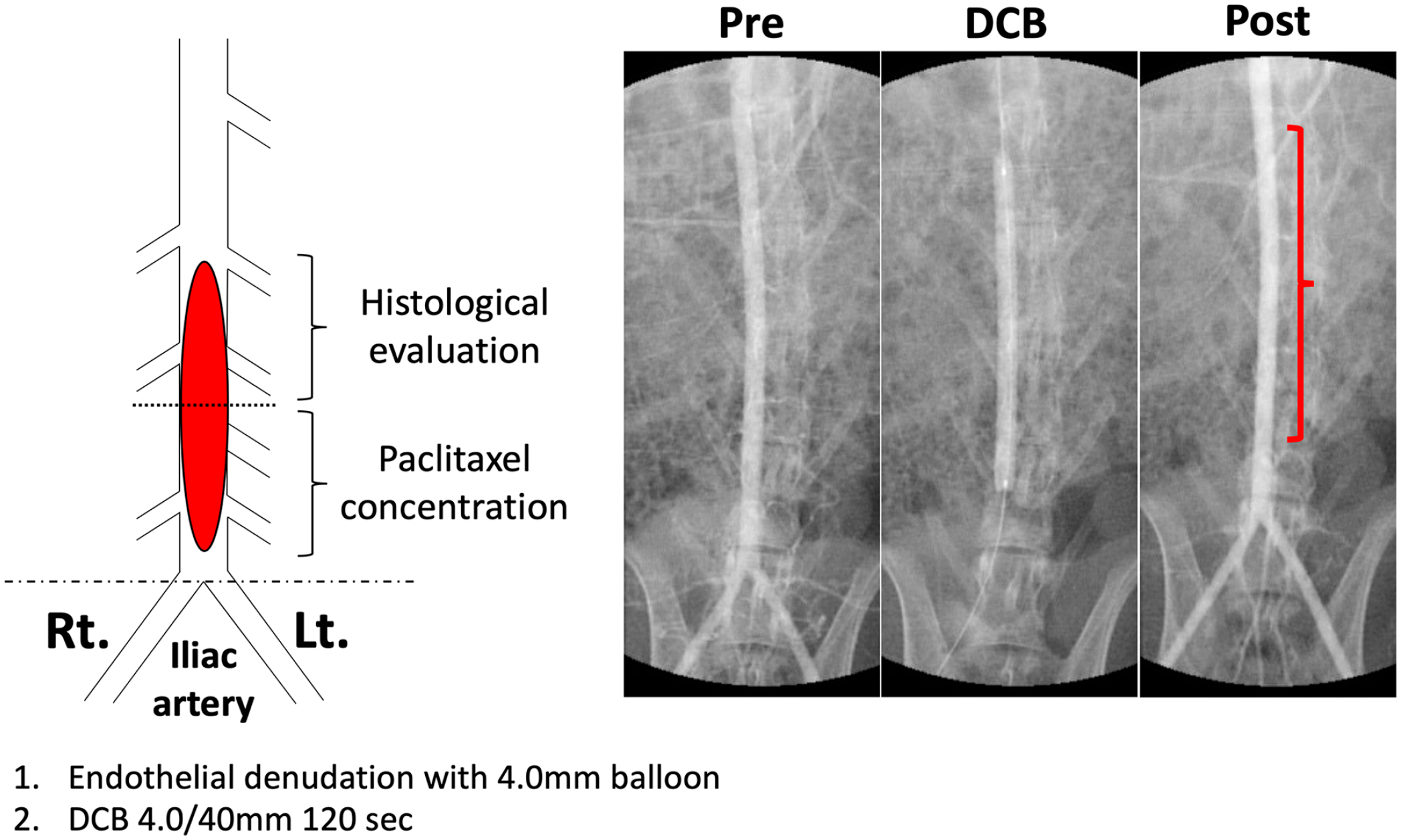
Study protocol schematic diagram (left) and series of angiograms in a rabbit (right). The treated descending aorta was 28 days following DCB use separated into 2 parts: the proximal part for histopathological evaluations and the distal part for measurements of paclitaxel concentrations. Rt., right; Lt., left; DCB, drug-coated balloon.
Collection of Rabbit Descending Aorta and Distal Skeletal Muscles
Twenty-eight days following the procedure, rabbits were again anesthetized with isoflurane via an inhalation mask. A 5F sheath was positioned in the left carotid artery and jugular vein. After nitroglycerin and heparin injection, angiography of the treated descending aorta was performed to confirm patency. The treated descending aorta was flushed with 1 L of lactated Ringer solution. To detect the precise position of the DCB-treated descending aorta, angiographic images of the previous procedure were carefully reviewed to determine the exact location of the treated lesion by using anatomic landmarks such as spinal vertebrae and the aortoiliac bifurcation. The treated lesion was divided into 2 parts, a proximal part for the histopathological analysis and a distal part for the paclitaxel analysis (Figure 1). After ligation of the center of the treated descending aorta detected with angiography, the distal part was removed and frozen at −80°C. The proximal part of the treated descending aorta was removed following fixation with 10% formalin perfusion and divided into proximal, middle, and distal segments. Each segment was subsequently subdivided into 4 to 6 subsegments, which were embedded in paraffin. Histological sections of 4 to 6 µm thickness were cut on a rotary microtome, mounted on charged slides, and stained with hematoxylin and eosin, as well as Movat Pentachrome. Three of the most affected histological sections from each treated descending aorta were used for histopathological analyses.
Skeletal muscle samples distal of the treated aorta were taken from three skeletal muscles below the knee region from both legs, ie, tibialis anterior, peroneal, and soleus muscles as previously performed. 12 Each skeletal muscle was divided into 2 parts for histological evaluation and measurement of paclitaxel concentration. Muscles for histological evaluation were fixed with 10% formalin and embedded in paraffin, followed by staining with hematoxylin and eosin and Movat Pentachrome stains. The other part of each muscle was kept frozen at −80°C for the bioanalysis of paclitaxel concentrations.
Histology and Histomorphometry
The histomorphometric analysis of the treated descending aorta was performed as previously described.10,11,17–20 In brief, the morphometric analysis was performed with computer-assisted software (Zen2, Zeiss, Oberkochen, Germany), and the external elastic lamina, internal elastic lamina, and lumen areas were measured. Percent area stenosis was calculated using the following formula: (1 − [lumen area/internal elastic lamina area]) × 100. The histological sections were examined for inflammation, fibrin deposition, calcification, hemorrhage, and medial injury. Biologic drug effects were evaluated using the medial SMC loss score and medial proteoglycan/collagen score. The extent of medial SMC loss was semi-quantified using a scoring system of 0–4, with 0 indicating none identified, 1 indicating an SMC loss of <25% of the medial circumference, 2 indicating 25–50% loss, 3 indicating 51–75% loss, and 4 indicating >75% loss. In addition to the semi-quantitative medial SMC score, the angle of circumferential severe SMC loss, which was defined as the circumferential angle of medial SMC loss of >50% of medial depth, was measured by the Zen2 software to detect detailed differences in paclitaxel effects in each DCB. The medial proteoglycan/collagen score was also semi-quantified using a scoring system of 0 to 4. All histomorphometric analyses were performed with the observer blinded to the treatment group. Further details of the histologic score systems are described in Supplementary Table 2.
Bioanalysis of Paclitaxel Concentrations in Treated Lesions and Downstream Skeletal Muscles
Bioanalyses of paclitaxel concentrations in treated lesions and downstream skeletal muscles were performed as previously reported.21,22 The treated aorta and downstream skeletal muscles were weighed and subsequently homogenized in 1 mL acetonitrile using a Shake Master Neo (Bio Medical Science, Tokyo, Japan). Homogenized samples were centrifuged to collect supernatants. The supernatants were then dried using a SpeedVac concentrator (Thermo Fischer Scientific, Waltham, MA, USA) and reconstituted in 100 µL of 75% methanol in ultrapure water. A 2 µL volume of the 10-fold diluted sample was injected into liquid chromatography-tandem mass spectrometry (LC-MS).
The quantitative analysis of paclitaxel concentrations was performed using an LCMS-8050 triple quadrupole mass spectrometer coupled to a UHPLC-Nexera system (Shimadzu, Kyoto, Japan). Samples were separated using a 2.0 × 150 mm, 1.9 µm Hypersil (Waltham, MA, United States of America) Gold C18 column (Thermo Fischer Scientific). Mobile phase A consisted of ultrapure water containing 0.1% acetic acid and 0.05% formic acid, and mobile phase B was 95% acetonitrile. Isocratic elution with 50% mobile phase B at a flow rate of 0.3 mL/min was employed. Mass spectrometric detection of paclitaxel was conducted in positive electrospray ionization mode. Other mass spectrometric parameters were as follows: flow rate of nebulizer gas, 3.0 L/min; flow rate of heating gas, 10.0 L/min; flow rate of drying gas, 10.0 L/min; interface temperature, 300°C; and heat block temperature, 400°C. MS1 and product ion spectrum, optimal selected reaction monitoring (SRM) conditions, a representative SRM chromatogram, and the calibration curve of paclitaxel are summarized in Supplementary Figure 1.
Statistical Analysis
Data are described as median with interquartile range (IQR). Normality of distributions was checked using graphic methods and the Shapiro–Wilk test. Comparison of variables with nonparametric distribution was performed by the Kruskal-Wallis test with Steel–Dwass post hoc analysis. A p<0.05 was considered statistically significant. JMP software (version 16.0, Cary, NC, USA) and GraphPad Prism (San Diego, CA, USA) were used for statistical analyses.
Results
Histomorphometric Analysis
All animals survived the scheduled 28 days without any vessel dissections, ectasia, or aneurysms noted on angiographic examination before sacrifice. Morphometric analysis of the treated descending aorta demonstrated that vessel dimensions such as internal/external elastic lamina, neointimal area, and percent stenosis were similar for the 3 DCBs (Table 1).
Morphometric Analysis of the Treated Arteries.
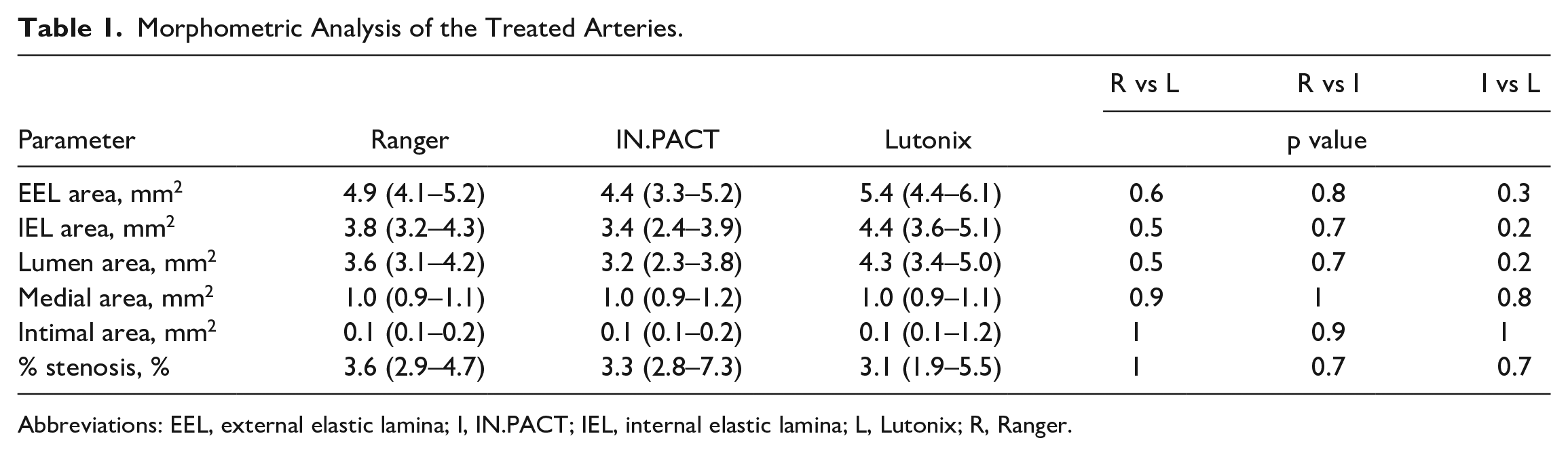
Abbreviations: EEL, external elastic lamina; I, IN.PACT; IEL, internal elastic lamina; L, Lutonix; R, Ranger.
Biologic Analysis of Paclitaxel Concentrations
In DCB-treated descending aortas, paclitaxel concentrations were the highest in Ranger, followed by IN.PACT and Lutonix (Ranger vs IN.PACT vs Lutonix, median value [IQR]: 1089 [745–2170] pmol/mg vs 638 [160–2075] pmol/mg vs 25 [10–304] pmol/mg, respectively; Figure 2A). The paclitaxel concentrations of the descending aorta were significantly lower in the Lutonix group compared with the Ranger (p=0.02) and IN.PACT (p=0.03) groups, whereas the difference between the Ranger and IN.PACT groups was not significant (p=0.5).
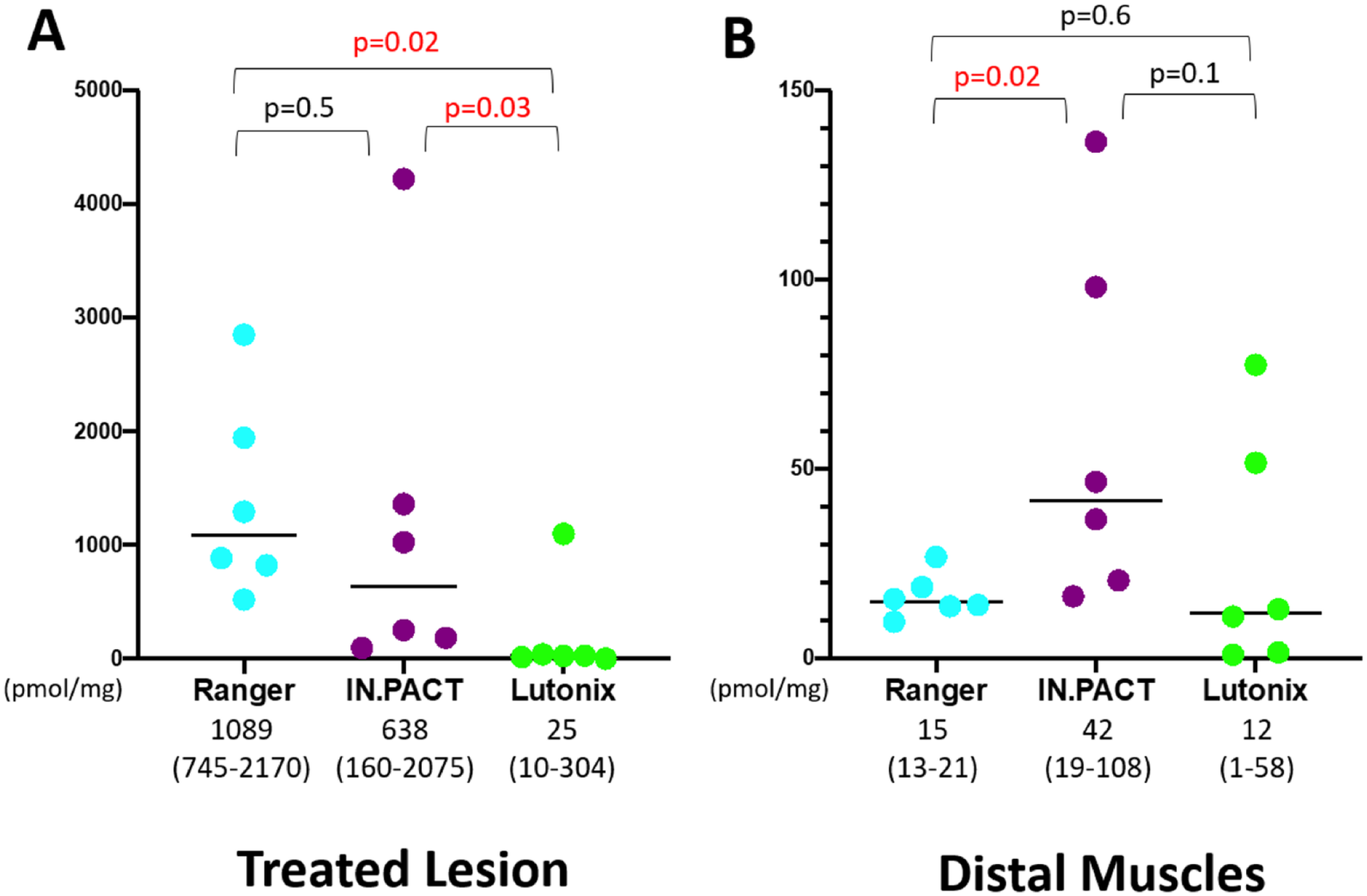
Paclitaxel concentrations of treated lesions and distal skeletal muscles 28 days after drug-coated balloon use. (A) In the treated lesion of the distal aorta, paclitaxel concentrations were the highest in the Ranger group, followed by the IN.PACT and Lutonix groups. (B) In skeletal muscles distal of the treated vessel, paclitaxel concentrations were the lowest in the Lutonix group, followed by the Ranger and IN.PACT groups.
In skeletal muscles distal of the treated vessel, paclitaxel concentrations were the lowest in the Lutonix group, followed by the Ranger and IN.PACT groups (Ranger vs IN.PACT vs Lutonix, median value [IQR], 15 [13–21] pmol/mg vs 42 [19–108] pmol/mg vs 12 [1–58] pmol/mg, respectively; Figure 2B). The paclitaxel concentrations of the distal skeletal muscles were significantly lower in the Ranger group compared with the IN.PACT group (p=0.02), whereas IN.PACT vs Lutonix (p=0.1) and Ranger vs Lutonix (p=0.6) groups were not significantly different.
Histopathological Evaluation of the Treated Descending Aorta
No significant vascular reactions were observed in the proximal part of the descending aorta. In treated lesions, the histopathological evaluation demonstrated that the score rating the depth of medial SMC loss was the highest in the IN.PACT group, followed by the Ranger and Lutonix groups (Ranger vs IN.PACT vs Lutonix, 3.2 [2.6–3.8] vs 3.5 [2.9–3.7] vs 2.5 [2.3–2.8], respectively; Figures 3 and 4, Table 2). The difference between the IN.PACT and Lutonix groups was significant (p=0.02). By contrast, the score regarding circumferential medial SMC loss was the highest in the Ranger group, followed by the IN.PACT and Lutonix groups (Ranger vs IN.PACT vs Lutonix, 2.2 [1.9–2.7] vs 1.8 [1.3–2.0] vs 1.7 [1.7–2.1], respectively; Figures 3 and 4, Table 2). Likewise, the angle of severe medial SMC loss was the largest in the Ranger group followed by the IN.PACT and Lutonix groups (Ranger vs IN.PACT vs Lutonix, 12.8 [8.0–20.4] degree vs 1.4 [1.2–5.2] degree vs 0.8 [0.5–2.5] degree, respectively; Figure 5, Table 2), with significant differences in the comparisons Ranger vs IN.PACT (p=0.007) and Ranger vs Lutonix (p=0.002).
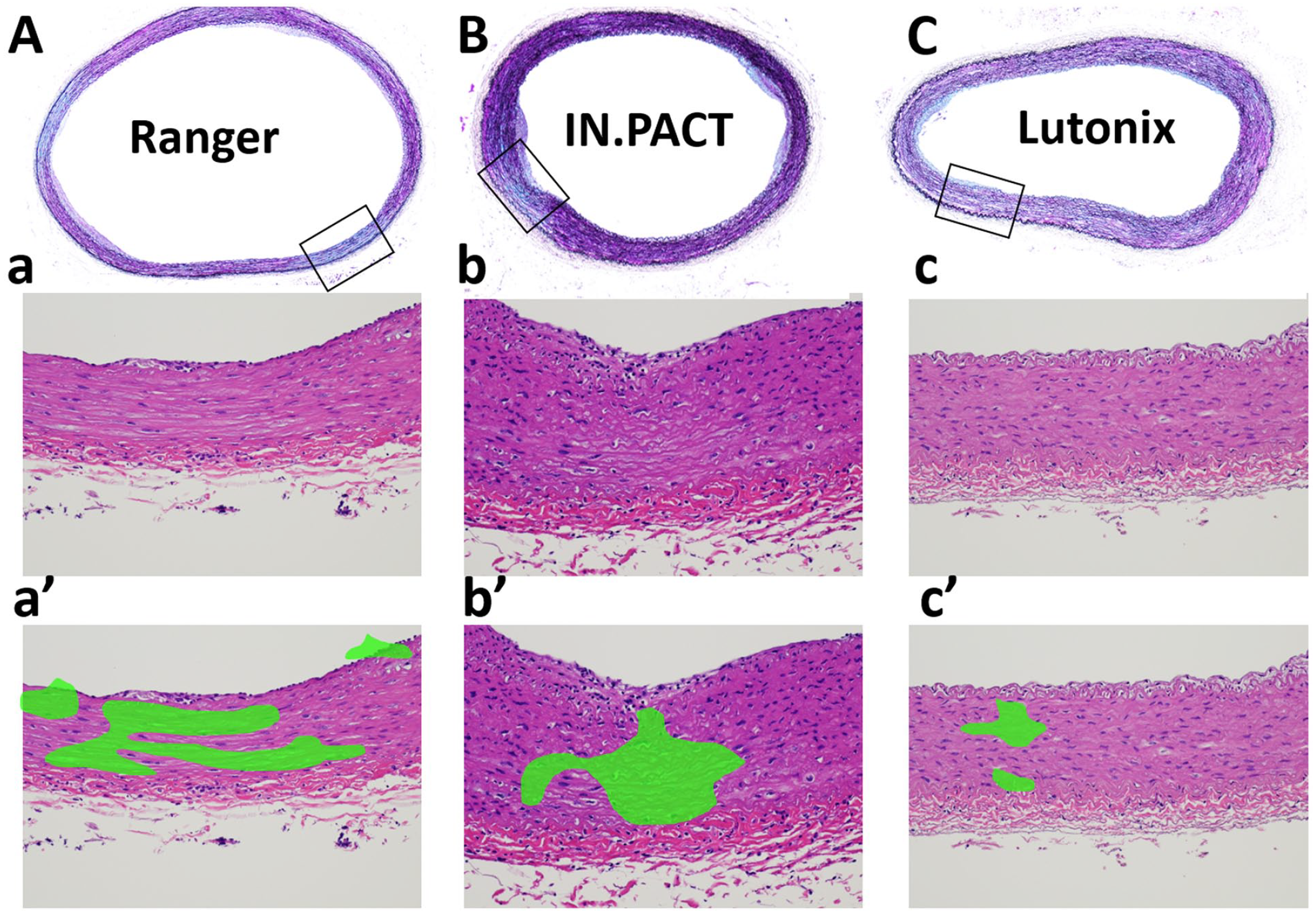
Representative pictures of descending aortas 28 days after drug-coated balloon use. Low-power (upper row, A–C, Movat pentachrome stain) and high-power (middle row, a–c, hematoxylin and eosin stain) images of descending aortas. Areas with smooth muscle cell loss are colored in green (lower row, a’–c’). Note the depth of smooth muscle cell loss is the highest in the IN.PACT column, whereas the largest circumferential loss of smooth muscle cells can be seen in the Ranger column.
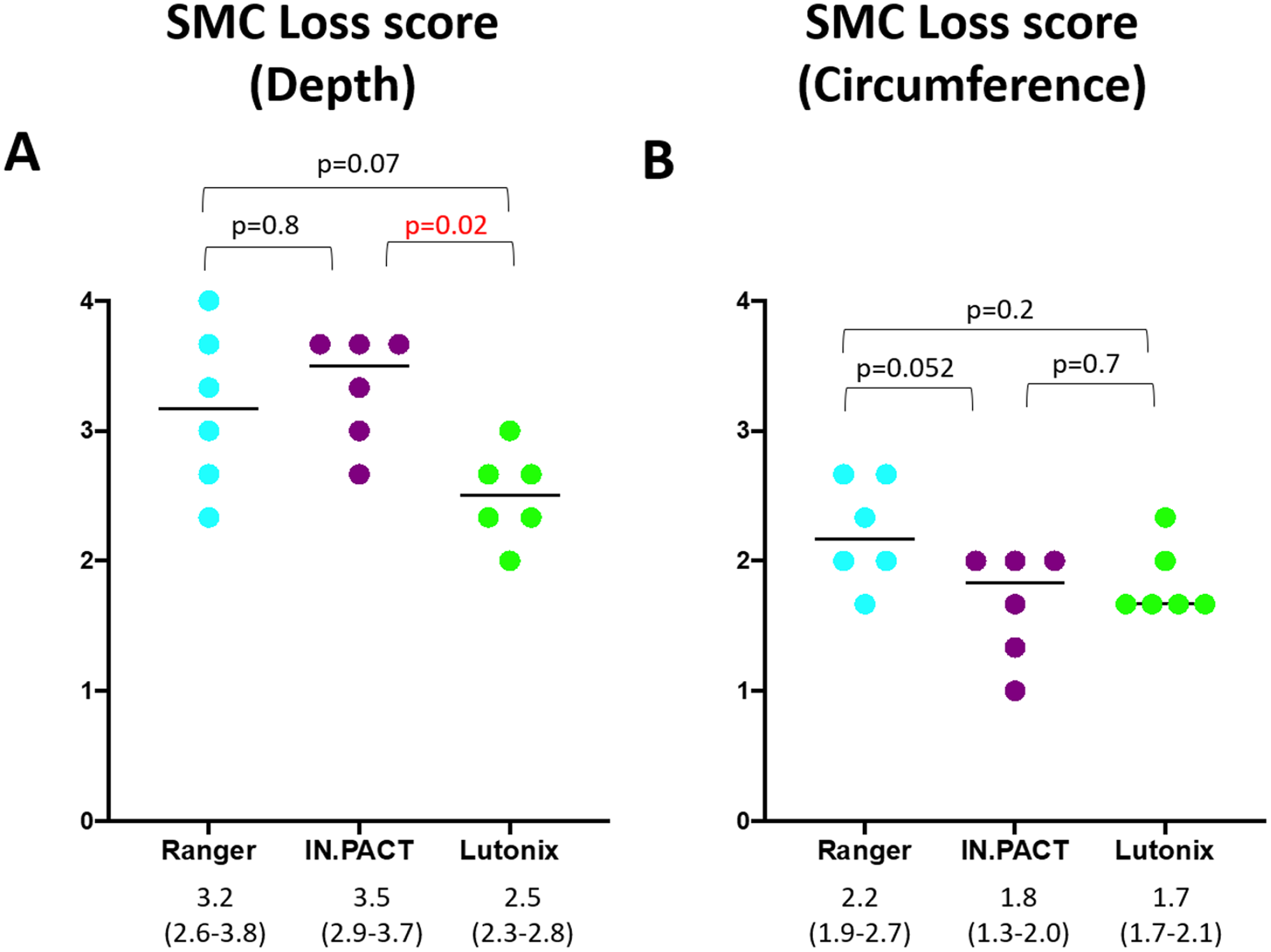
Histological scores of SMC loss (depth and circumference). (A) The score for the depth of medial SMC loss was the highest in the IN.PACT group, followed by the Ranger and Lutonix groups. (B) The score for the circumference of medial SMC loss was the highest in the Ranger group, followed by the IN.PACT and Lutonix groups. SMC, smooth muscle cell.
Pathological Analysis of the Treated Arteries and Distal Skeletal Muscles.
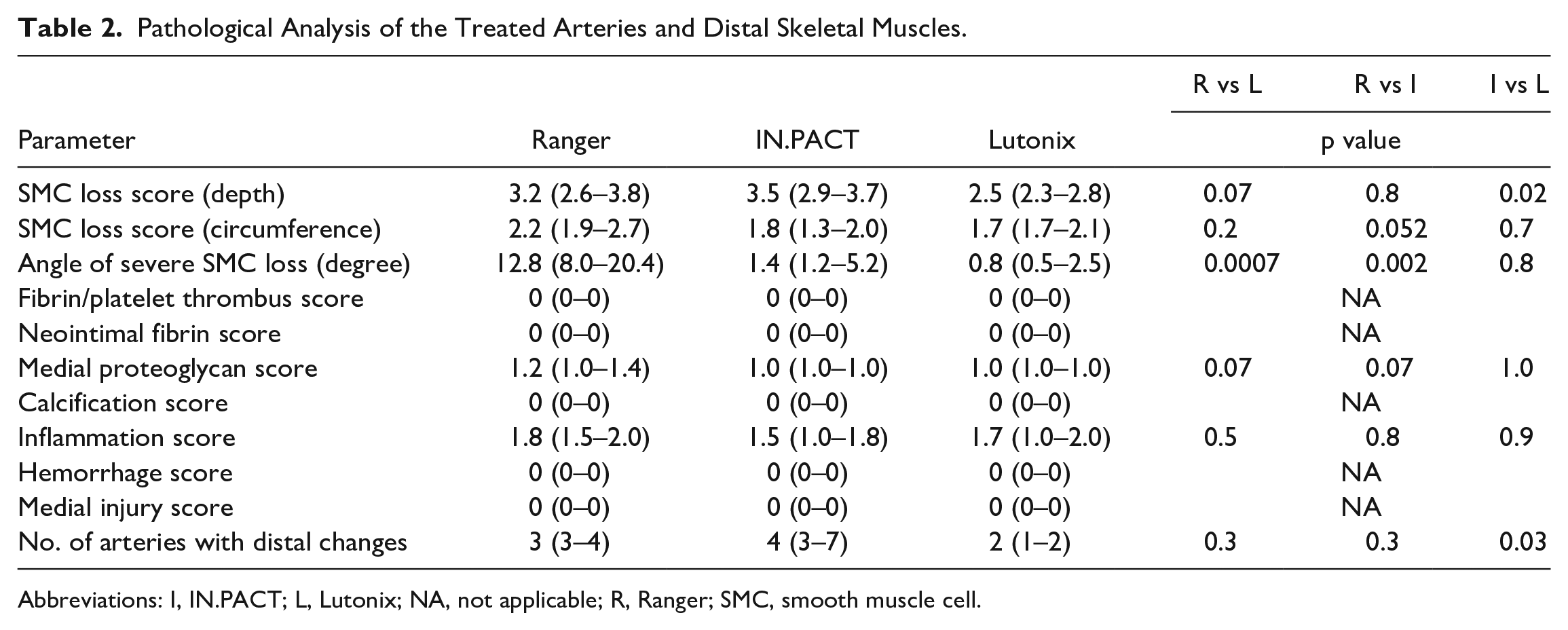
Abbreviations: I, IN.PACT; L, Lutonix; NA, not applicable; R, Ranger; SMC, smooth muscle cell.
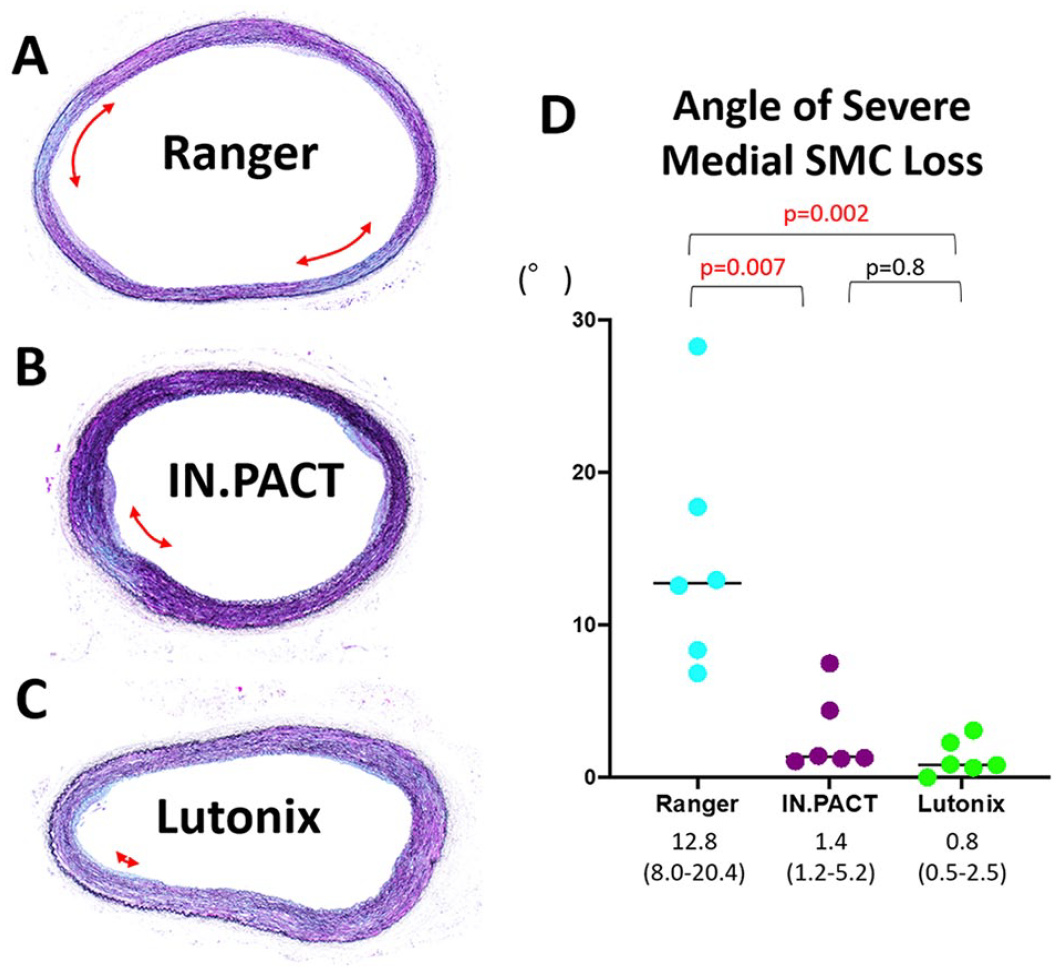
Angle of severe medial SMC loss (A–C) Representative pictures of the measured angle with severe medial SMC loss (red arrows) of each DCB. (D) The angle of severe medial SMC loss was the largest in the Ranger group, followed by the IN.PACT and Lutonix groups. DCB, drug-coated balloon; SMC, smooth muscle cell.
Histopathological Evaluation of Distal Skeletal Muscles
The histological analysis of the downstream skeletal muscles demonstrated vascular changes in all rabbits evaluated in the current study although the number of affected arteries differed among groups (Figure 6). The number of arteries with DCB-induced downstream effects was the highest in the IN.PACT group, followed by the Ranger and Lutonix groups (Ranger vs IN.PACT vs Lutonix, 3 [3–4] vs 4 [3–7] vs 2 [1–2], respectively; Table 2), which was consistent with the measured tissue paclitaxel concentrations.
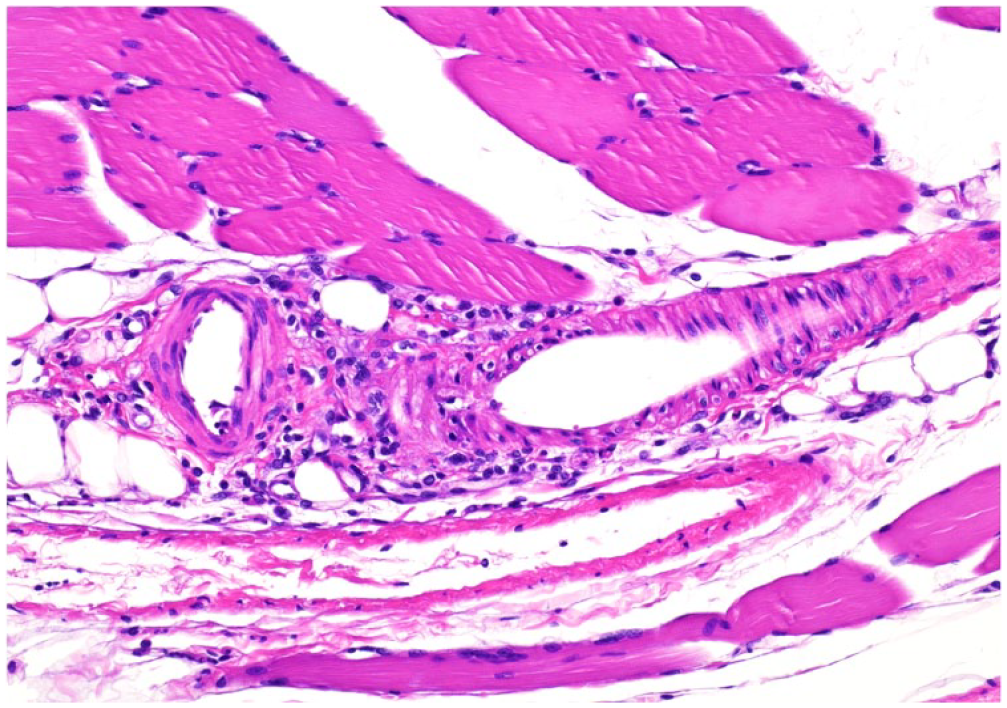
Vasculitis due to distal particulate emboli after IN.PACT use Note the moderate inflammatory cell reaction around arteries of the distal skeletal muscle.
Discussion
Our main findings are as follows: (1) the paclitaxel effect was the strongest for the low-dose paclitaxel-coated DCB Ranger, followed by IN.PACT and Lutonix. Histopathologically, paclitaxel had a more circumferentially distributed effect in the Ranger group compared with the other 2 DCB groups. (2) Distal particulate embolization effects were strongest for the high-dose paclitaxel-coated DCB IN.PACT, followed by Ranger and Lutonix, suggesting an influence of the paclitaxel dose for predicting downstream embolization. The results of the current study suggest that Ranger is one of the best DCBs compared with the other 2 examined DCBs, with the strongest paclitaxel effect to prevent restenosis, as well as the second best regarding the degree of distal particulate embolization.
This study has evaluated paclitaxel effects in the target vessel both pathologically and biologically. In this study, Ranger, which is one of the low-dose paclitaxel-coated DCBs, demonstrated a higher paclitaxel efficacy compared with the high-dose paclitaxel-coated DCB IN.PACT, especially regarding the histologically evaluated circumferential distribution of the paclitaxel effect. Although this result was not statistically significant, the tendency toward a superior effect was consistent with the findings of other preclinical studies.11,12 Moreover, Ranger showed significantly superior paclitaxel effects compared with Lutonix, another low-dose paclitaxel-coated DCB. This result was consistent with those of previous animal studies,10–12 suggesting the importance of the paclitaxel “coating integrity” rather than the drug dose. These results were also in line with the findings of clinical trials. The COMPARE trial, a prospective, randomized trial in patients with femoropopliteal lesions, demonstrated similar primary patency of IN.PACT and Ranger, suggesting better coating integrity in the Ranger low-dose paclitaxel-coated DCB (2.0 µg/mm2) compared with the IN.PACT high-dose paclitaxel-coated DCB (3.5 µg/mm2). 23
This study also demonstrated that distal particulate emboli, evaluated by the paclitaxel concentration in distal skeletal muscles, were less likely in low-dose paclitaxel-coated DCB groups (Lutonix and Ranger) than in the high-dose paclitaxel-coated DCB group (IN.PACT). This result may explain the concern described in the recent meta-analysis by Katsanos et al showing a higher risk of major amputation in patients treated with DCB, especially with high-dose paclitaxel, compared with those with plain balloon angioplasty. 9 However, one of the serious limitations of the meta-analysis was that RCTs for older-generation devices not available anymore, such as IN.PACT Amphirion DCB (Medtronic, Galway, Ireland) in the INPACT-DEEP trial, were included in the analysis. 24 More recently, Hata et al 25 published a multicenter retrospective study (RADISH trial) analyzing 927 CLTI patients with DCB use for femoropopliteal lesions. According to their study, the propensity score-matched comparison of the DCB group vs the non-DCB group revealed comparable rates of the 1-year cumulative incidence of wound healing (DCB group vs non-DCB group: 74.4% vs 71.9%, p=0.93) with a higher rate of primary patency (82.7% vs 69.2%, p=0.002).
The study findings from the INPACT-DEEP and RADISH trials suggest that paclitaxel-coated on DCBs improves primary patency. However, the higher incidence of distal emboli with older-generation DCBs might be harmful to distal tissues, resulting in a higher risk of major amputation. Therefore, the ideal DCB for femoropopliteal lesions in patients with CLTI would be a DCB with greater drug effect and fewer distal emboli.
A recent case report has demonstrated that distal particulate embolization resulted in focal vasculitis of the amputated big toe in a patient who had received upstream DCB treatment in the popliteal artery for CLTI 3 months before the amputation. 26 Although with varying degrees, distal particulate embolization occurs in all DCBs as shown in this study. Using DCBs for upstream diseased arteries may increase blood flow to the ulcerated lesion in patients with CLTI; however, the risk of downstream particulate embolization also increases and may cause deterioration of the ulcer. 27 Therefore, an adequate DCB with a strong paclitaxel effect and low risk of distal emboli should be used especially in patients with CLTI and limited flow reserve in downstream arteries below the knee. DES might be another effective treatment option, especially in lesions with severe calcification.28–32 A previous preclinical study has demonstrated significantly less risk of distal embolization in DES compared with IN.PACT. 17
Study Limitations
The current preclinical study has several limitations. This study was performed using descending aortas of healthy rabbits. This model does not fully represent the atherosclerotic and often highly calcified femoropopliteal arteries of humans. In addition, the current preclinical study does not contain any clinical data. However, in daily clinical practice, it is almost impossible to determine whether a CLTI exacerbation is due to distal particulate embolization after DCB use or the natural course of CLTI. Therefore, animal models may be one of the important options to compare drug effects, as well as the degree of distal particulate embolization, among several DCBs. Paclitaxel concentrations and histology should ideally be assessed in different rabbits. We have evaluated them in the same aorta which may have introduced errors due to technical difficulties. However, we have carefully checked the exact location of the treated lesion using angiogram guidance to prevent mislocalizing the treated lesion. Finally, the sample size was not calculated in the current preclinical study, and control animals with plain balloon treatment were not included. According to previous preclinical studies10–16 and a recommendation from a consensus group, 33 we believe that the number of animals used in the current study (n=6 per group) was adequate, and control groups with plain balloon treatment were not required.
Conclusion
The findings of this study suggest that Ranger is one of the best DCBs, being the best regarding the paclitaxel effect and the second best regarding distal particulate embolization. Further clinical head-to-head comparisons with larger numbers of patients are needed to examine which DCB is the most effective and safe treatment option.
Supplemental Material
sj-docx-1-jet-10.1177_15266028231161215 – Supplemental material for Differences in Biologic Drug Effects and Distal Particulate Embolization in Three Paclitaxel-Coated Balloons for Femoropopliteal Lesions in a Rabbit Model
Supplemental material, sj-docx-1-jet-10.1177_15266028231161215 for Differences in Biologic Drug Effects and Distal Particulate Embolization in Three Paclitaxel-Coated Balloons for Femoropopliteal Lesions in a Rabbit Model by Marie Yoshikawa, Sho Torii, Kazuki Aihara, Masatoshi Ito, Norihito Nakamura, Satoshi Noda, Ayako Yoshikawa, Sayo Utsunomiya, Gaku Nakazawa MD and Yuji Ikari in Journal of Endovascular Therapy
Supplemental Material
sj-docx-2-jet-10.1177_15266028231161215 – Supplemental material for Differences in Biologic Drug Effects and Distal Particulate Embolization in Three Paclitaxel-Coated Balloons for Femoropopliteal Lesions in a Rabbit Model
Supplemental material, sj-docx-2-jet-10.1177_15266028231161215 for Differences in Biologic Drug Effects and Distal Particulate Embolization in Three Paclitaxel-Coated Balloons for Femoropopliteal Lesions in a Rabbit Model by Marie Yoshikawa, Sho Torii, Kazuki Aihara, Masatoshi Ito, Norihito Nakamura, Satoshi Noda, Ayako Yoshikawa, Sayo Utsunomiya, Gaku Nakazawa MD and Yuji Ikari in Journal of Endovascular Therapy
Supplemental Material
sj-tif-3-jet-10.1177_15266028231161215 – Supplemental material for Differences in Biologic Drug Effects and Distal Particulate Embolization in Three Paclitaxel-Coated Balloons for Femoropopliteal Lesions in a Rabbit Model
Supplemental material, sj-tif-3-jet-10.1177_15266028231161215 for Differences in Biologic Drug Effects and Distal Particulate Embolization in Three Paclitaxel-Coated Balloons for Femoropopliteal Lesions in a Rabbit Model by Marie Yoshikawa, Sho Torii, Kazuki Aihara, Masatoshi Ito, Norihito Nakamura, Satoshi Noda, Ayako Yoshikawa, Sayo Utsunomiya, Gaku Nakazawa MD and Yuji Ikari in Journal of Endovascular Therapy
Footnotes
Acknowledgements
The authors thank Sachie Tanaka and Shuho Hori (Support Center for Medical Research and Education, Tokai University) for their valuable technical assistance.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This study was sponsored by Boston Scientific Japan (Tokyo, Japan). S.T. received research grants from Abbot Vascular Japan, Boston Scientific Japan, Medtronic, and received honoraria from Boston Scientific Japan. G.N. is a consultant for Boston Scientific, Abbott Vascular, Terumo Corp., and Japan Medical Device Technology Co., Ltd, and received research grants from Boston Scientific, Abbott Vascular, Terumo Corp., and Japan Medical Device Technology Co., Ltd.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by Boston Scientific Japan (Tokyo, Japan).
IRB Information
The Animal Care and Use Committee of Tokai University has reviewed and approved the current study (reference number: 211052).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.