
Abstract
Purpose:
The objective of this case is to report an endovascular occlusion of an acquired vascular fistula using an Amplatzer Vascular Plug II. Also, it is to review the available literature on risk factors, pathophysiology, and related management strategies about complications of the tunneled central venous catheter (TCVC).
Case Report:
The case was a 40-year-old man with a chronic kidney disease (CKD) on dialysis and with a history of several previous TCVC placements, along with recurrent infections. The last TCVC developed a fistula between the superior vena cava and the right pulmonary artery, shown by computed tomography (CT). We decided to remove a long-term TCVC and occluded the fistula applying an endovascular embolic device, an Amplatzer Vascular Plug II, subsequently. The patient was given parenteral treatment during 10 days of hospitalization. Over 9 months of follow-up, the device was appropriately positioned and did not obstruct the vascular flow.
Conclusion:
Tunneled central venous catheters are frequently used for hemodialysis in patients in the last stage of CKD who do not have an arteriovenous fistula. Occasionally, delayed complications such as adherence or catheter migration occur. This case illustrates an endovascular treatment with excellent results and low risk of morbidity and mortality.
Clinical Impact:
The purpose of this work is to present an endovascular occlusion by means of an Amplatzer® Vascular Plug II in a residual fistula. The endovascular way is decided in situations, for instance, once the cardiothoracic surgeons argue that the patient is not in general conditions to tolerate surgery, the surgical procedure would be complex, or, in a surgical approach with a difficult-to-resolve hemorrhage. We explain the technique and the materials we used for an excellent result and a low risk of complications. This case is intended to serve as an aid in the treatment of similar events.
Keywords
Introduction
Despite the recommendations of all clinical practice guidelines, tunneled central venous catheters (TCVCs) are commonly used for long-term vascular access for hemodialysis in the last stage of chronic kidney disease (CKD).1,2 After the first year of TCVC use, approximately one-third of patients have complications. They usually present with catheter failure, venous thrombosis, infection, or venous stenosis. 3 Vessel perforation and vascular or venobronchial fistulas are very rare complications that can be life-threatening. 4
Herein, we describe the case of a CKD patient on dialysis and with a history of several previous TCVC placements, along with recurrent infections. The left jugular TCVC developed a fistula between the superior vena cava (SVC) and the right pulmonary artery (RPA) and had a high probability of lethal sepsis and massive mediastinal hemorrhage or cardiac shunt. The fistula was effectively managed percutaneously by removing the catheter and using a closure device, an Amplatzer Vascular Plug II (VP II). The VP II is used to embolize large and high-flow vessels. 5 A literature review indicated that this is the first reported case of using a VP II to occlude this kind of acquired vascular fistula.
Case Report
A 40-year-old male patient (weight 54 kg, height 163 cm) with stage 5 CKD stemming from primary glomerulopathy had been on hemodialysis for 6 years. He had a history of TCVC placement in the right jugular (2016) and left jugular (2019) veins. He had also had a Tenckhoff catheter placed for peritoneal dialysis (2018), but it did not function for long as a result of recurring episodes of peritonitis caused by Staphylococcus aureus.
During the previous year, ampicillin-sensitive Enterococcus casseliflavus had been isolated twice, and later, oxacillin-resistant Staphylococcus lentus had been isolated once from the left jugular TCVC. Systemic antibiotics were administered in these cases. The patient remained asymptomatic until catheter dysfunction arose. A nontunneled catheter was placed in the right femoral vein, and during the first dialysis, the patient developed fever, chills, and hypotension. In-hospital antibiotic treatment and new blood cultures were required; the femoral catheter was removed because of the risk of sepsis. After evaluation by the vascular surgery department, a new TCVC was placed in the right jugular vein.
Chest radiograph and computed tomographic (CT) scans showed that the left TCVC tip was abnormally positioned in an RPA branch (Figures 1 and 2).
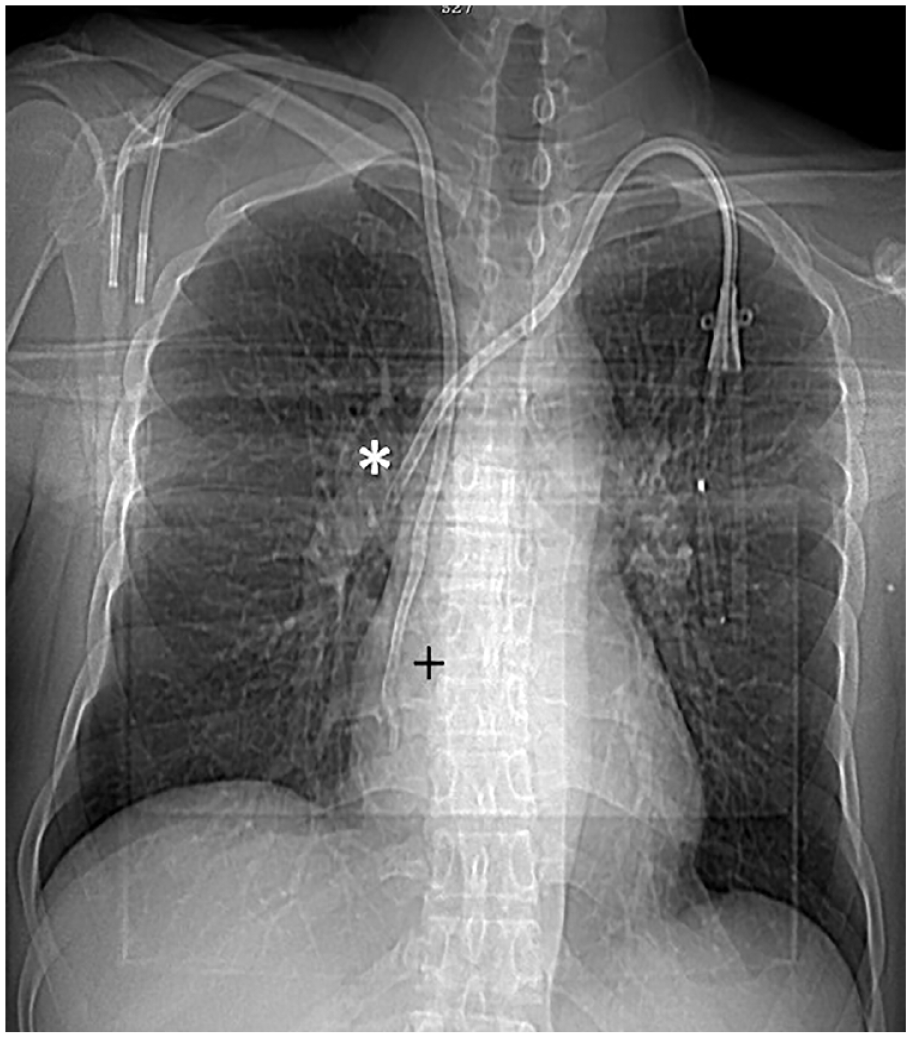
Chest radiograph showing the tip of the left TCVC in an anomalous position (*), unlike the right TCVC functioning in the right atrium (+). TCVC, tunneled central venous catheter.
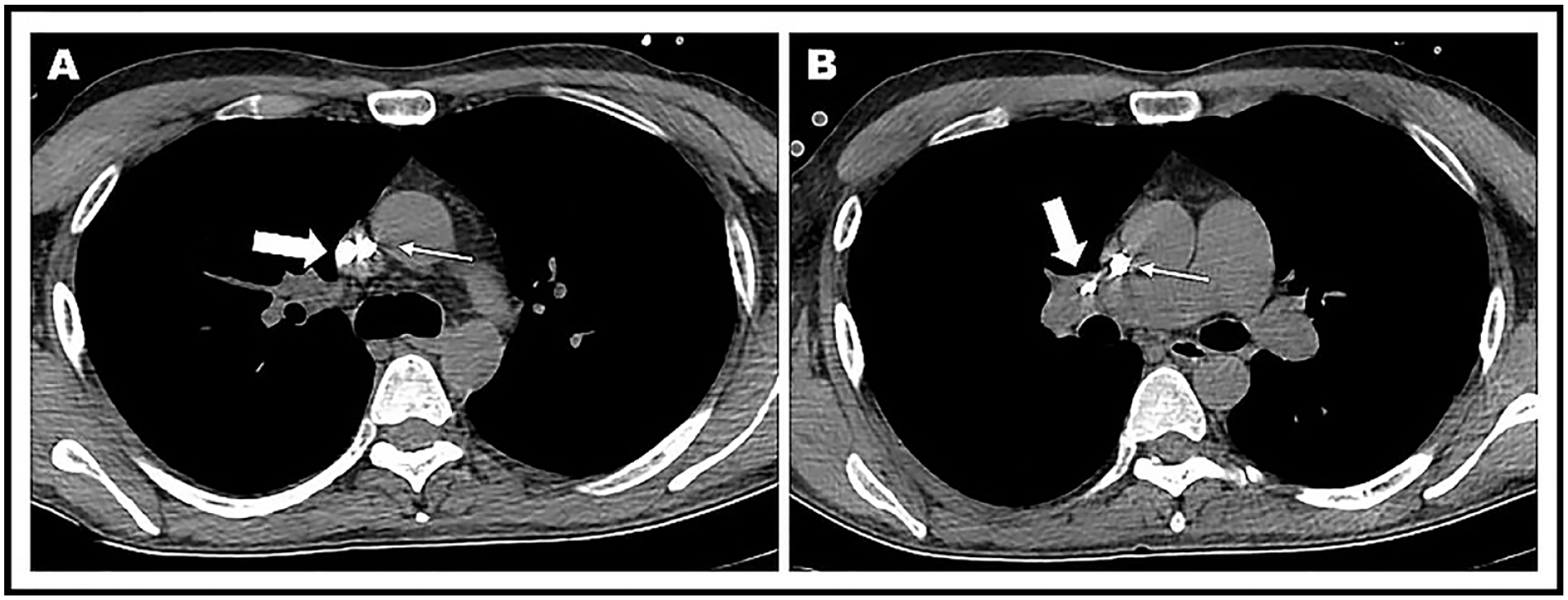
(A) On chest CT, the location of the left TCVC is situated on the lateral wall of the SVC (thick arrow) next to the right TCVC (thin arrow). (B) The tip of the left TCVC is observed in the RPA (thick arrow), and the right TCVC is in a satisfactory location within the SVC (thin arrow). CT, computed tomography; TCVC, tunneled central venous catheter; SVC, superior vena cava; RPA, right pulmonary artery.
Therapeutic Intervention
After multidisciplinary evaluation between the thoracic surgery, endovascular (hemodynamics), and vascular surgery departments, it was decided to endovascularly remove the left TCVC and close the vascular fistula using a VP II. A 6F introducer was used to achieve single right femoral venous access under local anesthesia. Initial phlebography was performed from a 5F pigtail catheter positioned in the left brachiocephalic vein (LBV), and a fibrin sheath was visualized around the TCVC in the LBV (Figure 3A). A 0.035″ × 260 cm hydrophilic guidewire (HydroSteer, SJM) was introduced through the left TCVC. We verified the location of the catheter tip via angiography (Figure 3B) and positioned the distal end of the guidewire in the pulmonary artery trunk. From the femoral access, an Amplatz Goose Neck Snare catheter (Medtronic) was introduced to connect the distal end of the upper guide wire (Figure 3C). The guidewire was gently pulled until femoral externalization was achieved. The left TCVC was then removed, and the catheter tip was sent for culture.
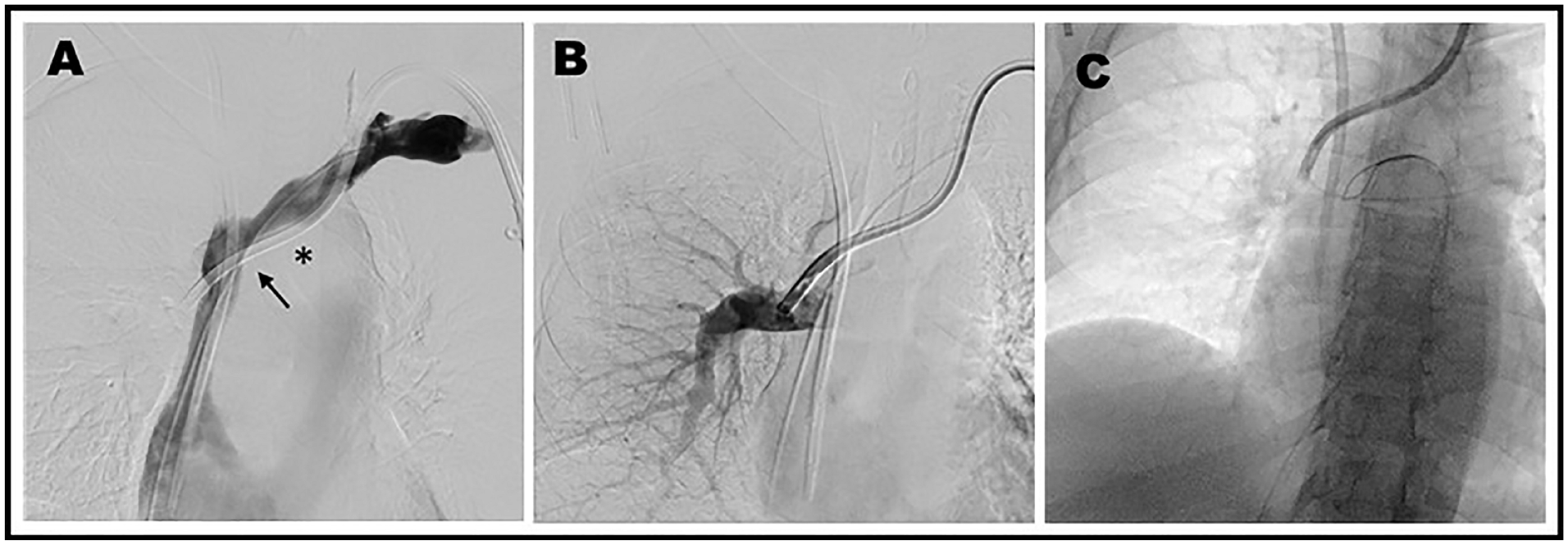
(A) LBV phlebography: a fibrin sheath is visible in the proximal segment of LBV (*) and the exit site of TCVC in SVC (arrow). (B) Direct injection through the left TCVC, confirming the position of the catheter tip in the right branch of the pulmonary artery. (C) Looping maneuver of the 0.035″ hydrophilic guidewire from the TCVC that was then exteriorized by a right femoral introducer. LBV, left brachiocephalic vein; TCVC, tunneled central venous catheter; SVC, superior vena cava.
A 5F right coronary Judkins catheter (JR 3.5) was introduced over the hydrophilic guidewire until it was positioned at the level of the inferior vena cava. The HydroSteer was then exchanged for an Amplatzer 0.035″ × 260 cm 1.5 J-tip guidewire whose distal end was located in the right primitive iliac vein. The JR catheter was removed, and an Amplatzer TorqVue 180 or 8F × 80 cm release catheter was placed over the Amplatzer guidewire to reach the level of the pulmonary artery trunk. After the removal of the Amplatzer guidewire, a 12-mm Amplatzer VP II was introduced, and through angiographic control, it was positioned between the SVC and RPA, thereby successfully closing the vascular fistula without occluding any vessels (Figure 4).
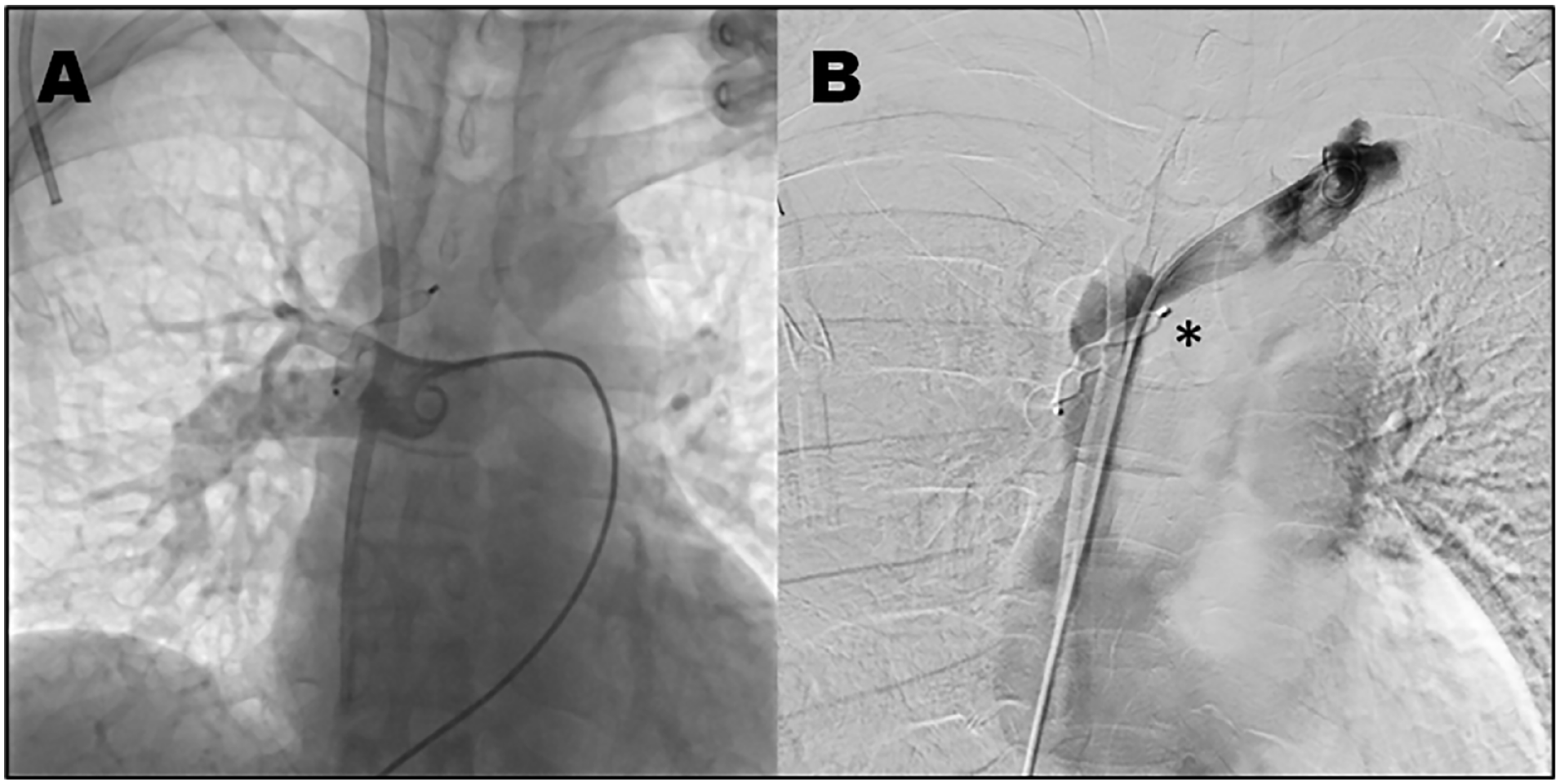
(A) Final angiographic control of the pulmonary artery: the permeability of all right pulmonary branches was verified. (B) Final angiographic control from the LBV: the permeability of the LBV and SVC was observed. The defective opening of the VP II proximal disc was also observed (*) because the fibrin sheath that developed in the TCVC over time was embolized. LBV, left brachiocephalic vein; SVC, superior vena cava; VP II, Vascular Plug II; TCVC, tunneled central venous catheter.
Follow-up and Outcome
Results from the blood and catheter tip cultures indicated Serratia plymuthica, a producer of AmpC-type beta-lactamase, and Candida parapsilosis, for which the patient was given parenteral treatment during 10 days of hospitalization. After discharge, he was referred to the vascular surgery department for performance of the arteriovenous fistula. The patient evolved asymptomatically over 9 months of follow-up, and echocardiographic and tomographic controls verified that the device was adequately positioned and did not obstruct the flow of the LBV, SVC, or RPA.
Discussion
The prolonged use of a TCVC for hemodialysis is common in patients who do not have a fistula or arteriovenous graft due to various anatomical or vascular factors or who refuse such procedures.1,2 Such was the case for the current patient, who desired to exclusively use hemodialysis catheters.
Tunneled central venous catheters allow blood flows greater than 300 mL/min; they are double-lumen devices with cross-sectional diameters between 13.5F and 15.5F. 2
Given the duration of use, blood flow, and incidence of complications, placing the TCVC in the left jugular vein is not recommended if there is access on the right side. 6 If the tip of the catheter is far from the right atrium, it is likely that over time it will adhere to the wall of the SVC and prevent its proper functioning, so it is better to place the tip of the device within the right atrium.4,6 The placement should be guided by imaging (digital fluoroscopy and ultrasound). 2
The most common complications associated with long-term catheter use are catheter dysfunction (secondary to mainly thrombotic events or catheter migration), catheter-related bacteremia (CRB), and pericatheter central venous stenosis.6,7 Our patient experienced recurrent CRB, probably associated with connector manipulation without signs of infection at the catheter entry site. Pathophysiologically, thrombogenesis and fibrin production can occur on the internal surface of the catheter; this process favors the colonization and proliferation of microorganisms, which form biofilms that progressively decrease the flow through the catheter. This decrease in flow leads to greater manipulation of the catheter, increasing the risk of infection and creating a vicious circle between mechanical complications and catheter colonization.8,9 Unusual complications of a delayed TCVC include adherence of the catheter tip 10 and perforation in the SVC with bronchial fistulization, 11 which are both associated with placement through the left jugular vein. As the catheter is placed, it passes through the lateral or posterior wall of the SVC. These 2 walls are relatively weak because they are not covered by the pericardium. In addition, when the tip of the catheter is along the wall of the SVC, the vessel endothelium can be damaged over time by breathing movements, cardiac contraction, and manipulation during dialysis. Together, these factors predispose patients to the formation of thrombi and thus to the adherence to and perforation of the venous wall.10 –12
Based on our analysis, we have described technical factors in placing the TCVC and its infectious and thrombotic aspects, along with erosion of the SVC and the RPA wall, leading to anomalous communication between the 2 vessels.
To initially determine the location of the catheter tip, a chest radiography was performed. However, the diagnostic technique of choice is angiography via the catheter. 1 A chest CT angiogram or a transesophageal or transthoracic echocardiogram can also be performed. 11
In addition to the administration of systemic antibiotics, it is essential to consider multiple options to manage catheters in the treatment of CRB.3,13 Here, the patient was recurrently treated exclusively with intravenous antibiotics for 1 year. We assume that he was so treated because of his hemodynamic stability and the absence of signs of infection in the device.
Some reports of delayed complications associated with central venous access recommend occluding arteriovenous fistulas by placing a coil at the site of the vascular connection or placing covered stents. 14 Alternatively, in the case of a venobronchial fistula, a balloon can be used to obstruct communication, and then gelatin sponge pledgets are used for embolization. 4
We chose endovascular management to reduce the risk of morbidity and mortality associated with open surgery. We considered removing the catheter because of the threat of lethal sepsis in the patient, in addition to occluding the fistula in the same procedure, due to high risk of massive hemorrhage or cardiac shunt. We selected the VP II for its double-anchoring design and flexible structure, which adjusts to the shape of the vessel and prevents migration after implantation; it was originally used to embolize peripheral arteriovenous vascular defects but has additional uses today.5,15 During the VP II placement, the opening and anchoring of the distal disc were achieved in the RPA. However, the proximal disc opening was not visualized because of the chronicity of the catheter, and a fibrin sheath had formed around it in the LBV, which we interpreted as an occlusion of the fibrin sheath without an impairment of vascular flow (Figure 4).
Conclusion
The long-term use of TCVCs should be limited because of their associated complications. Preventing complications begins with an adequate catheter insertion technique. The TCVC should be removed if dysfunction or persistent infection is observed. We recommend the endovascular option to treat this kind of acquired vascular fistulas, which yields excellent results and has a low risk of complications, as long as there is exhaustive image-guided planning. It is especially valuable in select and high-risk patients. Echocardiography and tomography are useful for the VP II follow-up.
Footnotes
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethics approval is not required.
Patient Consent Statement
Informed consent was obtained from the patient for publication of this case report and any accompanying images.