
Abstract
Purpose:
To measure the long-term proximal aortic neck dilatation (AND) after elective endovascular aortic aneurysm repair (EVAR) with a variety of contemporary, third-generation, endograft devices.
Materials and Methods:
This is a noninterventional prospective cohort study of 157 patients that underwent standard EVAR with self-expanding abdominal endografts. Patients’ recruitment lasted from 2013 to 2017, and postoperative follow-up was up to 5 years. A computed tomography angiography (CTA) was performed at the first month and then at 1, 2, and 5 years. Proximal aortic neck’s (PAN) basic morphological characteristics (diameter, length, angulation) were measured based on the analysis of CTA in a standardized fashion. Neck-related adverse events, such as migration, endoleak or rupture, and reinterventions were recorded.
Results:
Significant straightening of the PAN was evident even in the first-month CTA with concurrent neck shortening that became significant at 5 years. Both the suprarenal aorta and the PAN significantly dilated overtime, with PAN dilating more progressively. Mean neck dilatation at the juxtarenal level was 0.8±0.4 mm at 1 year, 1.8±0.8 mm at 2 years, and 3.9±1.7 mm at 5 years, with a mean neck dilatation rate of 0.07 mm/month overall. The incidence of AND ≥2.5 mm was 37.2% at 2 years and 58.1% at 5 years after EVAR and was considered important (≥5 mm) in 11.5% of patients at 2 years and 30.6% of patients at 5 years. A multivariate analysis performed showed that the endograft oversizing, the preoperative neck diameter, and the preoperative abdominal aortic aneurysm sac diameter served as independent predictors of AND at 5 years. At the 5-year follow-up, 8 late type Ia endoleaks (6.5%) and 7 caudal migrations (5.6%) were identified, while no late ruptures were reported. In total, 11 late endovascular reinterventions (8.9%) were performed. Overall, proximal neck-related adverse outcomes (5/7 migrations and 5/8 endoleaks) and reinterventions (7/11) were significantly associated with the presence of important late AND.
Conclusion:
Proximal AND after EVAR is common. It can influence the long-term durability of proximal endograft fixation and is significantly associated with adverse outcomes, often leading to reinterventions. A systemic and extended surveillance protocol is needed for maintenance of good long-term results.
Clinical Impact
This is a thorough and systematic analysis of the long-term geometric remodeling of the proximal aortic neck after EVAR, that highlights the importance of a strict, and extended surveillance protocol for maintenance of good long-term results of EVAR.
Keywords
Introduction
Endovascular aortic aneurysm repair (EVAR) has been established as the preferred, first-line surgical treatment of abdominal aortic aneurysms (AAAs) compared to open repair because of its well-known advantages and favorable short-term and midterm results.1,2 However, late complications such as endoleaks, stent-graft migration, and continuing sac expansion remain the Achilles’ heel of EVAR, often raising the need for reintervention to avoid secondary sac rupture.3,4 Post-EVAR remodeling of AAA’s anatomic features has been proposed to be the main cause of failure in the long-term; thus, an increased interest in studying this phenomenon is noted in contemporary literature.5,6 The maintenance of successful seal between the stent-graft and the proximal aortic neck (PAN) is of crucial importance, so any anatomical changes at this level can lead to long-term destabilization of the proximal sealing zone and should be dealt with caution.6,7
Aortic neck dilatation (AND) has been the subject of several, observational, clinical studies over the past years, with contradictory results.7–14 Previous review articles lead to the conclusion that AND seems to affect a considerable proportion of EVAR patients and is often associated with worst clinical outcomes.15,16 However, the main limitation of the reviewed observational studies was that many of them reported on the use of older and no-longer-available stent-graft devices, with well-recognized structural failures, that are outdated and the fact that most of them presented midterm outcomes. Moreover, some studies reported outcomes of a single stent-graft device, which does not allow firm conclusions with applicability in other types of endografts.
The aim of this study was to investigate, through an extensive radiological follow-up program, the long-term evolution of AND after elective EVAR in patients with infrarenal AAA treated with a variety of contemporary, third-generation, stent-graft devices and to evaluate the effect of different endograft devices on the extent of AND. The ultimate goal was to explore the pathophysiology and the role of possible predisposing factors, as well as the assessment of the clinical importance of AND on the long-term post-EVAR outcomes.
Materials and Methods
Inclusion and Exclusion Criteria
This is a noninterventional prospective cohort study from a single university vascular surgery tertiary center. The investigational protocol was approved by the institutional ethics committee and was in accordance with the principles set forth in the Helsinki Declaration. Patients’ recruitment was performed during 2013 to 2017 and included a total of 198 consecutive patients with a true fusiform infrarenal AAA with a maximum sac diameter ≥50 mm, which were treated in our department by elective EVAR with a contemporary self-expanding abdominal aortic stent-graft (SESG). The prospectively collected data were analyzed retrospectively, and all patients have given their informed consent for participation, storage, and analysis of their medical information within the study frame.
Exclusion criteria included hostile proximal neck anatomy, 17 such as tapered or conical shape, diameter >30 mm, length <12 mm, angulation >60°, or circumferential mural thrombus/calcification >50%; symptomatic AAAs; pseudo-aneurysms or inflammatory aneurysms; hybrid aortic aneurysm repair and advanced techniques such as chimney EVAR, fenestrated EVAR, and branched EVAR; presence of malignancy, autoimmune, or other severe systematic diseases lowering the life expectancy and limiting long-term follow-up; pre-existing or new-onset chronic renal failure with eGFR <45 mL/min/1.73 m2 restricting the ability for follow-up with iodine contrast-enhanced computed tomography angiography (CTA). Patients treated with an abdominal endograft with less than 10 total cases and those lost during follow-up were also excluded.
Clinical Methodology
Baseline evaluation included a detailed medical history of all patients with emphasis on the risk factors for AAA, comorbidities, and medication. A thorough vascular examination was performed, and the routine laboratory workup included echocardiogram, chest x-ray, complete blood count, and basic coagulation and metabolic panel tests. The imaging protocol included a CTA, with intravenous power injection of a nonionic iodine contrast, without per os Gastrografin (Bayer Hellas) uptake and with a slice thickness of 0.5 mm and interval 0.3 mm, at 3 phases: arterial, portal venous, and delayed. The postimaging processing of anatomical data for preoperative planning as well as for radiological follow-up was performed based on the preoperative and postoperative picture archiving and communication system (PACS) data with the use of the dedicated 3D CTA analysis Horos software (GNU Lesser General Public License, Version 3.0). Stent-graft selection was based on the patients’ individual anatomical and morphological AAA features and the availability of endograft devices in our hospital. More specifically, based on the preoperative CTA data (ie, proximal neck diameter, length, angulation, shape, length, tortuosity or narrowing of iliac arteries, total length from lower renal to iliac bifurcation), the theoretically most eligible, according to the instructions for use, stent-graft device was chosen among those available at that time.
All patients were operated with a standard EVAR procedure using the same mobile C-arm fluoroscopic machine and the same technique and materials, preferably under locoregional anesthesia and with femoral cutdowns. Perioperative medication included the bolus intravenous administration of 2500 units of unfractionated heparin just before the cannulation of the common femoral arteries and chemoprophylaxis with cefoxitin 1 g b.i.d. In addition, all patients received daily postoperative thromboprophylaxis with tinzaparin sodium (50 IU anti-Xa/kg), until discharge. Patients were discharged in the absence of any complications, under life-long single antiplatelet medication with aspirin 100 mg o.d., unless indicated otherwise.
Patients followed a common, strict follow-up protocol up to 5 years after EVAR at least, with clinical evaluation and colored duplex abdominal ultrasound (cDUS) every 6 months. Our institutional imaging protocol with CTA included a scan at first postoperative month to verify the 30-day technical success. Further CTA follow-up was performed at 1, 2, and 5 years to detect any adverse outcome such as endoleak, migration, stent-graft fatigue, or continuous sac expansion, as well to assess the potential aortic remodeling and quantify the morphological changes of the PAN. Interim CTAs beyond the scheduled follow-up were performed in any case of clinical or cDUS evidence of potential adverse outcomes (mentioned above).
In our study, we used the following 6 abdominal aortic bifurcated self-expanding stent-graft devices: Endurant ΙΙ (Medtronic, Santa Rosa, California), Anaconda (Terumo Aortic, Bolton Medical, Florida), Treo (Terumo Aortic, Bolton Medical), E-tegra (JOTEC, Hechingen, Germany), AFX 2 (Endologix, Irvine, California), and Ovation (Endologix). All these devices have a nitinol self-expanding scaffold, whereas the graft’s fabric liner is made of expanded polytetrafluoroethylene (ePTFE) in the AFX 2 and Ovation devices and of woven polyester in the remaining 4. With the exception of Anaconda, which has infrarenal fixation, the other 5 devices offer suprarenal fixation with an uncovered bare metal stent.
Imaging Measurement Methodology
The standardized measurement technique of the basic morphological characteristics of the PAN was based on the analysis of CTA PACS data using the Horos software. All measurements were performed using the curved-path reformation tool (3D curved multiplanar reconstruction) after manual reconstruction of the central lumen line.18,19 The diameter of the suprarenal and infrarenal aorta was measured outer-to-outer wall (or adventitia to adventitia) 19 at 6 specific levels: (1) 10 mm above the highest renal artery (RA)—suprarenal (D1), (2) between the 2 RAs—interrenal (D2), (3) at the level of the lowest RA—juxtarenal (D3), (4) 5 mm and 10 mm below the lowest RA—infrarenal (D4 and D5, respectively), and (5) at the caudal end of the PAN just above the origin of the aneurysmatic sac (D6). The maximum sac diameter was also measured (DAAA) (Figure 1A). Proximal aortic neck was defined as the infrarenal part of the abdominal aorta with a maximum diameter ≤30 mm.
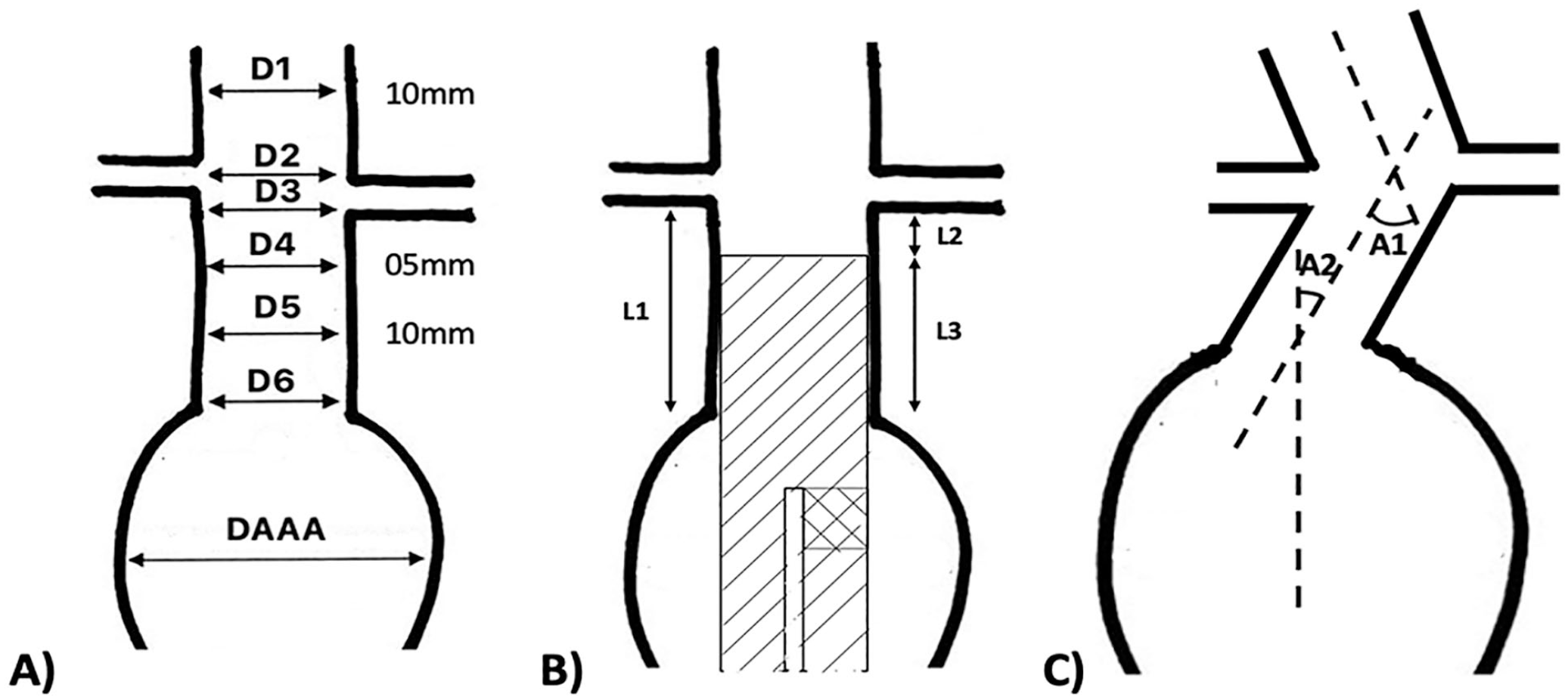
Illustration of the proximal aortic neck measurement methodology (description in text): (A) anatomical levels of aortic diameter measurements, (B) neck- and endograft-related length measurements after endovascular aortic aneurysm repair, and (C) neck’s proximal and distal angulation.
The length of PAN was measured as the longitudinal distance between the lowest RA and the caudal end of the PAN, which was considered also as the origin of the aneurysmatic sac (L1). L2 was defined as the distance between the lowest RA and the top of the covered part of the stent-graft and was involved in the definition of migration during follow-up. 20 L3 was defined as the length of the endograft’s proximal sealing zone and represented the region of overlapping between the stent-graft and the PAN (Figure 1B). Proximal or suprarenal angulation (A1) of the PAN was measured in regard to the longitudinal axis of the suprarenal abdominal aorta, whereas distal or infrarenal angulation (A2) was measured in regard to the longitudinal axis of the aneurysm sac (Figure 1C).
Each individual measurement in all CTAs was performed twice and blindly by 2 independent investigators (D.A.C. and A.G.P.). Following an intraobserver and interobserver variability analysis, the final value of each studied anatomical variable was calculated as the mean of 4 values; ie, the 2 blind measurements from the 2 observers. Per protocol, all potential differences between observers >10%, in any of the studied variables, were to be settled blindly by a third, senior investigator (G.A.P.).
Clinical and Imaging Outcome Definitions
Primary technical success was defined as the exclusion of the aneurysm sac, without any visible endoleak or technical failure and with zero mortality. 21 Assisted primary technical success was defined as the successful exclusion of the aneurysm sac after synchronous intraoperative correction of any detected primary failures. 21 Reintervention included all secondary, amending procedures that were performed during follow-up to correct EVAR-related late complications and prevent secondary rupture.
Aortic neck dilatation after EVAR was defined as the absolute increase of ≥2.5 mm in the PAN from the respective preoperative value at any level (D3–D6) and was considered important if it was ≥5 mm.1 The degree of endograft oversizing was measured as the ratio of the nominal main body diameter to the preoperative aortic neck diameter at the level of the lowest RA (D3). Migration was defined as the caudal displacement of the endograft and was considered clinically important if exceeded ≥10 mm (L2 ≥10 mm) from its original position on the 1-month CTA. 1 The presence of a type Ia endoleak at any time after EVAR was recorded, as was the continuous expansion of the aneurysm sac with or without rupture, requiring reintervention or not. Aneurysm sac regression was defined as the absolute diameter decrease of ≥5 mm from the respective preoperative value and was considered important if it was ≥10 mm.1
Statistical Analysis
All data were entered in a structured computerized database, and the statistical analysis was performed using the IBM SPSS Statistics program—version 22.0 for iOS (IBM, Armonk, New York). The significance level for all comparisons was defined at p<0.050. The interobservers’ and intraobservers’ variability was assessed by Bland-Altman plot and regression analysis, with excellent agreement between the blind measurements of the same observer and between the 2 observers in all cases. Categorical variables are presented as absolute and relevant frequencies and were analyzed with the chi-square test. Continuous variables that follow the normal distribution are presented as mean±standard deviation and were analyzed with paired 2-tailed Student t test, whereas those not following the normal distribution are presented as median and interquartile range and were analyzed with Mann-Whitney U test, as appropriate. Analysis of variance or Kruskal-Wallis test was used for comparisons of continuous variables between multiple independent groups, according to normality. Correlation between 2 continuous variables was performed with the Pearson rxy coefficient when both followed the normal distribution or by use of Spearman rs coefficient if at least one did not. A multivariate logistic regression was performed to assess the impact of the various independent variables on the incidence of AND, migration, and endoleak at 5 years. Finally, Kaplan-Meier analysis was used to construct survival curves to calculate freedom from AND during the follow-up.
Results
Supplementary Figure 1 depicts the study enrollment flowchart. Forty-one patients were excluded because of the exclusion criteria, and 157 patients were finally enrolled in analysis. The mean age was 73.2±7.1 years, and 151 (96.2%) were male. Patients’ demographics and baseline characteristics at the time of EVAR are presented in Table 1. The majority (n=148, 94.3%) were treated under spinal or local anesthesia with a mean operation time of 70.2±18.7 minutes and a mean fluoroscopy time of 12.3±4.5 minutes. The average volume of used contrast medium was 168±26 mL. The endograft device was deployed successfully in all cases. In 3 cases (1.9%), a type Ia endoleak due to proximal endograft misplacement was detected at the completion angiography and was managed successfully at the index procedure with implantation of a proximal aortic cuff. As such, assisted primary technical success was 100%. The median length of hospital stay was 3 days (2–5), and only 4 patients (2.5%) were required to stay in the intensive care unit for 24 hours, for monitoring, due to severe comorbidities. No 30-day mortality or major morbidity was noted.
Patients’ Demographics and Baseline Characteristics at the Time of EVAR.
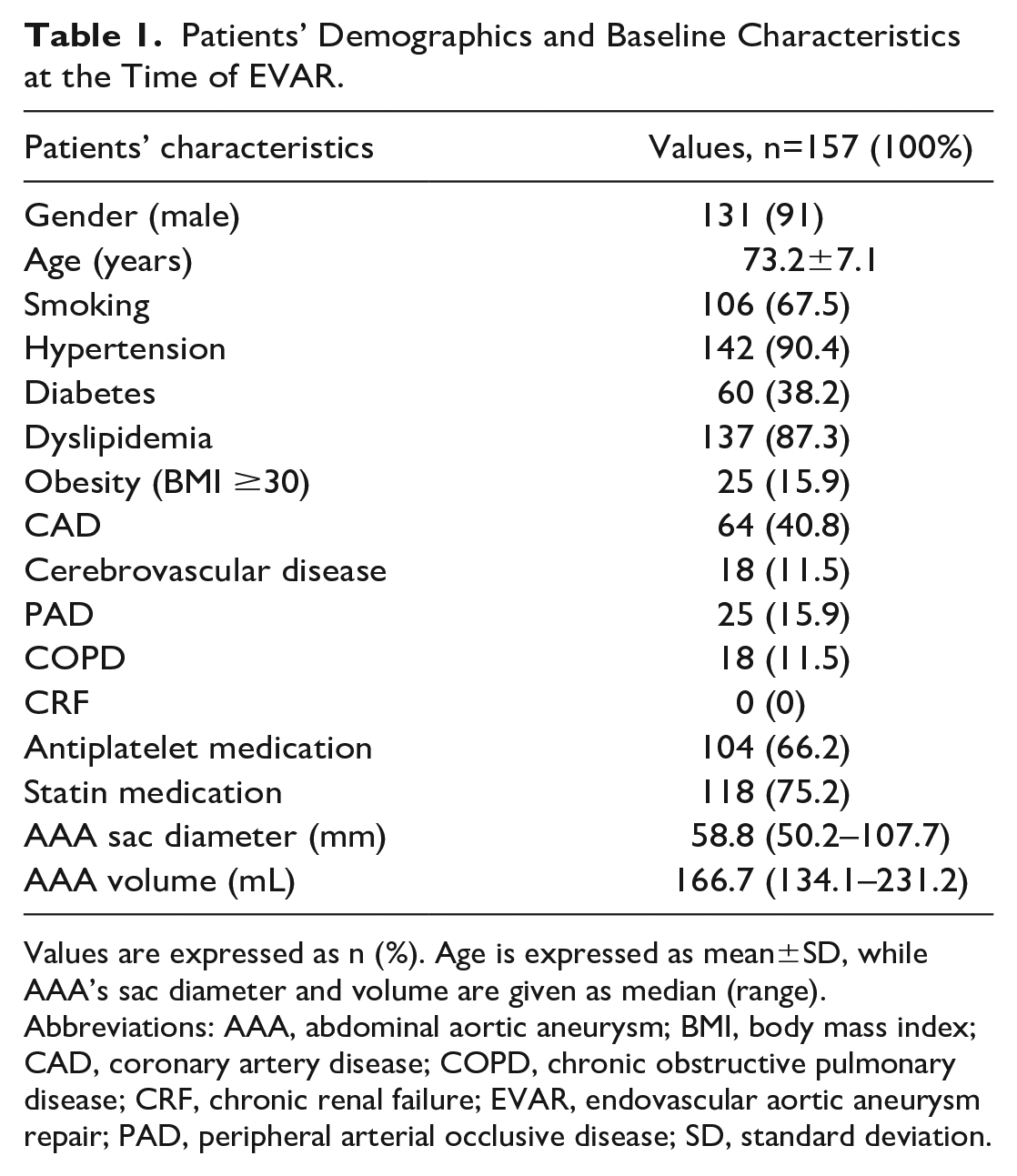
Values are expressed as n (%). Age is expressed as mean±SD, while AAA’s sac diameter and volume are given as median (range).
Abbreviations: AAA, abdominal aortic aneurysm; BMI, body mass index; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; CRF, chronic renal failure; EVAR, endovascular aortic aneurysm repair; PAD, peripheral arterial occlusive disease; SD, standard deviation.
Table 2 summarizes the clinical and imaging outcomes during the follow-up. All but 1 patient (n=156, 99.4%) completed the 2-year follow-up, with 124 (79%) of them reaching the 5-year follow-up milestone. All-cause mortality was 21% (n=33) at 5 years, with 32 deaths noted between 2 and 5 years, with none of them being aneurysm-, device-, or procedure-related (Table 2). At the 5-year follow-up, a total of 8 late type Ia endoleaks (6.5%) were discovered, which were accompanied by aneurysm sac expansion. Seven patients (5.6%) presented with important caudal stent-graft migration ≥10 mm. In 4 (57.1%) of them, the migration was accompanied by a type Ia endoleak, whereas in the remaining 3 (42.9%), the proximal sealing zone shortening was subclinical without measured sac expansion. All these cases (n=11 overall, 8.9%) were treated successfully with an endovascular placement of a proximal aortic cuff. No late rupture or graft infection were recorded in any case.
Clinical and Imaging Outcomes at 5-year Follow-up After EVAR.
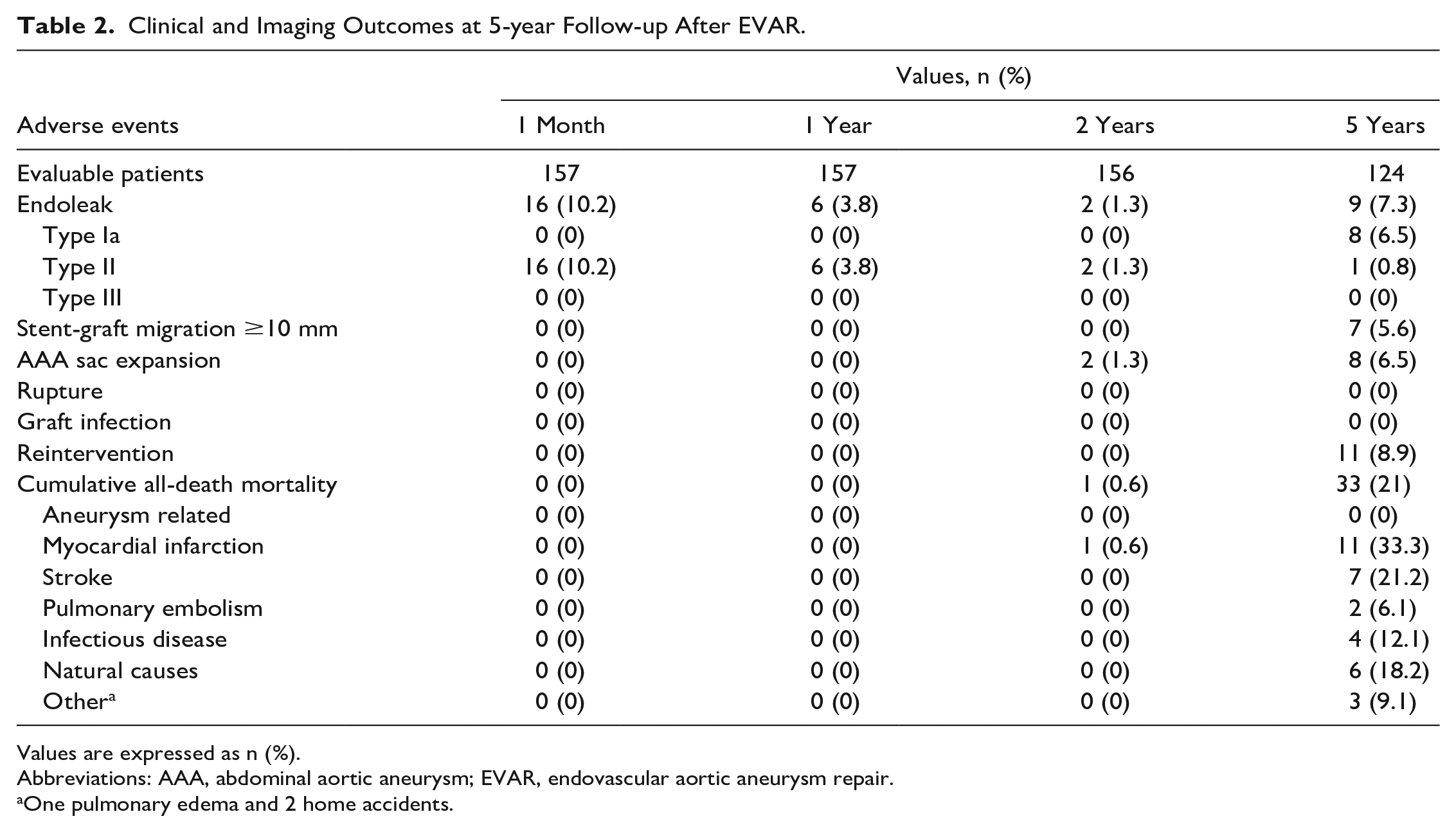
Values are expressed as n (%).
Abbreviations: AAA, abdominal aortic aneurysm; EVAR, endovascular aortic aneurysm repair.
One pulmonary edema and 2 home accidents.
Proximal Aortic Neck Remodeling
Substantial proximal aortic remodeling was observed during the long-term follow-up and involved the suprarenal aorta, the PAN (diameter, length, angulation), and the aneurysm sac per se. Significant straightening of the PAN was evident even in the first-month CTA with a proximal angulation (A1) decrease by 9.2±4.8° (p=0.046) and a distal angulation (A2) decrease by 17.3±8.1° (p=0.019). Over time, this phenomenon was smoothed down until the end of the 5-year follow-up (Table 3). The amount of PAN’s straightening was associated with the degree of the preoperative angulation at both levels. Patients with greater preoperative angulation of the PAN at any level experienced greater straightening after EVAR (r=0.69, p=0.001).
Proximal Aortic Neck Angulation Measurements During Follow-up.
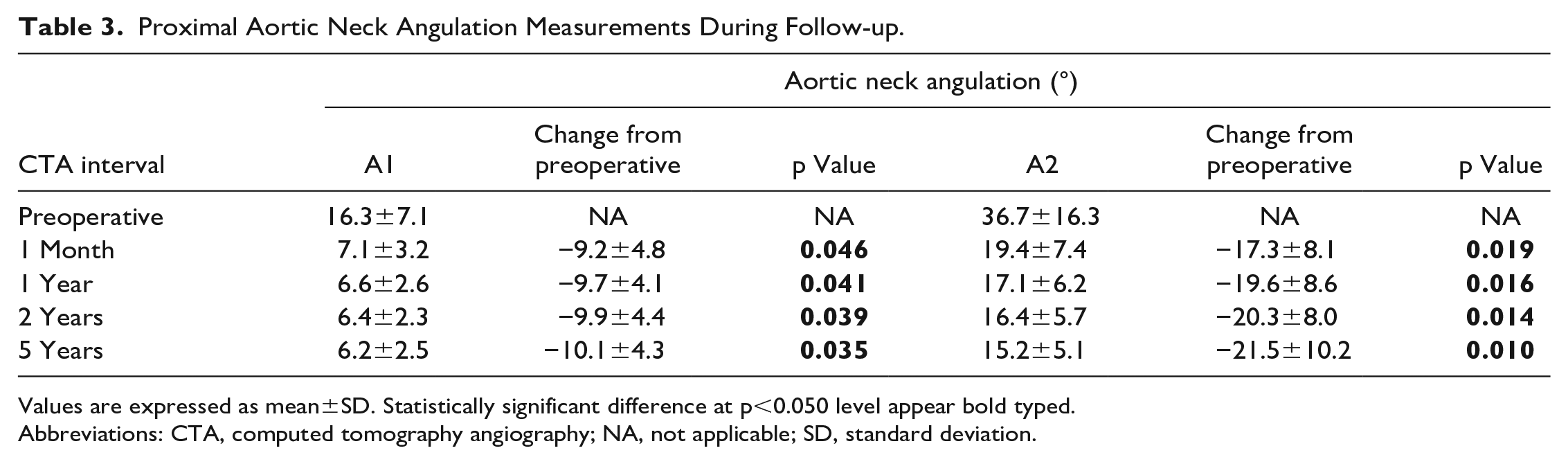
Values are expressed as mean±SD. Statistically significant difference at p<0.050 level appear bold typed.
Abbreviations: CTA, computed tomography angiography; NA, not applicable; SD, standard deviation.
The mean PAN’s preoperative length (L1) was measured at 24.8±3.8 mm. After EVAR, we witnessed a shortening of the PAN in our cases, with an L1 decrease by 1.2±0.6 mm at 1 year (p=0.123) and by 1.7±0.8 mm at 2 years (p=0.093), which became significant at 5 years (−2.4±1.1 mm, p=0.044) (Table 4). At the same time, the proximal sealing zone length (L3) was reduced by 1.5±0.7 mm at 2 years (p=0.102) and by 3.0±1.2 mm at 5 years (p=0.048). On average, the stent-grafts moved caudally 1.1±0.5 mm at 1 year and 2.0±1.0 mm at 2 years, reaching 4.0±1.9 mm at 5 years by the end of follow-up (p=0.038). We found a significant correlation of the L3 length at the 1-month CTA with the respective length change after 5 years (r=−0.51, p=0.022) and with the distance of migration (L2) at the same time (r=−0.47, p=0.031). As such, patients with a shorter L3 at the first month experienced greater reduction in proximal sealing zone length accompanied by greater caudal migration of the stent-graft. Moreover, the degree of PAN’s shortening (L1 decrease) was marginally correlated with PAN’s straightening at the infrarenal level (A2 decrease) (r=0.45, p=0.049). No significant correlation was found between the PAN’s shortening and the preoperative L1 length (p=0.088).
Proximal Aortic Neck Length Measurements During Follow-up.
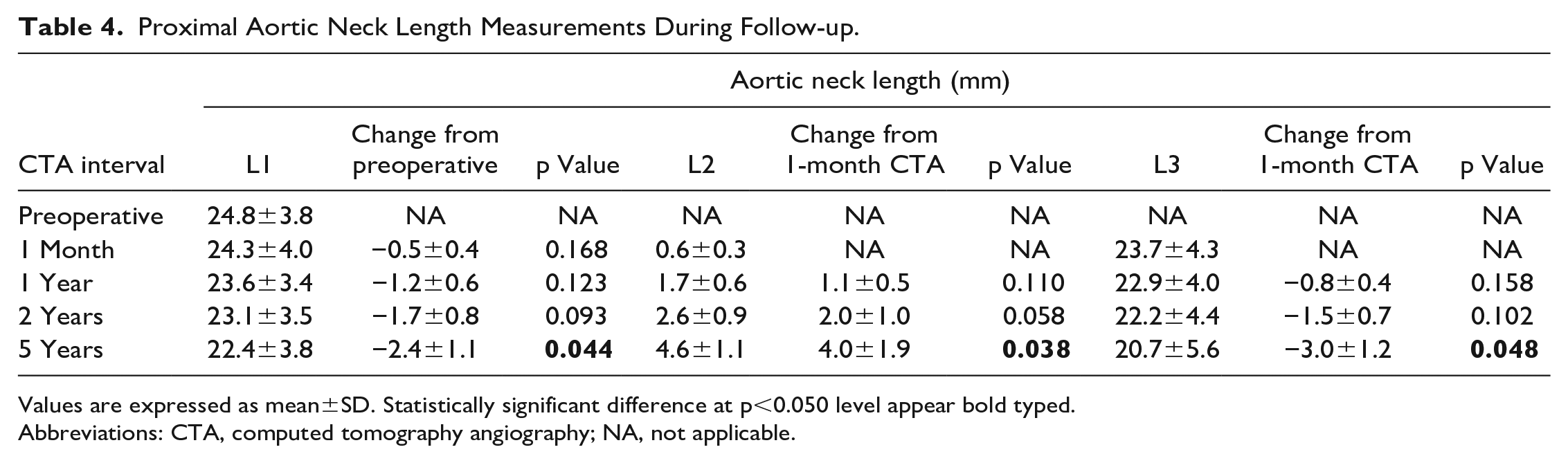
Values are expressed as mean±SD. Statistically significant difference at p<0.050 level appear bold typed.
Abbreviations: CTA, computed tomography angiography; NA, not applicable.
Table 5 depicts the diameter measurements of the PAN at various levels and their changes during the follow-up. Both the suprarenal aorta and the PAN significantly dilated overtime. The diameter of the suprarenal aorta at the level 10 mm above the highest RA (D1) and at the interrenal space (D2) increased by 2.9±1.6 mm (p=0.045) and 3.1±1.8 mm (p=0.038) at 5 years, respectively, with a mean dilatation rate of 0.05 mm/month overall, which was significantly higher during the first 2 years than that in the next 3 years (0.06 mm/month vs 0.04 mm/month, p=0.011). No correlation was found between straightening of the suprarenal aorta and its long-term dilatation (p=0.116).
Proximal Aortic Neck Diameter Measurements During Follow-up.
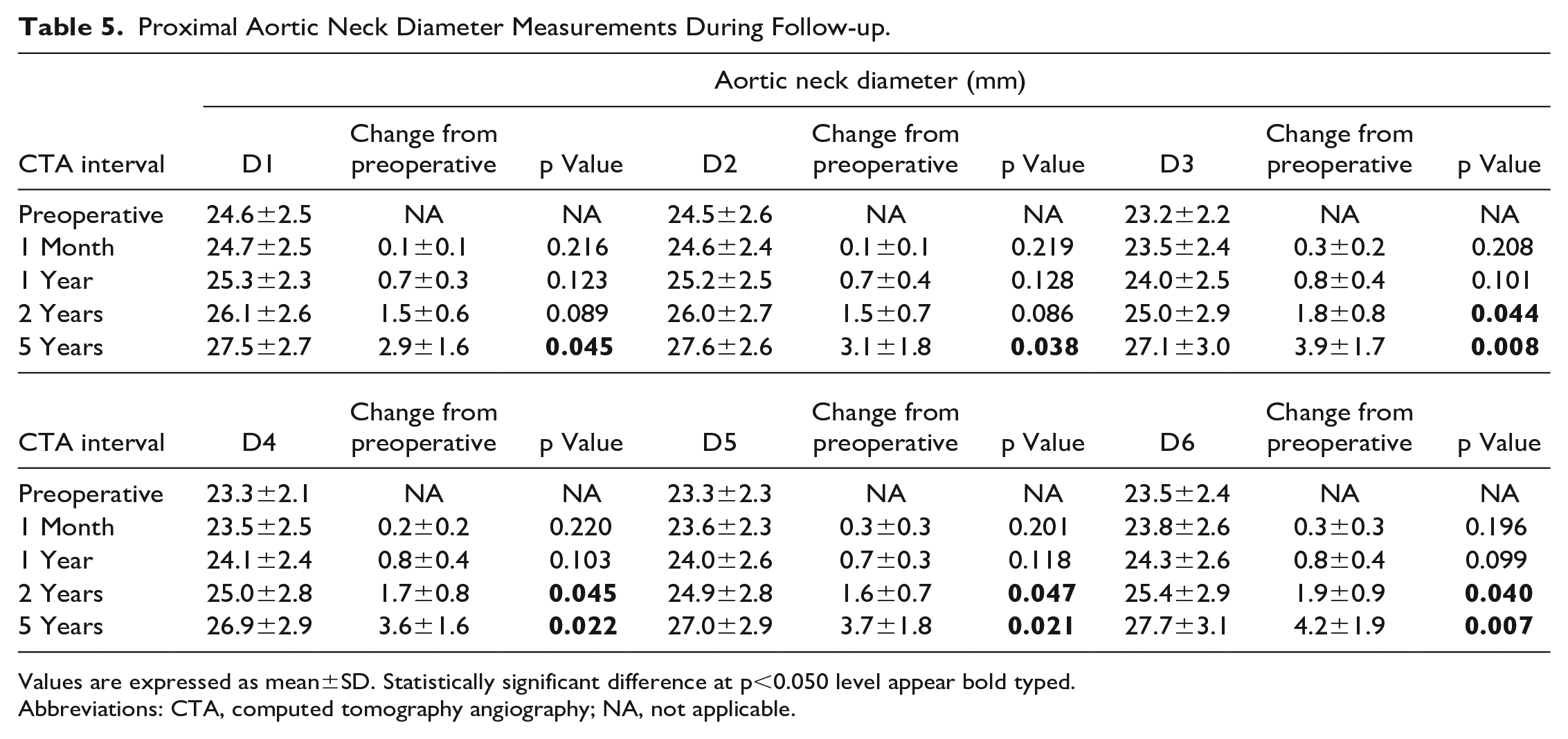
Values are expressed as mean±SD. Statistically significant difference at p<0.050 level appear bold typed.
Abbreviations: CTA, computed tomography angiography; NA, not applicable.
The PAN dilated more progressively over the years (Table 5 and Figure 2). The preoperative diameter at the level of the lowest RA (D3), 5 mm and 10 mm below the lowest RA (D4 and D5, respectively), and just above the aneurysm sac (D6) was measured at 23.2±2.2 mm, 23.3±2.1 mm, 23.3±2.3 mm, and 23.5±2.4 mm, respectively. During the 5-year follow-up, these diameters increased by 3.9±1.7 mm (D3; p=0.008), 3.6±1.6 mm (D4; p=0.022), 3.7±1.8 mm (D5; p=0.021), and 4.2±1.9 mm (D6; p=0.007). This increase was larger at the D3 and D6 levels (F=3.94, p=0.042) with a mean neck dilatation rate at the D3 level of 0.07 mm/month overall, which was significantly higher during the first 2 years than that in the next 3 years (0.08 mm/month vs 0.06 mm/month, p=0.038). Higher preoperative diameter values at any level were correlated with greater dilatation at 5 years at the same level (p=0.016), as was the larger preoperative sac diameter (p=0.029). Neither its angulation nor its length were significantly correlated to the diameter change (p=0.101 and p=0.094, respectively).
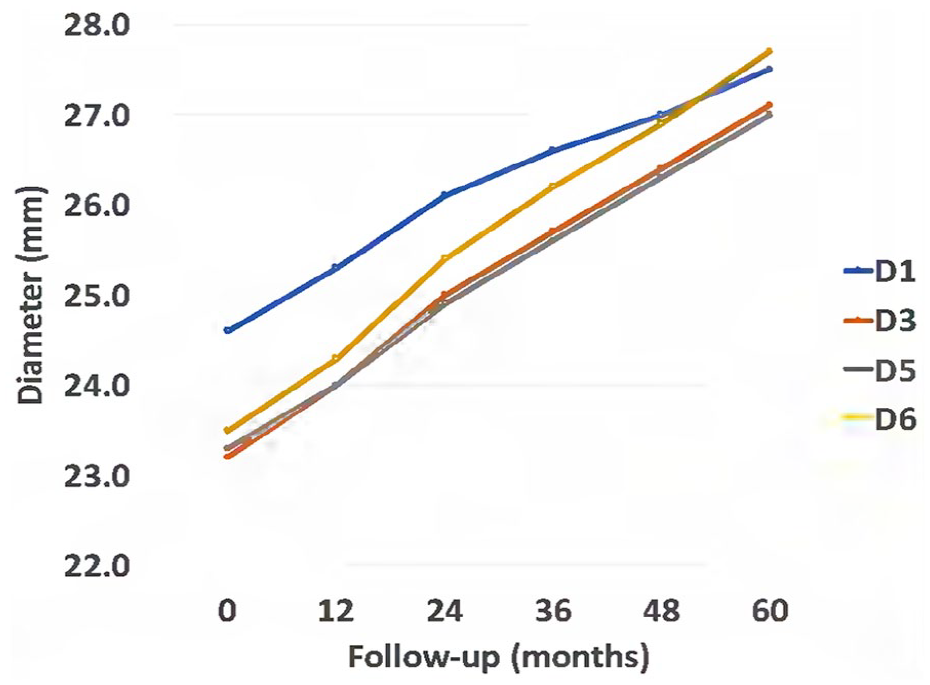
Suprarenal aorta (D1) and proximal aortic neck (PAN) (D3, D5, D6) dilatation during follow-up. PAN’s dilatation rate was higher at the D3 level during the first 2 years (p=0.051) and at the D6 level during the following 3 years (p=0.041). Overall, PAN’s diameter increased significantly more than the suprarenal aorta’s diameter (p=0.037).
Our results showed that AND ≥2.5 mm was evident in 12.7% (20/157) of patients at 1 year, 37.2% (58/156) at 2 years, and 58.1% (72/124) at 5 years after EVAR and was considered important (≥5 mm) in 11.5% (18/156) of patients at 2 years and 30.6% (38/124) of patients at 5 years (Figure 3). A Life-table survival analysis was used to determine the Kaplan-Meier estimators (Figure 4). Freedom from AND at 5 years after EVAR was estimated on an intention-to-treat basis at 49.5% (95% confidence interval [CI]: 38.1–58.3) for AND ≥2.5 mm and at 71.8% (95% CI: 60.5–80.8) for AND ≥5 mm. The median device diameter of the implanted endografts was 28 mm (24–36), thus oversizing at the D3 level of the PAN was calculated at 20.7±2.8%. Increased diameter of PAN at 5 years correlated with endograft oversizing at implantation (r=0.68, p<0.001); ie, patients with greater oversizing experienced more frequent and greater AND. Aortic neck dilatation did not exceed the device nominal diameter in 81.3% of the cases. The multivariate analysis showed that only the degree of oversizing, the preoperative neck diameter, and the preoperative AAA sac diameter served as independent predictors of AND at 5 years (odds ratio [OR]=2.67, 95% CI: 1.38–7.45, p=0.013; OR=2.19, 95% CI: 1.50–7.14, p=0.026; and OR=1.68, 95% CI: 1.12–6.06, p=0.037, respectively). The preoperative length of PAN was awarded with an OR=1.47 but was not statistically significant (p=0.097).
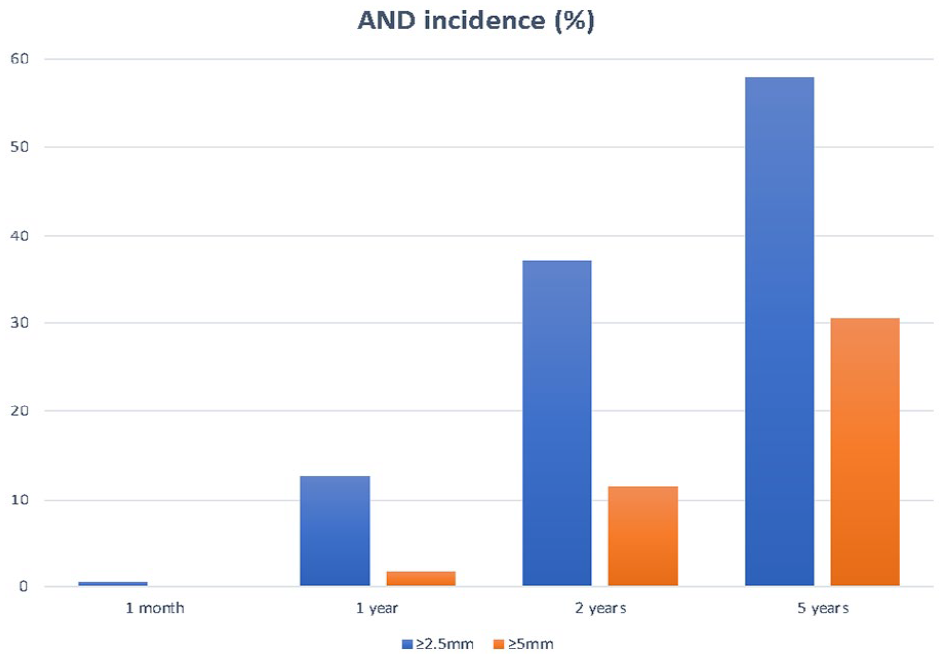
Proximal aortic neck dilatation (AND) incidence during follow-up. Differentiation was applied depending on the degree of AND (mm).
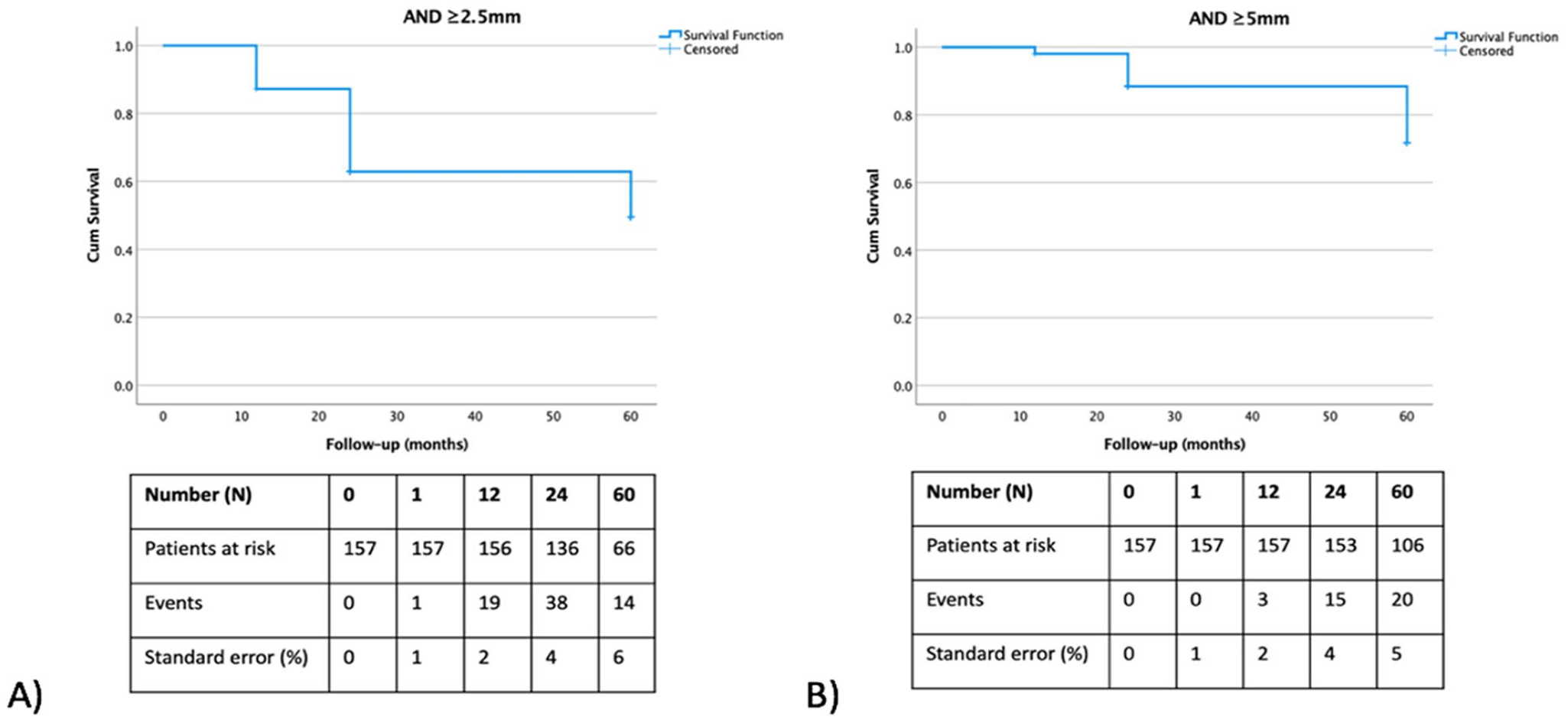
Kaplan-Meier estimators for (A) freedom from aortic neck dilatation (AND) ≥2.5 mm and (B) freedom from AND ≥5 mm, during follow-up. Freedom from AND on an intention-to-treat basis was estimated at 49.5% for AND ≥2.5 mm and at 71.8% for AND ≥5 mm.
Aneurysm sac regression was significant during the 5-year follow-up. The median sac diameter decreased from 58.8 mm (50.2–107.7) preoperatively to 48.9 mm (29.8–70.7) at 5 years (p=0.006). As such, sac regression ≥5 mm was evident in 61.3% at 5 years after EVAR and was considered important (≥10 mm) in 32.3% of patients at 5 years. The mean regression rate was 0.17 mm/month overall and was significantly higher during the first 2 years than that in the next 3 years (0.23 mm/month vs 0.12 mm/month, p=0.03). A higher preoperative sac diameter was related with significantly slighter sac regression (r=0.51, p=0.040).
Clinical Impact of Proximal Aortic Remodeling
In 7 patients (5.6%), a caudal stent-graft migration ≥10 mm was discovered at 5 years. Four (57.1%) of them were accompanied by loss of proximal sealing zone and a type Ia endoleak, whereas the remaining 3 (42.9%) were accompanied by subclinical proximal sealing zone shortening but without sac expansion or a type Ia endoleak. A strong correlation was found between the proximal sealing zone shortening and the distance of migration (r=0.76, p<0.001). The incidence of important AND was significantly higher in patients with clinical migration (5/7 or 71.4% vs 2/7 or 28.6%, p=0.002) with a strong relationship between the amount of proximal neck enlargement and the distance of migration (r=0.64, p=0.012). On average, endografts moved a mean of 6.8±2.8 mm caudally in those with AND ≥2.5 mm, compared to 3.9±2.3 mm in those with PAN dilatation <2.5 mm (p=0.019). Multivariate logistic regression showed that the length of the proximal sealing zone (OR=3.16, 95% CI: 1.79–6.48, p=0.014), the use of stent-graft devices with infrarenal fixation (OR=3.02, 95% CI: 1.68–6.05, p=0.012), the AND (OR=2.75, 95% CI: 1.44–7.02, p=0.023), and the degree of oversizing (OR=2.16, 95% CI: 1.12–5.68, p=0.034) served as independent predictors for caudal stent-graft migration.
A total of 8 late type Ia endoleaks (6.5%) were discovered at 5 years; 4 cases with simultaneous migration (mentioned above) and 4 others without clinical migration. A significant correlation was found between the proximal sealing zone shortening and the presence of endoleak (p=0.010). The incidence of important AND was significantly higher in patients with a late type Ia endoleak (5/8 or 62.5% vs 3/8 or 37.5%, p=0.015), which was size-dependent; meaning patients with greater neck dilatation had more possibilities of experiencing a type Ia endoleak (OR: 1.46, 95% CI: 1.19–4.12, p=0.042). Multivariate logistic regression showed that the length of the proximal sealing zone (OR=2.76, 95% CI: 1.48–5.66, p=0.032), the use of stent-graft devices with infrarenal fixation (OR=2.53, 95% CI: 1.31–5.15, p=0.040), and the AND (OR=2.32, 95% CI: 1.17–4.96, p=0.044) served as independent predictors for late type Ia endoleaks. The degree of oversizing was found to act as a protective factor but was barely significant (OR=0.69, 95% CI: 0.12–1.13, p=0.052).
No correlation was found between AND and sac regression (p=0.098), nor between PAN’s baseline characteristics and sac regression (p>0.050 for every parameter). The presence of a type Ia endoleak negatively affected the degree of sac regression and was statistically important (p=0.033), in contrast to endograft migration (p=0.139). No late ruptures were observed in our study. All patients with a type Ia endoleak or migration ≥10 mm (n=11 overall, 8.9%) were treated with proximal aortic cuff placement. A multivariate analysis on the risk of late reintervention showed that the presence of important AND at 5 years significantly increased the relative risk by 2.17 (hazard ratio=2.17, CI: 1.43–5.10, p=0.026).
Subgroup Analysis
A subgroup analysis was performed between the 6 abdominal aortic bifurcated self-expanding stent-graft devices used in our study (Table 6). No differences were observed regarding the patients’ demographics and baseline characteristics. Even though the PAN expanded in our series averagely about the same amount with each implanted device (p=0.056), we found a marginally significant difference regarding the incidence of important AND at 5 years. In particular, Ovation was found to be less prone to significant neck dilatation (p=0.049). Devices were then grouped together based on their fixation. The infrarenal fixation group consisted of the Anaconda device, whereas the remaining 5 devices formed the suprarenal fixation group. No statistically significant differences were observed between the 2 groups regarding the incidence and the extent of AND in the long term (31.3% vs 30.6%, p=0.106, and 3.5±1.8 mm vs 3.9±2.0 mm, p=0.061, respectively).
Clinical Outcomes of the Various Endograft Devices at 5 Years of Follow-up.
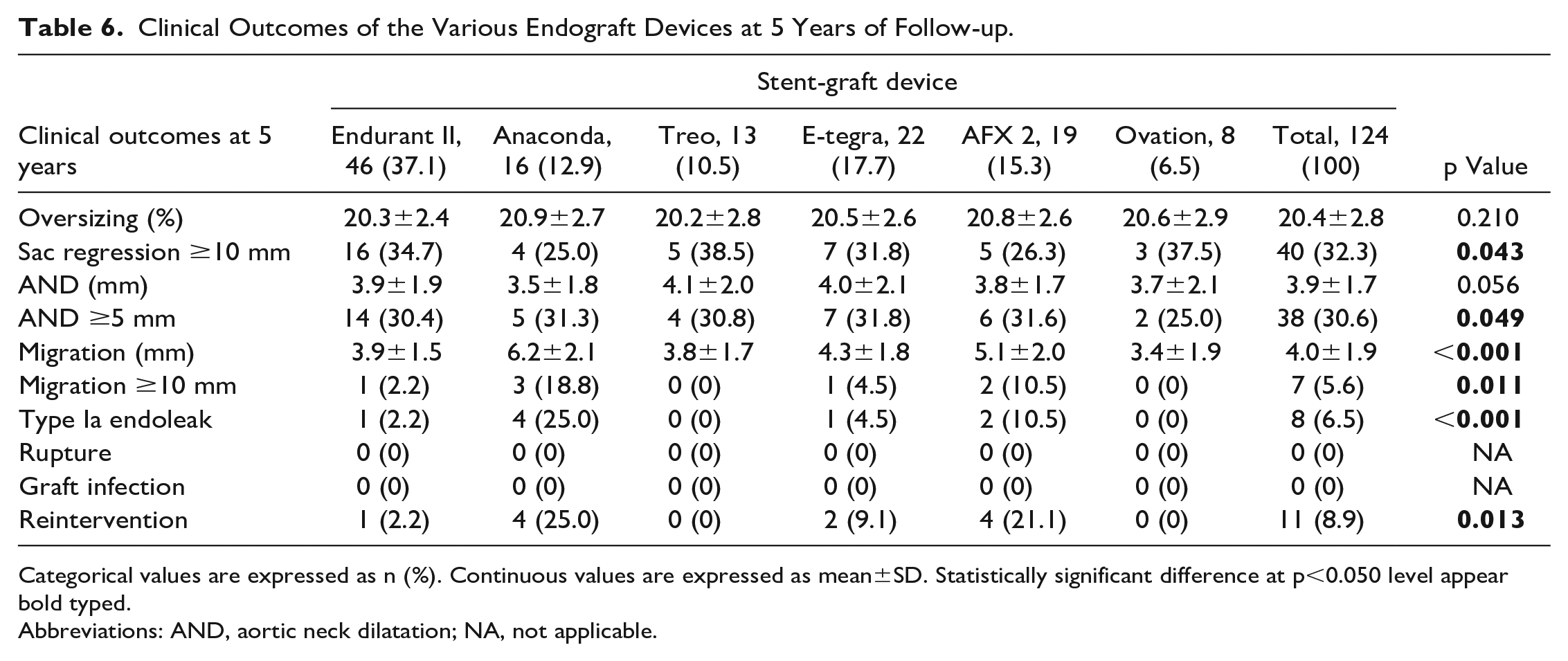
Categorical values are expressed as n (%). Continuous values are expressed as mean±SD. Statistically significant difference at p<0.050 level appear bold typed.
Abbreviations: AND, aortic neck dilatation; NA, not applicable.
Significant differences in the clinical outcomes were discovered between the individual devices at the 5-year follow-up. Important sac regression was more prominent with the Treo device, contrary to the Anaconda and AFX 2 devices (p=0.043). Caudal migration of the stent-graft ≥10 mm was far more frequent with Anaconda (p=0.011), accounting for 42.9% of the total migration cases, followed by AFX 2. On the other hand, Ovation seemed to be the less prone to significant migration, followed by Treo. Four of 8 or 50% of the total cases of late type Ia endoleaks in our series were attributed to Anaconda (p<0.001). Finally, the Anaconda and AFX 2 devices each accounted for 36.4% of the total cases of late reintervention and were the stent-grafts significantly associated with higher frequency of redo endovascular procedures (p=0.013).
Discussion
Endovascular repair of infrarenal abdominal aortic is currently considered the preferred treatment even for cases with complex AAAs.22–25 Continuous morphological changes of the abdominal aortic wall have been reported over time after EVAR, and this remodeling phenomenon contributes to proximal aortic neck failure, as it can lead to proximal sealing zone destabilization and serious long-term adverse events.26–28
Remodeling of PAN refers to changes in its diameter, length, and angulation, consequently altering its shape and its relation to the suprarenal aortic segment and the aneurysm sac.26,27 Ishibashi et al 29 described the straightening of the suprarenal aorta and the PAN and suggested that it occurs almost immediately after the deployment of the endograft, with an abrupt decrease in angulation during the first year, which continues over the following years at a much smaller rate. In our series, significant straightening of the PAN was evident even in the first-month CTA, reaching an average decrease in suprarenal and infrarenal angulation of 10.1±4.3° and 21.5±10.2°, respectively, at the end of the 5-year follow-up. Moreover, we found that patients with greater preoperative PAN angulation at any level experienced greater straightening postoperatively. However, no correlation was found between PAN’s straightening and sac regression in our series, in contrast to previous findings from Lee et al. 30
Postoperative length changes of the PAN are less clarified in literature. 31 Litwinski et al 20 in a large study applied a differentiation based on the presence of stent-graft migration. Patients with endograft slippage and true migration were accompanied by shortening of the PAN and loss of the proximal sealing zone. On the other hand, patients without migration experienced elongation of the PAN that created the radiographic perception of migration, without necessarily causing loss of the proximal fixation zone. 20 In our series, we witnessed a shortening of the PAN in almost all cases, which evolved slowly over the years and became significant only at 5 years. At the same time, the proximal sealing zone length was reduced by 3.0±1.2 mm. We also found that patients with a shorter proximal sealing zone length at the first month experienced greater reduction in sealing zone length, accompanied by greater caudal migration of the stent-graft. These findings are in accordance with previous studies.32,33 The degree of PAN’s shortening was marginally correlated with straightening at the infrarenal level. Finally, no correlation was found between PAN’s shortening and its preoperative length, nor with sac regression, in contrast to findings by Matsumura and Chaikof. 32
Proximal AND is the most important feature in the process of long-term PAN remodeling.27–29 Various definitions have been proposed over the years trying to quantify this increase and set a threshold over which AND is considered to be present.15,16 However, up to date, a universally accepted definition does not exist. Most authors set the threshold at 2.5-mm increase in PAN’s diameter.9,12,34–36 According to the Society for Vascular Surgery, AND is considered important when a ≥5-mm increase is noted. 1 Previous studies have reported an AND incidence ranging between 10% and 36% and reaching up to 62.9%.7–9,12,13,21,34–44 A meta-analysis by Chatzelas et al 45 reported a cumulative incidence of 22.9% during follow-up. In our series, AND ≥2.5 mm was evident in 12.7% of patients at 1 year, 37.2% at 2 years, and 58.1% at 5 years after EVAR and was considered important (≥5 mm) in 11.5% of patients at 2 years and 30.6% of patients at 5 years. Defining AND properly requires reporting the exact level of the diameter measurement. 45 In most previous studies, ≤3 infrarenal levels were used for measurement of the PAN. 45 In our study, we measured the diameter of the suprarenal segment at 2 levels (suprarenal and interrenal) and PAN’s diameter at 4 clearly defined levels (1 juxtarenal and 3 infrarenal). Due to this profound and detailed analysis, we consider that our reported high AND incidence is accurate and reliable.
Aortic neck dilatation is a continuous process that starts almost immediately after the implantation of the stent-graft and continues consistently over the years. 27 It remains unclear if this phenomenon is caused by the continuing degenerative aneurysm disease process or is the result of the self-expanding stent-graft’s radial force and the effort of adapting to the new hemodynamic conditions established after its implantation.27,28 Oberhuber et al 11 found similar late neck dilatation between EVAR and open repair, which supports the theory of the continuous progression of the aneurysmatic disease. On the other hand, the majority of studies agree that AND does not significantly exceed the nominal stent-graft diameter and, therefore, could be related to the presence of the endograft.41–44 Indeed, in our study, AND did not exceed the device's nominal diameter in 81.3% of the cases.
Evidence in literature supports the hypothesis that AND evolves in 2 phases: an immediate postimplantation one, which is strongly associated with the percentage of endograft’s oversizing, and a subsequent one, which is possibly associated with disease progression and stent-graft migration.10,13,38 The rate of neck dilatation has been reported to be greater in the early postoperative period rather than in the late follow-up.5,46,47 In our study and in accordance to Kaladji et al, 41 the PAN dilated significantly and homogenously at all levels and not just immediately below the RAs. Moreover, using a broad spectrum of contemporary SESGs, we found that PAN’s dilatation rate was significantly higher during the first 2 years than that in the next 3 years and that higher preoperative diameter values at any level were correlated with greater dilatation at 5 years. At the same time, no significant correlations between PAN’s angulation or length and its diameter change were reached. Hostile neck has been also associated with greater PAN dilatation.17,48 However, those cases were excluded from our analysis because we consider that hostile neck represents a unique anatomical and clinical situation and that it is different from usual and conventional EVAR cases and should be explored individually, in order to avoid false generalization of conclusions.
The effect of endograft oversizing on AND has also been investigated in many studies, but with contradictory results.5,12,38,41,44 Theoretically, greater expanding radial force in cases with aggressive oversizing (>25%) leads to increased wall stress at the level of the PAN, which in turn accelerates its dilatation.27,31 In our study, a strong correlation was found between AND at 5 years and the degree of endograft oversizing at implantation. Thus, patients with greater oversizing experienced AND more frequently and at a greater level. Our results are consistent with the study by Torsello et al, 49 who divided the patients into groups based on the degree of oversizing and found that the mean diameter increase was significantly more prominent as the degree of oversizing rose from <10% to >30%. In our multivariate analysis, we found that the degree of oversizing and the preoperative neck and sac diameter were independent factors of AND at 5 years. Considering that the PAN and AAA sac diameters reflect the clinical aggressiveness of the aneurysmatic disease, the natural degenerative history of AAA may contribute to the etiology of long-term AND, while the impact of stent-graft’s oversizing is greater but not limited to the early follow-up period.
Studies comparing the effect of different stent-graft devices on AND failed to prove any significant correlation.36,38,40,44 A common assumption was that suprarenal fixation would accelerate the dilatation of the suprarenal segment.27,28 In our study, 6 contemporary abdominal aortic bifurcated self-expanding stent-graft devices were used, and our subgroup analysis showed that patients treated with each device experienced roughly the same amount of neck dilatation and that no significant differences were observed between individual devices nor between fixation types. This suggests that AND occurs nearly universally after EVAR over a time interval of 5 years, regardless of the device type, the device-specific characteristics, or the fixation mechanism and confirmed the data reported by Deltomme et al. 50 However, in the subgroup analysis, significant differences in the clinical outcomes between the individual devices at the 5-year follow-up were evident. The infrarenal fixation Anaconda device, even though it experienced the same long-term AND, resulted in greater caudal stent-graft migration and higher incidence of late type Ia endoleaks, accounting for 42.9% of the migration cases and 50% of the type Ia endoleaks, than the suprarenal fixation devices. Moreover, 36.4% of the total number of secondary operations pertained to the Anaconda device. These results are consistent with earlier studies that have reported a higher adverse event rate with older infrarenal fixation endograft devices. 40 However, more recent studies have shown equally successful and durable long-term results between newer-generation suprarenal and infrarenal fixation endograft devices, such as the Excluder device (Gore, Phoenix, Arizona). 51
The clinical impact of AND has also been controversial. A higher adverse event rate as well as a higher reintervention rate during follow-up in patients with AND were evident in most studies, even after many years.16,45 In our study, the incidence of migration and type Ia endoleaks was 5.6% and 6.5% at 5 years, respectively. Both were strongly associated with the presence of AND, with the correlation being size-dependent; meaning patients with greater neck dilatation had more possibilities of migration or a type Ia endoleak. The degree of oversizing was found to act as a protective factor against type Ia endoleaks but was barely significant. Moreover, the presence of important AND at 5 years significantly increased the relative risk of late reintervention by 2.17. Finally, no late ruptures were observed in our study probably because of the early detection and treatment of AND-related EVAR failures, which highlights the value of our CTA follow-up protocol.
Limitations
The main limitation of our study is the lack of randomization in endograft selection, possibly resulting in selection bias. The decision of which endograft was to be implanted in each case was purely clinical, based on the anatomical features of the aneurysm as well as the stent-graft availability at that time. However, we report on a consecutive series of conventional EVAR cases with a strict and long-term follow-up protocol, and we consider that our results largely reflect the everyday clinical praxis. The number of included patients in each endograft subgroup was relatively small to draw definite and robust conclusions about the long-term performance of the various devices, but it was sufficient enough to reach some important and statistically significant results. Larger, multicenter, randomized trials are needed to evaluate the progressive remodeling of the PAN, its clinical impact on long-term durability of EVAR, and its association with baseline anatomical characteristics.
Conclusions
Remodeling of the PAN is a universal phenomenon and a continuous process, evident in all patients after EVAR. It starts immediately after the implantation of the endograft, develops at 2 phases, with a higher dilatation rate during the first 2 years, and is driven by the stent-graft’s expanding force in association with the continuous progression of the aneurysmatic disease. Long-term AND is the most important feature that affects a considerable proportion of patients. It is significantly related to worse clinical outcomes, as indicated by the increased rates of late type Ia endoleaks, caudal stent-graft migration, and reintervention, even though the overall incidence of late adverse events after EVAR was low. Baseline anatomical characteristics of the PAN as well as the degree of oversizing seem to play the primordial role in the progression of AND. Finally, a systemic, strict, and extended surveillance protocol is needed for maintenance of good long-term results of EVAR.
Supplemental Material
sj-tif-1-jet-10.1177_15266028231167998 – Supplemental material for Long-term Evaluation of Proximal Aortic Neck Dilatation After Endovascular Abdominal Aortic Aneurysm Repair With a Variety of Contemporary Endografts
Supplemental material, sj-tif-1-jet-10.1177_15266028231167998 for Long-term Evaluation of Proximal Aortic Neck Dilatation After Endovascular Abdominal Aortic Aneurysm Repair With a Variety of Contemporary Endografts by Dimitrios A. Chatzelas, Apostolos G. Pitoulias, Charalampos N. Loutradis, Theodosia N. Zampaka, Christos D. Karkos, Dimitrios C. Christopoulos and Georgios A. Pitoulias in Journal of Endovascular Therapy
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Approval was obtained from the Bioethics Committee of Faculty of Medicine, Aristotle University of Thessaloniki.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.