
Abstract
Objective:
To report demographics and clinical, laboratory, and imaging features of acute renal infarction (ARI) due to symptomatic isolated spontaneous renal artery dissection (SISRAD) and to analyze outcomes after the initial therapy for SISRAD.
Methods:
Thirteen patients with ARI due to SISRAD between January 2016 and March 2021 were enrolled in this retrospective study. We reviewed the demographics, clinical, laboratory, and imaging features (location of the infarct kidney, the branch artery involved by dissection, true lumen stenosis, false lumen thrombosis, and aneurysm), treatment modalities, and follow-up results; analyzed the difference between SISRAD and other causes of ARI; and propose an appropriate therapy strategy for SISRAD based on our data and literature.
Result:
Patients with ARI due to SISRAD were mostly young men (43 [24–53] years; 12/13 [92%]). No patients had atrial fibrillation or acute kidney injury at admission (0/13). All 13 patients received conservative treatment as the initial treatment. Sixty-two percent (8/13) of patients progressed, and 88% (7/8) of them had dissection aneurysm on the admission computed tomographic angiography (CTA) image. Seventy-five percent (6/8) of patients underwent endovascular intervention as follows, stent placement in 1 patient, renal artery embolization in 1, and stent placement with embolization in 4. Two patients with disease progression died: 1 during the conservative treatment period and 1 after the stent placement. Thirty-eight percent (5/13) of patients in remission continued to receive conservative treatment, none of whom had dissection aneurysm on the admission CTA.
Conclusion:
Symptomatic isolated spontaneous renal artery dissection is a rare and fatal disease. For young ARI patients with no previous history of tumors and cardiogenic diseases, CTA examination is recommended to exclude SISRAD. Dissection aneurysm seems to be a risk of progression for SISRAD in this series. Conservative treatment, a recognized initial treatment, has a good effect on patients without dissection aneurysm, and we recommend endovascular intervention as the initial treatment for the patient with dissection aneurysm at admission. Multicenter clinical studies are needed to explore a more-appropriate treatment for patients with SISRAD.
Clinical Impact
This article report the related factors, risks, demographics and laboratory data of Acute renal infarction (ARI) due to Symptomatic isolated spontaneous renal artery dissection (SISRAD) and explore a better initial therapy strategy for SISRAD. It will help improve the effectiveness of SISRAD treatment and reduce the mortality rate from this rare but lethal disease.
Introduction
Acute renal infarction (ARI) is a clinical condition caused by renal artery occlusion. Patients often present with a sudden onset of abdominal pain initially. The most common cause of ARI is cardiogenic thromboembolism. 1 However, few cases were reported in which ARI is caused by symptomatic isolated spontaneous renal artery dissection (SISRAD). Symptomatic isolated spontaneous renal artery dissection is a rare disease and limited to case reports since the first case was reported in 1944. 2 It has the potential to progress and may cause fatal complications. There is no consensus on the best treatment for SISRAD, and the management strategy has not yet been established. The current researches generally regard conservative treatment as the first choice for initial treatment.3–6 However, more and more experts suggested positive interventions including endovascular therapy and open surgery for SISRAD, as the prognosis of conservative treatment is highly variable.2,5 In this retrospective study, we aimed to discuss the demographics; clinical, laboratory, and imaging features; treatment plan; and prognosis of patients who were diagnosed with ARI due to SISRAD.
Methods
Study Population
This single-center, retrospective study included 13 consecutive patients with SISRAD in our department between January 2016 and March 2021. All the patients presented with an acute-onset pain including abdominal pain, flank pain, or back pain. Patients present with ARI due to other causes (n=55), including 37 patients with atrial fibrillation, 5 patients with infective endocarditis, 4 patients with aortic thrombosis, and 9 patients with an unknown cause. Among the 9 patients, 4 patients underwent relevant examinations but excluded diseases such as atrial fibrillation, infective endocarditis, or aortic thrombosis, and 5 patients refused to undergo relevant examinations. Patients with concomitant aortic dissection or other visceral artery dissections (n=7) were excluded (Figure 1). We retrospectively reviewed the clinical features, risk factors, computed tomographic angiography (CTA) images, treatment modalities, follow-up results, and prognosis of the 13 patients.
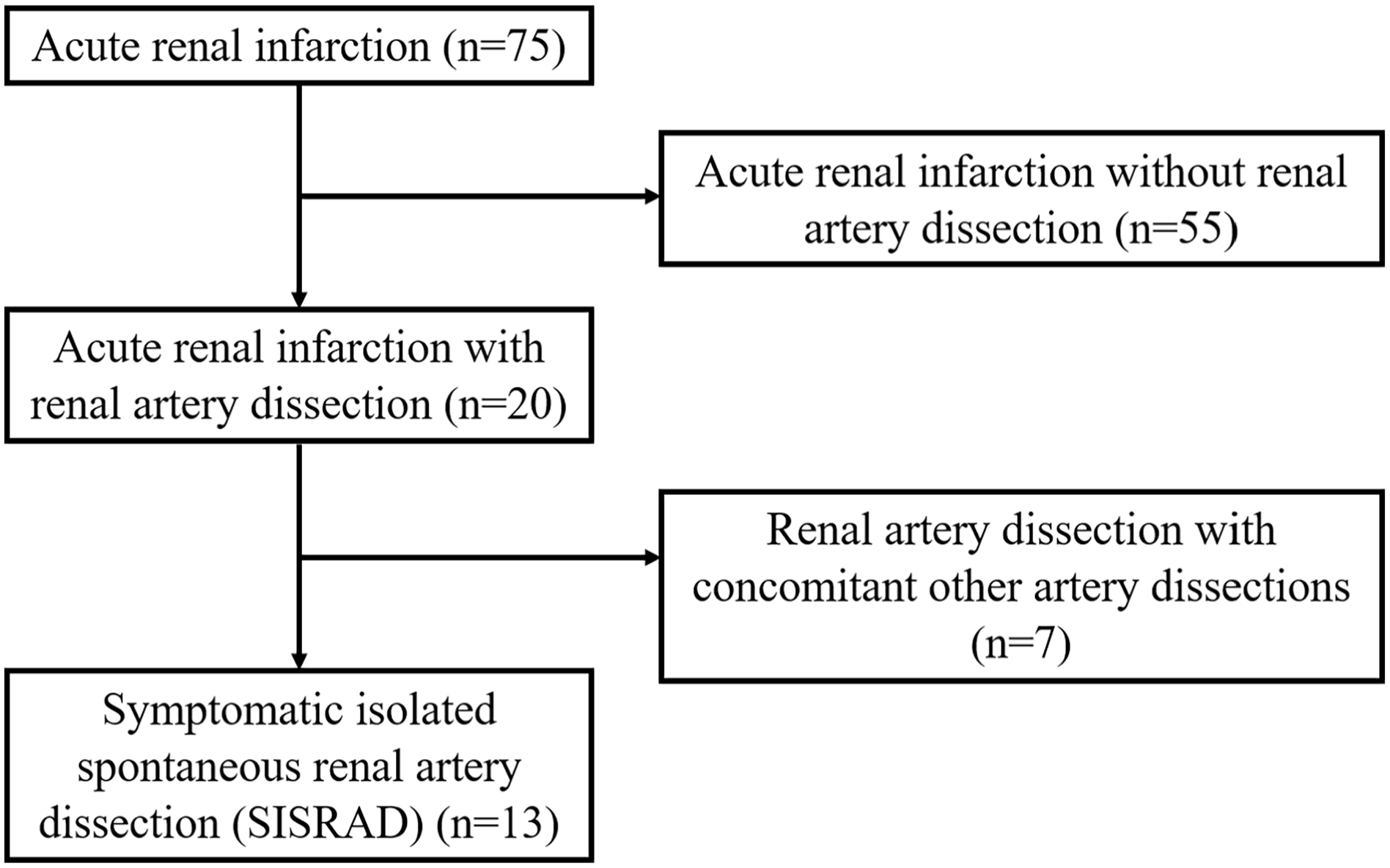
Flow chart of patient inclusion.
Diagnostic Workup
The diagnosis of SISRAD was made according to spiral CTA findings. Imaging characteristics such as the location of the infarct kidney, the branch artery involved by dissection, true lumen stenosis, false lumen thrombosis, and aneurysm were analyzed from the initial CTA findings. Aneurysm was defined as dilatation or widening of the artery at least 1.5-times larger than the normal arterial diameter. True lumen stenosis was defined as narrowing of the arterial diameter (≥50%) compared with the normal diameter.
Treatment Options
All the 13 patients with SISRAD included in the study received conservative treatment initially. Conservative treatment included strict blood pressure control (target systolic blood pressure<140 and diastolic blood pressure<90 mm Hg), pain management, bowel rest, and parenteral nutritional support with anticoagulation for patients with vomiting. Low-molecular-weight heparin was injected at a dose of 815 U/kg every 12 hours after excluding the high risk of bleeding. Patients were divided into a stable SISRAD group and a progressive SISRAD group based on their prognosis. The stable SISRAD group included patients with remission or disappearance of symptoms and no progress in follow-up CTA while under conservative treatment. Patients with the following characteristics were included in the progressive SISRAD group: (1) symptoms unimproved (aggravated pain or persistent pain unrelieved after conservative treatment), (2) recurrence of symptoms, and (3) follow-up CTA suggested aggravated dissection (the enlargement of dissection, narrowing of true lumen, and enlarging of false lumen). The endovascular intervention included stent placement (Pulsar-18; Biotronik AG, Bulach, Switzerland, Neuroform EZ; Stryker, Kalamazoo, Michigan) in the true lumen with or without coil embolization of the false lumen aneurysm in the dissected renal artery and coil embolization (Axium; Medtronic, Irvine, CA, Interlock; Boston Scientific, Cork, Ireland) of the dissected artery. Patients undergoing endovascular stenting received antiplatelet drugs for 6 months postoperatively.
Statistical Analysis
Categorical variables are reported as frequencies and percentage, and continuous variables as mean and standard deviation(presenting a normal distribution) or median and range(not presenting a normal distribution). A statistical analysis was conducted using Fisher exact test and independent-samples t test with the SPSS software (23.0 v; SPSS Inc, Chicago, Illinois). Statistical significance was determined with p values <.05.
Results
The study involved 12 men and 1 woman with ages ranging from 24 to 53 years (median age 43 years). All the patients suffered from acute pain, including 8 patients with abdominal pain, 3 patients with flank pain, 1 patient with abdominal and flank pain, and 1 patient with flank and back pain. The demographics of the patients are shown in Table 1. Hypertension was detected in 1 of 13 (8%) patients, and hyperlipidemia in 1 of 13 (8%) patients. None of the patients were diagnosed with Marfan syndrome, Ehlers-Danlos syndrome, neurofibromatosis, or Takayasu arteritis. They denied vasculitis-related skin lesions before and on admission and were all negative for vasculitis-related markers such as Anti-neutrophil cytoplasmic antibody (ANCA) and Circulating endothelial cells (CEC). Three patients had microhematuria and microalbuminuria, and 1 patient only had microhematuria. The mean serum creatinine and serum lactate dehydrogenase levels were 97.1 mg/dL and 563.8 U/L, respectively. None of patients had acute kidney injury (AKI). During conservative treatment, 8 patients had progressed, and 5 patients were stable. The patients in the progressive SISRAD group were younger than those in the stable SISRAD group (39 vs 48, p=0.04).
Demographics and Laboratory Data of Patients With SISRAD.
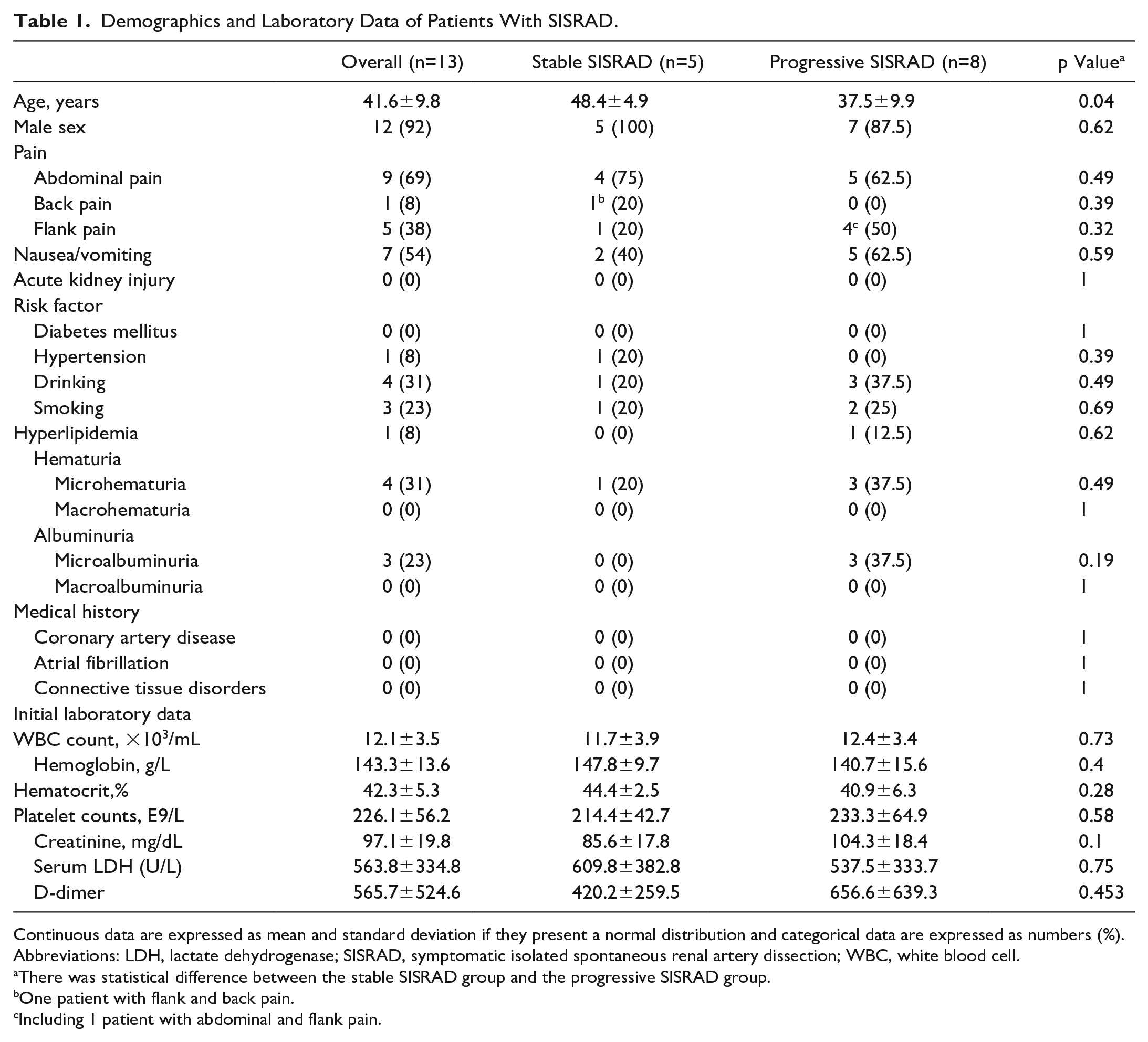
Continuous data are expressed as mean and standard deviation if they present a normal distribution and categorical data are expressed as numbers (%).
Abbreviations: LDH, lactate dehydrogenase; SISRAD, symptomatic isolated spontaneous renal artery dissection; WBC, white blood cell.
There was statistical difference between the stable SISRAD group and the progressive SISRAD group.
One patient with flank and back pain.
Including 1 patient with abdominal and flank pain.
According to the initial CTA findings (shown in Table 2), 9 of 13 (69%) patients had left renal infarction, and 4 of 13 (31%) patients had right renal infarction. All patients showed true lumen stenosis and involvement of the main and branch renal arteries. Twelve of 13 (92%) patients had false lumen partial thrombosis, and 7 of 13 (54%) patients had aneurysm. The progressive SISRAD group more frequently had dissection aneurysm than the stable SISRAD group (87.5% vs 0%, p=0.005).
Computed Tomography Angiography Appearances of Patients With SISRAD.
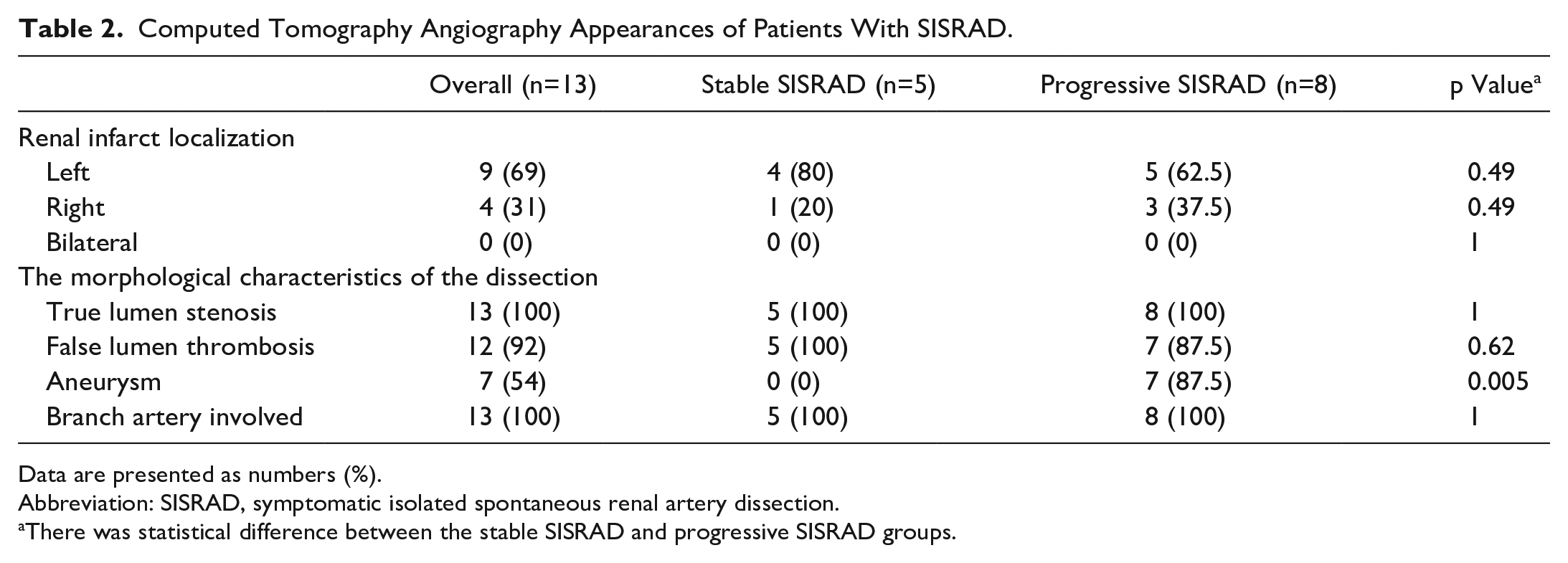
Data are presented as numbers (%).
Abbreviation: SISRAD, symptomatic isolated spontaneous renal artery dissection.
There was statistical difference between the stable SISRAD and progressive SISRAD groups.
Follow-up involved an assessment of symptoms and computed tomography scan at 1 month, 6 months, and yearly thereafter. The median time of follow-up was 16 months, with a range of 8 to 42 months. Eight patients had progressed as follows (shown in Table 3): 5 patients with persistent pain unrelieved by conservative treatment, 1 patient dying of a sudden ruptured dissection aneurysm and failing in rescue (Figure 2A and B), and 2 patients showing the dissection deterioration at 1-month follow-up CTA findings. The 5 patients with persistent pain underwent endovascular intervention, including stent placement in 1 patient, renal artery embolization in 1, and stent placement with embolization in 3. One patient died 2 days after isolated stent placement, which was suspicious of dissection rupture (Figure 2C and D), and other patients showed good prognosis postoperatively. One of the patients with progressive follow-up CTA refused intervention, and the other one underwent stent placement with embolization (Figure 3). All patients were free of chronic renal failure, hypertension, and connective tissue disease during the follow-up period, except for 1 patient with pre-existing hypertension (Table 4). Patients with previous symptoms of microhematuria and albuminuria returned to normal. One patient receiving stent placement combined with false lumen coil embolization showed primary renal artery dissection improvement on CTA at 1 and 3 months postoperatively. However, he developed new-onset dissection of the contralateral renal artery without renal infarction and did not feel any pain at 3 months after surgery. Therefore, he received conservative treatment for the contralateral renal artery dissection, and the dissection was stable at 22 months after surgery. No patients developed new aneurysms. The 5 stable patients continue to receive conservative treatment and achieved good results. Overall, conservative treatment yielded a 38% (5/13) success rate.
Disease Progression of SISRAD.
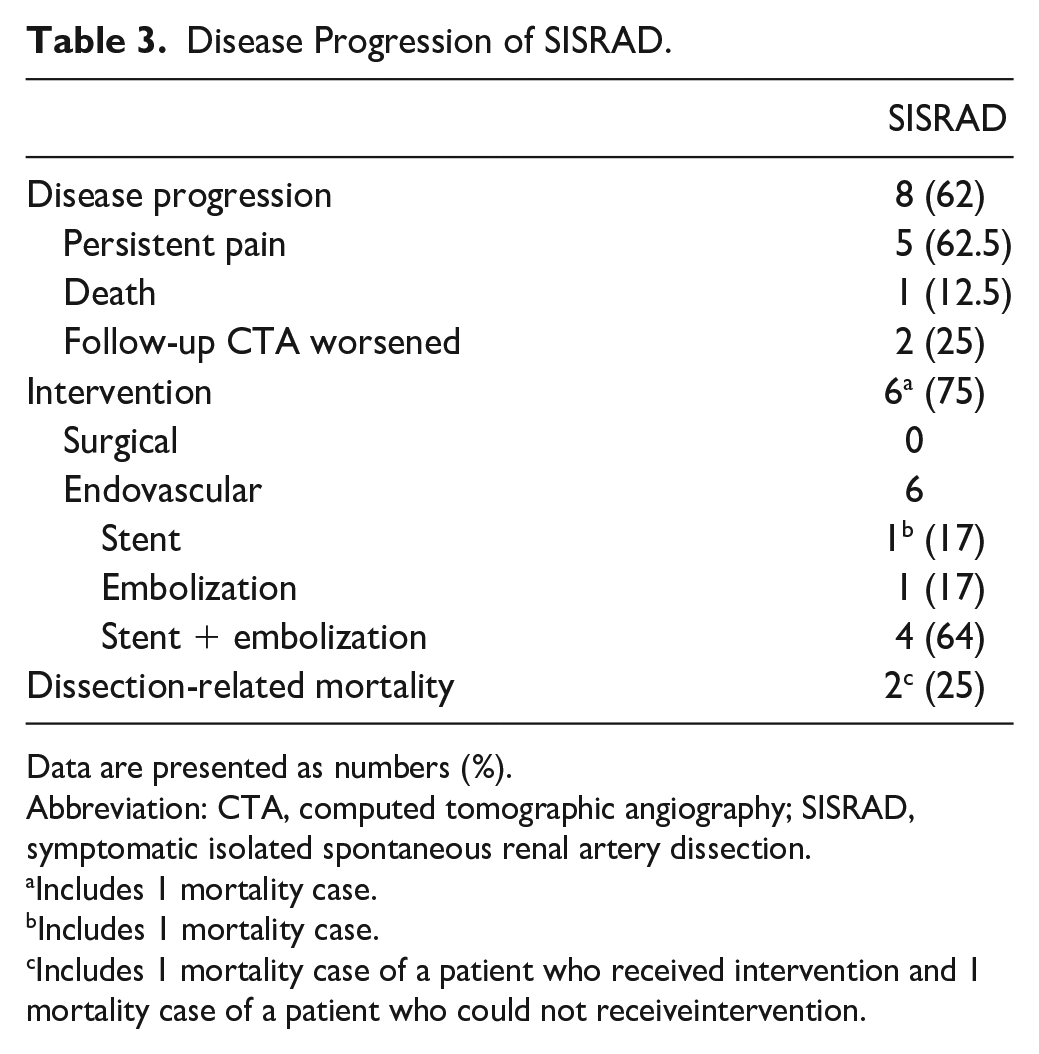
Data are presented as numbers (%).
Abbreviation: CTA, computed tomographic angiography; SISRAD, symptomatic isolated spontaneous renal artery dissection.
Includes 1 mortality case.
Includes 1 mortality case.
Includes 1 mortality case of a patient who received intervention and 1 mortality case of a patient who could not receiveintervention.
Follow-up Profile of Patients With SISRAD.
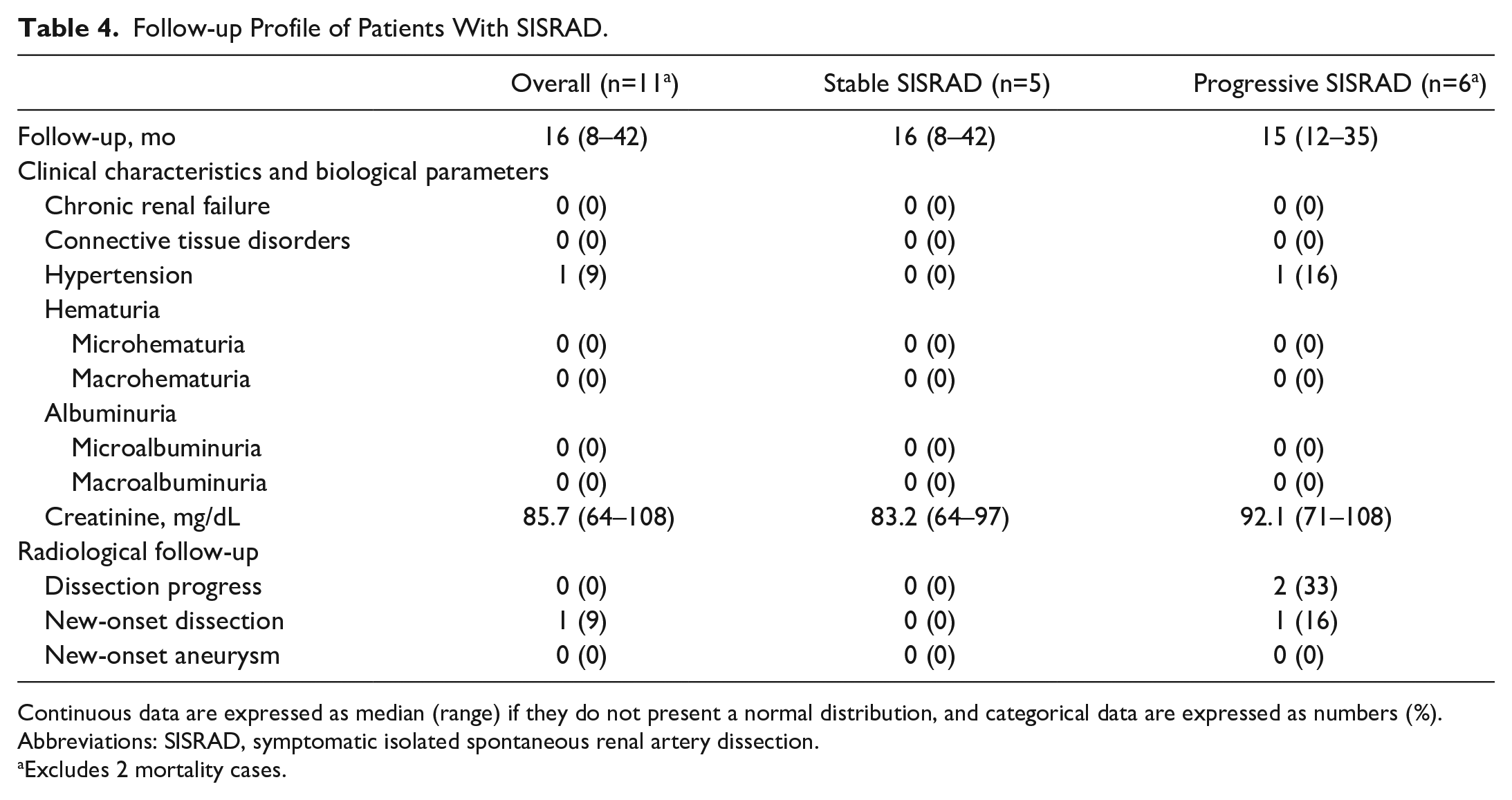
Continuous data are expressed as median (range) if they do not present a normal distribution, and categorical data are expressed as numbers (%).
Abbreviations: SISRAD, symptomatic isolated spontaneous renal artery dissection.
Excludes 2 mortality cases.
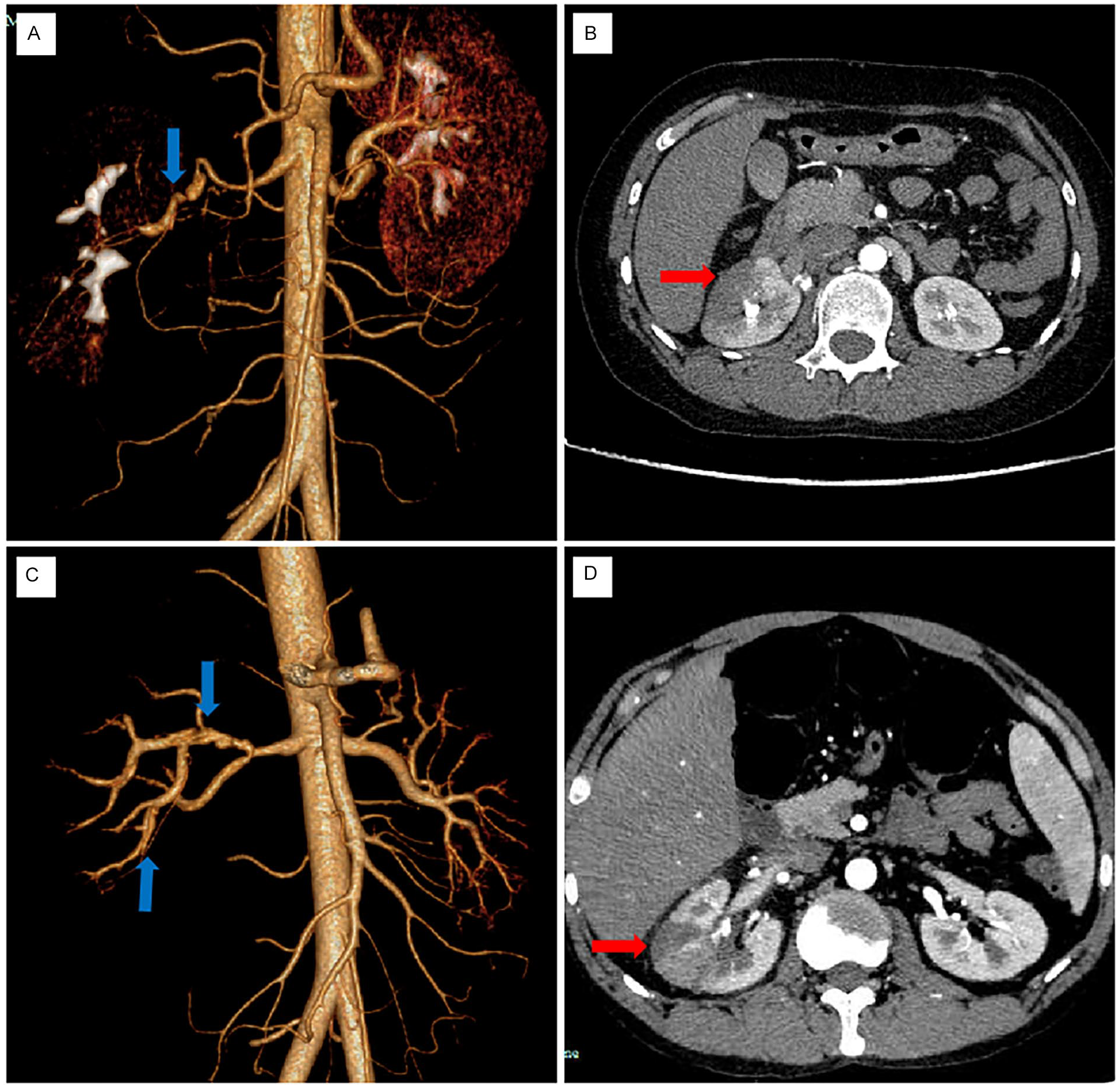
Two mortality cases resulting from rupture of dissection aneurysm, including a 32-year-old woman with conservative treatment (A and B) and a 35-year-old man with stent placement (C and D). Their CTA findings at admission indicated the presence of dissection aneurysm on the right renal artery. The blue arrows represent renal artery dissection, and the red arrows represent the renal infarct area. CTA, computed tomographic angiography.
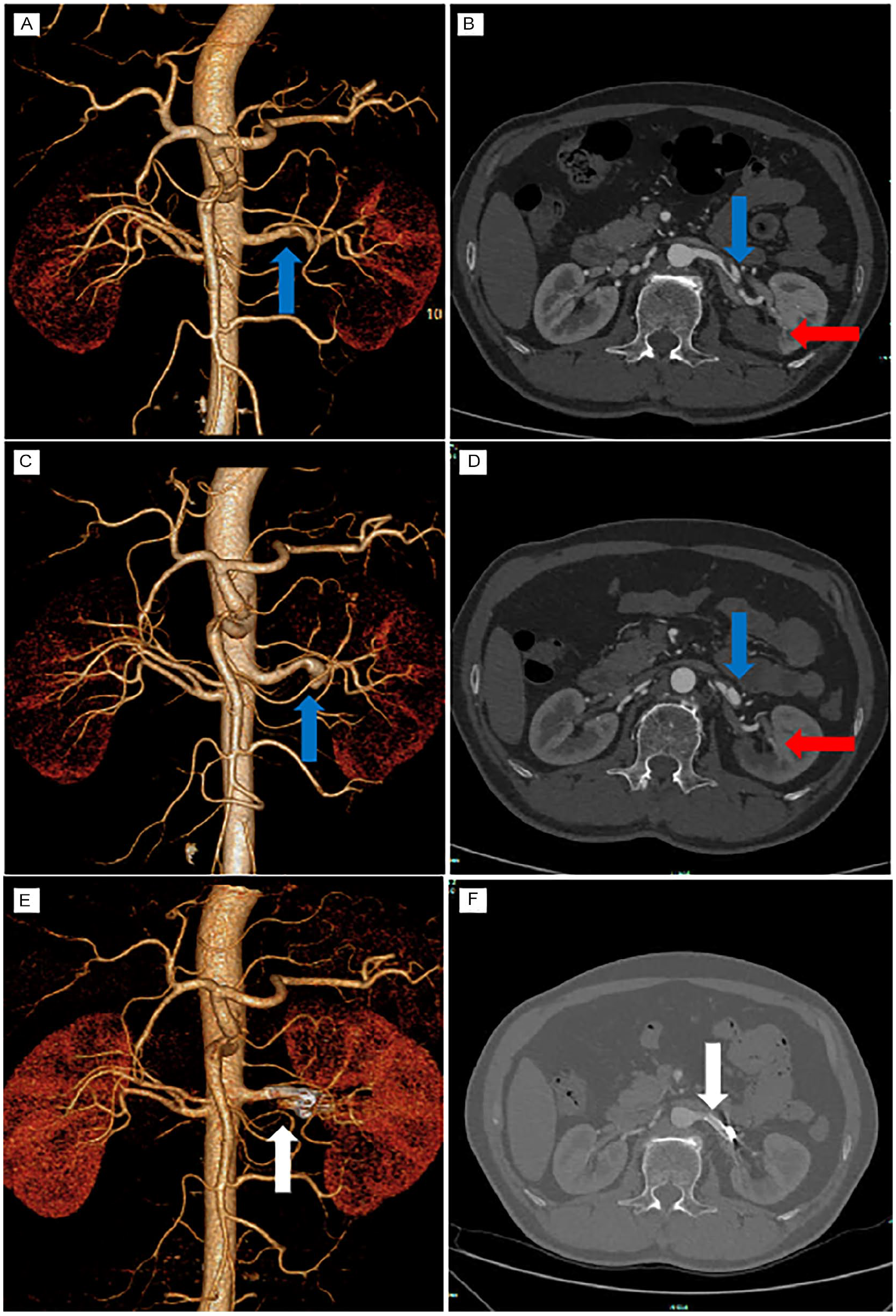
A 53-year-old man with dissection aneurysm on the left renal artery. The CTA findings at admission (A and B) showed significant left renal artery dissection. The follow-up CTA after 1 month of conservative treatment (C and D) revealed that the false lumen aneurysm was expanded while the true lumen was narrowed. The follow-up CTA after 1 month of endovascular treatment (E and F) revealed that the stent was patent and the false lumen was thrombosed. The blue arrow represents renal artery dissection, the red arrow represents the renal infarct area, and the white arrow represents the renal artery dissection after receiving stent placement and coil embolization. CTA, computed tomographic angiography.
Discussion
Acute renal infarction is an uncommon disease whose incidence among all emergency admissions is as low as 0.007%. 7 Owing to its nonspecific clinical signs and symptoms, its diagnosis may be confused with acute pyelonephritis and nephrolithiasis. In a study by Yang et al, 8 34.8% patients with ARI had AKI at the time of diagnosis. A delayed diagnosis may aggravate impaired renal function or even result in death. According to the article by Siddiqui et al, 9 cardioembolic diseases, of which atrial fibrillation constitutes a major part, were the most common cause of ARI.
Symptomatic isolated spontaneous renal artery dissection is a rare cause of ARI. However, the etiology of SISRAD remains unclear. Some studies indicated conditions that may be related, including malignant hypertension, atherosclerosis, neoplastic disorders, and connective tissue disorders such as fibromuscular dysplasia, Marfan syndrome, and Ehlers-Danlos syndrome.10,11 Jha et al 2 revealed the mean age of SISRAD presentation was 43 years, which was similar to that in our study (43 years, range: 24–53). There is a strong male predominance, which is consistent with other reports.5,12 We found that arterial dissection in the visceral area, such as the superior mesenteric artery (SMA), seems to be more common in men. Whether it is related to hormones is unknown. We look forward to a larger sample size to explore this issue in the future. Because the patient with SISRAD is generally young and healthy, with few complications, the diagnosis is more likely to be delayed. The risks of primary outcomes, defined as aggravation of dissection requiring intervention and dissection-related mortality, were substantial in SISRAD. In a retrospective study of Jeong et al, 5 39% of the patients had progressed after conservative treatment, and among these patients, 44% with the worsened condition died, which corresponded to our study results (39% vs 62% [8/13], 44% vs 25% [2/8]). All mortality cases, including the article by Jeong et al, 5 resulted from an abrupt rupture of the dissection aneurysm. This outcome reminds us that the SISRAD has the potential to progress and may cause fatal complications in the acute phase. Except for the 2 deaths, the remaining patients had a good prognosis, and the symptoms of hematuria and albuminuria disappeared, which may have originated from the body’s stress response during ARI. Similar to the research of Faucon et al, 12 the occurrence of de novo arterial dissections in any renal or extrarenal vascular territory was low.
In addition, compared with other visceral artery dissections, SISRAD has a higher mortality rate. Although the exact pathogenesis is unknown, there are 3 possible hypotheses. (1) According to the literature, the average renal artery blood flow of adults is approximately 1000 mL/min, whereas the SMA blood flow is 517 mL/min,13,14 resulting in higher pressure on the wall of the renal artery. (2) Compared with SMA, renal artery has fewer branch arteries to decrease the pressure from the main trunk. Meanwhile, the branch arteries of the renal artery are commonly involved, which leads to renal infarction. (3) Jeong et al 5 also raised another causative factor that SMA was surrounded by dense lymphatic tissue, and these supporting structures had relatively higher resistance to artery dissection rupture.
Treatment of SISRAD can be classified into conservative treatment, endovascular intervention, and open surgery. There is a lack of a standardized and evidence-based consensus on a best initial treatment for this potentially fatal disease. According to the few case reports and literature available, conservative treatment is the first choice of initial treatment.3,5,6,15 Faucon et al 12 revealed that patients with renal artery dissection due to isolated renal artery dissection, fibromuscular dysplasia, and multisite arterial disease have good prognosis after conservative treatment. In our study, intestinal rest, pain control, and blood pressure control were selected as the basic components of medication. Additionally, anticoagulation and antiplatelet drugs were also used to prevent true lumen thrombosis. However, the choice of antiplatelet or anticoagulation drugs still remains controversial. Our study showed that patients with disease progression were younger than patients with a stable disease (39 vs 48, p=0.04) and had a high proportion of presence of dissection aneurysm in the CTA at admission (0% vs 87.5%, p=0.005). Thus, we speculated the presence of aneurysm is an early indicator of the urgency of the disease. We recommended intervention rather than conservative treatment as the initial treatment for young patients with dissection aneurysm (shown in Figure 4).
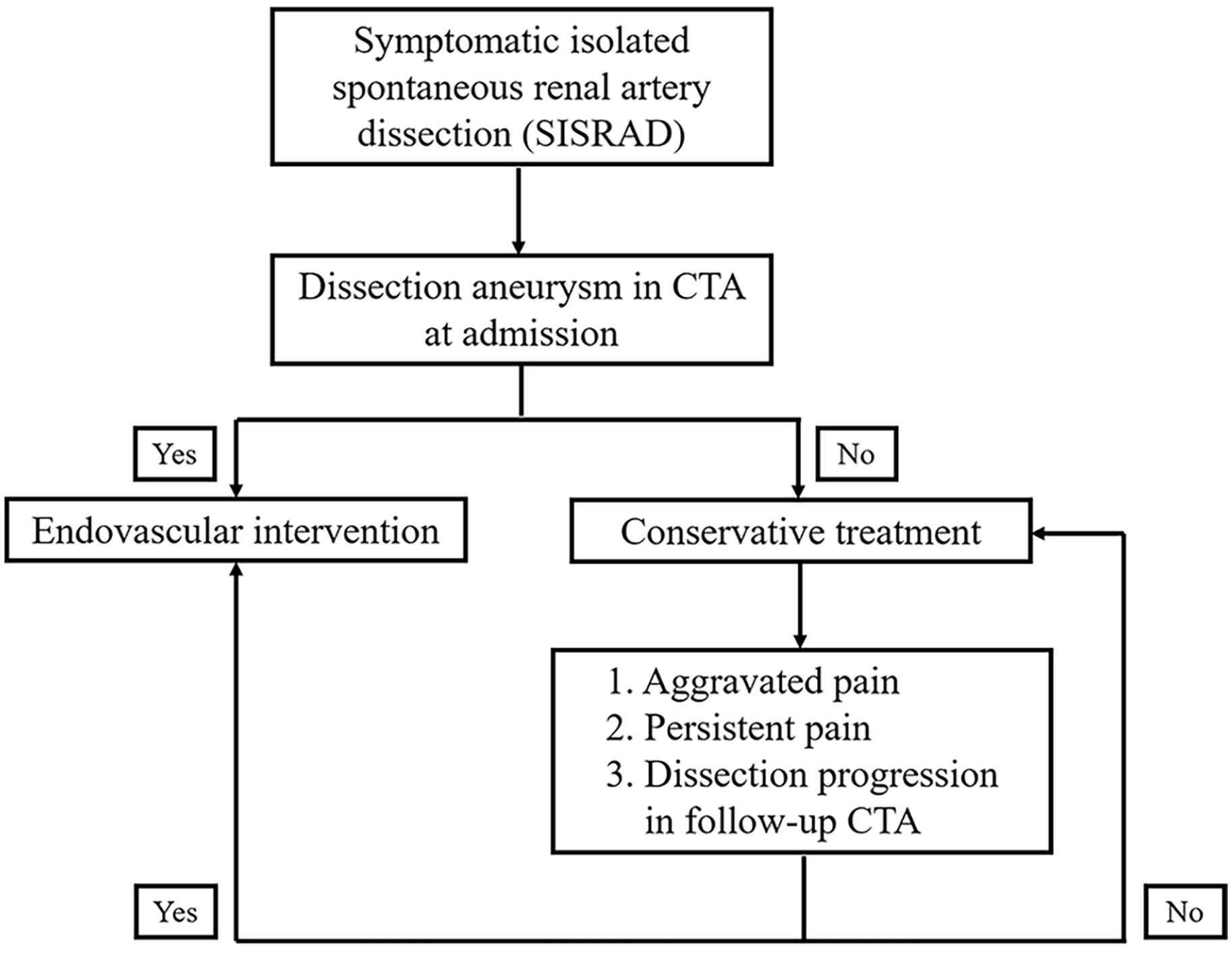
A more appropriate initial treatment strategy for SISRAD as expected. CTA, computed tomographic angiography.
Endovascular intervention is usually applied in visceral artery dissection cases including coil embolization to prevent dissection rupture and stent to maintain blood supply. In our study, 1 patient received isolated stent placement, 1 patient received isolated coil embolization, and 4 patients received stent placement combined with false lumen coil embolization. The endovascular intervention yielded an 83% (5/6) survival rate. Open surgery, including renal artery revascularization and nephrectomy, follow the same treatment ideas as endovascular intervention. With the rapid development of percutaneous endovascular intervention, open surgery is generally not considered because of the large trauma area and the difficulty of the operation.
This study has several limitations. First, it is a retrospective study, and prospective multicenter trials in the future are needed to explore the best strategy for SISRAD. Second, the patients only completed some routine tests when they were admitted to the hospital and lacked some specialized tests to better evaluate the condition and prove our speculation. Third, the number of patients involved in the study was relatively small, and the follow-up duration was relatively short. The natural history of SISRAD and the prognosis should be observed over a longer period. Finally, there are many conjectures about renal artery dissection in the article, but it is difficult to establish an animal model of renal artery dissection. There is a lack of pathological mechanisms and basic researches to support some of our conjectures.
In conclusion, SISRAD is a rare and fatal disease. Differentiating SISRAD from other causes of ARI in the early stage of the disease is important for the prognosis of the disease. Computed tomographic angiography examination is essential for ARI to diagnosis SISRAD. Dissection aneurysm at admission is a high-risk factor for progression of SISRAD and even renal artery rupture. We recommend endovascular intervention as the initial treatment for the SISRAD with dissection aneurysm.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The protocol was approved by the institutional review board from the ethics committee of Zhejiang University.