
Abstract
Purpose:
The purpose of this study was to investigate which treatment method for abdominal aortic aneurysm (AAA), endovascular or open repair, has better outcomes in young patients.
Materials and Methods:
A systematic review was conducted to identify observational studies or randomized controlled trials (RCTs) that compared endovascular and open repair of intact AAA in young patients. MEDLINE, EMBASE, and CENTRAL were searched up to March 2022 using the Ovid interface. The risk of bias was assessed with the Newcastle-Ottawa scale (NOS), with a maximum score of 9, or version 2 of the Cochrane risk of bias tool. The certainty of evidence was assessed with the GRADE framework. Primary outcomes were perioperative, overall, and aneurysm-related mortality. Secondary outcomes were reintervention, hospital length of stay, and perioperative complications. Effect measures in syntheses were the odds ratio (OR), risk difference (RD), mean difference (MD), or hazard ratio (HR) and were calculated with the Mantel-Haenszel or inverse variance statistical method and random-effects models.
Results:
Fifteen observational studies and 1 RCT were included, reporting a total of 48 976 young patients. Definitions of young ranged from 60 to 70 years. The median score on the NOS was 8 (range: 4–9), and the RCT was judged to be high risk of bias. The perioperative mortality was lower after EVAR (RD: −0.01, 95% CI: −0.02 to −0.00), but the overall and aneurysm-related mortality was not significantly different between EVAR and open repair (HR: 1.38, 95% CI: 0.81 to 2.33; HR: 4.68, 95% CI: 0.71 to 31.04, respectively), as was the hazard of reintervention (HR: 1.50, 95% CI: 0.88 to 2.56). The hospital length of stay was shorter after EVAR (MD: −4.44 days, 95% CI: −4.79 to −4.09), and the odds of cardiac (OR: 0.22, 95% CI: 0.13 to 0.35), respiratory (OR: 0.17, 95% CI: 0.11 to 0.26), and bleeding complications were lower after EVAR (OR: 0.26, 95% CI: 0.11 to 0.64). The level of evidence was low or very low.
Conclusion:
Patient preferences and perspectives should be considered during shared decision-making process considering the available evidence. EVAR may be considered in young and fit patients with a suitable anatomy.
Protocol registration:
PROSPERO, CRD42022325051
Clinical Impact
Uncertainty surrounds the optimal treatment strategy for abdominal aortic aneurysm in young patients. Meta-analysis of some 48,976 young patients showed that endovascular aneurysm repair (EVAR) has a lower perioperative mortality and morbidity and a shorter hospital and intensive care unit stay than open surgical repair, but the overall and aneurysm-related mortality in the short to medium term are not significantly different between EVAR and open repair. EVAR can be considered in young patients.
Introduction
Endovascular aneurysm repair (EVAR) is the most used therapeutic method for abdominal aortic aneurysm (AAA). Clinical practice guidelines specify 2 factors that should be considered when making decisions on treatment for AAA: anatomy and life expectancy.1,2 Although EVAR carries a lower perioperative morbidity and mortality risk, the long-term results may not be as good as with open repair.3,4 Randomized controlled trials (RCTs) have demonstrated a higher survival after EVAR than after open repair in the short term (up to 6 months), which is almost certainly attributed to the lower perioperative mortality of EVAR. 3 RCTs have also shown that the survival curves of patients treated with EVAR and open repair converge within 2 years after treatment, while open surgery has a survival advantage in the long term.3,5–7 Such observations may relate to higher rates of secondary interventions and aneurysm-related mortality in patients undergoing EVAR. Analyses of long-term data from large administrative datasets echo findings of RCTs, also casting a shadow on the durability of EVAR.8,9 Thus, in fit patients with a long life expectancy, open surgical repair may be advantageous over EVAR.1–3
Such observations have important implications in young patients. Indeed, while an average survival of 9 years has been reported following AAA repair, a longer survival is expected in younger patients. 10 Such patients might benefit from open surgery, which carries a lower risk of death and aneurysm-related complications in the long run. 10 This, coupled with the low perioperative mortality after open AAA repair in young and fit patients questions the use of EVAR in this age group. The objective of the review was to investigate whether EVAR has similar or worse outcomes compared with open AAA repair in young patients.
Materials and Methods
Review Design, Protocol Registration, Support, and Competing Interests
The objectives and methods of the review were prespecified in a protocol, which was registered in PROSPERO (CRD42022325051). No amendments to the review protocol were made during the conduct of the review. The review was developed in line with principles described in the Cochrane Handbook for Systematic Reviews of Interventions. 11 Reporting of the review complied with the updated Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 guidelines. 12 The PRISMA 2020 checklist was generated using a Shiny App available at https://prisma.shinyapps.io/checklist/ (Supplementary Appendix 1), and the study flow diagram was developed using a Shiny App available at https://www.eshackathon.org/software/PRISMA2020.html. A list of studies that were excluded from this review with reasons, template data collection forms, data extracted from included studies, data used for all analyses, and analytical code can be obtained from the corresponding author upon request. Such data are not publicly available. No financial or non-financial support was received for this review, and none of the review authors have any competing interests.
Eligibility Criteria
Types of studies
Studies that compared outcomes of standard endovascular repair versus open repair for intact AAA qualified for inclusion. No restrictions were applied to study design, ie, observational study versus RCT or prospective versus retrospective, number of institutions, ie, single center versus multicenter, time of treatment, or publication date. Studies with any duration of follow-up were eligible. Small case series reporting <10 cases were excluded, as were case reports and review articles. When 2 or more studies reported overlapping populations from the same institution(s), the largest study was eligible for inclusion. Publication report status, eg, conference abstract, was not an eligibility criterion. Only studies published in English were considered.
Types of participants
Eligible participants were young males or females who underwent endovascular or open repair for intact AAA. For the purposes of meta-analyses, we used the definition of “young” of the primary studies, but only definitions <70 years were accepted. Young patients treated for symptomatic ruptured or unruptured AAA were not considered.
Types of interventions
The intervention of interest was standard EVAR with any aortic device. The comparator intervention was open surgical repair. Complex endovascular or open surgical procedures, eg, fenestrated EVAR or open repair of para-/supra-renal or thoraco-abdominal aortic aneurysm, were not considered.
Types of outcome measures
Primary outcome measures were perioperative mortality, overall mortality, and aneurysm-related mortality. Aneurysm-related deaths were those that occurred during the hospital stay for or within 30 days from the index procedure or secondary intervention and those that occurred after AAA rupture confirmed on diagnostic imaging, during the operating procedure, or on post-mortem examination. Secondary outcomes were reintervention, hospital length of stay, need for and length of intensive care unit (ICU) stay, and perioperative complications. Studies should report at least 1 outcome measure to be eligible for inclusion in the review.
Literature Search Strategy and Information Sources
The literature search strategy was developed by a review author (G.A.) experienced in outreach, knowledge, and evidence search. The PICO (patient, intervention, comparison, outcome) approach was used to form the strategies. A combination of controlled vocabulary (subject headings) and free text terms was used to search electronic literature sources. Subject headings/thesaurus trees, search operators, and search limits in each of the electronic databases were adapted accordingly. Electronic searches were last run on the March 30, 2022. Database-specific search syntaxes are presented in Supplementary Appendix 2.
MEDLINE (Medical Literature Analysis and Retrieval System Online) and EMBASE (Excerpta Medica Database) were searched using the Ovid interface. CENTRAL (Cochrane Central Register of Controlled Trials) was also searched. Access to healthcare databases was via online sources of institutional library services. A second level search was conducted by interrogating the bibliographic list of articles that qualified for inclusion in this review.
Study Selection/Data Collection Process and Data Items
Two review authors (A.G., M.K.) conducted the prespecified literature searches and evaluated the eligibility of studies against the inclusion criteria independently. When disagreement arose, a third review author acted as an arbitrator (N.K.).
Data to be collected from individual studies were prespecified during the development of the review protocol. Additional relevant data identified during the data collection process were extracted. Data were extracted from the main text, figures, tables, or supplementary material of the original publications and were entered into a Microsoft Excel spreadsheet. Data extracted from Kaplan-Meier curves were digitalized using an open-source software (http://plotdigitizer.sourceforge.net). A mixture of direct methods, eg, from reported hazard ratios (HRs) with confidence intervals (CIs) and indirect methods, eg, from survival curves incorporating numbers at risk, was applied to calculate individual study HRs and standard errors (SEs) for specific outcome measures.13,14
When 2 or more reports corresponding to a study were available, the most recent was considered for data synthesis. Only published material was considered, and no study investigators were contacted to obtain or confirm relevant information. Two independent review authors (K.G., M.K.) extracted data from selected studies. Data were then cross-checked by a third review author (N.K.).
Data items were grouped as follows:
Study level data: first author, journal and year of publication, study period, country where the study was conducted (or of the corresponding author in case of multi-national studies), study design, number of institutions contributing to the study, definition of “young,” number of patients in the intervention and control group, and length of follow-up.
Individual study population data: sex, age, and maximum AAA diameter.
Data pertaining to risk of bias assessment.
Outcome data, as outlined in the Eligibility criteria section.
The outcomes were classified according to their importance for decision-making as critical, important but not critical, and of limited importance, in accordance with the Grading of Recommendation, Assessment, Development, and Evaluation (GRADE) framework.
Risk of Bias Assessment and Evidence Appraisal
The Newcastle-Ottawa scale (NOS) was used to assess the methodological quality of observational studies. 15 The tool is based on 3 domains, ie, selection, comparability, and exposure, with a total of 8 items and a maximum score of 9. Version 2 of the Cochrane risk of bias tool (RoB 2.0) was used to assess the risk of bias in RCTs. 16 The tool contains 5 domains: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in measurement of the outcome, and bias in selection of the reported result. An overall risk of bias judgment for a specific outcome is reached as follows: low risk of bias, some concerns, high risk of bias. Two review authors (N.G., N.K.) assessed the studies independently. When disagreement arose, consensual agreement was reached with discussions with the entire review team.
The quality of evidence for the primary and secondary outcomes was graded using the GRADE framework, which specifies 4 levels of the certainty of evidence for a given outcome, namely high, moderate, low, and very low.17,18 A summary of findings table was generated using an online platform (https://gdt.gradepro.org/app/).
Synthesis Methods
For binary outcomes, the effect measure used in synthesis was the odds ratio (OR) or risk difference (RD), if zero events were reported in both groups in at least 1 study, and 95% CI. For continuous outcomes, the effect measure was the mean difference (MD) and 95% CI. When standard deviations (SDs) of continuous variables were not reported in the original articles, they were calculated from CI limits, SEs, or range values according to methods proposed by Hozo et al 19 and Wan et al. 20 For follow-up outcomes, a time-to-event data meta-analysis was conducted using aggregate data, and the result was reported as summary HR and 95% CI.
All studies reporting the primary and/or secondary outcomes were eligible for data synthesis. Numbers of events and total numbers of patients in each group for dichotomous variables, mean values, corresponding SDs, and total numbers of patients in each group for continuous variables, and log HRs and SEs for time to event variables were inputted into the RevMan computer program (Version 5.4, Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2020). Pooled effect estimates for binary outcomes were calculated using the Mantel-Haenszel statistical method, and those for continuous and time to event outcomes were calculated using the inverse variance method. A forest plot was generated for graphical presentation of meta-analysis for each outcome.
Because of the anticipated between-study heterogeneity, random-effects models proposed by DerSimonian and Laird 21 were used for all meta-analyses. The extent and impact of between-study heterogeneity were assessed by inspecting the forest plots and by calculating the tau-squared and the I-squared statistics, respectively. Inconsistency was quantified and interpreted as previously described. 22
To assess risk of bias due to missing results, the effect by the inverse of its SE was plotted for each study and a funnel plot was generated. Publication bias was assessed both visually and mathematically using the Egger’s regression intercept for outcomes reported in 10 or more studies.
Sensitivity analyses were conducted to explore the robustness of the meta-analyses by excluding RCTs that were deemed to be high risk of bias on RoB 2.0 or observational studies with a NOS score <7. Separate meta-analyses of RCTs and observational studies were also conducted. Furthermore, the analyses were repeated after removing 1 study at a time to examine the impact of each study on the overall meta-analysis.
Results
Study Selection
Electronic literature searches yielded 19 381 reports. Sixteen studies met the review inclusion criteria and were included in qualitative and quantitative syntheses.9,23–37 The literature flow diagram is presented in Figure 1.
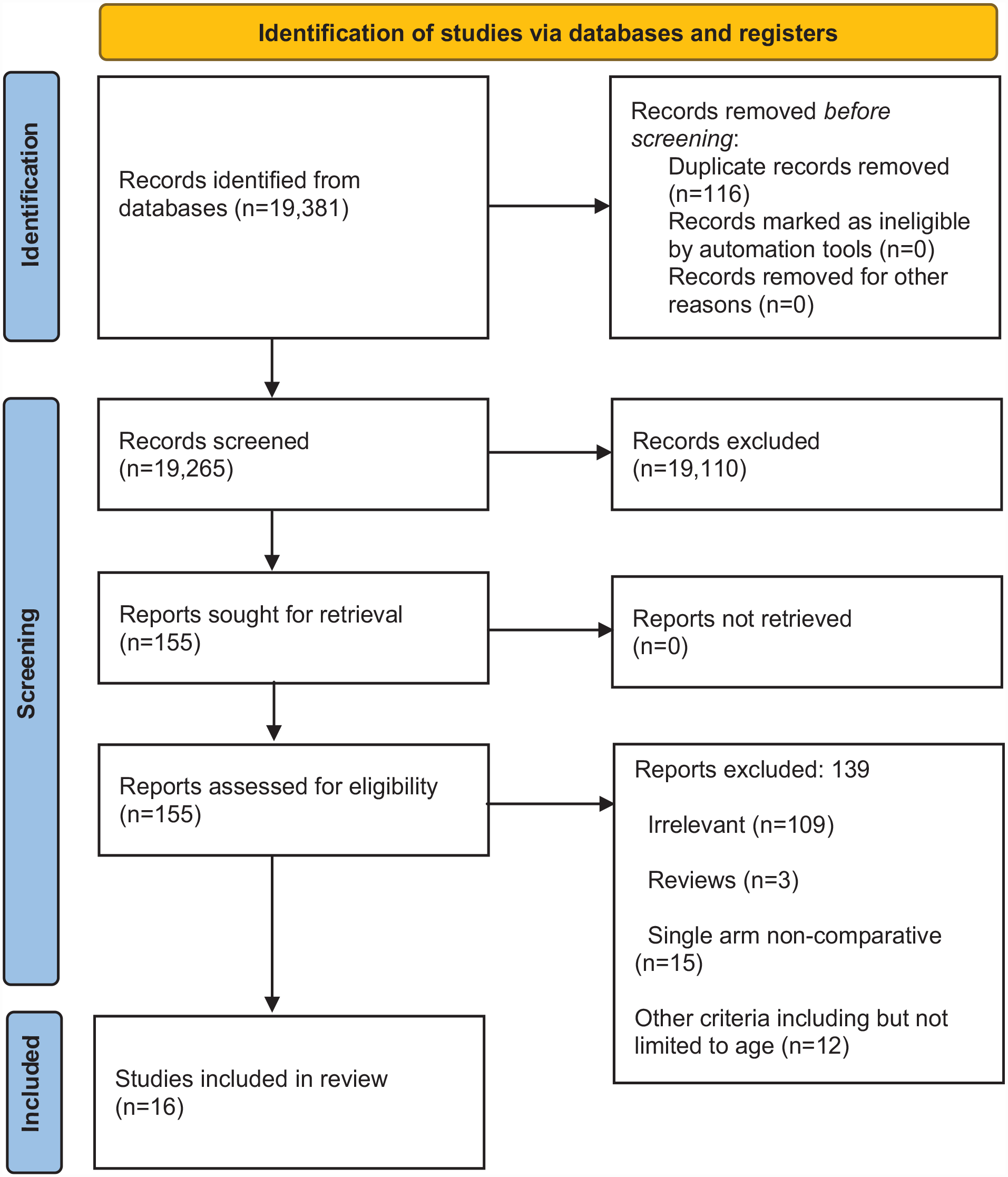
Literature flow diagram generated using a Shiny App available at https://www.eshackathon.org/software/PRISMA2020.html.
Study Characteristics
Of the 16 studies included in the review, 9 were retrospective observational studies (8 single center and 1 multicenter),23,26,27,29,30,33–36 6 reported administrative databases,9,24,25,28,31,32 and another 1 was an RCT. 32 The studies were published between 2008 and 2022, and the study recruitment period spanned from 1994 to 2021.
The studies reported a total of 48 976 young patients, of whom 26 227 were treated with EVAR, and the remaining 22 749 had open surgical repair. The individual study characteristics are summarized in Table 1.
Characteristics of the Studies Included in the Systematic Review.
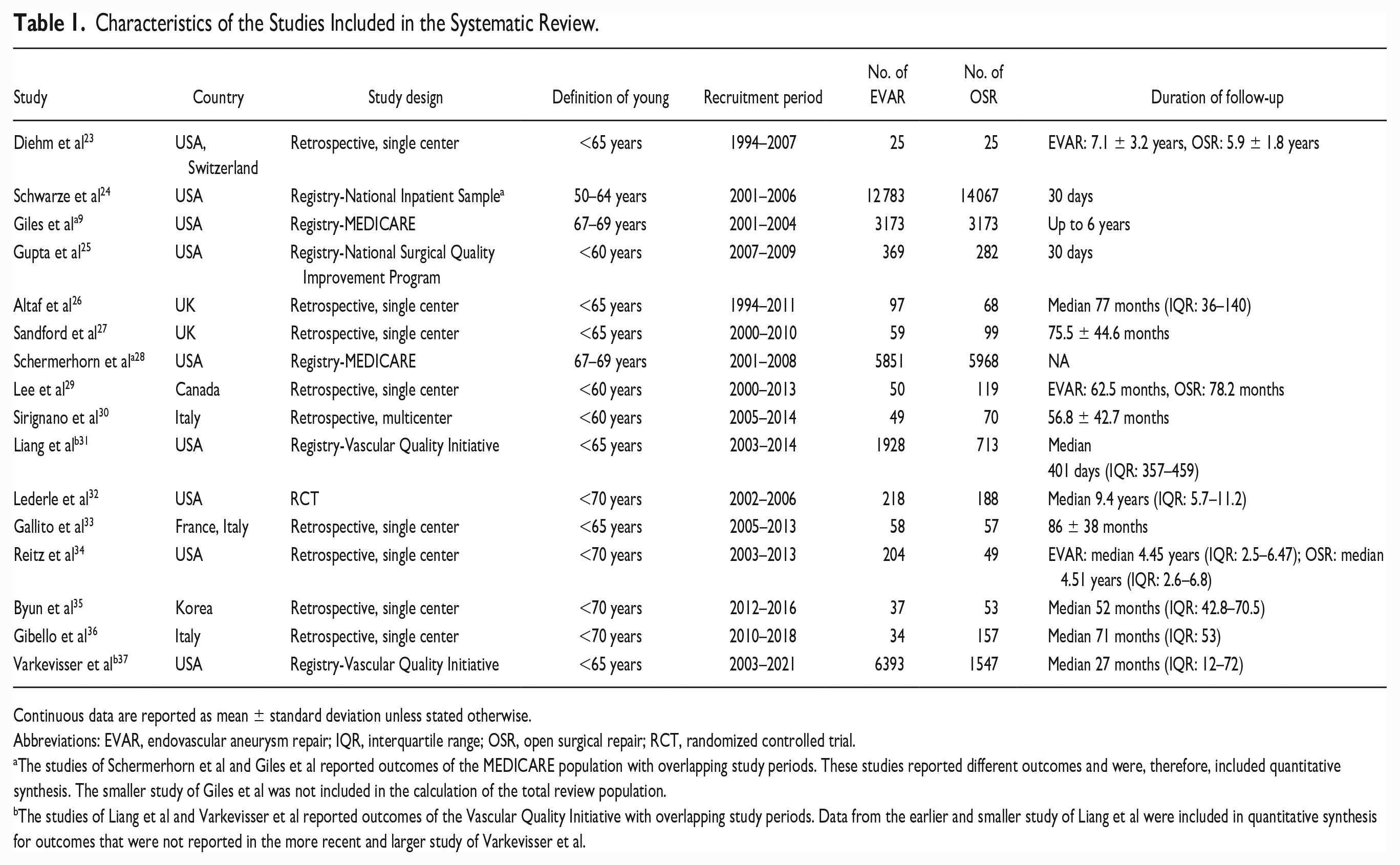
Continuous data are reported as mean ± standard deviation unless stated otherwise.
Abbreviations: EVAR, endovascular aneurysm repair; IQR, interquartile range; OSR, open surgical repair; RCT, randomized controlled trial.
The studies of Schermerhorn et al and Giles et al reported outcomes of the MEDICARE population with overlapping study periods. These studies reported different outcomes and were, therefore, included quantitative synthesis. The smaller study of Giles et al was not included in the calculation of the total review population.
The studies of Liang et al and Varkevisser et al reported outcomes of the Vascular Quality Initiative with overlapping study periods. Data from the earlier and smaller study of Liang et al were included in quantitative synthesis for outcomes that were not reported in the more recent and larger study of Varkevisser et al.
Definitions of young patients varied across the studies. Age thresholds to define young patients ranged from 60 to 70 years, with 7 studies23,24,26,27,31,33,37 using the threshold of 65 years, 4 studies32,34–36 using the threshold of 70 years, 2 studies9,28 using the threshold of 69 years, and 3 studies25,29,30 using the threshold of 60 years. The mean follow-up ranged from 30 days to 9.4 years. Most studies reported medium-term data (4–8 years), with 2 studies24,25 with a total of 27 501 studies reporting 30-day outcomes only. Baseline characteristics of the study populations are summarized in Supplementary Table 1.
Risk of Bias in Studies
The median score on the NOS for observational studies was 8 (range: 4–9). Issues were identified in case definition, representativeness of the cases, selection of controls, and comparability. In general, studies reporting administrative databases were judged to be of lower methodological quality, mainly due to limitations in the “selection” domain (Supplementary Table 2).
The RCT was judged to be high risk of bias (Supplementary Figure 1). Issues were identified in domain 2 (deviations from intended interventions) and domain 5 (selection of the reported result).
The results of the GRADE assessment are presented in Table 2. The level of evidence was very low for all outcomes except for the need for ICU and respiratory complications, for which the certainty of evidence was low. Downgrading of the evidence was mainly due to high risk of bias in included studies and inconsistency due to statistical heterogeneity and variability in definitions of young patients across the studies.
GRADE Assessment of the Certainty of Evidence for Reported Outcomes.
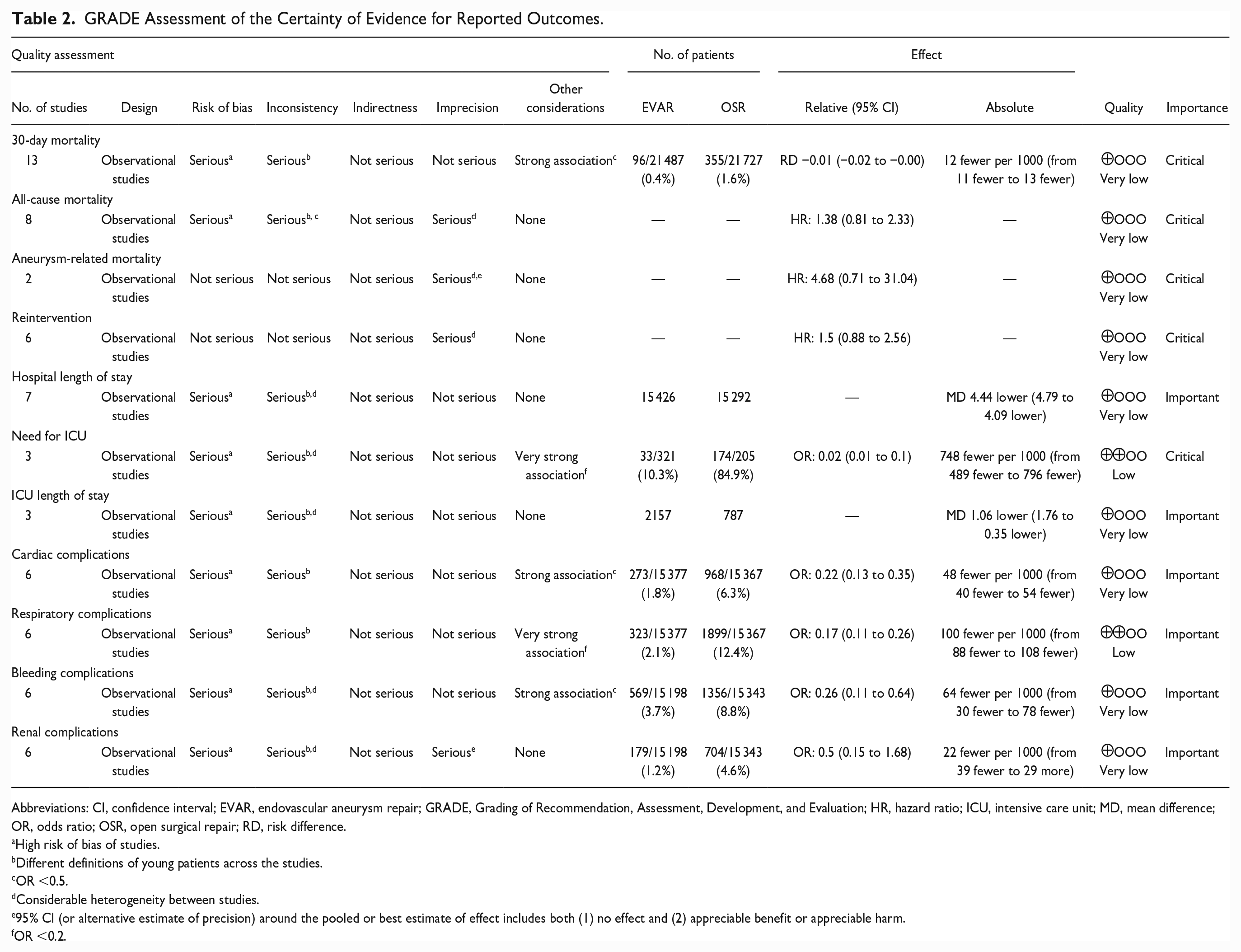
Abbreviations: CI, confidence interval; EVAR, endovascular aneurysm repair; GRADE, Grading of Recommendation, Assessment, Development, and Evaluation; HR, hazard ratio; ICU, intensive care unit; MD, mean difference; OR, odds ratio; OSR, open surgical repair; RD, risk difference.
High risk of bias of studies.
Different definitions of young patients across the studies.
OR <0.5.
Considerable heterogeneity between studies.
95% CI (or alternative estimate of precision) around the pooled or best estimate of effect includes both (1) no effect and (2) appreciable benefit or appreciable harm.
OR <0.2.
Results of Syntheses
Primary analyses
The forest plots for the primary and secondary outcomes are presented in Figures 2 and 3, respectively.
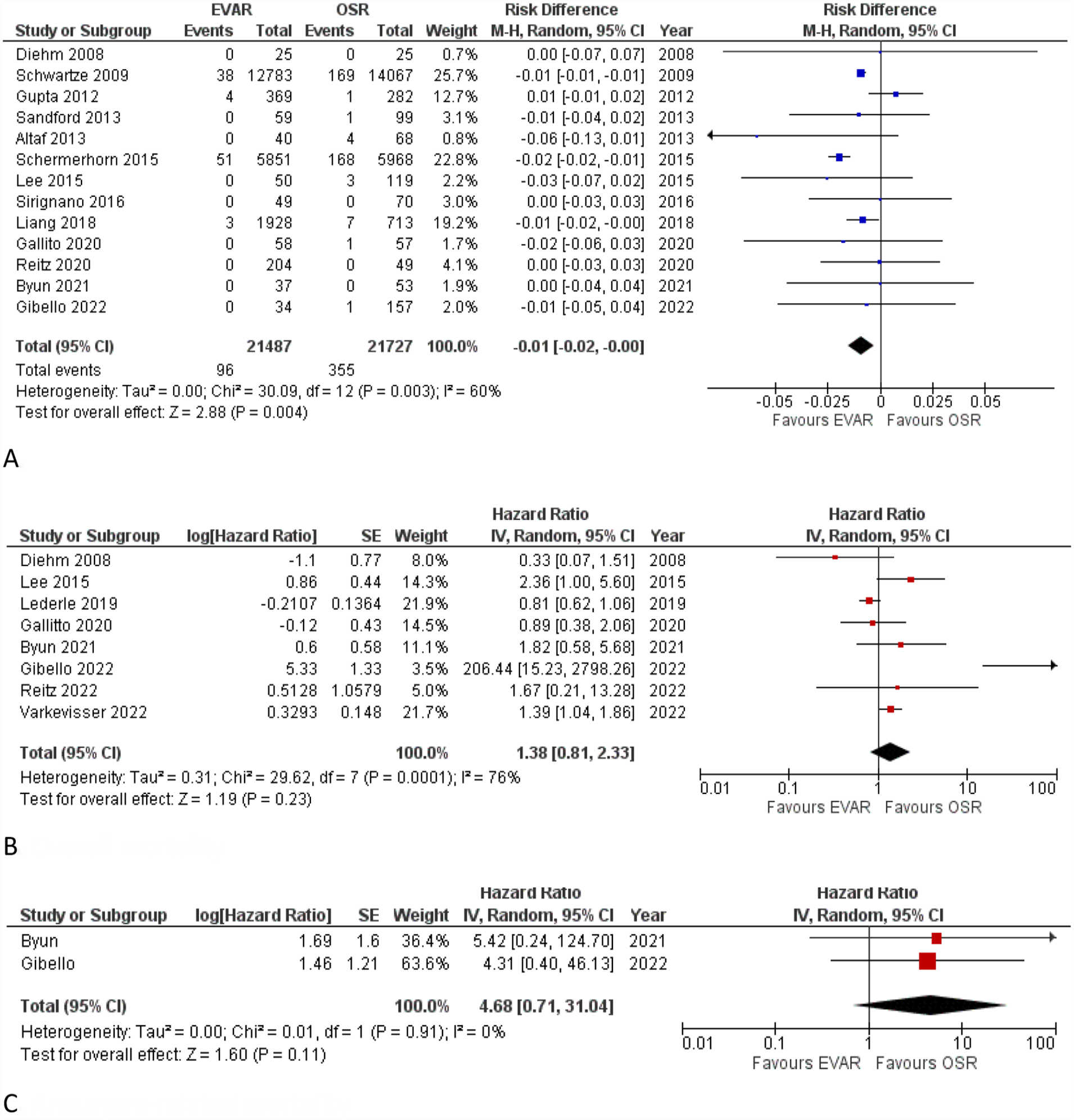
Forest plots of comparison of EVAR versus OSR for the primary outcomes. The solid squares denote the odds ratios, risk differences, or hazard ratios; the horizontal lines represent the 95% CIs; and the diamonds denote the pooled odds ratios, risk differences, or hazard ratios. (A) Perioperative mortality. (B) Overall mortality. (C) Aneurysm-related mortality. EVAR, endovascular aneurysm repair; OSR, open surgical repair; CI, confidence interval; M-H, IV, inverse variance; Mantel–Haenszel; SE, standard error.
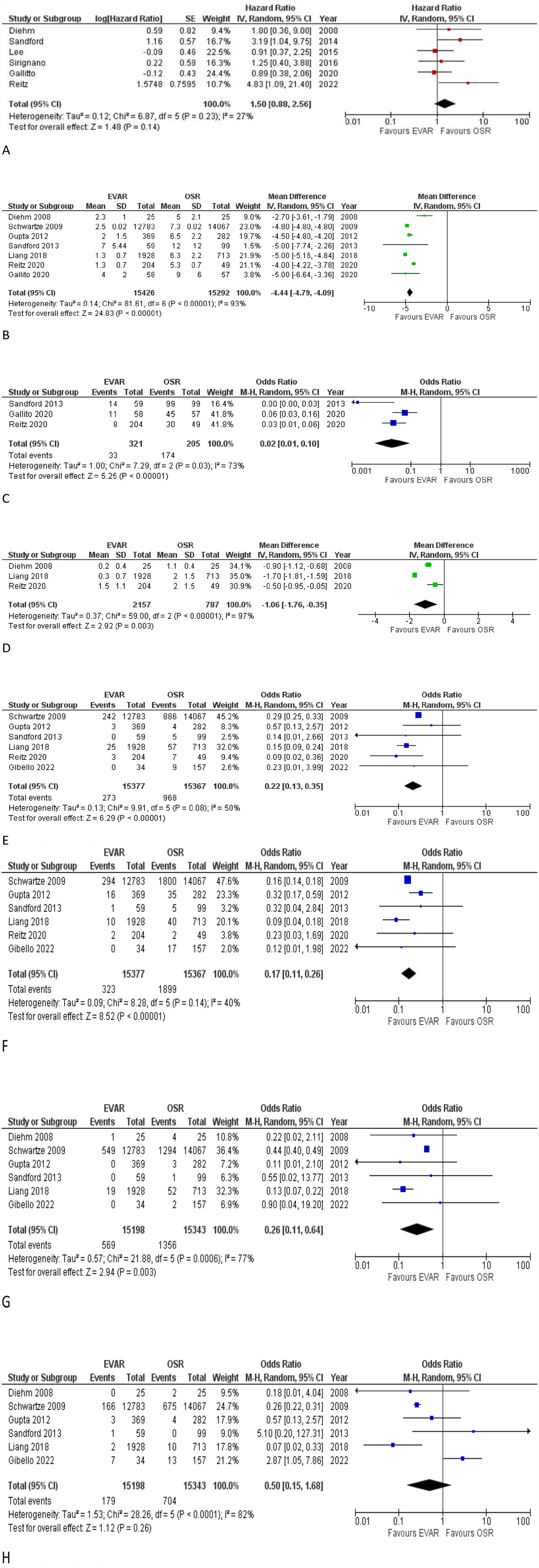
Forest plots of comparison of EVAR versus OSR for the secondary outcomes. The solid squares denote the odds ratios, hazard ratios, or mean differences; the horizontal lines represent the 95% CIs; and the diamonds denote the pooled odds ratios, hazard ratios, or mean differences. (A) Reintervention. (B) Hospital length of stay. (C) Need for ICU. (D) ICU length of stay. (E) Cardiac complications. (F) Respiratory complications. (G) Bleeding complications. (H) Renal complications. EVAR, endovascular aneurysm repair; OSR, open surgical repair; CI, confidence interval; ICU, intensive care unit; IV, inverse variance; M-H, Mantel–Haenszel; SE, standard error.
Perioperative mortality
Thirteen studies23,24,25–31,33–36 with a total of 43 214 patients (21 487 treated with EVAR and 21 727 treated with open repair) reported data on perioperative mortality. The perioperative mortality was lower in patients treated with EVAR (0.4%) compared with open repair (1.6%), with the difference being statistically significant (RD: −0.01, 95% CI: −0.02 to −0.00; p=0.004). The between-study heterogeneity was important (p=0.003, I2=60%). There was no statistical evidence of publication bias (p=0.932).
Overall mortality
Data on overall mortality were available from 8 studies.23,29,32–37 The overall mortality was not statistically significantly different between EVAR and open repair (HR: 1.38, 95% CI: 0.81 to 2.33; p=0.23). The between-study heterogeneity was substantial (p<0.001, I2=76%).
Aneurysm-related mortality
Data on aneurysm-related mortality were available from 2 studies.35,36 The aneurysm-related mortality was not statistically significantly different between EVAR and open repair (HR: 4.68, 95% CI: 0.71 to 31.04; p=0.11). The between-study heterogeneity was not important (p=0.91, I2=0%).
Reintervention
Data on reintervention were available from 6 studies.23,27,29,30,33,34 No statistically significantly difference in reintervention was found between EVAR and open repair (HR: 1.50, 95% CI: 0.88 to 2.56; p=0.14). The between-study heterogeneity was not important (p=0.23, I2=27%).
Hospital length of stay
Data on hospital length of stay were reported in 7 studies23,24,25,27,31,33,34 with a total of 30 718 patients (15 426 treated with EVAR and 15 292 treated with open repair). Patients treated with EVAR had a statistically significantly shorter hospital stay than those treated with open repair (MD: −4.44 days, 95% CI: −4.79 to −4.09; p<0.001). The between-study heterogeneity was considerable (p<0.001, I2=93%).
Need for and length of ICU stay
Data on the need for ICU stay after AAA treatment were reported in 3 studies27,33,34 with a total of 526 patients (321 treated with EVAR and 205 treated with open repair). Need for ICU stay was statistically significantly less in patients treated with EVAR (OR: 0.02, 95% CI: 0.01 to 0.10; p<0.001). The between-study heterogeneity was significant (p=0.03, I2=73%). Data on length of ICU stay were reported in 3 studies23,31,34 including a total of 2944 patients (2157 treated with EVAR and 787 treated with open surgical repair). ICU stay was shorter in patients treated with EVAR with the difference being statistically significant (MD: −1.06 days, 95% CI: −1.76 to −0.35; p=0.003). The between-study heterogeneity was significant (p<0.001, I2=97%).
Perioperative complications
Data on cardiac and respiratory complications were reported in 6 studies24,25,27,31,34,36 including a total of 30 744 patients (15 377 treated with EVAR and 15 367 treated with open repair). The odds of cardiac and respiratory complications were statistically significantly lower in patients treated with EVAR (OR: 0.22, 95% CI: 0.13 to 0.35; p<0.001, I2=50% and OR: 0.17, 95% CI: 0.11 to 0.26; p<0.001, I2=40%, respectively). Data on bleeding and renal complications were reported in 6 studies23,24,25,27,31,36 including a total of 30 541 patients (15 198 patients treated with EVAR and 15 343 treated with open repair). The odds of bleeding were statistically significantly lower in patients treated with EVAR (OR: 0.26, 95% CI: 0.11 to 0.64; p=0.003, I2=77%), but the difference in renal complications was not statistically significant (OR: 0.50, 95% CI: 0.15 to 1.68; p=0.26, I2=82%).
Sensitivity analyses
Sensitivity analyses excluding studies of low methodological quality did not show changes in the direction of effect estimate for any of the outcomes, but the statistical significance was lost for perioperative mortality (OR: 0.42, 95% CI: 0.10 to 1.68; p=0.22) and bleeding complications (OR: 0.40, 95% CI: 0.08 to 1.96; p=0.26). Exclusion of 1 study at a time did not affect the direction of effect estimate or statistical significance for any of the outcomes except for renal complications, where removal of the study of Gibello et al resulted in a statistically significant difference in favor of EVAR (OR: 0.28, 95% CI: 0.12 to 0.65; p=0.003). Further sensitivity analyses excluding the 4 studies32,34–36 that used 70 years as the cutoff age to define young patients did not affect the direction or significance of effect estimate for any of the outcomes. Similarly, meta-analyses of studies that used ≤65 years as the age cutoff to define young showed similar results to the overall meta-analysis for the primary outcomes (Supplementary Table 3).
Discussion
Our analysis showed that in young age groups, EVAR had a lower perioperative mortality than open surgical repair, but the overall and aneurysm-related mortality was not significantly different. The hazard of reintervention was not significantly different between EVAR and open repair, but the ICU and hospital stay were shorter after EVAR, and the risk of cardiac, respiratory, and bleeding complications occurring in the perioperative period was lower in patients treated with EVAR. Of note, the certainty of evidence was very low for nearly all of the outcomes, mainly due to high risk of bias and inconsistency. Inconsistency was due to different study designs (eg, observational studies versus randomized clinical trials versus administrative datasets), different study populations, and, most importantly, different age cutoffs to define young patients, with the cutoff ranging from 60 to 70 across the studies. Nevertheless, sensitivity analyses excluding studies with different age thresholds, eg, those with a cutoff >65 years, corroborated the results of the primary analyses demonstrating no changes to the direction or significance of effect estimates for the investigated clinical outcomes.
The perioperative survival advantage and lower complication rates with EVAR compared with open surgical repair in young patients are consistent with outcomes in all age groups, with all RCTs comparing EVAR with open surgical repair demonstrating such benefits. 3 The pooled perioperative mortality of open repair in our review population of nearly 22 000 patients was 1.6%, reflecting low perioperative risks in young and fit patients. Corresponding figures for EVAR in a total of nearly 21 500 young patients was much lower, with a pooled rate of 0.4%. Interestingly, sensitivity analyses excluding 6 studies of low methodological quality showed no statistically significant difference in perioperative mortality between EVAR and open repair with a low between-study heterogeneity (total number of patients: 1253; RD: −0.01, 95% CI: −0.02 to 0.00, p=0.20; test for heterogeneity: I2=0%, p=0.84). Expectedly, perioperative cardiac, respiratory, and bleeding complications were less frequent in patients treated with EVAR, and both the ICU and hospital stay were shorter after EVAR, reflecting the lower physiological impact of EVAR compared with open repair. Secondary interventions in follow-up were more frequently required after EVAR, though the difference in hazard was not statistically significant. Data granularity in retrospective observational cohort studies does not allow interpretation of the absence of significant difference in reintervention rates or making inferences about indications and nature of reinterventions in the treatment arms. Invasiveness of surgery, risk of postoperative complications, and likelihood of survival have been identified as most important determinants of patients’ decisions, 38 thus a balanced discussion of potential benefits of EVAR and open repair in individual patients should be undertaken during shared decision-making processes.
Meta-analysis of 2 studies reporting a total of 281 patients showed no significant difference in aneurysm-related mortality between EVAR and open repair in the young, which is not consistent with RCT data on all age groups. 3 This finding may reflect the paucity of relevant data in young age groups, considering that most studies included in our review had an observational design, thus ascertainment of outcome was difficult, if not impossible, in such retrospective studies. Therefore, the absence of a difference may merely be the result of type II error.
Advances in medical technologies and the increasing experience of vascular specialists in endovascular techniques and devices have resulted in improvements in short- and long-term outcomes of EVAR over time. Newer generation devices have been shown to be associated with aneurysm sac shrinkage and lower rates of conversion, reintervention, and aneurysm sac expansion.39,40 Such findings are particularly relevant in young patients, in whom a good long-term result is of importance, and indicate that the existing RCTs of EVAR versus open repair, where older generation devices were used, may be outdated. Interestingly, analyses of long-term data for patients <70 years in the OVER trial showed superior survival after EVAR compared with open surgery. 32 Similarly, a recent meta-analysis of long-term data on around 300 000 patients showed that the survival benefit of open surgery over EVAR was lost when older studies were excluded, indicating a significant improvement of EVAR outcomes over time. 4
Two previous meta-analyses have investigated outcomes of EVAR versus open surgery in young patients. The first, published in 2015 and including 9 studies with a considerably smaller population compared with the present analysis, found a perioperative survival advantage of EVAR over open repair but no significantly different mortality or reintervention rates during follow-up. 41 This study is limited by not applying appropriate time to event meta-analytical techniques, which account for time and the differential censoring of the subjects, ie, whether the event occurred and the time that has elapsed since some well-defined starting point. The second meta-analysis, published in 2019, is problematic with several critical methodological issues, making interpretation of the results impossible (ie, the authors state they included studies reporting on young patients, but this was not the case). 42
The findings of our study should be viewed and interpreted in the context of strengths and limitations. Nearly all studies included in meta-analyses were observational, inevitably limited by selection bias. Important prognostic parameters, such as neck anatomy and adherence to instructions for use, may be different between the groups and have not been taken into account in the analyses, eg, patients who underwent open repair may have had more complex anatomy. 43 The methodological quality of several studies was moderate or low, with issues of comparability in the design and/or analysis identified. Furthermore, the certainty of evidence was downgraded owing to clinical between-study heterogeneity resulting from variability in definitions of young patients, differences in demographics, clinical, and anatomical characteristics of the study populations, and varied clinical practices across the participating institutions. Inconsistency may have also resulted from methodological constraints, such as inconsistent outcome reporting. Notably, critical outcomes, such as aneurysm-related mortality, were not reported by most studies, most probably because of their retrospective design. Despite the limitations, this is a report of a large meta-analysis population, representing real-world experiences, with a strong association for several of the outcomes.
Conclusions
EVAR has superior perioperative outcomes compared with open repair in young patients, though meta-analysis of the higher quality studies showed no statistically significant difference in perioperative mortality. The overall and aneurysm-related mortality are not significantly different between EVAR and open surgical repair in the short and medium term. Patient preferences and perspectives should be considered during shared decision-making process considering the available evidence. EVAR may be considered in young and fit patients with a suitable anatomy. Higher level evidence from RCTs in young age groups may shed further light on potential advantages of EVAR with newer generation devices and modern endovascular technologies.
Supplemental Material
sj-docx-1-jet-10.1177_15266028231179419 – Supplemental material for Systematic Review With Meta-Analysis of Endovascular Versus Open Repair of Abdominal Aortic Aneurysm Repair in the Young
Supplemental material, sj-docx-1-jet-10.1177_15266028231179419 for Systematic Review With Meta-Analysis of Endovascular Versus Open Repair of Abdominal Aortic Aneurysm Repair in the Young by Nikolaos Kontopodis, Aikaterini Gavalaki, Nikolaos Galanakis, Michalis Kantzas, Christos Ioannou, George Geroulakos, John Kakisis and George A. Antoniou in Journal of Endovascular Therapy
Supplemental Material
sj-docx-2-jet-10.1177_15266028231179419 – Supplemental material for Systematic Review With Meta-Analysis of Endovascular Versus Open Repair of Abdominal Aortic Aneurysm Repair in the Young
Supplemental material, sj-docx-2-jet-10.1177_15266028231179419 for Systematic Review With Meta-Analysis of Endovascular Versus Open Repair of Abdominal Aortic Aneurysm Repair in the Young by Nikolaos Kontopodis, Aikaterini Gavalaki, Nikolaos Galanakis, Michalis Kantzas, Christos Ioannou, George Geroulakos, John Kakisis and George A. Antoniou in Journal of Endovascular Therapy
Supplemental Material
sj-docx-3-jet-10.1177_15266028231179419 – Supplemental material for Systematic Review With Meta-Analysis of Endovascular Versus Open Repair of Abdominal Aortic Aneurysm Repair in the Young
Supplemental material, sj-docx-3-jet-10.1177_15266028231179419 for Systematic Review With Meta-Analysis of Endovascular Versus Open Repair of Abdominal Aortic Aneurysm Repair in the Young by Nikolaos Kontopodis, Aikaterini Gavalaki, Nikolaos Galanakis, Michalis Kantzas, Christos Ioannou, George Geroulakos, John Kakisis and George A. Antoniou in Journal of Endovascular Therapy
Supplemental Material
sj-docx-4-jet-10.1177_15266028231179419 – Supplemental material for Systematic Review With Meta-Analysis of Endovascular Versus Open Repair of Abdominal Aortic Aneurysm Repair in the Young
Supplemental material, sj-docx-4-jet-10.1177_15266028231179419 for Systematic Review With Meta-Analysis of Endovascular Versus Open Repair of Abdominal Aortic Aneurysm Repair in the Young by Nikolaos Kontopodis, Aikaterini Gavalaki, Nikolaos Galanakis, Michalis Kantzas, Christos Ioannou, George Geroulakos, John Kakisis and George A. Antoniou in Journal of Endovascular Therapy
Supplemental Material
sj-docx-5-jet-10.1177_15266028231179419 – Supplemental material for Systematic Review With Meta-Analysis of Endovascular Versus Open Repair of Abdominal Aortic Aneurysm Repair in the Young
Supplemental material, sj-docx-5-jet-10.1177_15266028231179419 for Systematic Review With Meta-Analysis of Endovascular Versus Open Repair of Abdominal Aortic Aneurysm Repair in the Young by Nikolaos Kontopodis, Aikaterini Gavalaki, Nikolaos Galanakis, Michalis Kantzas, Christos Ioannou, George Geroulakos, John Kakisis and George A. Antoniou in Journal of Endovascular Therapy
Supplemental Material
sj-docx-6-jet-10.1177_15266028231179419 – Supplemental material for Systematic Review With Meta-Analysis of Endovascular Versus Open Repair of Abdominal Aortic Aneurysm Repair in the Young
Supplemental material, sj-docx-6-jet-10.1177_15266028231179419 for Systematic Review With Meta-Analysis of Endovascular Versus Open Repair of Abdominal Aortic Aneurysm Repair in the Young by Nikolaos Kontopodis, Aikaterini Gavalaki, Nikolaos Galanakis, Michalis Kantzas, Christos Ioannou, George Geroulakos, John Kakisis and George A. Antoniou in Journal of Endovascular Therapy
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.