
Abstract
Purpose:
To determine whether the STOP-Bang questionnaire, which is a tool for evaluating obstructive sleep apnea, is associated with aortic remodeling after thoracic endovascular aortic repair (TEVAR) in patients with type B aortic dissection (TBAD).
Methods:
Patients with TBAD who underwent standard TEVAR at our center from January 2015 to December 2020 were enrolled. For the included patients, we recorded baseline characteristics, comorbidities, preoperative computed tomographic angiography findings, procedure details, and complications. The STOP-Bang questionnaire was administered to each patient. Total scores comprised points for 4 yes/no questions and 4 clinical measurements. STOP-Bang ≥5 and STOP-Bang <5 groups were then created using the STOP-Bang total scores. We evaluated aortic remodeling 1 year after discharge and the reintervention rate, as well as false lumen complete thrombosis (FLCT) and non-FLCT length.
Results:
Fifty-five patients were enrolled in the study; STOP-Bang <5, n=36, and STOP-Bang ≥5, n=19. Compared with the STOP-Bang ≥5 group, the STOP-Bang <5 group achieved statistically significantly higher descending aorta positive aortic remodeling (PAR) rates in zones 3 to 5 (zone 3: p=0.002; zone 4: p=0.039; zone 5: p=0.023), higher total descending aorta-PAR rate (66.7% vs 36.8%, respectively; p=0.004), and lower reintervention rate (8.1% vs 38.9%, respectively; p=0.005). In the logistic regression analysis, STOP-Bang ≥5 had an odds ratio of 0.12 (95% confidence interval: 0.03–0.58; p=0.008). There was no significant difference in overall survival between the groups.
Conclusion:
STOP-Bang questionnaire scores were associated with aortic remodeling after TEVAR in patients with TBAD. Increasing the frequency of surveillance after TEVAR might be beneficial in these patients.
Clinical Impact
We analysed aortic remodelling 1 year after thoracic endovascular aortic repair (TEVAR) in acute type B aortic dissection (TBAD) patients with STOP-Bang < 5 and STOP-Bang ≥ 5. Aortic remodelling was better, and the reintervention rate was higher in patients with STOP-Bang < 5 compared with patients with STOP-Bang ≥ 5. In patients with STOP-Bang ≥ 5, aortic remodelling was worse in zones 3–5 compared with zones 6–9. This study suggests that the STOP-Bang questionnaire results is associated with aortic remodelling after TEVAR in patients with TBAD.
Keywords
Introduction
Aortic dissection is a common catastrophic aortic event with a rate of 3 to 10 per 100 000 people.1–3 According to the Stanford classification, aortic dissection (AD) can be classified as type A and type B, where type B dissection is defined as an AD with an entry tear in zone 1 or beyond. 4 Thoracic endovascular aortic repair (TEVAR) has become the first-line treatment for complicated type B aortic dissection (TBAD) and an important treatment for uncomplicated TBAD with high-risk features. According to the recent Society of Thoracic Surgeons/American Association guidelines, the main goal of TEVAR in the management of TBAD is rapid control of a rupture or covering the primary entry tear to restore true lumen flow. Achieving this goal induces false lumen (FL) thrombosis and promotes long-term aortic remodeling. 5 Even with coverage of the proximal entry tear, some patients do not achieve positive aortic remodeling (PAR) and may require reintervention.6,7 Identifying these patients and performing TEVAR with concurrent adjunct techniques (e.g., FL embolization, Provisional Extension To Induce Complete Attachment, Stent-Assisted Balloon-Induced Intimal Disruption and Relamination in Aortic Dissection Repair) to avoid additional reinterventions is valuable clinically.
Recently, researchers have become interested in the relationship between obstructive sleep apnea (OSA) and AD. 8 Patients with thoracic aorta dissection present with a high prevalence of previously undiagnosed and frequently severe OSA. 9 However, reports of the effect of OSA on aortic remodeling after TEVAR in patients with acute TBAD are lacking. Although the gold standard for OSA diagnosis is polysomnography, owing to the severe condition of AD patients, it is considered unethical to perform polysomnography in each of these patients preoperatively, especially in patients with complicated AD. In this case, using the STOP-Bang questionnaire is a simpler and quicker alternative because a STOP-Bang score in the range of 5 to 8 identifies surgical patients with moderate/severe OSA with high sensitivity and specificity.10–12 The objective of this study was to investigate whether the STOP-Bang questionnaire was associated with aortic remodeling after TEVAR in patients with acute TBAD.
Materials and Methods
Patients and Data Collection
We retrospectively collected data from the electronic medical records system for patients with TBAD who had undergone standard TEVAR at our center from January 2015 to December 2020. The need for informed consent was waived because of the study’s retrospective design. This study complied with the Strengthening the Reporting of Observational Studies in Epidemiology statement. Patients who survived for <1 year after TEVAR were excluded because they would not have computed tomographic angiography (CTA) results. Patients who developed serious complications requiring reinterventions were excluded because this situation was inconsistent with aortic remodeling with standard TEVAR. Patients who had undergone TEVAR previously and those with chronic TBAD, dialysis histories, active malignancy, Marfan syndrome, or connective tissue diseases and incomplete data were also excluded from the present study. In addition, patients who developed major adverse events (e.g., stroke, paraplegia, serious cardiovascular events, or rupture) were excluded from this study because they could not undergo CTA at the 1-year follow-up; these patients had incomplete data. The included patients’ data for baseline characteristics, comorbidities, preoperative CTA findings, and procedure details were collected for this study.
STOP-Bang and Procedure Details
The patients received optimal medical therapy on admission and were subsequently asked the questions in the STOP-Bang questionnaire. 10 Four yes/no questions related to snoring, tiredness during the daytime, observed apnea during sleep, and hypertension were asked. Four clinical characteristics (body mass index [BMI], age, neck circumference, and sex) were then recorded. One point was recorded if the patient answered yes to a question, and one point each was recorded if the patient was male, had a BMI >35 kg/m2, was ≥50 years of age, or had a neck circumference of >40 cm. The total points were the patient’s final STOP-Bang score. Patients were then divided into a STOP-Bang ≥5 group and a STOP-Bang <5 group based on the STOP-Bang score.
For patients with complicated TBAD, TEVAR was performed as soon as possible, depending on the patient’s condition. For patients with uncomplicated high-risk TBAD, TEVAR was delayed until the subacute phase. All patients received standard TEVAR using the Ankura Thoracic Aorta Stent Graft System (Lifetech Scientific, Shenzhen, China) to cover the primary entry tear, and the landing zone was extended using the fenestration or chimney technique if the proximal landing zone did not reach 20 mm.
Patients continued optimal medical therapy postoperatively lifelong and were followed up in the outpatient clinic 1 month after discharge. Patients were ordered to undergo CTA 1 year after discharge and are currently being followed up annually until death.
Definitions of Aortic Remodeling and FL Thrombosis
According to the Society for Vascular Surgery and the Society of Thoracic Surgeons reporting standards for TBAD, the term “PAR” is defined as an aorta that demonstrates at least one of the following: (1) FL reduction in maximal diameter or volume and no growth in total aortic diameter or volume; (2) true lumen expansion in maximal diameter or volume and no growth in total aortic diameter or volume; and (3) total aortic maximal diameter reduction with variable changes in true and FL diameters. 4 Negative aortic remodeling (NAR) represents the opposite conditions or a failure to demonstrate any of the descriptions for PAR. Positive aortic remodeling in all segments of the descending aorta of patients (from zones 3–9) was defined as total descending aorta-PAR (TDA-PAR). The indications for patients requiring reintervention were consistent with those for chronic AD, which comprised aneurysmal dilatation (total: ≥55–60 mm), increasing rate of enlarging diameter (>10 mm/year), and/or symptoms (pain, malperfusion). 5
False lumen complete thrombosis (FLCT) was defined as complete thrombosis of the aortic FL on arterial- and delayed-phase imaging, whereas patent FL (flow present throughout the entire aortic FL with arterial-phase or delayed contrast-enhanced imaging) and FL partial thrombosis (clots within the aortic FL but with a residual patent flow channel on arterial-phase or delayed contrast-enhanced imaging) were defined as non-FLCT.
The primary outcome of this study was aortic remodeling and the need for reintervention 1 year after discharge. The secondary outcomes were FLCT and non-FLCT length 1 year after discharge and 5-year overall survival.
Statistical Analysis
All statistical analyses were performed using SPSS software, version 22.0, (IBM Corp., Armonk, NY) and GraphPad Prism software, version 9.0.0, (GraphPad Software, Inc., San Diego, CA). Continuous variables are expressed using means and standard deviations, and categorical variables are expressed using frequencies and percentages. After the Shapiro-Wilk test, normally distributed continuous variables were compared using Student’s t test, and skewed-distribution data were compared using the Mann-Whitney U test. The χ2 or Fisher’s exact test (theoretical frequency [T] <1 or n<40) were used to test the categorical variables. Baseline characteristics with p<0.1 were included in a binary logistic regression analysis to determine whether the STOP-Bang was truly associated with aortic remodeling. Five-year overall survival was compared using the Kaplan-Meier univariable analysis, and log-rank tests were performed to analyze the difference between the groups. Kaplan-Meier survival curves were used to determine the overall survival between the groups. Statistical significance was observed when p<0.05.
Results
Patients’ Baseline Characteristics and TEVAR Details
Fifty-five patients were enrolled in this study after applying the inclusion and exclusion criteria, namely 36 in the STOP-Bang <5 group and 19 in the STOP-Bang ≥5 group (Figure 1). There were no significant differences in age (p=0.78), low-density lipoprotein concentration (p=0.060), hypertension (p=0.10), diabetes (p=0.39), smoking history (p=0.81), or drinking history (p=0.99) between the two groups. The STOP-Bang <5 group had a lower proportion of male patients (47.2% vs 89.5%; p=0.002) and lower BMI (23.22±3.35 kg/m2 vs 25.06±2.41 kg/m2; p=0.025) and serum creatinine concentration (72.19±22.00 µmol/L vs 88.17±30.11 µmol/L; p=0.029) than the STOP-Bang ≥5 group (Table 1). There was no statistically significant difference between the groups in the procedure phase (p=0.64), rate of complicated dissections (p=0.82), maximum aortic diameter (p=0.67), dissection length (p=0.60), stent graft coverage length (p=0.93), fenestration or chimney technique (p=0.74), and procedure time (p=0.20) (Table 2).
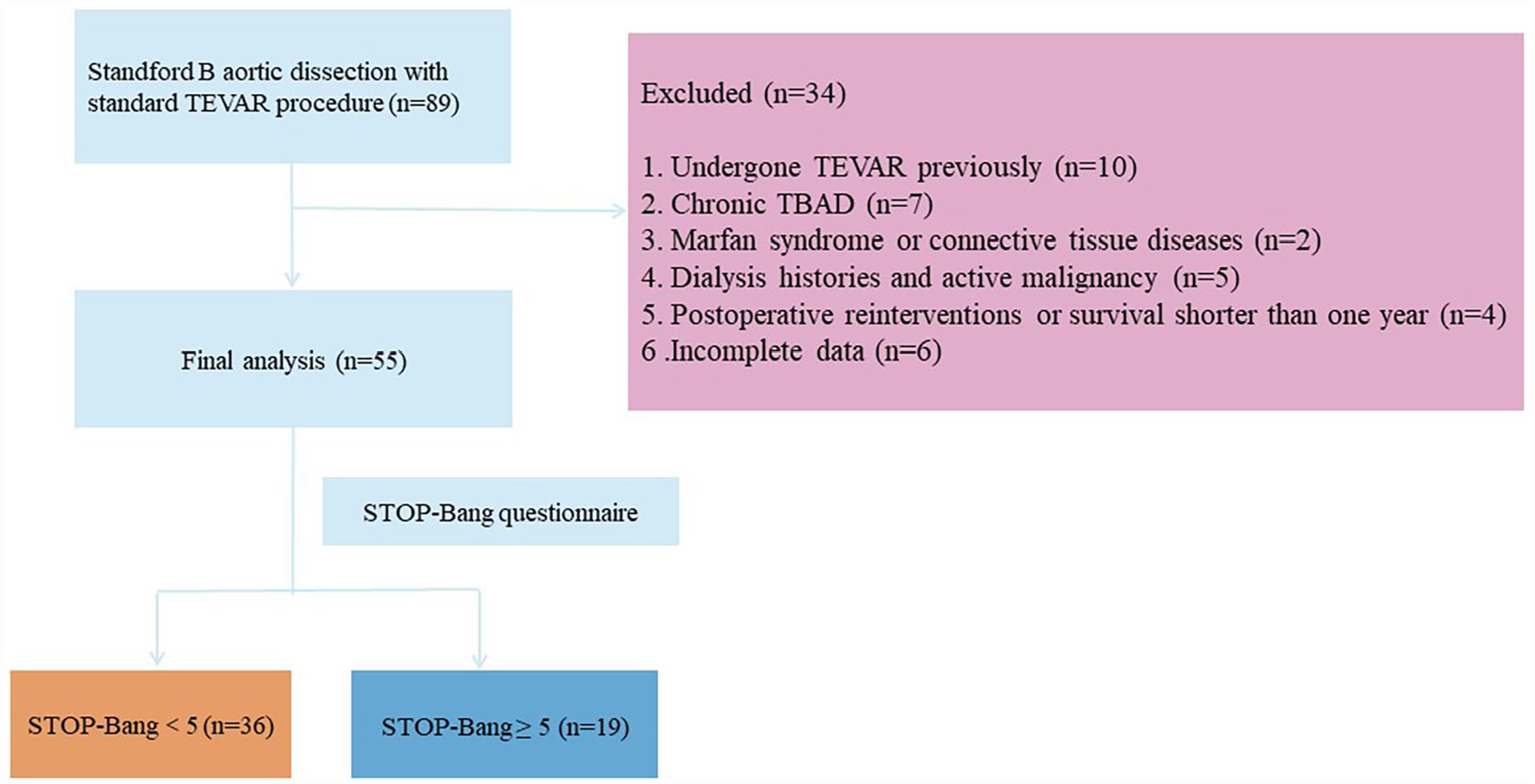
Flowchart of patient enrollment. TBAD, type B aortic dissection; TEVAR, thoracic endovascular aortic repair.
Baseline Characteristics.
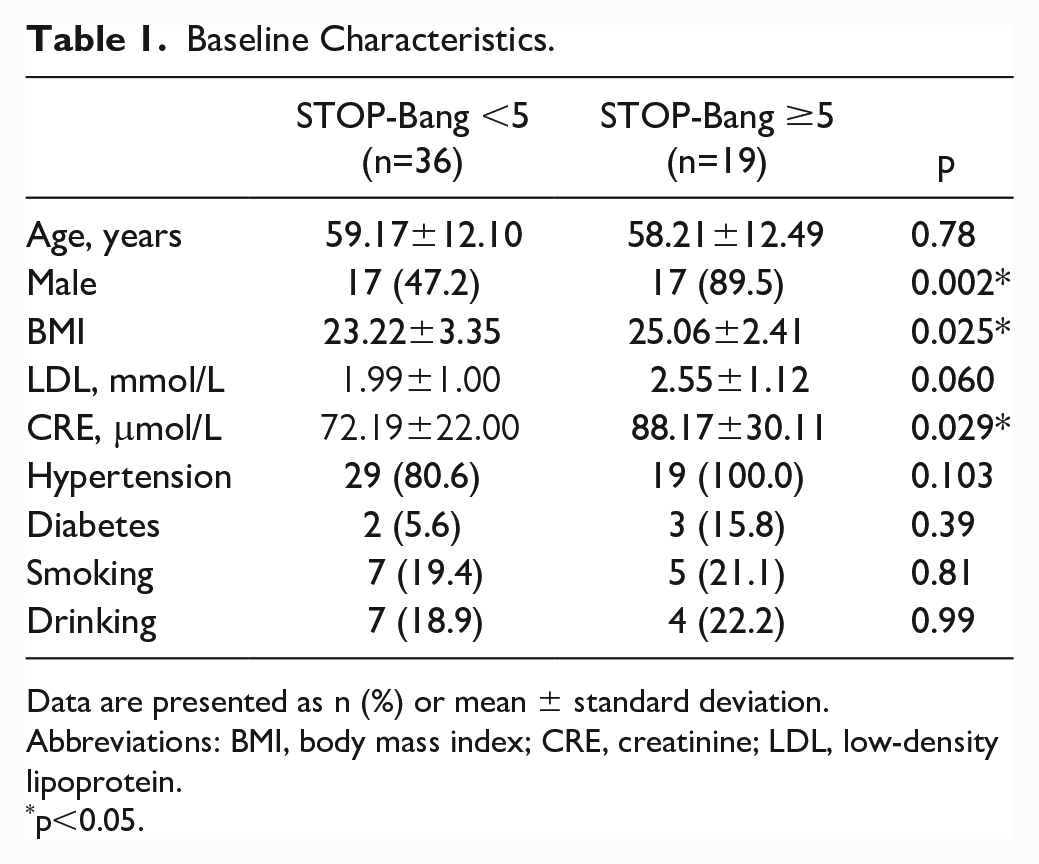
Data are presented as n (%) or mean ± standard deviation.
Abbreviations: BMI, body mass index; CRE, creatinine; LDL, low-density lipoprotein.
p<0.05.
TEVAR Details and Outcomes.
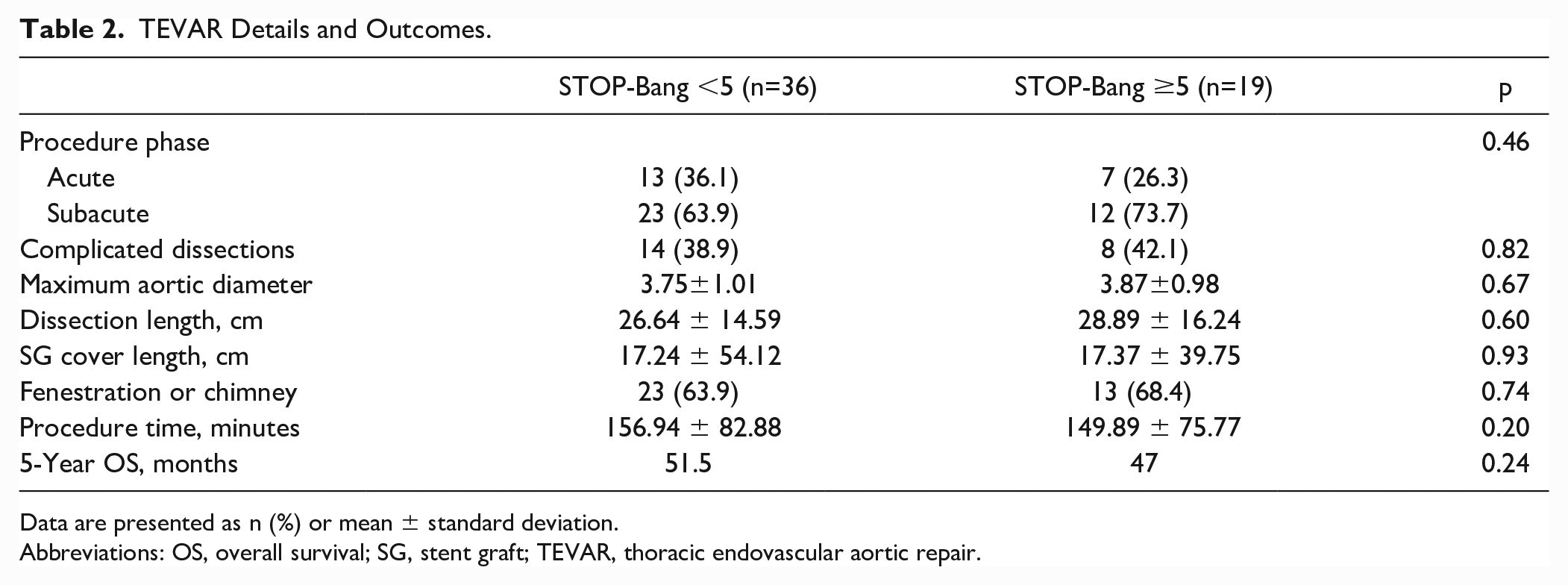
Data are presented as n (%) or mean ± standard deviation.
Abbreviations: OS, overall survival; SG, stent graft; TEVAR, thoracic endovascular aortic repair.
Aortic Remodeling
One year after discharge, patients in the STOP-Bang <5 group achieved higher descending aortic PAR than patients in the STOP-Bang ≥5 group with rates of 86.1% versus 47.4% in zone 3 (p=0.002), 83.3% versus 57.9% in zone 4 (p=0.039), 89.9% versus 63.2% in zone 5 (p=0.023), 83.3% versus 63.2% in zone 6 (p=0.094), 86.1% versus 63.3% in zone 7 (p=0.050), 83.3% versus 68.4% in zone 8 (p=0.20), and 91.7% versus 73.7% in zone 9 (p=0.072), respectively. Patients in the STOP-Bang <5 group also had higher TDA-PAR than those in the STOP-Bang ≥5 group (66.7% vs 36.8%, respectively; p=0.004) (Figure 2A). Although not statistically different, there appeared to be a trend toward more FLCT (59.1% vs 36.8%; p=0.16) and shorter non-FLCT lengths (10.12±11.65 cm vs 12.48±13.08 cm; p=0.498) in patients in the STOP-Bang <5 group than in the STOP-Bang ≥5 group, respectively, (Figure 2B). In addition, patients in the STOP-Bang <5 group had a lower reintervention rate than those in the STOP-Bang ≥5 group (8.1% vs 38.9%, respectively; p=0.005) (Table 3) (Figure 2C).
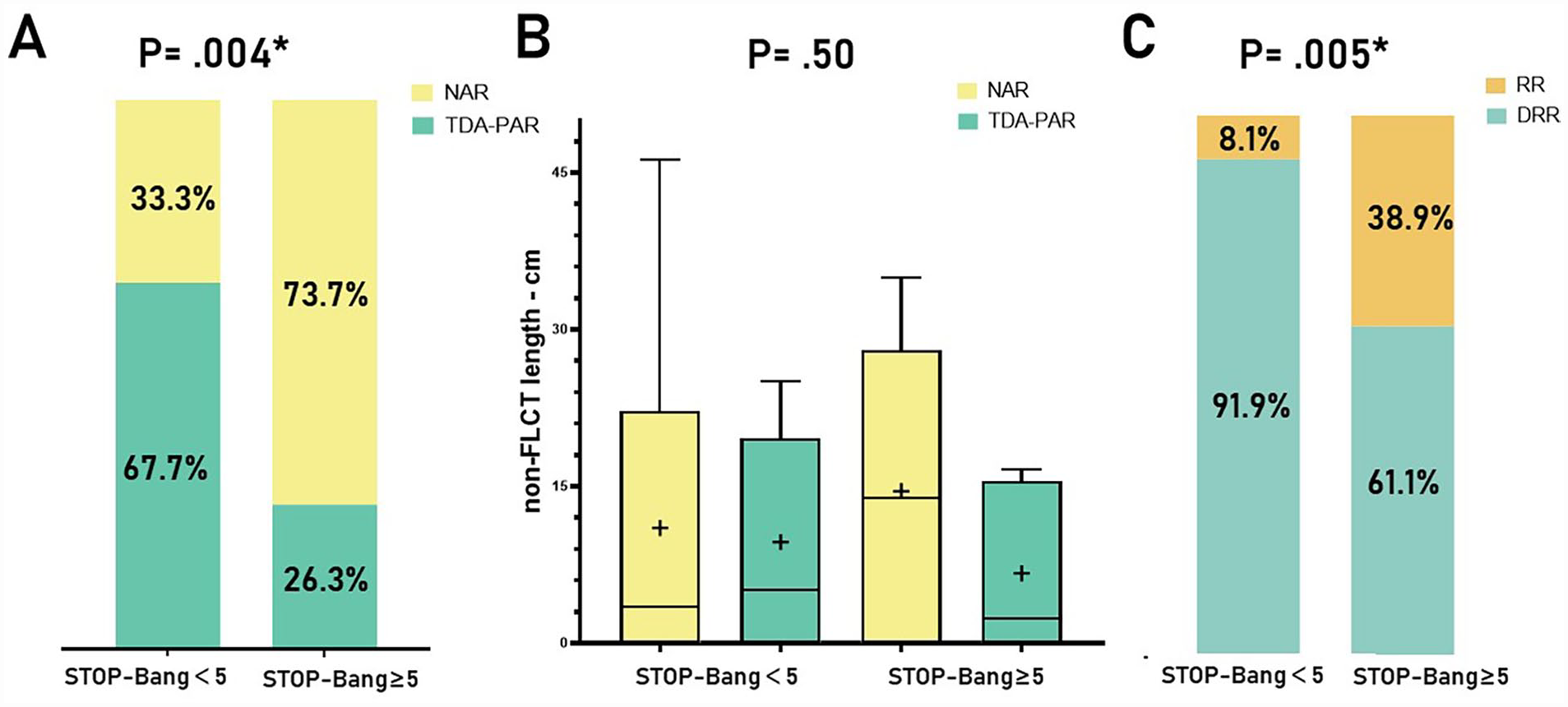
Comparison of aortic remodeling (A), false lumen thrombosis rate (B) and non-FLCT length, and (C) reintervention rates between the STOP-Bang <5 and ≥5 groups. DRR, did not require reintervention; NAR, negative aortic remodeling; non-FLCT, non-false-lumen complete thrombosis; RR, required reintervention; TDA-PAR, total descending aorta-positive aortic remodeling.
Aortic Remodeling at 1-Year Follow-up After TEVAR.
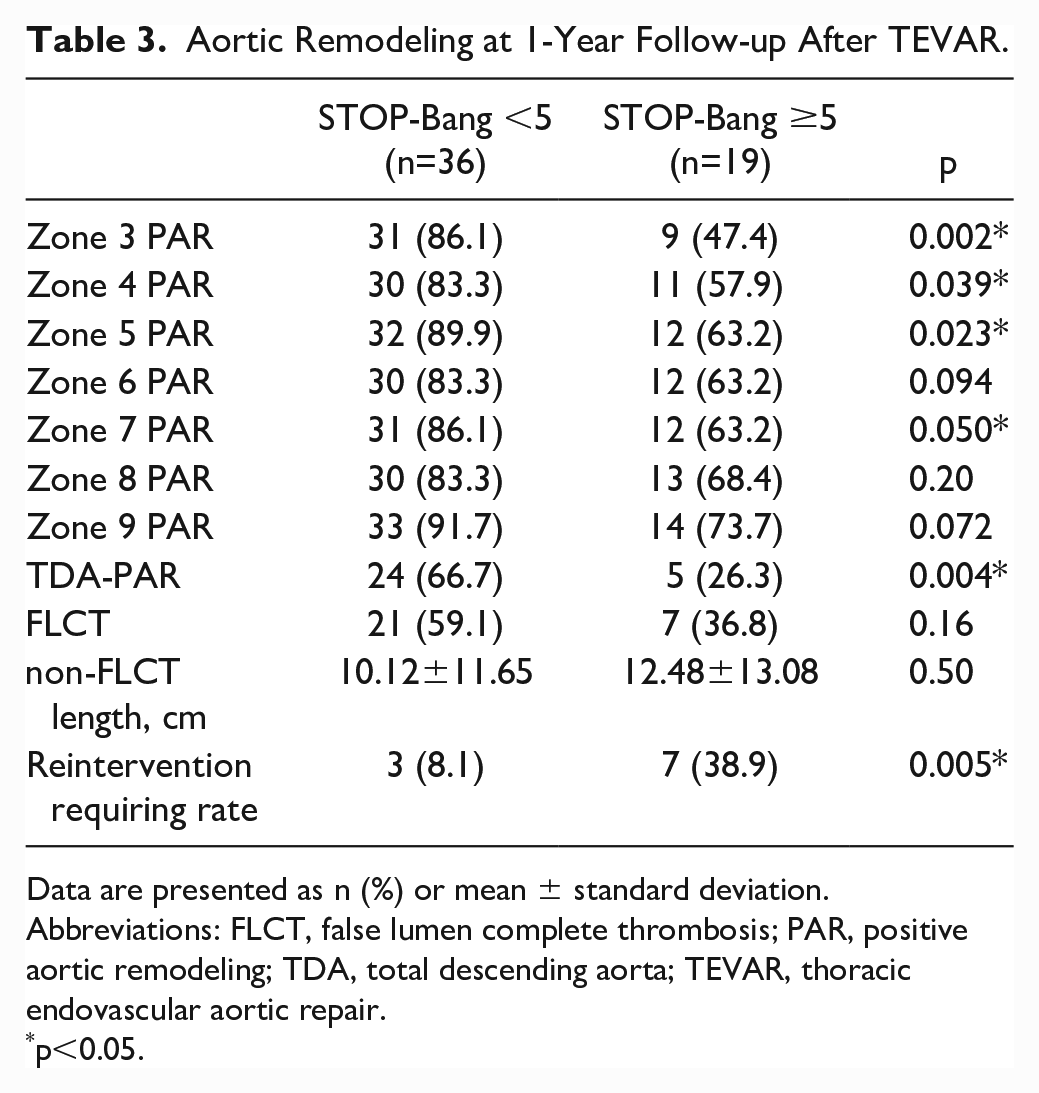
Data are presented as n (%) or mean ± standard deviation.
Abbreviations: FLCT, false lumen complete thrombosis; PAR, positive aortic remodeling; TDA, total descending aorta; TEVAR, thoracic endovascular aortic repair.
p<0.05.
Patients in the STOP-Bang <5 group achieved a relatively high PAR throughout the descending aorta. Although patients in the STOP-Bang ≥5 group had a worse PAR throughout the descending aorta than those in the STOP-Bang <5 group, the PAR of the thoracic descending aorta in the STOP-Bang ≥5 group appeared to be worse than that in the abdominal aorta (Figure 3). Although the difference in non-FLCT length was not significantly different between the two groups, patients with PAR in the STOP-Bang ≥5 group had lower non-FLCT lengths than those with NAR. Data with p<0.1 in the baseline characteristics (male, BMI, and serum creatinine and low-density lipoprotein concentrations) were included in the logistic regression analysis with STOP-Bang ≥5, and the results showed that STOP-Bang ≥5 (odds ratio: 0.12; 95% confidence interval: 0.03–0.58; p=0.008) was indeed associated with the postoperative TDA-PAR of TBAD patients who underwent TEVAR (Table 4).
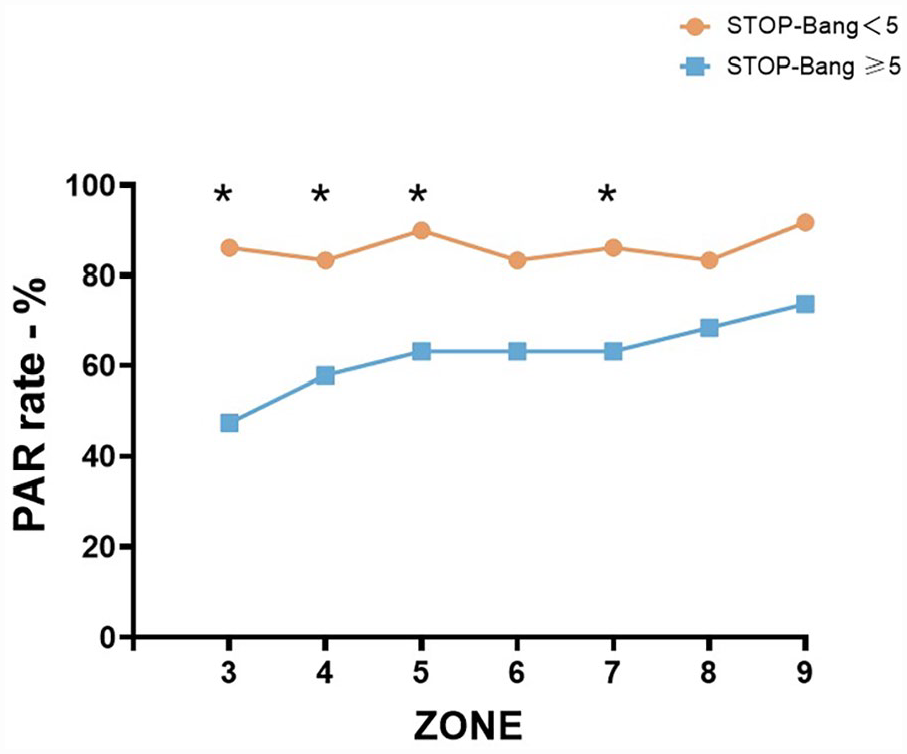
Aortic remodeling in different zones. PAR, positive aortic remodeling.
Multivariate Analysis of Factors of Positive Aortic Remodeling.
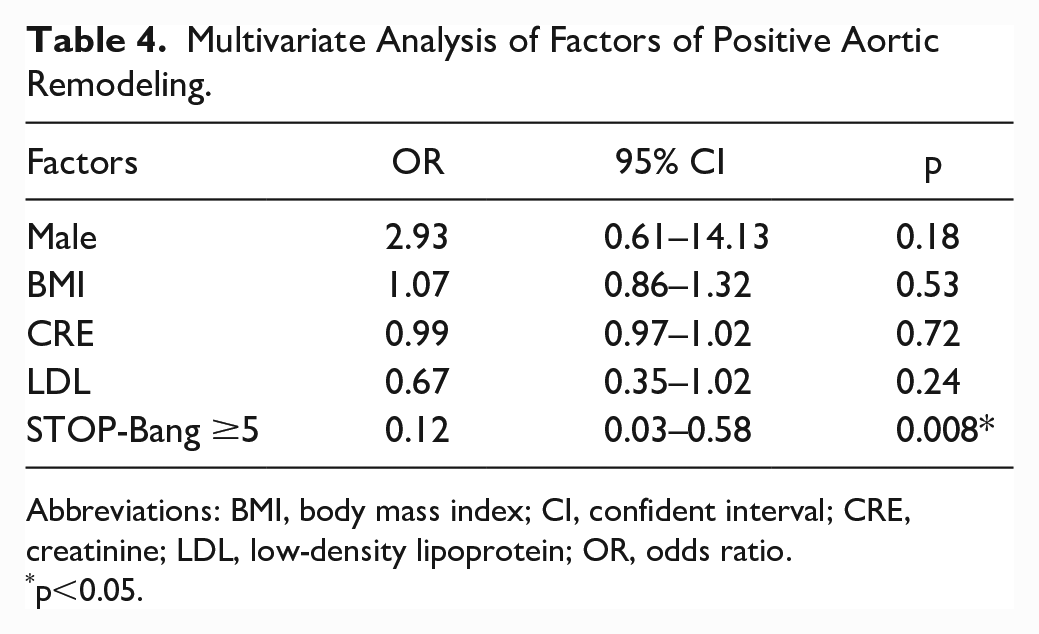
Abbreviations: BMI, body mass index; CI, confident interval; CRE, creatinine; LDL, low-density lipoprotein; OR, odds ratio.
p<0.05.
Survival
Patients in the STOP-Bang <5 group had higher 5-year overall survival than those in the STOP-Bang ≥5 group, but the difference was not statistically significant (51.5 months vs 47 months, respectively; p=0.24). The 5-year survival curves of the patients in both groups are shown in Figure 4. The survival of patients in the STOP-Bang <5 group was consistently longer than that in the STOP-Bang ≥5 group.
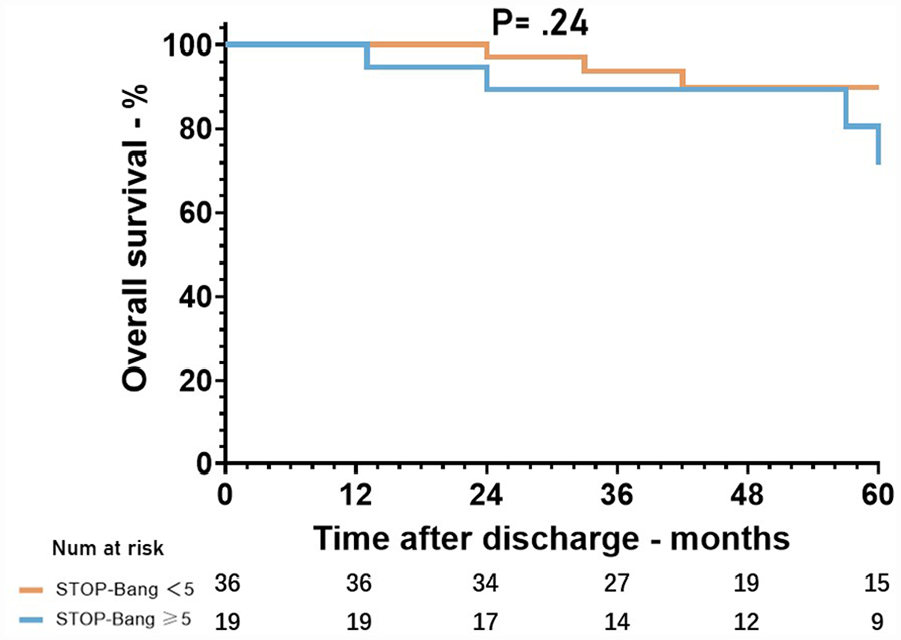
Survival curve of the included patients 5 years after discharge.
Discussion
In the present study, we analyzed PAR in each descending aortic artery zone and TDA-PAR and the FL thrombosis status between patients in the STOP-Bang <5 group and the STOP-Bang ≥5 group and found that aortic remodeling was worse, and the reintervention rate was higher in patients in the STOP-Bang ≥5 group than in patients with STOP-Bang <5. Furthermore, patients with STOP-Bang ≥5 had worse PAR in the thoracic aorta than in the abdominal aorta, and non-FLCT appeared to have a greater effect on aortic remodeling in these patients than in patients with STOP-Bang <5.
Several previous studies have reported on the relationship between OSA and aortic disease. In our study, patients with STOP-Bang ≥5 had worse PAR compared with those with STOP-Bang <5, suggesting that OSA may not only implicate in aortic disease but may also affect aortic remodeling after TEVAR. Patients in the STOP-Bang ≥5 group had poor PAR of the aorta covered by the thoracic stent graft (zone 3–5) and relatively good remodeling of the abdominal uncovered stented aortic segment instead, which may imply the presence of specific mechanisms leading to persistent enlargement of the FL in patients with OSA. The pathological mechanisms underlying the impact of OSA on the thoracic aorta mainly include intrathoracic pressure changes leading to shear stress on artery walls, intermittent hypoxia leading to oxidative stress and sympathetic stimulation, and arousal-induced sympathetic activation with subsequent repetitive blood pressure surges.13–15 The combined effect of these mechanisms ultimately leads to fibrinolytic imbalance and chronic hypertension, which may synergistically affect remodeling after TEVAR in patients with OSA. 8
Long-term remodeling of AD is related to thrombosis of the FL.16,17 Although aortic PAR did not occur exclusively in patients with FLCT, aortic remodeling was better in patients with FLCT than that in patients with FL partial thrombosis or patency. 18 Some studies have suggested that severe OSA is associated with FL patency and FL expansion in TBAD patients.19,20 Although not significant, in the current study, a lower proportion of patients in the STOP-Bang ≥5 group had FLCT compared with the STOP-Bang <5 group, and patients in the STOP-Bang ≥5 group who achieved TDA-PAR had a somewhat shorter non-FLCT length than the patients with NAR (Figure 2).
In this study, patients in the STOP-Bang <5 group had longer overall survival than those in the STOP-Bang ≥5 group although the difference was not statistically significant. However, the survival of patients in the STOP-Bang <5 group was consistently longer than that of patients in the STOP-Bang ≥5 group, indicating the possibility that the survival rate of patients in the STOP-Bang <5 group was higher than that in the STOP-Bang ≥5 group. However, the insufficient sample size resulted in a difference that was not statistically significant. Our study focused on the aortic remodeling of TBAD patients after TEVAR; therefore, patients who died perioperatively and those who died within 1 year were excluded because they did not undergo 1-year CTA, which may have created bias regarding overall survival in this study.
Clinically, we usually perform standard TEVAR to cover the entry tears in patients with acute TBAD. After TEVAR, coexisting distal entry tears persist in some patients, resulting in incomplete disappearance of FL flow and even continued progression of the FL, which becomes a common reason for reinterventions after TEVAR. Thoracic endovascular aortic repair protects the aorta only in the area covered by the stent; if distal tears are present and the flow rate through the distal tears is rapid, this may affect FL thrombosis and aortic remodeling. 21 Early additional interventions with standard TEVAR may improve the outcomes of patients with TBAD. 22 Several adjunct techniques have been used for FL obliteration after TEVAR, and the use of these techniques has been reported to be beneficial in selected patients.23–26 In the present study, patients in the STOP-Bang ≥5 group had a high reintervention rate, with more than one-third of the patients requiring secondary intervention after the initial TEVAR. Therefore, our study suggests that adjunct interventions with standard TEVAR for patients with TBAD in the STOP-Bang ≥5 group might improve long-term outcomes for these patients and avoid potential reinterventions. A potentially controversial aspect is that polysomnography was not performed in this study. Instead, the STOP-Bang questionnaire was used, which might lead to errors in the diagnosis of OSA. Because the purpose of this study was to analyze the association between the STOP-Bang questionnaire and aortic remodeling after TEVAR, this point may not have a significant impact.
The present study had limitations. First, this was a single-center retrospective study with a small sample size, which might have introduced bias. Second, patients were followed up for a relatively short period of time, and some perioperative deaths or short-term postoperative deaths were excluded, which could also have introduced bias. Third, this study lacked an analysis of the FL thrombosis in each zone and an analysis of the entry tears (size and location of main entry tear, number of re-entries).
Conclusion
The STOP-Bang questionnaire score is associated with aortic remodeling after TEVAR in patients with acute TBAD. For patients with STOP-Bang scores ≥5, it may be beneficial to increase the frequency of surveillance after TEVAR.
Footnotes
Acknowledgements
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by Natural Science Foundation of Fujian Province (2020J01960).
Availability of Data and Materials
All data generated or analyzed during this study are included in this article.