
Abstract
Purpose:
Patients undergoing carotid endarterectomy (CEA) or carotid artery stenting (CAS) are at substantially increased risk of short-term and long-term cardiac complications. Still, the role of perioperative troponin in predicting cardiac events remains unclear. The objective was to systematically summarize the existing evidence on the topic and provide directions for further research.
Materials and Methods:
Studies that examined perioperative troponin values and its association with myocardial injury, and/or myocardial infarction (MI), and/or major adverse cardiac events (MACE) and postoperative mortality in exclusively CEA/CAS patients, published in English until March 15, 2022, were retrieved through a systematic search of MEDLINE and Web of Science. The study selection process was independently performed by 2 authors, while the third researcher resolved disagreements.
Results:
Four studies with 885 participants met the inclusion criteria. Age, chronic kidney disease, presentation of carotid disease, type of closure (primary closure/venous patch/Dacron/polytetrafluoroethylene patch), coronary artery disease, chronic heart failure, and the long-term use of calcium channel blockers represent risk factors for troponin elevation, which occurred in 11% to 15.3%. Myocardial infarction and MACE occurred in 23.5% to 40%, that is, 26.5% of patients with troponin elevation, respectively, during the first 30 postoperative days. Elevated postoperative troponin levels were significantly associated with adverse cardiac events during the long-term surveillance period. The rates of cardiac-related and all-cause mortality were higher in patients with postoperative troponin elevation.
Conclusion:
Troponin measurement could be helpful in the prediction of adverse cardiac events. The predictive role of preoperative troponin, the patient population in whom routine troponin sampling should be used, and a comparison of different treatment methods/anesthesia techniques in carotid patients should be further examined.
Clinical Impact
The present scoping review critically appraises the extent and nature of the existing literature data on the predictive value of troponin on the occurrence of cardiac complications in patients undergoing CEA and CAS. In particular, it provides clinicians with essential insights by systematically summarizing the core evidence and identifying knowledge gaps that may direct future research. This, in turn, may significantly alter the current clinical practice and perhaps even reduce the incidence of cardiac complications in patients undergoing CEA/CAS.
Keywords
Introduction
Cardiac troponins are among the most commonly measured biomarkers. 1 The fact that modern definitions of myocardial injury and infarction rely on troponin measurement justifies the recommendation for routine clinical use of those biomarkers. 2 Their usefulness is particularly apparent during the perioperative period. Numerous large-scale studies have shown that troponin elevation following noncardiac surgery strongly predicts cardiac complications and its association with an increased short-term and long-term mortality rate.3–8 Furthermore, due to the predominantly silent presentation of myocardial injury,9,10 which is strongly associated with adverse cardiac events, the role of troponin is even more significant.
More than a decade ago, it was demonstrated that vascular patients are susceptible to the development of perioperative myocardial ischemia and myocardial infarction (MI). 11 The rates of those complications and mortality of vascular patients remain high even today.12–14 Besides the high prevalence of concomitant carotid and coronary artery disease, 15 carotid stenosis represents an independent predictor of cardiac-related death. 16 Consequently, patients undergoing carotid endarterectomy (CEA) or carotid artery stenting (CAS) are at substantially increased risk of short-term and long-term cardiac complications,17,18 with a 5-year survival rate of 56%. 19 Bearing in mind that more than half of the patients undergoing CEA have silent myocardial ischemia, which increases the risk of late cardiac adverse events, 20 perioperative troponin measurement may be helpful in the identification of patients at risk. On the other hand, there is even less research on the role of perioperative troponin measurement in predicting cardiac events in CAS patients. Although numerous studies have investigated this issue in various surgical fields when it comes to carotid patients, contemporary literature data are limited. Thus, the present review seeks to answer the question: “What is the value of troponin measurement following CEA/CAS and its association with adverse cardiac events?”
Materials and Methods
Study Design and Registration
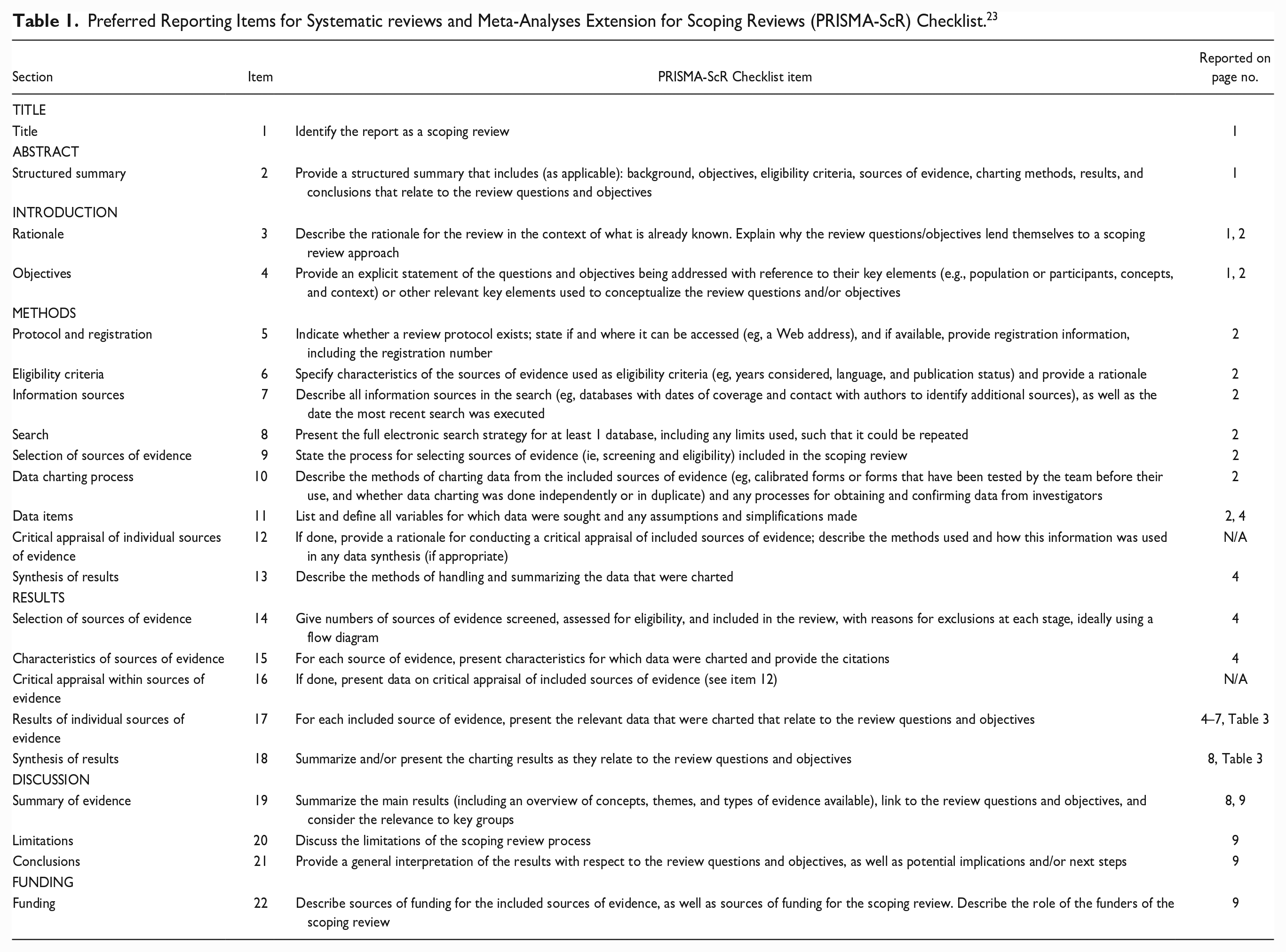
The design of this review was guided by the methodological guidance suggested by the Joanna Briggs Institute, 21 while reporting was in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) (Table 1).22,23 The research protocol was registered with the Open Science Framework (10.17605/OSF.IO/JV2UZ).
Preferred Reporting Items for Systematic reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) Checklist. 23
Eligibility Criteria
Original studies that examined preoperative and postoperative troponin elevation and its association with cardiac events (myocardial injury and/or MI), other major adverse cardiac events (MACE), and postoperative mortality in carotid patients were of interest for the present review. To be included, the article had to be a cohort study (prospective or retrospective), published until March 15, 2022, to have included only patients who underwent CEA/CAS, in all of whom routine troponin sampling was used, and to have evaluated the association of troponin elevation with adverse cardiac events during both short-term and long-term follow up. Studies that investigated cohorts other than carotid patients (including cohorts in which this group could not be clearly separated), were published in languages other than English, belonged to different study types, and evaluated the predictive effects of troponin in combination with other biomarkers (mutually) were excluded.
Information Sources and Search Strategy
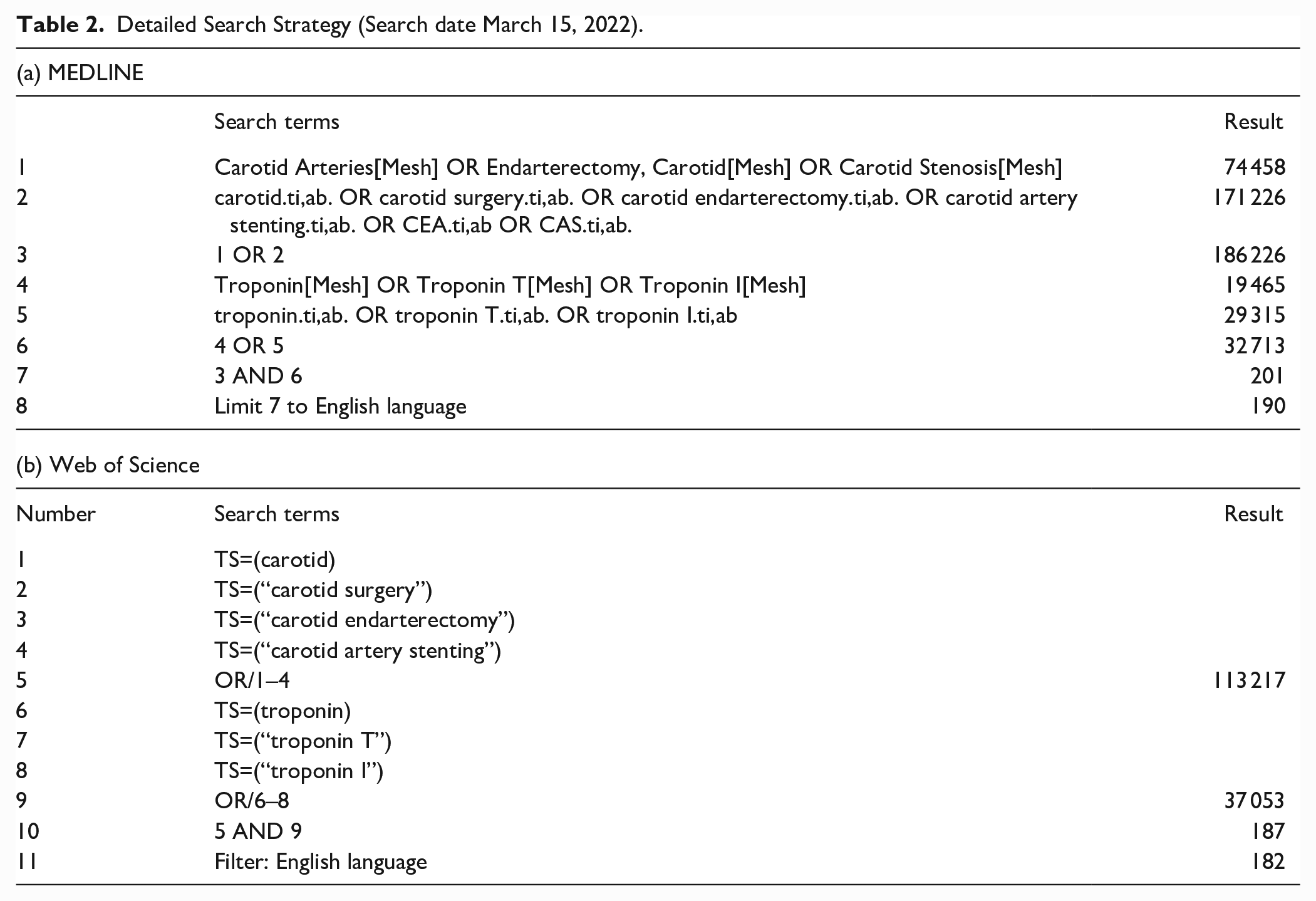
The studies of interest were retrieved from MEDLINE and Web of Science. Our search strategy included a combination of the following MeSH terms and keywords: “carotid,” “carotid surgery,” “carotid endarterectomy,” “carotid artery stenting,” “CEA,” “CAS,” “troponin,” “troponin T” and “troponin I,” with the application of Boolean operators OR and (Table 2). We did not contact experts in the field to obtain new data.
Detailed Search Strategy (Search date March 15, 2022).
Study Selection Process
To ensure reliability, the study selection process was independently performed by 2 authors, and disagreements were resolved in a constructive discussion with a third researcher, who made the final decision. Following the initial reading of the title and abstract and the exclusion of unsuitable articles, the remaining articles were screened in full. Studies that met the predetermined inclusion criteria were included. To retrieve further studies, the reference lists of the full-text articles were checked for suitability.
Data Collection Process and Data Items
Two authors conducted the data collection process independently using a data extraction form designed and piloted prior to use. The following data were collected from each article: author(s), publication date and country, study design, sample size, type of carotid procedure and anesthesia, timing and type of troponin measurement, duration of follow-up, main outcomes, key findings, and limitations.
Synthesis of Results
The main results of included studies and their relation to the present review’s research question were narratively summarized.
Results
Search Results and Study Selection
Details of the study selection process are presented in the PRISMA flow diagram 24 (Figure 1). The initial search of databases retrieved a total of 372 studies. After removing 134 duplicates, 238 articles were eligible for the title and abstract screening. A total of 53 articles were eligible for full-text screening. The screening of the reference lists of the full-text articles retrieved no additional eligible articles. In concordance with the exclusion criteria, 41 articles were excluded, while 8 articles were irrelevant to the review question. Finally, a total of 4 studies were included in the present review.
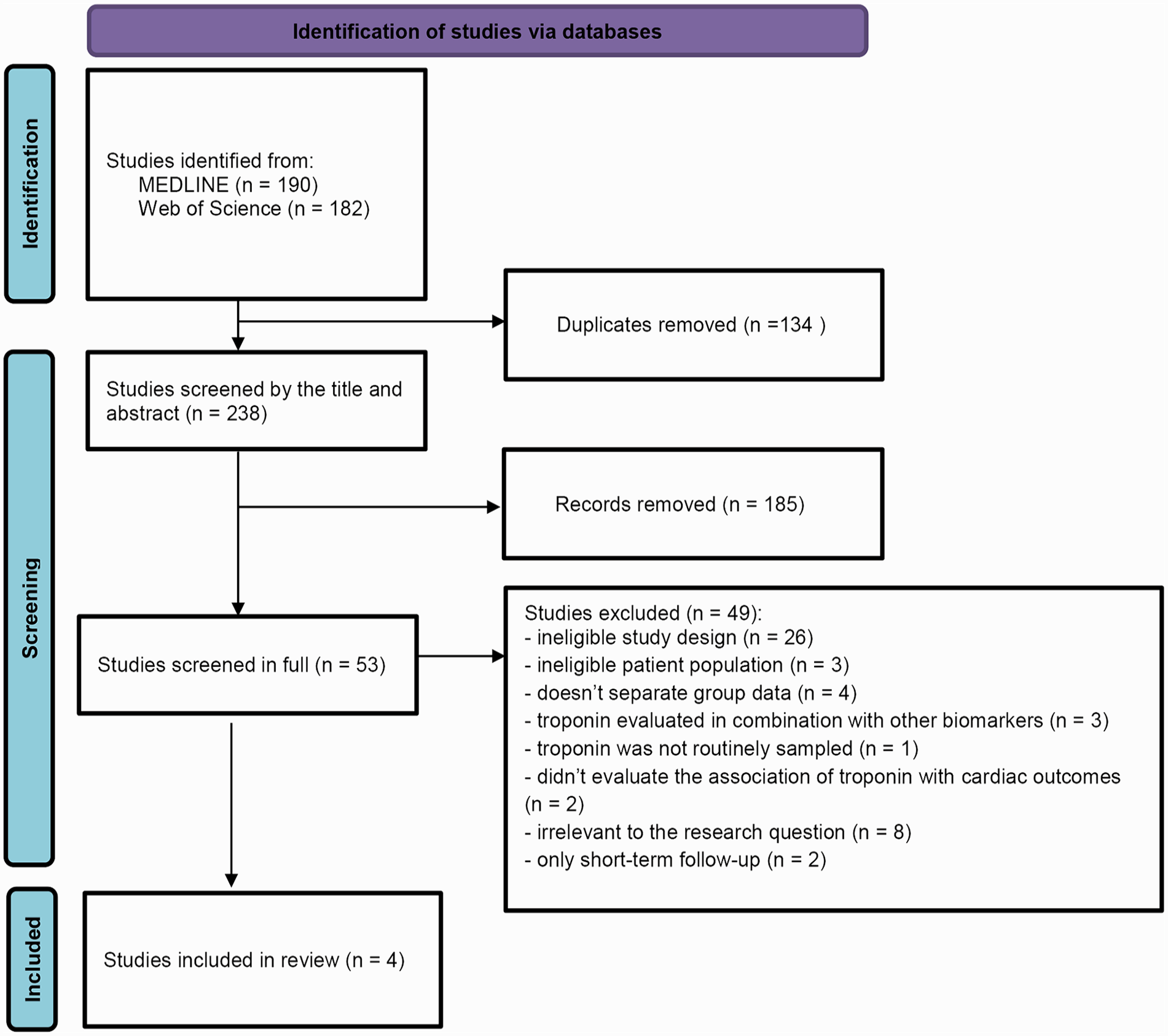
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram for observational studies reporting the process of identification, review, eligibility, and inclusion or exclusion of the studies.
Characteristics of the Included Studies
Of the 4 studies included in the present review,17,18,25,26 only 1 study was published in the last 5 years, 17 2 were prospective,25,26 and troponin measurement was performed both preoperatively and postoperatively only in 1 study. 25 Although inclusion and exclusion criteria were similar across the studies, only 1 study 26 included both CEA and CAS patients. Both general and regional anesthesia (RA) techniques were used. Only 1 study 17 defined MI and injury according to the up-to-date definition, 27 while the remaining18,25,26 used the older definitions (contemporary at the time of publication). The most commonly reported outcomes were myocardial injury, MI, MACE, and all-cause mortality. The time points at which these outcomes were evaluated varied in a range from 30 days (short-term) up to 5 years (long-term) (Table 3).
The Main Characteristics of the Included Studies.
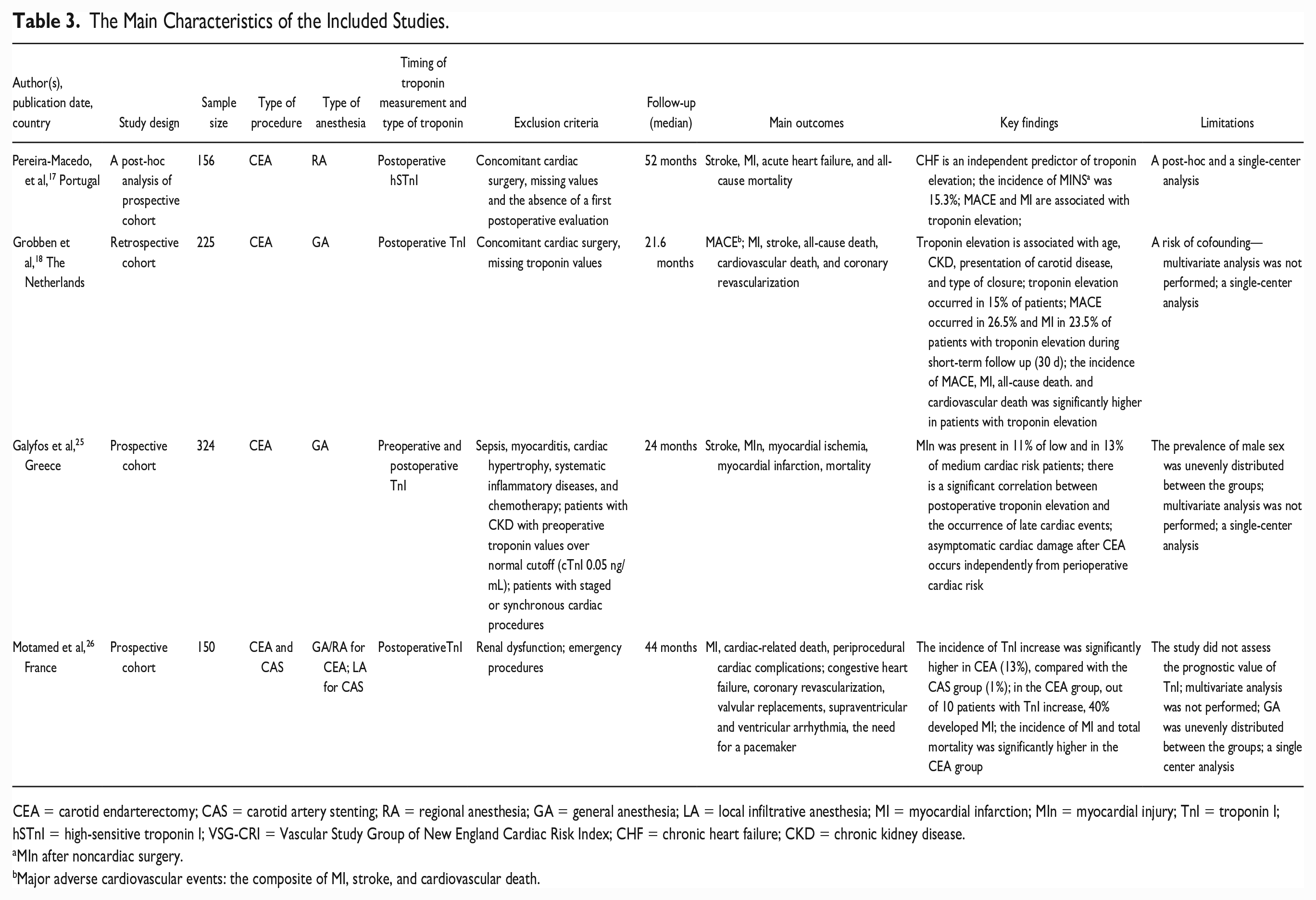
CEA = carotid endarterectomy; CAS = carotid artery stenting; RA = regional anesthesia; GA = general anesthesia; LA = local infiltrative anesthesia; MI = myocardial infarction; MIn = myocardial injury; TnI = troponin I; hSTnI = high-sensitive troponin I; VSG-CRI = Vascular Study Group of New England Cardiac Risk Index; CHF = chronic heart failure; CKD = chronic kidney disease.
MIn after noncardiac surgery.
Major adverse cardiovascular events: the composite of MI, stroke, and cardiovascular death.
Results of Individual Studies
A post hoc analysis of the prospective cohort by Pereira-Macedo et al 17 assessed the incidence of myocardial injury after noncardiac surgery (MINS) and the prognostic value of troponin elevation on the occurrence of adverse outcomes (MI, related cardiovascular events, and mortality). The study included a total of 156 (symptomatic and asymptomatic) patients undergoing CEA under RA who were under acetylsalicylic acid (100 mg) and atorvastatin (40 mg) for at least 2 days before the planned procedure. Troponin I () and high-sensitive troponin I (hsTnI) were registered postoperatively (48 hours), while the median follow-up was 52 months. Outcomes of interest were stroke, MI, acute heart failure, and all-cause mortality, and they were assessed 30 days postoperatively and in the long-term follow-up period. The mean age of patients was 69.6 years, and the majority belonged to the male sex (76.3%). The incidence of MINS, defined according to the Fourth universal definition of MI, 27 was 15.3%. The clinical presentation of carotid disease was not associated with the occurrence of MINS. Troponin elevation was significantly associated with coronary artery disease, chronic heart failure, and long-term use of calcium channel blockers. Still, results of multivariate analysis showed that only chronic heart failure represents an independent predictor of troponin elevation: patients with chronic heart failure have over 4 times greater risk of developing MINS (odds ratio [OR]=4.458, 95% confidence interval [CI]: 1689–11.708, p=0.002). Regarding the prediction value of troponin elevation, no significant differences were noted in the incidence of major outcomes during the short-term follow-up (30 days). Still, during the long-term surveillance period, the prognostic value of this cardiac biomarker was observed: patients with MINS had significantly higher rates of MI and MACE (hazard ratio [HR]: 3.318, 95% CI: 0.97–13.928, p=0.025; HR: 1.955, 95% CI: 1.01–4.132, p=0.046, respectively). However, troponin elevation could not predict the occurrence of stroke and all-cause mortality in this cohort. The authors suggest that troponin levels should be routinely measured following CEA in high-risk patients. The main limitations of this study are reflected in a post hoc, single-center, observational design.
In 2016, Grobben et al 18 investigated the incidence of troponin elevation and its predictive role on the occurrence of long-term adverse cardiovascular events in patients following CEA under general anesthesia (GA). The study included a total of 225 patients who were under dual antiplatelet therapy. TnI was postoperatively measured in all patients, and the median follow-up was 1.8 years. The primary outcome was MACE (the composite of MI, stroke, and cardiovascular death), while MI, stroke, all-cause mortality, cardiac-related mortality, and coronary revascularization rates were also assessed. The mean age of patients was 73 years, and the majority were men (72.9%). Only 10.2% of patients were asymptomatic, while the rest presented with stroke, transient ischemic attack (TIA), or ocular symptoms. Troponin elevation occurred in 15% of patients. It was associated with age, renal failure (glomerular filtration rate <45 mL/min), the clinical presentation of carotid disease, and type of closure (primary closure/venous/Dacron/ polytetrafluoroethylene [PTFE] patches). There was a statistically significant difference in clinical presentation between patients with and without troponin elevation. In patients with elevated troponin, stroke was the most common clinical presentation, while TIA was the most common symptom in the other group. Primary closure was significantly more often applied in patients with troponin elevation, while venous patch and Dacron/PTFE patch were less frequently used in this patient group. Postoperative hypertension occurred more commonly in patients with troponin elevation. Major adverse cardiac events and MI occurred more frequently in patients with postoperative troponin elevation compared with those with normal troponin levels (26.5% vs 2.6%, p<0.001; 23.5% vs 0%, p<0.001, respectively), not just during a short-term follow-up period but also during long-term surveillance (29.4% vs. 6.3%, p<0.001; 23.5% vs. 1.6%, p<0.001, respectively). Furthermore, postoperative troponin elevation was significantly associated with cardiovascular death (HR: 11.8, 95% CI: 1.1–131) and all-cause mortality (HR: 3.0, 95% CI: 1.0–8.7). In this single-center study, the association between elevated troponin levels and main outcomes may be confounded by some risk factors as the multivariate analysis was not performed.
In 2015, a prospective cohort study by Galyfos et al 25 evaluated the incidence of postoperative cardiac damage, defined as TnI elevation, among patients with various cardiac risk, examined the incidence of cardiac complications, and assessed the long-term cardiac outcome. A total of 324 CEA patients, operated on under the conditions of GA and the usage of routine shunting, who were under statin, antiplatelet, and antihypertensive therapy, were included in the study. Troponin I was measured preoperatively and postoperatively, and the median follow-up was 2 years. A total of 165 patients (50.9%) presented with TIA/amaurosis fugax or stroke before surgery. The primary outcomes included stroke, myocardial injury, myocardial ischemia, MI, and mortality. The mean age of patients was 67.3 years, and the majority were men (64%). Myocardial injury was present in 11% of low and 13% of medium cardiac-risk patients; none of the high-risk patients had troponin elevation. During the follow-up period, 67% of patients with postoperative troponin elevation experienced MI. A significant correlation between postoperative troponin elevation and late cardiac events was found. The authors suggested that postoperative troponin evaluation should be used in all patients undergoing CEA. In this single-center study, a multivariate analysis was not performed due to the low incidence of events.
In 2005, Motamed et al 26 published a prospective cohort study that evaluated the incidence of short-term and long-term cardiac complications in relation to postoperative TnI values and compared them between CEA/CAS patients. The study included 150 CEA/CAS patients operated on under GA and RA, that is, local infiltrative anesthesia. Prior neurologic symptoms were recorded in 80 patients (53.3%). The median follow-up was 44 months. The outcomes of interest were MI, cardiac-related death, periprocedural cardiac complications, congestive heart failure, coronary revascularization, valvular replacements, supraventricular and ventricular arrhythmia, and the need for a pacemaker. The mean age of patients was 71 years, and the majority were men (81.3%). The incidence of TnI increase during short-term follow-up was significantly higher in CEA compared with the CAS group (13% vs 1%, p=0.02). In the CEA group, out of 10 patients with TnI increase, 40% developed MI postoperatively. Regarding long-term cardiac events, the incidence of MI and total mortality was significantly higher in the CEA group (20% vs 5%, p<0.01). The CAS patients had a significantly lower incidence of major cardiac events and cardiac-related death than patients undergoing CEA (p=0.003, HR: 5.3). It should be noted that some of those differences, especially during the long-term follow-up, might be attributed to the fact that CAS patients had a clopidogrel/aspirin combination in the first month, which was not administered in all CEA patients. This single-center study did not assess the predictive value of TnI, multivariate analysis was not performed, and GA was unevenly distributed between the groups.
Synthesis of Results
The sample size ranged from 150 to 324 patients, while the total number of patients in the included studies was 885. The total average age of participants from the included studies was 67.5 years. In all the included studies, the male sex was more prevalent. Age and sex were not predictors of troponin elevation in 3, while 1 study showed that troponin elevation was significantly associated with older age. 18 Regarding preoperative cardiac status, preoperative cardiac risk factors were very similar in the included studies. For instance, the incidence of preoperative hypertension varied from 80% 26 to 85% 17 of patients, while diabetes mellitus was present in 16% to 39.7%17,26 of patients. Three of the included studies reported that over half of the patients were smokers.17,25,26 At the same time, dyslipidemia was present in one-third 25 to two-thirds of patients.17,18 In the study by Motamed et al 26 14.7% of patients had a history of MI and 12.7% had a prior coronary intervention, while Grobben et al 18 reported slightly higher percentages: 24.4% and 27.5%, respectively. In 3 of the included studies17,25,26 patients underwent routine preoperative assessment, and no data of additional cardiac assessment (eg, cardiology consultation, transthoracic echocardiography, or preoperative coronarography) were reported. On the contrary, due to angina, cardiac rhythm abnormalities, and ischemia, Grobben et al 18 performed additional cardiac testing in 19 patients (8.5%) (coronary angiography in 1 patient, echocardiography in 7, and exercise test with an echocardiogram in 2 patients). Based on the results of 2 studies,17,18 coronary artery disease, chronic heart failure, long-term use of calcium channel blockers, chronic kidney disease, presentation of carotid disease, and type of closure significantly affected troponin levels. Chronic heart failure is an independent predictor of troponin elevation. 17
The incidence of troponin elevation varied in a range from 11% 25 to 15.3%. 17 Two studies reported that the incidence of MI was 23.5%, 18 that is, 40% 26 in patients with troponin elevation, while MACE occurred in 26.5% of those patients, 18 within 30 days following the procedure. Troponin elevation did not affect the occurrence of stroke during the first 30 postoperative days, according to 2 of the included studies.17,18 In the remaining 2, the stroke rate was 0.25,26
Elevated postoperative troponin levels were significantly associated with adverse cardiac events during the long-term surveillance period, according to the results of 3 included studies.17,18,25 Furthermore, 2 studies have shown that the rate of cardiac-related mortality, as well as the rate of all-cause mortality, was higher in patients with postoperative troponin elevation.18,25 The results of the only study that included CAS patients 26 show that they have a lower incidence of TnI increase and cardiac complications during both short-term and long-term follow-up compared with the CEA group. Still, based on those results, prognostic value of TnI in patients undergoing CAS could not be determined.
Discussion
Although troponins have been the subject of considerable research during past decades, even the largest studies did not provide a clear answer to the question raised in the present review. One possible explanation for this may be the fact that in most such studies, the primary aim was not the assessment of the role of troponins in the prediction of adverse cardiac events but mainly a comparison of 2 methods of carotid revascularization.28,29 For instance, in 2 post hoc analyses of the CREST study30,31—a randomized, controlled trial that included 2052 CEA/CAS patients, elevated levels of cardiac biomarkers were associated with increased long-term mortality. Still, troponin levels were collected in only 60% of patients in combination with other cardiac biomarkers; MI was defined as ≥2-fold elevation of troponin or creatine kinase-MB (CK-MB) with electrocardiogram or clinical evidence of myocardial ischemia, while the “biomarker-positive” group implied an elevation of CK-MB or troponin. These facts explain why CREST and subsequent post hoc analyses cannot provide definitive conclusions regarding the prediction role of troponin.
In the latest version of the European Society for Vascular Surgery Clinical Practice Guidelines on the Management of Atherosclerotic Carotid and Vertebral Artery Disease, 32 one of the unanswered questions was: “Is there a role for routine preoperative and postoperative troponin measurement in CEA or CAS patients?” Thus, we believe the present scoping review represents a first step toward answering that question.
Elevated troponin levels are seen in a significant percentage of patients (up to 15.3%). 17 Almost 1 in every 4 patients with troponin elevation develops an MI 30 days following the procedure. Furthermore, elevated troponin levels are associated with adverse cardiac events during long-term follow-up and, most importantly, with higher mortality rates. This means troponin could predict adverse cardiac outcomes in patients undergoing carotid revascularization.
Still, when it comes to the patient population in whom troponin should be routinely sampled, the findings of the present review and the results of included studies provide only a partial answer. Although age, chronic kidney disease, presentation of carotid disease, type of closure, 18 coronary artery disease, chronic heart failure, and long-term use of calcium channel blockers 17 significantly affected troponin levels, it was found that only chronic heart failure represents an independent predictor of troponin elevation. 17 Still, the included studies did not assess the relationship between additional preoperative cardiology screening and troponin elevation. Thus, future studies should provide a more thorough insight into patients’ and procedure characteristics that influence troponin elevation, that is, to determine the population of patients in whom routine troponin measurement should be used. Also, a cost-effectiveness analysis regarding troponin measurement in carotid patients may be required. As the association between elevated troponin and clinical presentation of carotid stenosis was confirmed in only 1 study, 18 this association should be the subject of future research. Similarly, although diabetes mellitus is associated with worse outcomes in CEA/CAS patients 33 and, at the same time, it represents a well-established risk factor for troponin elevation, 34 none of the included studies have demonstrated the influence of diabetes mellitus on troponin elevation in carotid patients. Thus, we believe that this issue should also be further explored. Also, as the role of preoperative (elevated) troponin in predicting short-term and long-term cardiac adverse events and mortality was evaluated in only 1 study, 17 we may say that this topic currently represents a knowledge gap.
Finally, the difference between the 2 surgical methods of carotid revascularization and different anesthesia techniques in terms of troponin elevation is not sufficiently studied. A study by Motamed et al 26 was the only one that included CAS patients and tried to explore the difference between CEA/CAS patients in terms of perioperative TnI increase. Still, the difference in potential TnI predictive value on the occurrence of cardiac complications between CEA/CAS patients remains unclear and hence represents the direction for further research.
The main limitations of the present review are reflected in the fact that selection bias might be present. The gray literature was not considered, the search strategy included 2 databases, and English language filters were applied. Also, randomized controlled trials were not included as these usually estimate the efficacy of a treatment modality or an intervention and use strict inclusion criteria that may compromise generalizability—hence could not be related to the concept of the present review. Finally, a small number of studies included in the present review may be considered a potential limitation as it may reflect strict inclusion criteria. On the other hand, this limited number of studies denotes relative novelty and the exploratory nature of this scoping review. Still, to the best of our knowledge, this is the first scoping review that addressed such a relevant topic in exclusively carotid patients. A thorough search strategy, unique research question, public protocol registration, and accordance with the up-to-date methodological guidelines represent the true strengths of the present review.
Conclusion
The present scoping review raised several questions that remain (mostly) unanswered. Although a limited number of prospective, single-center trials have shown that elevated troponin levels are associated with short-term and long-term cardiac complications and increased mortality, the exact usefulness of this cardiac biomarker in predicting those events remains unknown. Further prospective, multicenter studies focusing on the predictive role of troponin in patients undergoing carotid revascularization are needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.