
Abstract
Purpose:
The covered endovascular reconstruction of the aortic bifurcation (CERAB) technique offers an alternative for Trans-Atlantic Inter-Society Consensus (TASC) C/D lesions involving the aortic bifurcation. The study aims to evaluate the outcomes of the CERAB technique for extensive aortoiliac occlusive disease (AIOD) using the BeGraft balloon-expandable covered stent (BECS).
Materials and Methods:
This is a physician-initiated, multicenter, retrospective, observational study. Between June 2017 and June 2021, all consecutive patients who underwent the CERAB procedure using the BeGraft stent (Bentley InnoMed, Hechingen, Germany) in 3 clinics were enrolled. Patients’ demographics, lesion characteristics, and procedural results were collected and retrospectively analyzed. Follow-up was done at 1, 6, and 12 months and then annually with clinical examination, ankle-brachial index (ABI), and duplex ultrasound. The primary endpoint was the patency at 12 months. Secondary endpoints included procedural-related complications, secondary patency, freedom from target lesion revascularization (TLR), and clinical improvement.
Results:
In all, 120 patients (64 men) with a median age of 65 years (range: 34–84 years) were analyzed. Most patients had extensive AIOD classified as TASC II C (n=32; 26.7%) or TASC II D (n=81; 67.5%). The median duration of the procedure was 120 minutes (interquartile range [IQR]: 80–180 minutes). All 454 BeGraft stents (137 aortic and 317 peripheral) were successfully delivered and deployed. The overall procedural complication rate was 14 (11.7%). The median hospital length of stay was 5 days (IQR: 3–6 days). All patients improved clinically, and the ABI increased significantly (p<0.05). The median follow-up was 19 months (range: 6–56 months). The primary patency rate, secondary patency rate, and freedom from TLR at 12 months were 94.5%, 97.3%, and 93.5%, respectively.
Conclusions:
The CERAB procedure with BeGraft BECSs has a high technical success rate, favorable patency outcomes, and low morbidity, even in relatively ill patients with extensive AIOD. Prospective randomized studies on the CERAB technique are definitely recommended.
Clinical Impact
This study evaluates the outcomes of BeGraft stents used during the covered endovascular reconstruction of the aortic bifurcation (CERAB) procedure. To date, several balloon-expandable covered stents have been used for this technique with satisfactory results. This study showed the safety and excellent patency of the CERAB technique in extensive AIOD using BeGraft balloon-expandable covered stents.
Introduction
Approximately 202 million people are affected by lower extremity artery disease (LEAD) worldwide. 1 Aortoiliac occlusive disease (AIOD) is a common localization of the symptomatic LEAD requiring a revascularization procedure. 2 According to the Trans-Atlantic Inter-Society Consensus (TASC-II) document, open surgical reconstruction (OSR) with aorto-bifemoral bypass graft placement has been recommended as the standard treatment of choice for extensive AIOD requiring revascularization. 3 This procedure is associated with high patency rates up to 90% at 5 years. 4 However, OSR of AIOD is associated with significantly increased complication and mortality rates.5,6 According to the European Society for Vascular Surgery (ESVS) guidelines, an endovascular-first strategy should be considered when planning a reconstruction for AIOD in patients with severe comorbidities. 1 However, since these recommendations, there have been notable advances in endovascular techniques for TASC II C and D lesions aiming to provide a similar to open surgery long-term patency rate with a lower complication rate. 7 Endovascular treatment of complex AIOD is considered a valid alternative to OSR even in low-risk and young patients. 8
During the last decade, advances in endovascular techniques and devices have allowed the treatment of complex AIOD using totally endovascular procedures. Apart from primary stenting of the iliac arteries, the “kissing stents” configuration is frequently used whenever the aortic bifurcation is involved. However, the long-term results of this technique are still inferior to those achieved with open surgery. 7 The randomized COBEST trial brought some evidence that covered stents are beneficial regarding patency and clinical outcome compared with bare-metal stents (BMS). 9 Endovascular stent-graft technology was also applied as an effective alternative treatment for AIOD with acceptable outcomes. 10 However, only a small series using the AFX unibody stent-graft has been reported. 11
The covered endovascular reconstruction of the aortic bifurcation (CERAB) technique offers an endovascular alternative for complex TASC C/D lesions involving the aortic bifurcation.12,13 Several recent studies have shown satisfactory results of the CERAB technique, with favorable primary and secondary patency rates and technical success rates reaching 95.1% to 97%.13–17 In vitro data suggest that CERAB geometry can reduce radial mismatch compared with nitinol or covered “kissing stents” in the aorta, thereby possibly improving patency. 18 However, the role of different stent designs (self-expanding vs balloon-expandable stents) has yet to be fully analyzed for the CERAB procedure. Despite technical limitations, CERAB has the potential to significantly reduce the mortality associated with the treatment of TASC-D lesions.7,19 Minimally invasive procedures such as CERAB are also beneficial in the era of the COVID-19 crisis as a way to shorten hospital stays and the need for intensive care unit (ICU) hospitalization. 20 Nevertheless, there is a lack of multicenter real-world prospective studies and long-term results.
This study reports a multicenter experience with the CERAB technique in the treatment of advanced AIOD. The purpose of the study was to evaluate the results of CERAB using BeGraft balloon-expandable covered stents.
Materials and Methods
Study Design and Data Collection
This is a physician-initiated, multicenter, retrospective, observational study. The “Strengthening the Reporting of Observational Studies in Epidemiology” (STROBE) guidelines were used in the analysis of collected data. Consecutive patients who underwent the CERAB procedure due to AIOD in 3 high-volume vascular centers between June 2017 and June 2021 were prospectively collected in a database and retrospectively analyzed.
Indication for treatment included the presence of extensive AIOD and symptoms of chronic LEAD, either disabling intermittent claudication (IC) or chronic limb-threatening ischemia (CLTI). Anatomical suitability for the CERAB procedure was assessed using computed tomography angiography (CTA). The clinical status of symptomatic patients was evaluated and graded according to the Rutherford-Baker classification for chronic ischemia. 21
Demographic data, medical history, clinical status, procedural data, perioperative complications, and follow-up information were collected and analyzed. The morphology of atherosclerotic lesions was analyzed and scored according to the TASC-II guidelines. 3 After clinical evaluation, all patients underwent duplex ultrasound (DUS) with ankle-brachial index (ABI) measurement. The Ethics Committee approval was waived due to the retrospective character of the study, and written informed consent for the procedure was obtained from each patient.
Technique
All CERAB procedures were performed in a hybrid operating theater under local, regional, or general anesthesia. A detailed description of the CERAB technique was previously published.12,13 In this observational study, all patients with AIOD were treated by implantation of the BeGraft balloon-expandable covered stents (BECSs) (Bentley InnoMed, Hechingen, Germany) using transfemoral vascular access (Figure 1). In case of unsuccessful retrograde recanalization, additional left brachial artery access was obtained for the anterograde approach. Following endovascular treatment of the aortoiliac lesions, in some cases, additional surgical procedures such as femoral endarterectomy with or without patch closure were performed. Completion angiography was performed to assess the appropriate stent deployment, successful revascularization, and procedural complications (Figure 1B). All patients received statin and dual antiplatelet therapy for at least 6 months postoperatively (clopidogrel and acetylsalicylic acid), after which single antiplatelet and statin therapy was continued.
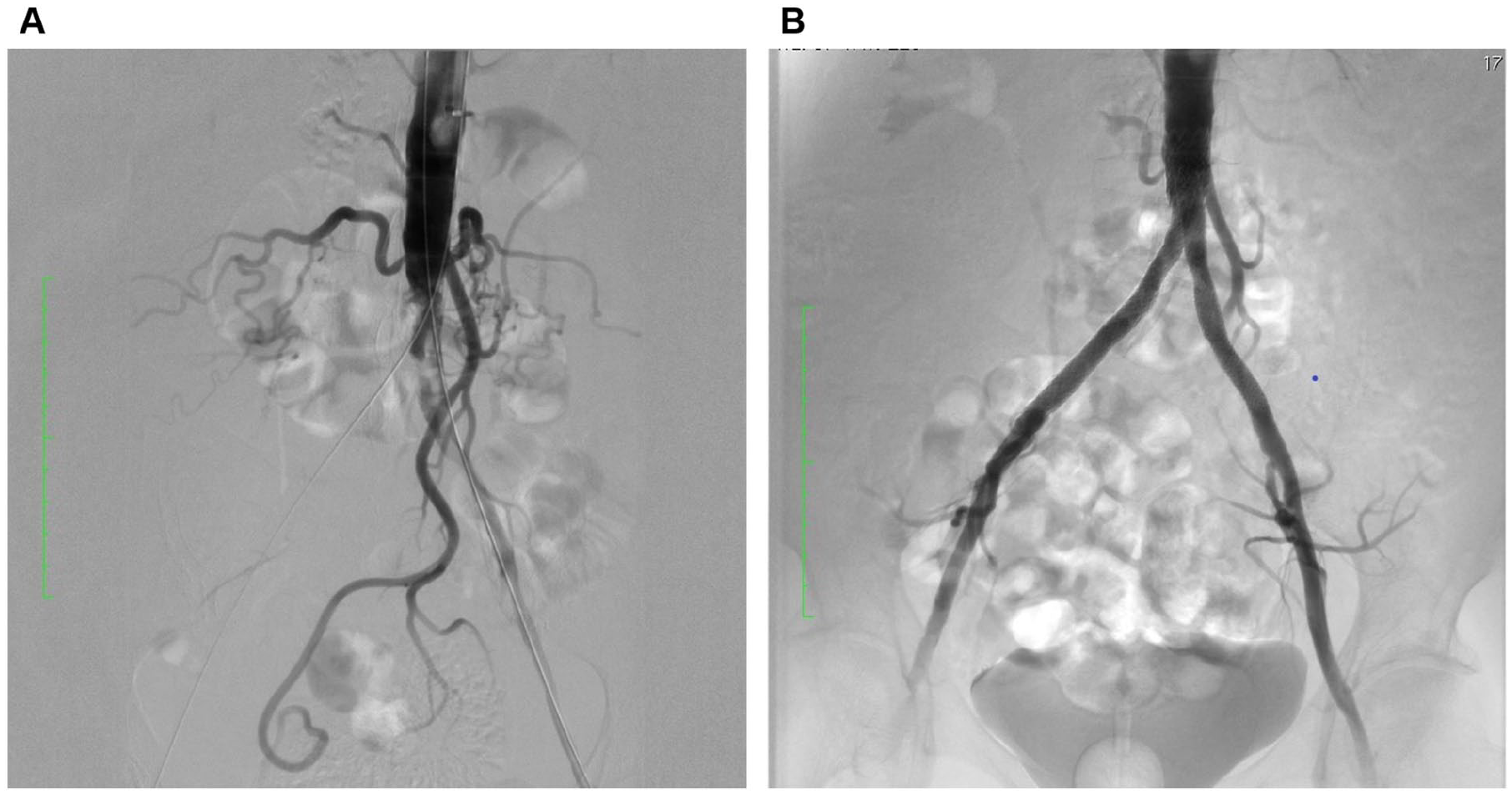
A 74-year-old patient with chronic lower extremity ischemia (Rutherford 4). (A) Initial procedural angiography demonstrates extensive aortoiliac occlusive disease (AIOD) with severe calcification in the aortic bifurcation. (B) Final arteriography after covered endovascular reconstruction of the aortic bifurcation (CERAB) procedure with 1 BeGraft aortic 16.0 × 58.0 mm stent and 2 BeGraft peripheral 9.0 × 57.0 mm stents.
Definitions and Follow-up
The primary endpoint of the study was primary patency at 12 months. Secondary endpoints included procedure-related complications (30-day morbidity and mortality), secondary patency, freedom from target lesion revascularization (TLR), and clinical improvement. Follow-up examinations were scheduled within 30 days following intervention, at 6 and 12 months, and then annually over 5 years with clinical assessment and DUS with ABI evaluation. Computed tomography angiography was performed if indicated by clinical suspicion of symptom recurrence.
Primary patency was defined as the duration of stent patency without any reintervention and was determined by Doppler ultrasound (DUS). Restenosis was defined as a peak systolic velocity ratio (PSVR) ≥2.5 as measured in the endograft and proximal or distal to the endograft. Secondary patency was defined as the duration of patency of the treated segment after successful reintervention. Target lesion revascularization was defined as any endovascular reintervention of the target lesion due to restenosis/reocclusion during the follow-up period. Clinical improvement was defined as an increase of at least 1 Rutherford category, whereas hemodynamic improvement was defined as ABI increase of at least 0.1.
Statistical Analysis
Continuous variables were tested for normality using the Shapiro-Wilk test. The obtained data were presented as mean ± SD in a case of a normal distribution or as median and interquartile range (IQR) in other distributions. Categorical variables are presented as counts and percentages. In all patients, the mean ABI of both legs was calculated, and the difference was preoperatively and postoperatively assessed with a paired t test. Outcomes such as patient survival, target vessel patency, and freedom from TLR were assessed over the 2 years with Kaplan-Meier survival analyses. A 2-sided p value <0.05 was considered statistically significant. All statistical analyses were conducted with GraphPad Prism 9.0 (GraphPad Software Inc, La Jolla, California).
Results
Study Population and Preoperative Data
During the study period, 120 consecutive patients (64 men and 56 women) who underwent elective CERAB procedures were included and retrospectively analyzed. The median age of the study group was 65 years (range: 33–84 years). Baseline characteristics of the patients and comorbidities are presented in Table 1. All patients with symptoms of IC were initially treated conservatively with exercise therapy. The median resting ABI in the most severely affected limb at baseline was 0.6 (range: 0.2–0.8).
Baseline Characteristics of 120 Patients Treated With CERAB Technique.
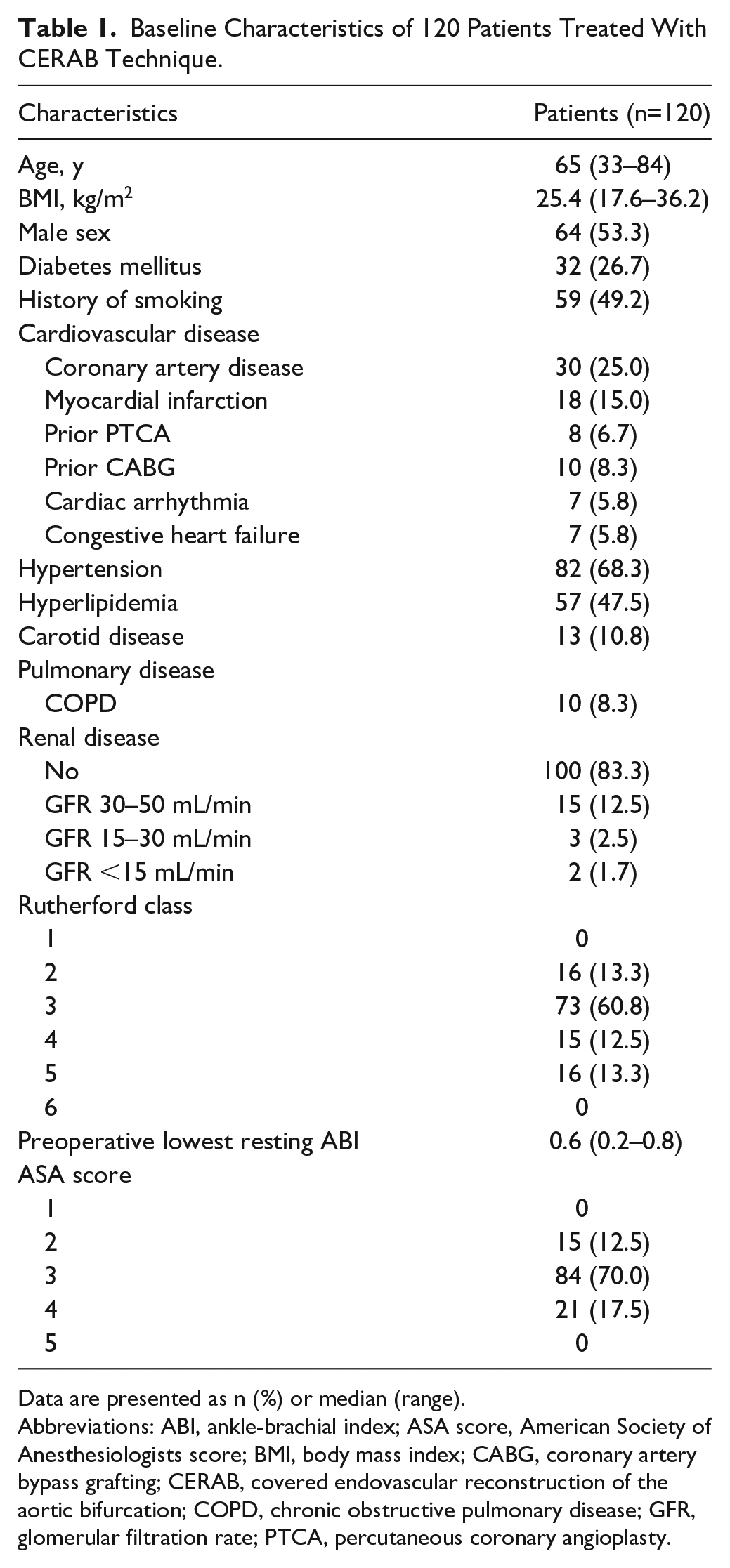
Data are presented as n (%) or median (range).
Abbreviations: ABI, ankle-brachial index; ASA score, American Society of Anesthesiologists score; BMI, body mass index; CABG, coronary artery bypass grafting; CERAB, covered endovascular reconstruction of the aortic bifurcation; COPD, chronic obstructive pulmonary disease; GFR, glomerular filtration rate; PTCA, percutaneous coronary angioplasty.
Most of the patients had extensive aortoiliac atherosclerotic lesions, either severe stenosis or chronic aortoiliac total occlusions (40.0%) with moderate to severe calcification levels. Preoperative CTA showed in 32 (26.7%) cases of TASC II C and 81 (67.5%) cases of TASC II D lesions. In 17 patients (14.2%), a concomitant penetrating abdominal aortic ulcer (PAU) was diagnosed. The preoperative CTA anatomical and lesion characteristics are shown in Table 2.
Anatomical Characteristics at Baseline in 120 Patients Treated With CERAB Technique.
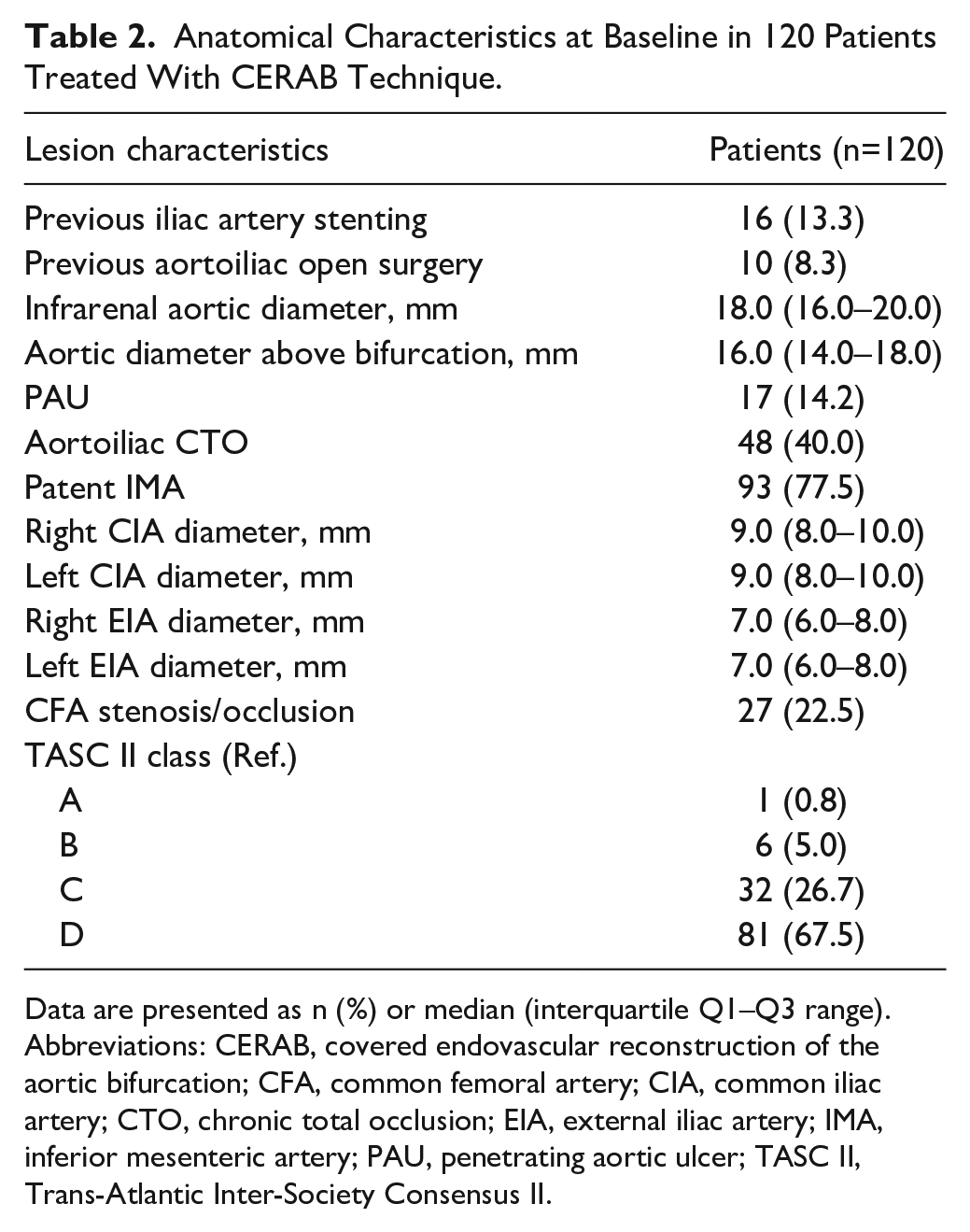
Data are presented as n (%) or median (interquartile Q1–Q3 range).
Abbreviations: CERAB, covered endovascular reconstruction of the aortic bifurcation; CFA, common femoral artery; CIA, common iliac artery; CTO, chronic total occlusion; EIA, external iliac artery; IMA, inferior mesenteric artery; PAU, penetrating aortic ulcer; TASC II, Trans-Atlantic Inter-Society Consensus II.
Procedural Results
Most procedures were performed under local/regional anesthesia (70.0%). Nineteen procedures (15.8%) were performed percutaneously by a bilateral common femoral approach. In 101 procedures, percutaneous access was used on one side, and surgical cut-down was performed on the contralateral side, combined with an endarterectomy of the common femoral artery (CFA) or distal external iliac artery (EIA) in 30 patients. Additional brachial access was used in 28 cases (23.3%).
All 454 BeGraft stents (137 aortic and 317 peripheral) were successfully delivered and deployed. The median number of BECSs used during a procedure was 3 (range: 3–6). In 54.2% of the procedures, the CERAB was completed with the use of only 3 covered stents. The other required proximal or distal extensions to cover the entire diseased segment. In 42 patients (35.0%), the covered iliac stent was distally extended with an uncovered self-expanding nitinol stent to preserve the patent internal iliac artery (IIA). In 75 patients (62.5%), patent inferior mesenteric artery (IMA) was intentionally covered to treat the occlusive disease of the distal abdominal aorta. The procedural characteristics and stent specifications are listed in Table 3. Distal embolism, stent kinking, or significant residual stenosis did not occur in any patient. An additional open surgical procedure was needed in 30 patients (25.0%). The median duration of the procedure was 120 minutes (IQR: 80–180 min).
CERAB Procedural Characteristics.
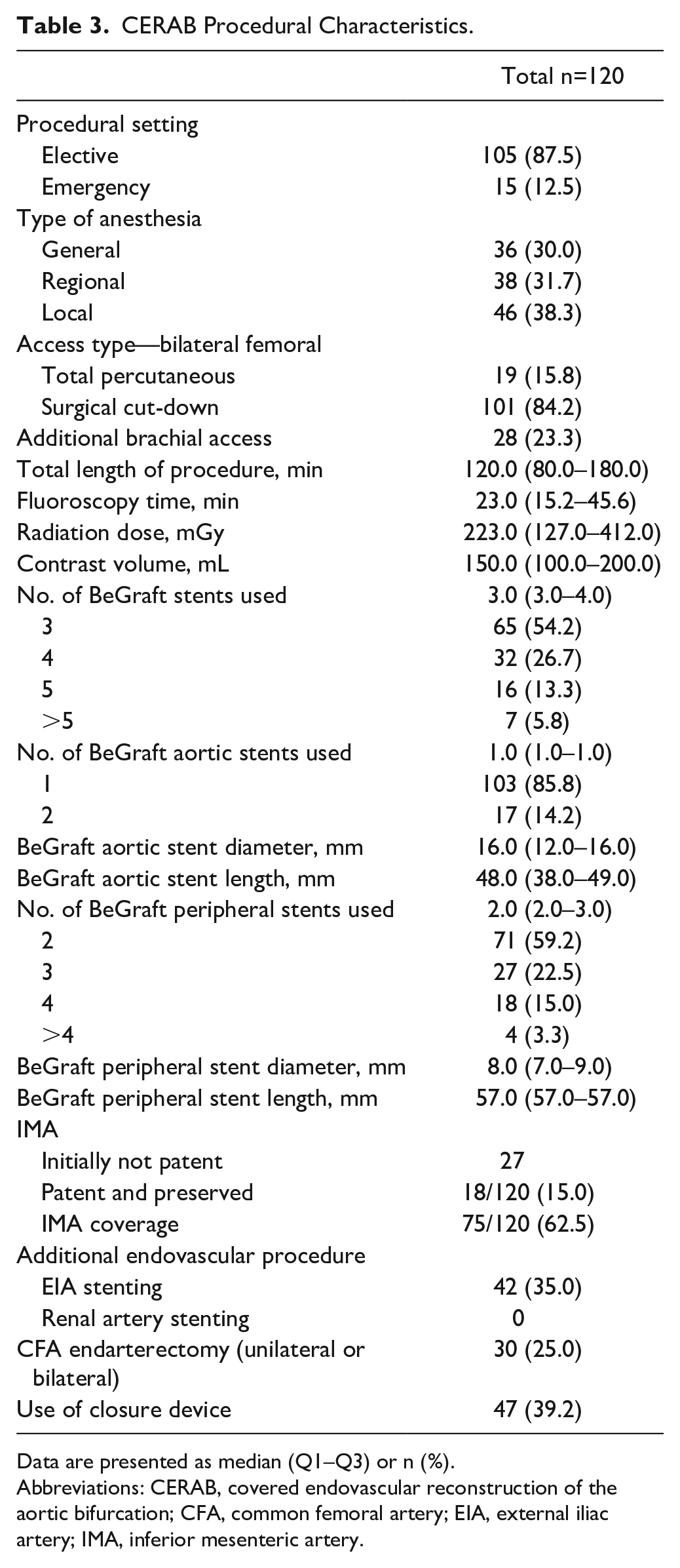
Data are presented as median (Q1–Q3) or n (%).
Abbreviations: CERAB, covered endovascular reconstruction of the aortic bifurcation; CFA, common femoral artery; EIA, external iliac artery; IMA, inferior mesenteric artery.
Intraoperative complications included flow-limiting dissections in 6 patients (2 in the aorta and 4 in the iliac tract). All were treated with endovascular procedures (prolonged balloon dilatation, followed by covered stent or BMS placement) and did not lead to any permanent deficit. Two patients experienced an intraprocedural rupture of the EIA. It was treated by a covered stent in the same procedure without conversion to open surgery. Two retrograde aortic dissection cases occurred, which were managed with additional brachial artery access for antegrade recanalization. The overall procedural complication rate was 14 (11.7%), all of which were successfully resolved during the index procedure.
Early Outcomes (In-hospital and 30-Day Follow-up)
The median hospital length of stay (LOS) was 5 days (IQR: 3–6 days). Thirty patients (25.0%) were admitted to an ICU with a median stay of 6 days (IQR: 5–8 days). The median postoperative LOS was 3 days (IQR: 1.0–4.0 days). None of the patients were lost to early follow-up. Postprocedural complications and early outcomes are listed in Table 4.
Postoperative Outcomes.
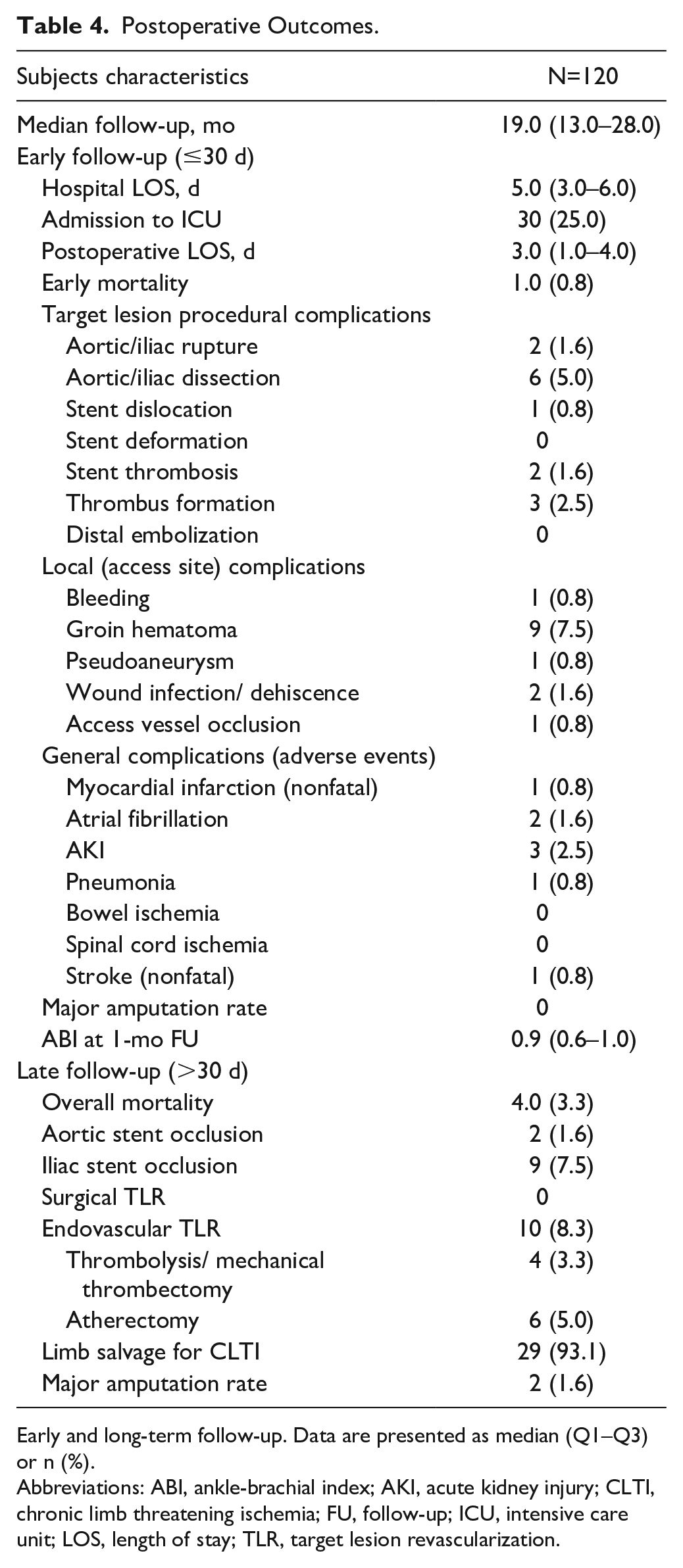
Early and long-term follow-up. Data are presented as median (Q1–Q3) or n (%).
Abbreviations: ABI, ankle-brachial index; AKI, acute kidney injury; CLTI, chronic limb threatening ischemia; FU, follow-up; ICU, intensive care unit; LOS, length of stay; TLR, target lesion revascularization.
The 30-day mortality rate was 0.8%. One early death occurred. The patient developed deterioration of his cardiac function following a technically successful CERAB procedure, resulting in ventricular fibrillation, cardiac arrest, and in-hospital death. The overall 30-day complication rate in this cohort was 19.2%. There were 14 local (access site) minor complications and 9 general complications (adverse events). A surgical reintervention was necessary in 2 cases: one due to bleeding from the CFA and the other due to access site (brachial artery) thrombosis.
Clinical improvement with at least 1 Rutherford category occurred in all initially symptomatic patients. Ankle-brachial indices significantly increased from 0.6 (range: 0.2–0.8) preoperatively to 0.9 (range: 0.4–1.0) at 1-month follow-up (p<0.05). There was no limb loss during the early follow-up period.
Mid-term and Long-term Outcomes (>30 Days of Follow-up)
The median follow-up was 19 months (range: 6–56 months). Follow-up at 6, 12, and 24 months was available in 112, 94, and 38 cases, respectively. Two patients were lost to follow-up. The survival rate at the last follow-up was 96.7%. One patient died during an in-hospital stay (mentioned above). Three patients died due to non-procedure-related causes (1 patient died 2 months after the procedure as a result of a cardiac event, 1 patient died from pancreatic cancer 6 months after the CERAB procedure, and 1 died 34 months after the procedure due to unknown reason).
The primary patency rate, secondary patency rate, and freedom from TLR at 24 months were 93.3%, 97.3%, and 91.1%, respectively (Figure 2A). Figure 2B demonstrates the cumulative survival curve as estimated by Kaplan-Meier analysis.
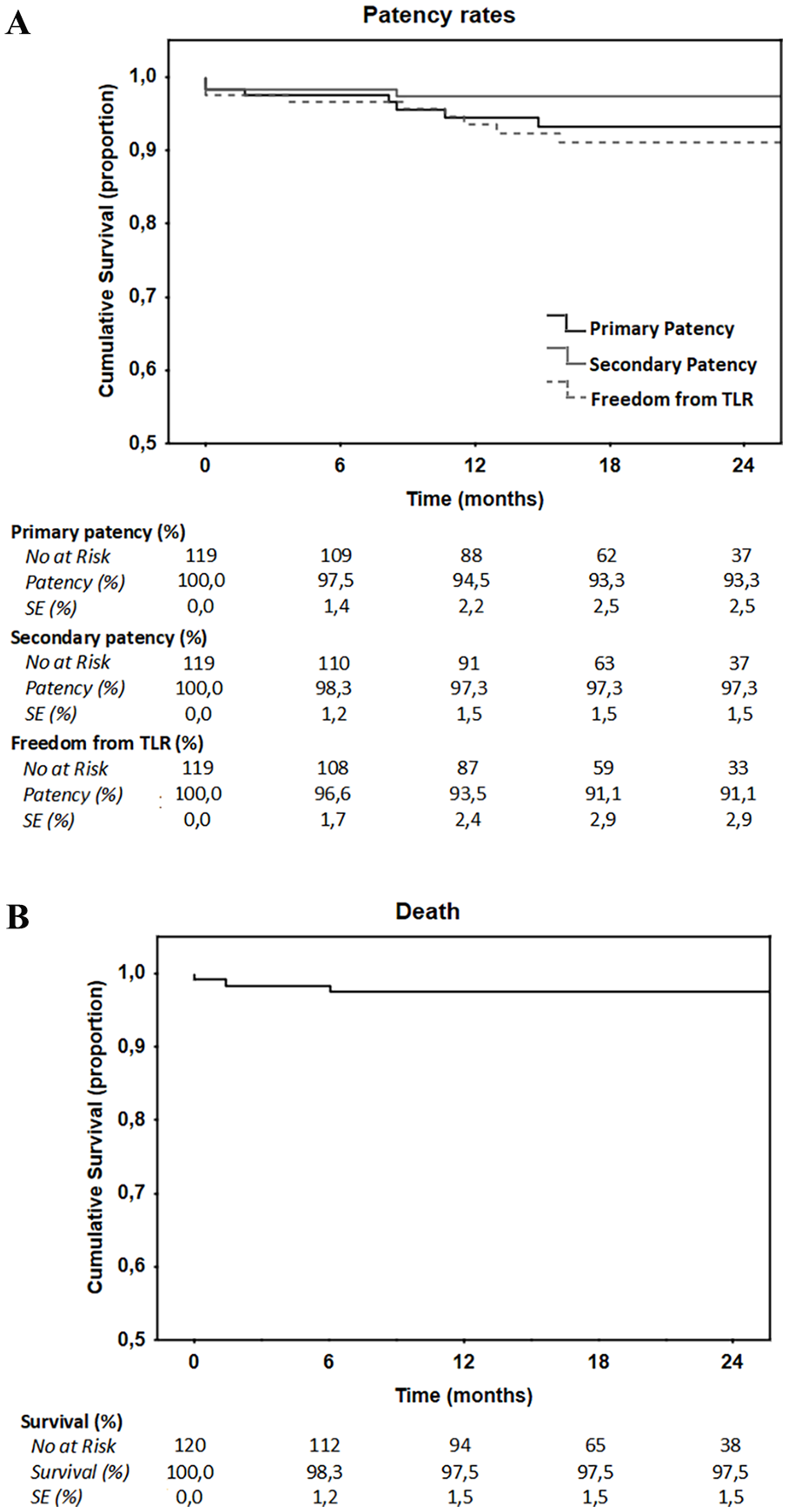
Kaplan-Meier survival analysis showing patency curves (A) and all-cause survival (B) of patients treated with covered endovascular reconstruction of the aortic bifurcation (CERAB).
A total of 10 patients needed repeated percutaneous intervention of the target lesion due to symptomatic restenosis/reocclusion occurring during the follow-up period. Most of the reinterventions (80.0%) were performed within 12 months after the initial procedure. Reasons for reinterventions and reintervention types are presented in Table 4. In 4 acute cases treated with catheter-directed thrombolysis (CDT), outflow stenosis was found in the EIA or CFA and treated by percutaneous transluminal angioplasty (PTA) in 3 cases and open endarterectomy in 1 case. The other 6 patients developed a chronic restenosis above the aortic stent (n=1) or distal to the iliac stents (n=5), referred to as edge stenosis. All those patients were treated with a mechanical atherectomy device followed by additional angioplasty. An example of a successful endovascular revascularization procedure is presented in Figure 3.
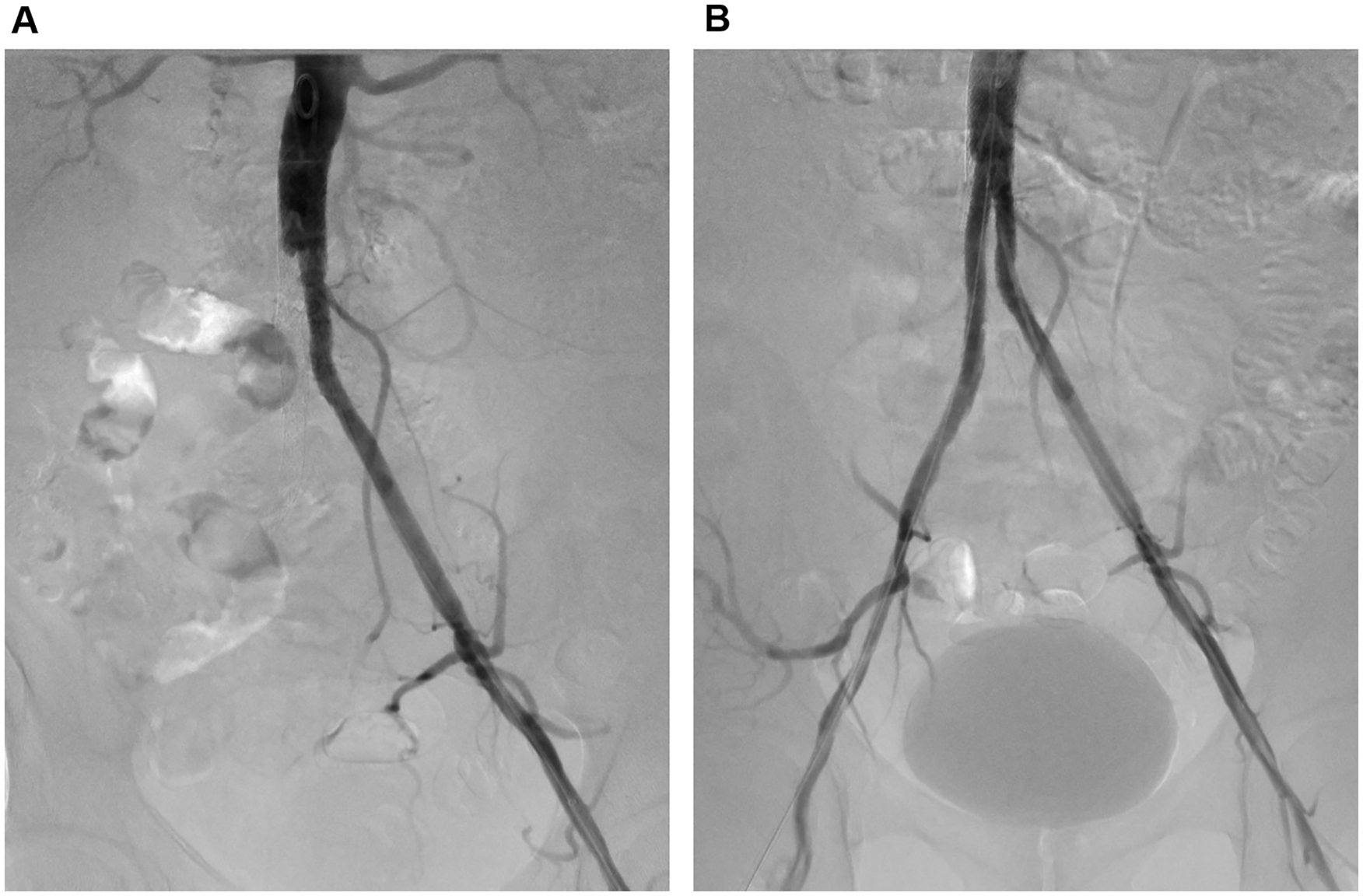
A 68-year-old man with chronic lower extremity ischemia (Rutherford 3) 2 years after endovascular reconstruction of the aortic bifurcation (CERAB) procedure during the target lesion revascularization (TLR) procedure. (A) Initial procedural angiography demonstrates total occlusion of the right iliac extension. (B) Final arteriography after endovascular recanalization with ROTAREXTM 8F atherectomy system.
Two major amputations were reported during follow-up. The limb salvage for CLTI was 93.1%. None of the patients suffered symptoms of spinal cord ischemia or large bowel ischemia perioperatively nor in the late follow-up period. There were no stent migration, twisting, or stent fractures over the 2 years of follow-up.
Discussion
Increasing evidence indicates that the more complex TASC C/D lesions can be treated using endovascular techniques with satisfying results. This multicenter study evaluating the application of the BeGraft BECSs in a series of patients with complex AIOD demonstrates favorable results in terms of technical success, morbidity, and patency.
The BECS may reduce the incidence of complications during extensive AIOD procedures with better patency rates than BMS. A possible advantage of polytetrafluoroethylene (PTFE)-covered stents is the immediate covering of ulcerated plaques and vessel wall thrombus, preventing distal embolization. The use of BECS placement for a focal occlusive disease of the infrarenal aorta was shown to have a very low complication rate and excellent patency. 22 Covered stents are a viable treatment option also for patients with complex AIOD because of their high technical success rates and favorable patency at 12 months.23–25
In this study, we have demonstrated promising results of the CERAB procedure with 2-year primary patency, secondary patency, and freedom from TLR rates of 93.3%, 97.3%, and 91.1%, respectively. Our results are comparable to already published data. However, in this study, 25.8% of the patients were treated for CLTI, lower than in other studies.13,14 In addition, in our study group, the incidence of TASC D lesions was lower (67.5%), probably influencing the reported outcomes. The early (in-hospital) overall major complication rate of 6.7% is higher than the 3.4% demonstrated by Saratzis et al. 16 Nevertheless, it is much lower in comparison with the 30-day major complication rate reported after aorto-bifemoral bypass surgery. 8
The choice of an ideal covered stent for CERAB is based on the anatomical characteristics of both the aorta and iliac arteries. To date, none of the BECSs that are currently available have been specifically designed and evaluated for that purpose. The BeGraft stent differs from other commonly used stents by being made of cobalt-chromium rather than stainless steel. The results from previously published studies using BeGraft BECSs in the aortoiliac field are satisfactory.26,27
One of the advantages of this study is that we only included CERAB procedures with only BeGraft stents used. Other CERAB series published included several types of covered stents. In the study by Saratzis et al, 16 77% of stents used were BeGraft stents, although the authors found no differences in outcomes between stents used. In 45.8% of cases, we could not complete the CERAB procedure with 3 stents only, which is very similar to the results of Taeymans et al. 14 The choice of the diameter of the aortic and peripheral covered stents used for CERAB configuration depends on the infrarenal aortic diameter and the common iliac artery diameter. In the CERAB technique, the proximal two-third part of the aortic stent is usually flared with a larger balloon, thereby creating a funnel-shaped covered stent. The iliac stents are then positioned proximally in the distal one-third of the aortic stent. The median aortic stent diameter for all procedures was 16.0 mm.
According to previous data, which were also confirmed by our results, abdominal PAU often coexists with complex AIOD resulting from atherosclerotic plaques with severe calcification. The search for the optimal treatment of PAU in the presence of AIOD is a challenging task.26,27 This study shows that the CERAB procedure with BECS for the treatment of infrarenal PAU coexisting with AIOD is both safe and very effective.
As with any new treatment alternative, the CERAB technique has limitations. Compared with the “kissing stents” technique, the CERAB with BeGraft aortic stent requires a larger profile introducer sheath (9F–14F), multiply access sites are in use, and the whole procedure is likely to be more expensive. Finally, the flaring technique of the proximal aortic stent commonly used during CERAB is still out of the instruction for use (IFU). 15 Placing a covered stent in the abdominal aorta also has a higher potential for coverage of collateral vessels and the IMA. In our study group, no visceral or spinal cord ischemic events occurred. However, the CERAB procedure with a chimney graft implantation to the IMA was also described. 28 Our initial experience with CERAB procedures showed low procedural-related complications, and the majority of these were related to the recanalization of chronic total occlusion (CTO) lesions, not the stent’s implantation. We advise an additional brachial approach for every case of aortic CTO to prevent retrograde dissection. The majority of procedure-related complications were treated with endovascular therapy at the time of the procedure. The high incidence of groin-related complications in this study may be related to the fact that many patients underwent open surgical access and CFA endarterectomy procedure.
During follow-up, we found favorable patency of CERAB. Target lesion revascularization was necessary for 10 patients. In the study of Taeymans et al, 14 88% of reinterventions were performed within the first year after treatment. In our study, the loss of primary patency was also highest within the first 12 months after the CERAB procedure, suggesting relatively stable patency rates afterward. The authors of this study suggest strict follow-up within the first 12 months to prevent early occlusion. Reinterventions after CERAB can be managed by percutaneous techniques, with subsequent secondary patency rates of 95.0% to 97.0% at 2 years of follow-up.13,14 Secondary patency rates in our study were excellent, reaching 97.3% at 2 years. During follow-up in our study group, we have not observed any stent collapse, which was noticed by Grimme et al. 13 The authors suggested that highly calcified lesions overcome the radial force of the covered stents used in that study. 13
The currently available published studies on CERAB have several limitations. All studies are retrospective from high-volume experienced institutions with limited follow-up. The CERAB procedure has excellent short-term and mid-term results. Long-term follow-up is required to confirm these promising results. In all 3 clinics participating in this study, an endovascular first strategy is now applied, and aorto-bifemoral bypass grafting is reserved only for those patients in whom CERAB cannot be performed. The relatively high rate of perioperative morbidity in this series may result from the fact that high-risk patients with complex TASC C/D lesions were included and represent everyday clinical practice. As a less invasive procedure, the CERAB technique is associated with a lower complication rate than aorto-bifemoral bypass surgery. However, a randomized control study is mandatory to confirm this statement.
Conclusion
This is the largest study to examine the use of BeGraft stents for the treatment of AIOD using the CERAB technique. It was found that the procedure had a high technical success rate and low morbidity, even in relatively ill patients with TASC C/D lesions. The use of BECS during the CERAB procedure appears to be a safe and effective endovascular treatment for complex AIOD patients that may otherwise require aorto-bifemoral bypass. Prospective studies on the CERAB technique are definitely recommended.
Footnotes
Authors’ Note
This study was presented during the Leipzig Interventional Course 2022, Leipzig, Germany, June 6–9, 2022; during the 35th Hybrid Annual Meeting, Rotterdam, The Netherlands, September 28–29, 2021; and European Society for Vascular Surgery 33rd Annual Meeting, Hamburg, Germany, September 24–27, 2019.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.