
Abstract
Background:
To assess the feasibility and first-in-human experience of a novel endovascular robotic system for treatment of lower extremity peripheral arterial disease (PAD).
Methods:
Between November 2021 and January 2022, consecutive patients with obstructive lower extremity PAD and claudication (Rutherford 2–5) with >50% stenosis demonstrated on angiography were enrolled in this study. Lower extremity peripheral arterial intervention was performed using the endovascular robotic system, which consisted of a bedside unit and an interventional console. The primary endpoints were technical success, defined as the successful manipulation of the lower extremity peripheral arterial devices using the robotic system, and safety. The secondary endpoints were clinical success, defined as 50% residual stenosis at the completion of the robot-assisted procedure without major adverse cardiac events and radiation exposure.
Results:
In total, 5 patients with PAD were enrolled in this study (69.2±6.0 years; 80% men). The novel endovascular robotic system successfully completed the entire procedure of endovascular treatment of lower extremity PAD. Conversion to manual operation, including advancement, retracement, rotation of the guidewires, catheters, sheaths, deployment, and release of the balloons and stent grafts, was not necessary. We achieved the criteria for clinical procedural and technical success in all patients. No deaths, myocardial infarctions, or ruptures occurred in the period up to 30 days after the procedure, and no device-related complications were observed. The robotic system operator had 97.6% less radiation exposure than that at the procedure table, with a mean of 1.40±0.49 μGy.
Conclusions:
This study demonstrated the safety and feasibility of the robotic system. The procedure reached technical and clinical performance metrics and resulted in significantly lower radiation exposure to the operators at the console compared with that at the procedure table.
Clinical Impact
There were some reports about several robotic systems used in the peripheral arterial disease, but no robotic system was able to perform entire procedure of endovascular treatment of lower extremity peripheral arterial disease (PAD).
To solve this problem, we designed a remote-control novel endovascular robotic system. It was the first robotic system that can perform entire procedure of endovascular treatment of PAD worldwide. A novelty retrieval report about this is provided in the supplementary materials.
The robotic system is compatible with all commercial endovascular surgical devices currently available in the market, including guidewires, catheters and stent delivery systems. It can perform all types of motion, such as forward, backward, and rotation to meet the requirements of all types of endovascular procedures. During the operation, the robotic system can perform these operations in a fine-tuned manner, so it is easy to cross the lesions, which is the key factor influencing the success rate of the operation. In addition, the robotic system can effectively reduce the exposure time to radiation, thereby reducing the risk of occupational injury.
Keywords
Introduction
Patients with peripheral arterial disease (PAD) can be treated by endovascular procedures, such as angioplasty and stent placement, which are currently widely used. However, these procedures are facilitated by x-ray-based fluoroscopy, which is harmful to the medical staff. 1 In some instances, absorbed doses have been large enough to induce deterministic effects. Epilation, radiation-induced erythema, and blistering have been reported.2–5 To mitigate this, clinicians are required to wear heavy lead aprons at the bedside in relative proximity to x-ray sources. However, these heavy lead aprons may cause orthopedic complications. 6 In the last few decades, there has been a substantial increase in the manual control advancement of endovascular devices. Therefore, robot-assisted lower extremity peripheral vascular intervention (PVI) has begun to be developed, with the benefit of a dramatic reduction of radiation exposure in physicians. 7
In addition, low accuracy associated with manual operations could also be solved using robotic systems.8,9 Currently, there are many kinds of endovascular interventional robotic systems. 10 Although there are some reports of several robotic systems used in percutaneous coronary intervention (PCI) and PVI,11–13 no previous research has indicated that a robotic system has been able to perform the entire endovascular treatment procedure of lower extremity PAD.14,15
Recently, we developed a novel endovascular robotic system (ALL;VAS, Aopeng Medical, Shanghai, China). This system can be controlled remotely to perform the entire PVI, which aids in decreasing the risk of occupational hazards caused during the procedure. The system can also enhance the accuracy and control of the interventional procedure.
In this study, we report the first 5 cases of PVI performed with this endovascular robotic system at Changhai Hospital (Shanghai, China) who were treated for lesions of the lower extremity peripheral arteries. The aim of this study was to assess the feasibility and first-in-human experience of a novel endovascular robotic system for treatment of lower extremity PAD.
Materials and Methods
Study Design
This study was a single-arm, single-center feasibility and safety trial. The investigation of a novel endovascular robotic system for PAD was conducted between November 2021 and January 2022. The study protocol was approved by the Ethics Committee of Changhai Hospital (Shanghai, China) and conducted following the Declaration of Helsinki. All 5 participants provided written informed consent. All relevant data are presented in this article. All the techniques used had been previously tested in animal laboratory experiments. 16 The novel endovascular robotic system successfully performed bilateral iliac artery stent implantation on multiple pigs using commercialized guidewires, catheters, and stent delivery systems.
Study Population
Patients with earlier angiographic documentation of obstructive lower extremity PAD and evidence of lifestyle-limiting claudication (Rutherford classes 2–5) were enrolled in the study. Inclusion criteria involved a de novo stenosis of at least 50%, verified by angiography or confirmed occlusion of femoropopliteal arteries.
Exclusion criteria included planned PVI or target artery bypass graft surgery; angiographic evidence of target vessel aneurysm, dissection, perforation, or acute thrombosis; or the calcification of the culprit lesion, which would require atherectomy.
All patients were followed up within 30 days after surgery, for every 3 months in the first year after treatment, and for every 6 months thereafter. Follow-up imaging was mainly performed using duplex ultrasound. Computed tomography angiography was performed when symptoms recurred or more than 50% restenosis was detected on duplex ultrasound. The clinical secretary conducted a monthly telephone follow-up to assess the incidence of bleeding.
Study Endpoints
The primary endpoints were technical success and safety, defined as the successful introduction of the endovascular device into the target vessels and retraction of the PVI devices (eg, guidewire, guide catheter, angioplasty balloon, stent graft) by the robotic system and the completion of percutaneous transluminal angioplasty without an unexpected switch to a manual procedure or device-related serious adverse event in the periprocedural period. The secondary endpoints were clinical success and radiation exposure. Clinical success was defined as 50% residual stenosis determined by a quantitative angiographic core laboratory at the completion of the procedure. Furthermore, there could not be any serious adverse device–related events that caused prolonged hospitalization, life-threatening incidents or death during the surgery, or in-hospital major adverse cardiac events. Major adverse cardiac events were defined as myocardial infarction, rupture, or death.
Robotic System
A new type of endovascular robotic system, composed of a bedside unit (Figure 1A) and an interventional console (Figure 3C), was designed for all endovascular interventional surgeries, including PAD.
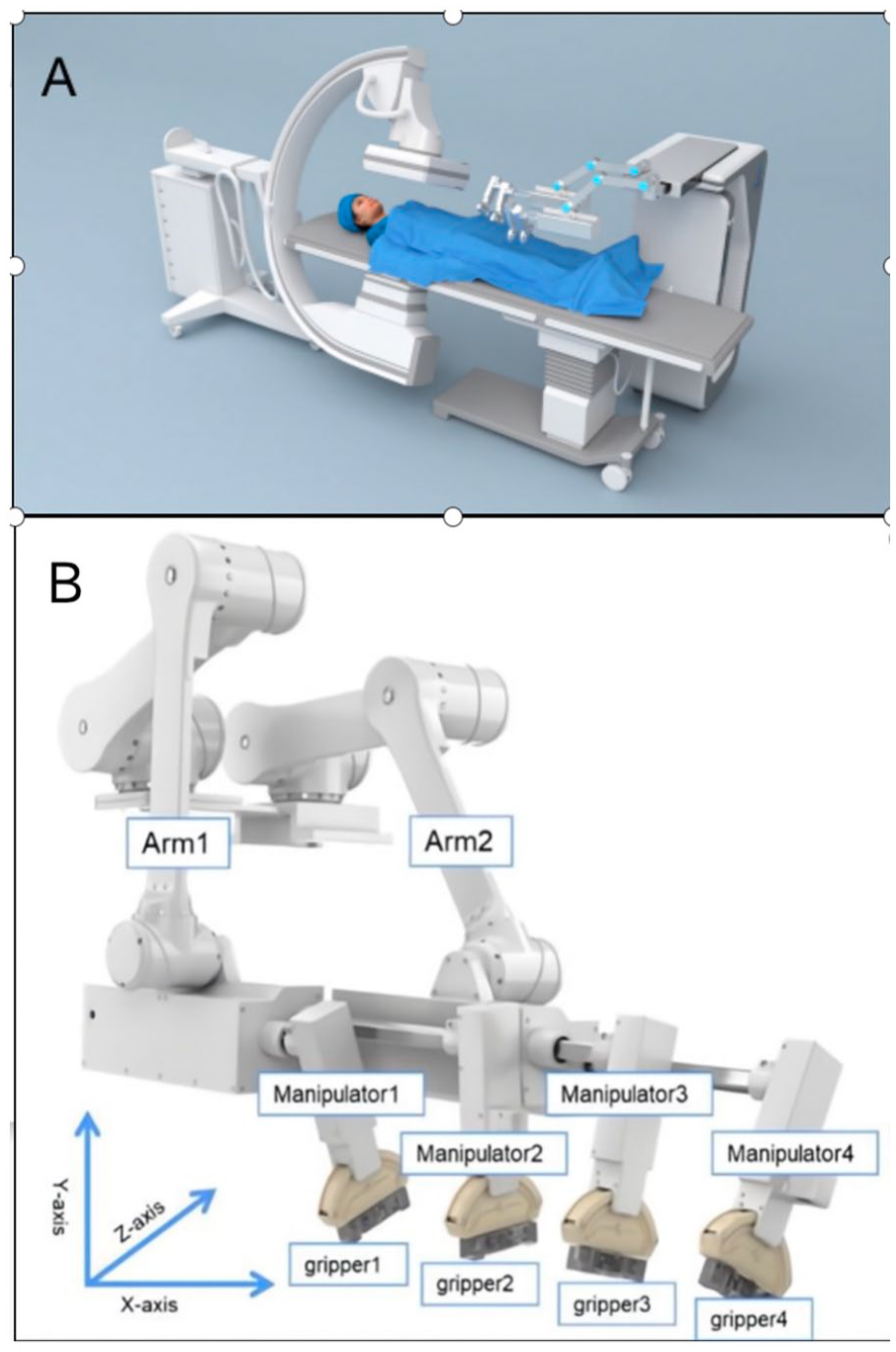
(A) Schematic diagram of the bedside robotic unit. (B) The bedside robotic unit of the novel endovascular robotic system.
The bedside unit has an open architecture system designed specifically to suit all endovascular devices, including both rapid-exchange and over-the-wire catheter systems.
The unit consists of 2 groups of independent mechanical arms, each having 3 degrees of freedom (DOFs), allowing the arms to move independently in all 3 dimensions. In addition, each arm has 2 manipulators, and each manipulator has 1 gripper (Figure 1A and B). The grippers are designed in a double V-shaped form (Figure 2A and B), with 2 modes of clamp and release (Figure 2C and D), and 12 DOFs. A surgeon can operate the joystick to control long axial movements of the manipulators. When all 4 manipulators are clamping the endovascular devices, long axial movements of the manipulators can be converted into the movement of the endovascular devices.
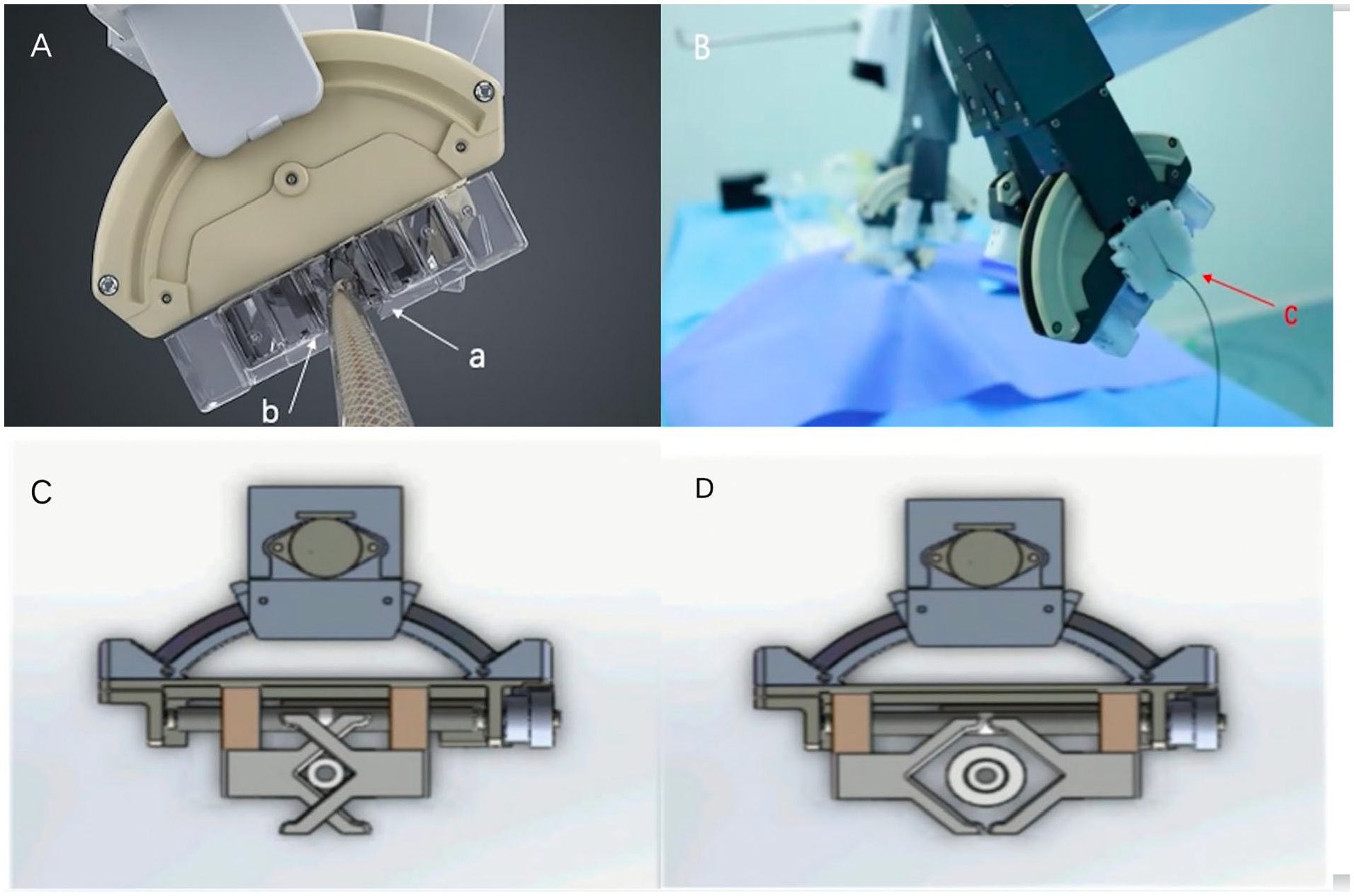
(A) (a, b) Double V-shaped grippers. (B) (c) The third V-shaped relay gripper that clamps the device when the grippers are released and rotate. It releases when the double V-shaped grippers clamp the device and rotate. (C, D) The working states of the double V-shaped grippers: (c) clamping state and (d) loosening state.
The interventional console is a radiation-shielded mobile workstation that can be placed away from the bed, even outside the catheterization laboratory. Surgeons can perform PVI remotely from the control console with console joysticks or touchscreen buttons, which is expected to reduce radiation-associated occupational hazards (Figure 3). In the procedure, angiography and electrocardiography are used simultaneously, which elicits a need for dual monitors inside the console to enable better visualization from a closer distance.
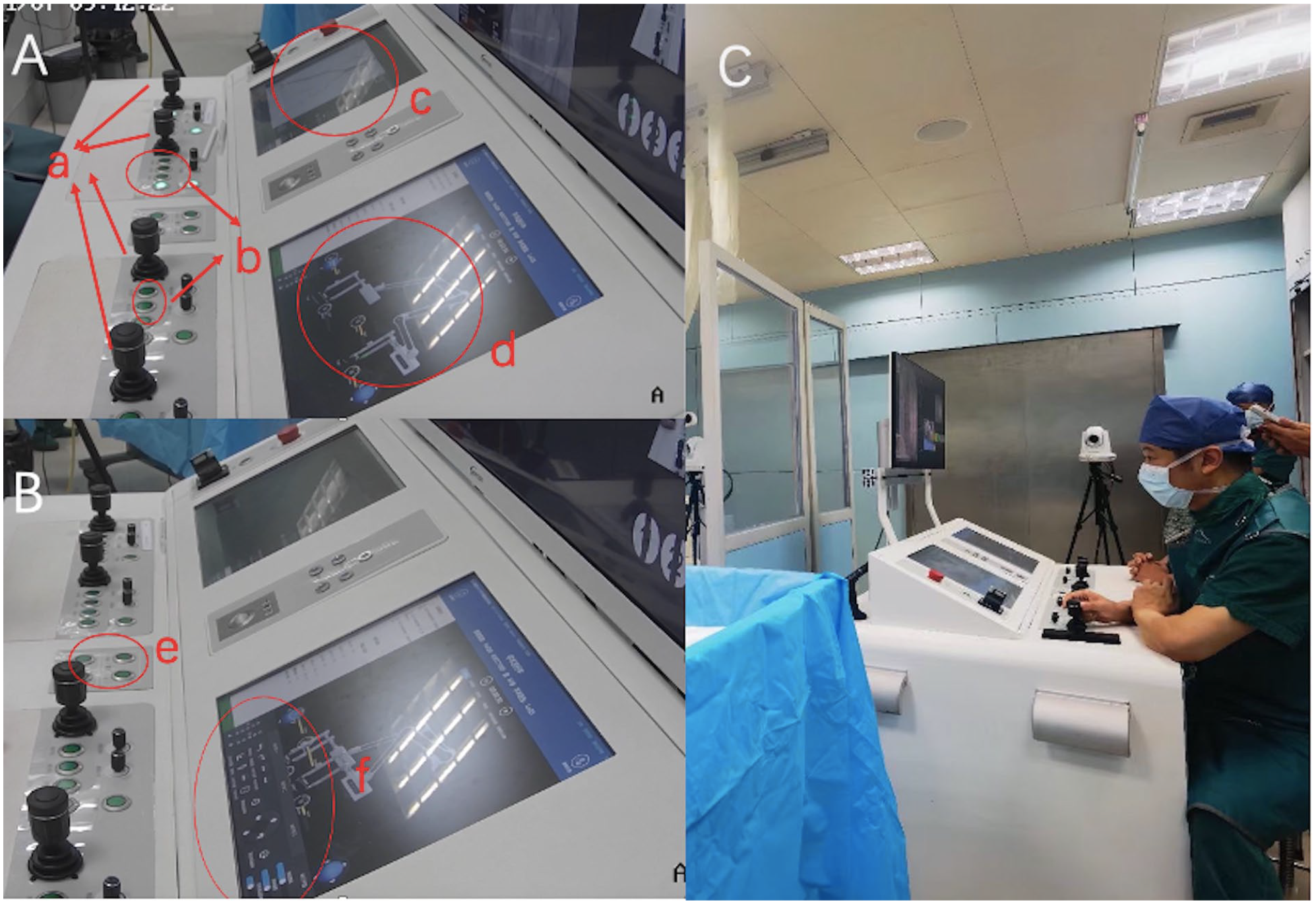
(A) The interventional console: (a) console joysticks; (b) buttons that control manipulators; (c) screen 1 shows angiography and electrocardiography; (d) screen 2 shows movements of the robotic system. (B) (e) Buttons that control the mechanical arms; (f) touchscreen buttons that control the movements of the manipulators. (C) A panorama of the interventional console and operators.
Interventional Procedure
A surgeon with prior experience in the use of the robotic system and performance in the animal laboratory operated the robotic system in 5 human procedures. In the patient with iliac artery occlusion and the 3 patients who had lesions in the superficial femoral artery, guidewires and catheters were advanced to the target lesions automatically by the robot. Operators loaded balloons into the system and advanced the device with the robotic system to perform pre-dilation and post-dilation of the target lesions. Stent grafts were introduced to the blood vessels in the 4 patients. The procedures for stent-graft deployment, release, and retrieval were all performed using the robotic system. Completion angiograms confirmed the optimal stent-graft deployments and ruled out the presence of any associated complications, which indicated a 100% success rate of surgery. The novel endovascular robotic system can accommodate all types of devices in the PVI surgeries, and all the procedures in this study were performed by the robotic system exclusively without manual conversion. A detailed operation video is available in Supplemental Video 2.
In the patient whose popliteal artery was occluded, the angiogram suggested residual stenoses and many thrombi. Therefore, instead of deploying stent grafts, the surgeons decided to select a thrombolytic catheter to perform a catheter-directed thrombolysis because of the thrombi. They loaded the thrombolytic catheter on the robotic manipulator and advanced it using the robot system. The thrombi were then reconfirmed via angiography, using a thrombolytic catheter. The absence of stent-graft implantation was not considered to be an operational failure of the robotic system.
We used direct electronic dosimeters to monitor the operator’s radiation exposure at the console and the procedure table. The dosimeter was shielded with a lead apron and placed 30 cm away from the radiation source. This was equivalent to the distance between the operator and the radiation source in manual endovascular treatment of PAD.
Statistical Analysis
Standard summary statistics were calculated for all patients and study outcome variables. Continuous variables were expressed using means and standard deviations (mean±SD). Categorical data were summarized as percentages (%).
Results
Baseline Demographic and Clinical Characteristics
Patients were elderly (69.2±6.0 years of age; 80% men) and primarily categorized as Rutherford class 2 (20%), 3 (60%), and 4 (20%). The mean ankle-brachial index was 0.3. Two patients were classified as TransAtlantic Iner-Society Consensus (TASC) B, 2 as C, and the last as D (Table 1). Seven lesions were found in the 5 study patients, with the majority being in the superficial femoral artery (57.1%). One lesion was found in the popliteal artery, and the other 2 lesions were found in the iliac artery. Two of those lesions were stenotic, and the others were occlusive. The lesions were relatively long (124.71±139.26 mm), and the blood vessels were slightly curved (100%), with relatively heavy calcification (57.1% heavy) (Table 2).
Demographic Data and Procedural Characteristics of All Patients Intervened.
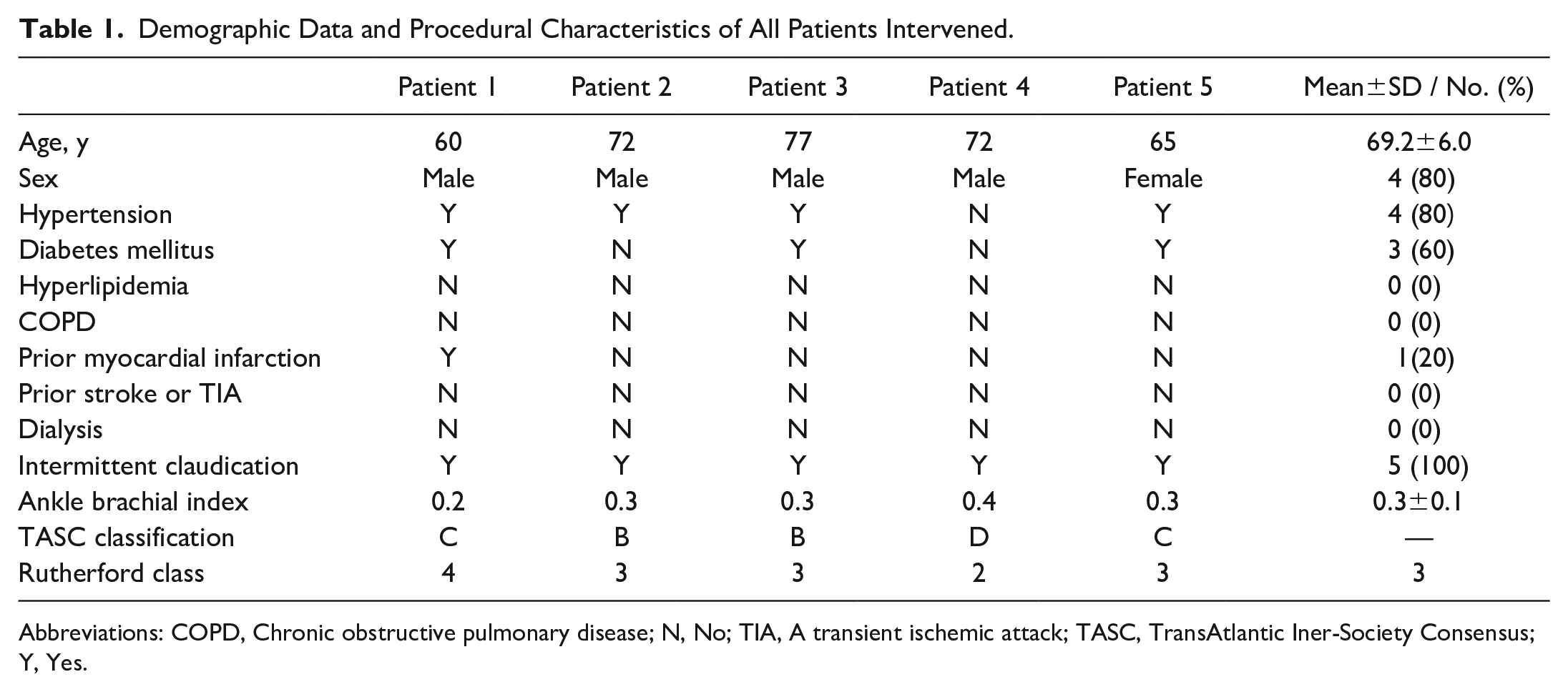
Abbreviations: COPD, Chronic obstructive pulmonary disease; N, No; TIA, A transient ischemic attack; TASC, TransAtlantic Iner-Society Consensus; Y, Yes.
Baseline Lesion Characteristics.
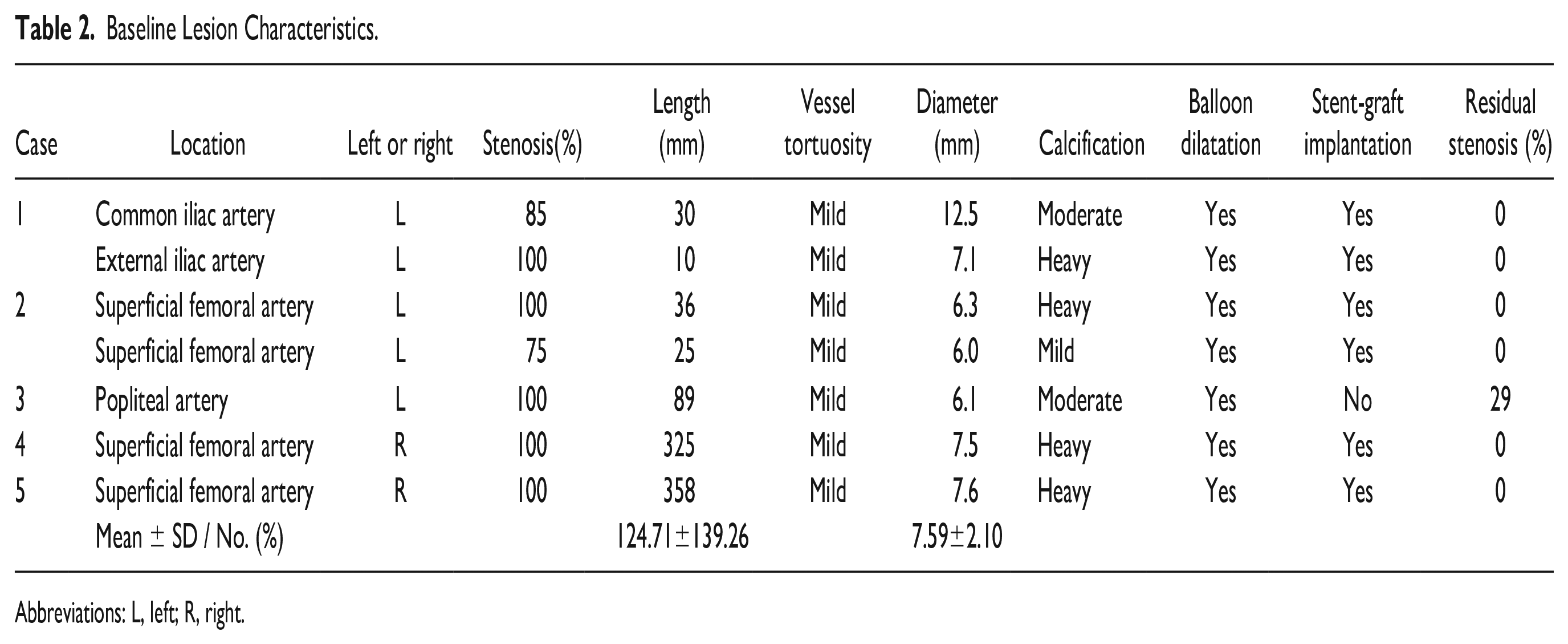
Abbreviations: L, left; R, right.
Primary Endpoints
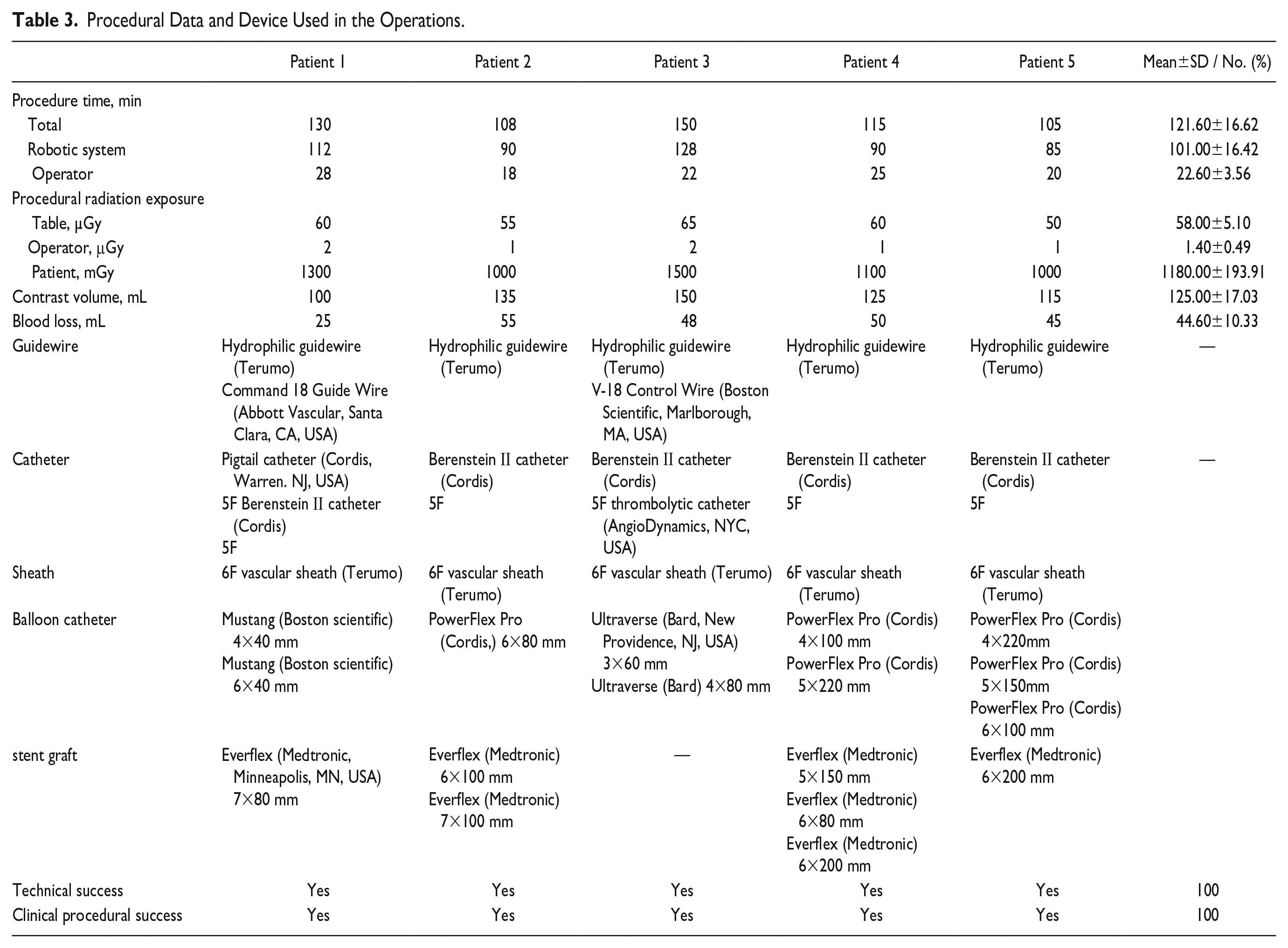
All PVI procedures were performed via femoral arterial access, with 6Fguiding catheters. Surgeons selected appropriate devices (eg, guidewires, catheters, sheaths, balloons, stent grafts.) that were used in the robot-assisted treatment of lower extremity PAD (Table 3), similar to manual PVI. All these devices were commercially approved. Operators successfully introduced the endovascular devices into the target vessels and retracted the PVI devices by the robotic system. No unexpected switch to a manual procedure or device-related serious adverse event in the periprocedural period was observed. The primary endpoints were all achieved in all 5 patients (100%).
Procedural Data and Device Used in the Operations.
Secondary Endpoints
Severe vascular stenosis and occlusion were relieved intraoperatively. All the sites of preoperative vascular occlusion were found to be unobstructed after surgery, and angiography revealed that the stenosis rate decreased from 100% to 0%, except in patient 3, whose residual stenosis was 29%. Typical imaging contrasts before and after treatment of the 4 patients are shown in Figure 4, and those of patient 3 are shown in Supplemental Video 2. There were no serious adverse events related to the procedures or the endovascular robotic system. In addition, there was no incidence of major adverse cardiac events by the 6-month follow-up after the procedure.
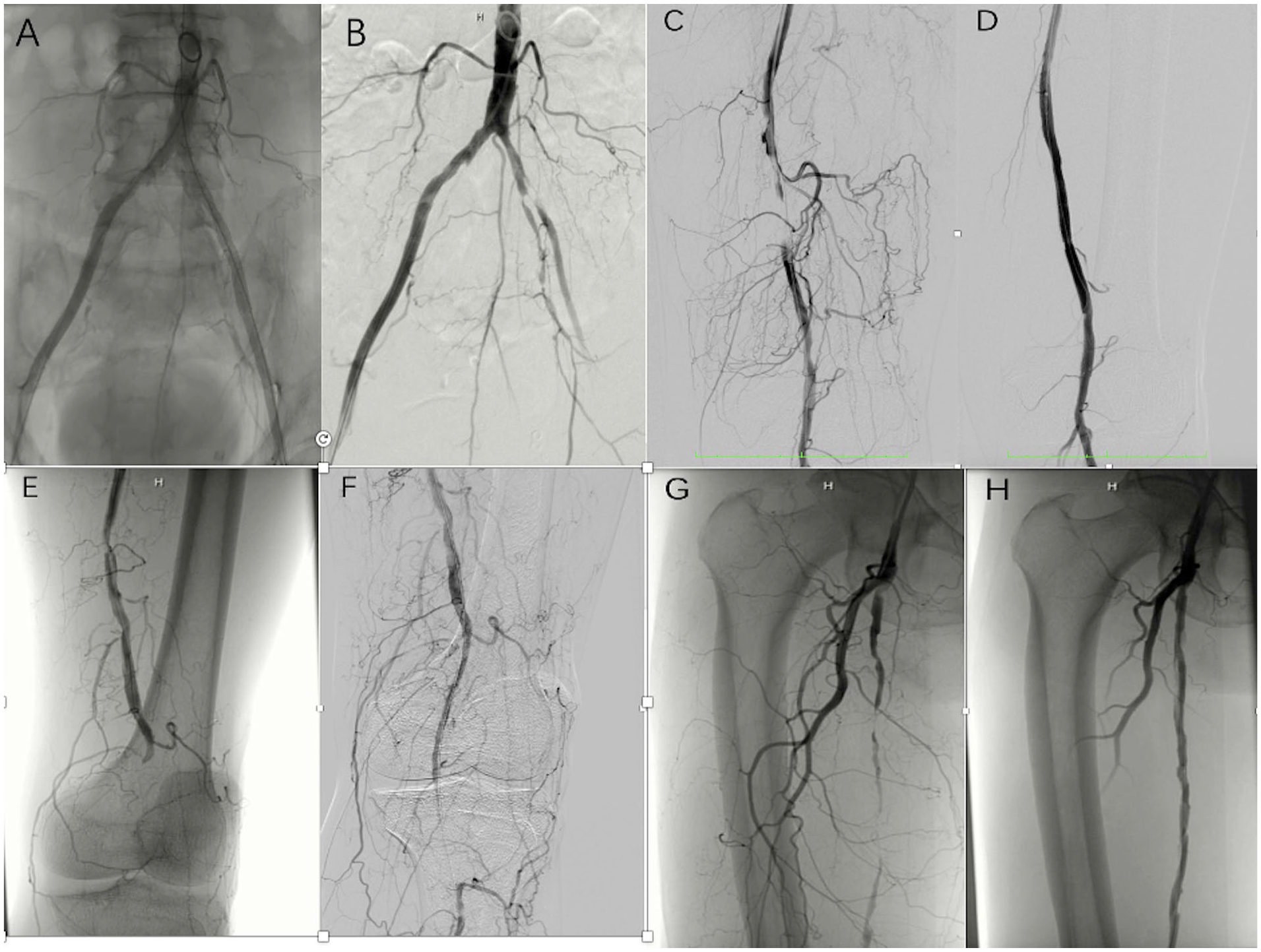
(A, B) Typical imaging contrasts before and after treatment of patient 1. (C, D) Typical imaging contrasts before and after treatment of Patient 2. (E, F) Typical imaging contrasts before and after treatment of patient 3. (G, H) Typical imaging contrasts before and after treatment of patient 5.
The operation time did not exceed 2.5 hours. The robotic system achieved a mean procedure time of 101.00±16.42 min, whereas the mean operator procedure time was 22.60±3.56 min. Intraoperative blood loss and the amount of contrast agent used were found to be similar to those in artificial peripheral vascular interventional surgeries. 17 The operator of the robotic system had 97.6% reduced radiation exposure compared with that at the procedure table, with a mean of 1.40±0.49 μGy (Table 3).
The secondary endpoints were all achieved in all 5 patients (100%).
Discussion
This is the first study to demonstrate the feasibility and safety of the novel endovascular robotic system we developed for the treatment of lower extremity PAD.
Previous research had suggested that robotic systems could be used to reduce radiation exposure.18–23 Intervention operators develop posterior lens opacities and cataracts at younger ages and at higher rates than do other professionals. A recent observational report raised concern of a possible association between career-long exposure to radiation in interventional operators with the development of parotid gland tumors.2–4,6,24,25 In our study, we measured the radiation exposure of the operators seated in the shielded interventional console and compared it with the radiation exposure at the procedure table. We found a significant decrease in operator radiation exposure, with a mean reduction of 97.6%, confirming the finding that performing lower extremity peripheral arterial interventional surgery with the robotic system can reduce the operator’s radiation exposure.
In 2012, a second-generation robotic interventional surgical system, the Magellan robotic system, received a 510 (k) license from the US Food and Drug Administration (FDA) in 2012 for its ability to manipulate guidewires and catheters during peripheral vascular interventional procedures. Currently, the Corpath 200 (Corindus Vascular Robotics, Inc.) is the only endovascular surgical robot approved by the FDA and Conformitè Europëenne (CE) for coronary and peripheral interventional therapy currently. It can meet most of the work requirements of the 0.014-inch rapid-exchange system, with catheters up to 7F in diameter. However, remedial stents can only be used manually. Other studies have evaluated the efficacy of Corpath GRX in intracranial aneurysm embolization. These commercialized robot-assisted systems have a single moving mechanical arm, which remains a common problem because a considerable proportion of endovascular procedures are conducted manually by the surgeons and assistants during the operation. 26
In contrast to these robot-assisted systems that can be used for PCI and PVI, the remote-control endovascular robotic system we designed consists of 2 mechanical arms and each with 2 manipulators. In addition, each manipulator has 3 DOFs: advancement/withdrawal, rotation, and clamping/releasing. Through the coordinated movement of the 4 manipulators (including manipulators moving in the same, opposite, and reverse directions), the novel robotic system can accomplish complex procedures, such as super selection, crossing actions, stent-graft deployment, and all other technical steps for the completion of lower extremity PAD interventional surgery. Conversion to manual operation for advancement, retracement, rotation of the guidewires, catheters, sheaths, deployment, or release of the balloons and stent grafts was not necessary in the 5 procedures in this study.
Another aspect that contributes to the robotic system’s robustness in the procedure is the design of the grippers. Owing to the different choices of guidewires, catheters, sheaths, balloons, and stent grafts in lower extremity peripheral arterial interventional surgeries, the endovascular robotic system should be designed to adopt all the different types of devices to perform the entire procedure. However, limitations still exist, such as the fact that most commercialized endovascular surgery robotic systems can only adopt customized catheters, which cost more than standard catheters.27–30 The grippers of the robotic system used in this study were designed as double V-shaped, which has effectively solved this problem. By choosing a suitable diameter of endovascular devices to be used in the operation, surgeons can make arbitrary adjustments to the grippers accordingly. The grippers can simulate manual grip, maximize the reliability and repeatability of the procedures, and minimize the risks associated with current endovascular devices. In the case of device entrapment in rotation, we designed a third V-shaped relay gripper, which is released when the double V-shaped gripper clamps. When it activates, the double V-shaped grippers are released and rotate back to the original place (Figure 2B).
Subintimal angioplasty is occasionally used to block the lesion segment through the lower limbs. During the entire operation, the grasping force of the grippers is strong, and each gripper can achieve a maximum clamping force of 13.89 N, 31 which provides sufficient strength to control the catheter better. Pushing the guidewire into the loops through the occlusion section to perform artificial subintimal dissection is enabled by this enhanced control.
The novel endovascular robotic system can not only complete the entire procedure but also improve its precision. With the robotic system, the relatively large manual movements made by the surgeon can be changed into subtle movements on the device, which can increase surgical operation efficiency. Moreover, the system can precisely rotate (1° steps) the catheter in position (1 mm steps), 32 improve the accuracy of the stent-graft delivery system, and effectively reduce the risk of iatrogenic injury. Although it is likely that endovascular imaging guidance is vital to improve the precision of the entire operation, the robot-assisted system facilitates the whole procedure with a high degree of accuracy.8,33,34
To ensure patient safety, we performed several actions. Although we used a novel robotic system to complete the entire procedure, every step was carefully monitored. The robotic system is equipped with a warning device and cameras, which provide surgeons with feedback about the events at the operating table. When the robotic system encounters an equipment failure or any other problem with the program, the warning device provides an alarm.
In some procedures, we must cross a relatively long occlusion. To realize this, the endovascular robotic system needs to continuously advance or retrace guidewires and catheters. This process was automated using pre-programmed software. The distance and speed of movements can be modified by the surgeons before the procedure. Then, surgeons only need to press the button to issue advancement or retracement instructions, and the system automatically moves the guidewires, catheters, and other devices, achieving semi-automation (Supplemental Video 1). This advanced unique technology and design ensures the accessibility and refinement of procedures. It benefits not only the surgeons but also the patients and lays the foundation for full automation of endovascular procedures in the future. It is expected that this novel robotic system will gradually be transformed into a fully automated model.
Limitations
Although the feasibility and safety of this novel endovascular robotic system have been preliminarily validated, human assistance is still needed to change devices in the procedures. In addition, clinical studies with larger sample sizes should be conducted in the future to further confirm this result.
Conclusion
This study confirmed the feasibility and safety of the novel endovascular robotic system for the treatment of lower extremity PAD. Although similar studies investigating this subject have been published in recent years, there have been no reports of an endovascular robotic system completing the whole procedure. This robotic system has laid a solid foundation for the future development of more accurate and intelligent robotic surgery systems.
Footnotes
Acknowledgements
We would like to thank Editage for English language editing.
Declaration of Conflicting Interests
None.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Science and Technology Innovation 2030: “New Generation Artificial Intelligence” Major Project, Research on Key Technologies of Endovascular Interventional Surgery Robot, 2018AAA0102603; 2019 Medical Leading Talents Program of Shanghai Health Commission, Robot-based Precision Minimally Endovascular Treatment for Aortic Dilatation Disease, 2019LJ17.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.