
Abstract
Purpose:
Clinical trials have demonstrated the superiority of drug-coated balloon (DCB) to noncoated balloon angioplasty for the treatment of femoropopliteal (FP) lesions. In those trials, the difference of primary patency between DCB and noncoated angioplasty widens especially after 6 months, speculating that the antirestenosis effect of paclitaxel is manifested after 6 months. Factors associated with restenosis after 6 months differ from those associated with restenosis within 6 months. This study aimed to elucidate the prognostic factors associated with early (within 6 months) and late (after 6 months) restenosis following DCB treatment in real-world FP practice.
Materials and Methods:
This multicenter, retrospective study analyzed 486 FP lesions (mean lesion length, 11.9±10.1 cm; chronic total occlusion, 21.0%) in 423 patients (diabetes mellitus, 59.3%; hemodialysis, 37.1%; chronic limb-threatening ischemia, 41.6%) who underwent successful DCB treatment between January 2018 and December 2019. The outcome measure was restenosis which is defined as a peak systolic velocity ratio >2.4 based on duplex ultrasound findings. Early and late restenosis were classified by the cutoff period of 6 months after the procedure. The associations of baseline and procedural characteristics with early and late restenosis were explored using Cox proportional hazards regression analysis.
Results:
The mean follow-up period was 25.3±12.1 months. The 6, 12, 18, and 24 month cumulative incidences of restenosis were 7.4%±2.4%, 20.9%±3.9%, 29.9%±4.5%, and 38.4%±5.1%, respectively. During the follow-up period, early and late restenosis was evident in a total of 31 lesions and 138 lesions, respectively. Multivariate analysis revealed that chronic total occlusion (hazard ratio [HR], 2.29; 95% confidence interval [CI], 1.07–4.92; p=0.033) and superficial femoral artery ostial lesion (HR, 2.73; 95% CI, 1.28–5.80; p=0.009) were significantly associated with early restenosis. On the other hand, calcification circumference over 270° (HR, 1.67; 95% CI, 1.17–2.37; p=0.004), distal external elastic membrane diameter under 5 mm assessed by intravascular ultrasound (HR, 1.90; 95% CI, 1.29–2.79; p=0.001), and involving popliteal arterial lesion (HR, 1.54; 95% CI, 1.08–2.21; p=0.017) were significantly associated with late restenosis.
Conclusion:
The prognostic factors associated with late restenosis differed from those associated with early restenosis in the real-world FP-DCB practice.
Clinical Impact
The current multicenter, retrospective study revealed that factors associated with early restenosis differed from those with late restenosis in the real-world FP-DCB practice. CTO and SFA ostial lesion were associated with early restenosis, while severe calcification, smaller vessel, and involving popliteal arterial lesions were associated with late restenosis.
Early restenosis indicates “balloon failure” and would potentially result from recoil, which primary stent implantation might be required. On the other hand, late restenosis after 6 months would be attributed to “DCB failure”, with inadequate drug uptake into the arterial wall, which might be minimized by the use of atherectomy devices.
Introduction
Drug-coated balloon (DCB) treatment plays a central role in the endovascular approach for mild-to-moderate femoropopliteal (FP) lesions in symptomatic patients with lower-extremity artery disease (LEAD). Randomized control trials (RCTs) have showed superior long-term outcomes over noncoated balloon angioplasty.1–7 In these trials, the difference of primary patency between DCB and noncoated angioplasty widens especially after 6 months, speculating that the antirestenosis effect of paclitaxel would be manifested 6 months after the treatment. In this context, factors associated with the risk of restenosis after 6 months would potentially differ from those within 6 months. However, previous studies analyzing the risk factors for restenosis after DCB treatment did not distinguish between early and late restenosis events.8–12 The aim of this study was to reveal the prognostic factors associated with early (within 6 months) and late (after 6 months) restenosis after FP DCB treatment in real-world symptomatic LEAD patients with FP lesions.
Materials and Methods
Study Design
This was a multicenter, retrospective, and observational study. Between January 2018 and December 2019, 423 patients with symptomatic LEAD underwent FP DCB treatment for 486 de novo FP lesions without residual stenosis (≥50%) or severe dissection (greater than grade D). The current study was performed in accordance with the declaration of Helsinki and was approved by the ethics committee of each hospital. The current study was an observational research without invasiveness and did not use human biological specimens. Accordingly, the written informed consent of patients was waived in accordance with the ethical guidelines for medical and health research involving human subjects in Japan. Instead, relevant information regarding the study has been made open to the public.
Intervention Procedure
An ipsilateral or contralateral approach was used to obtain vascular access via the common femoral artery under local anesthesia, and a 6Fr guiding sheath was mostly used. After the guiding sheath was placed above the target FP lesion, 5000 units of heparin were routinely injected via the arterial route. A 0.035, 0.018, or 0.014 guidewire was selected according to the lesion morphology at the discretion of the physicians. After the guidewire successfully passed through the entire lesion, intravascular ultrasound (IVUS) was routinely used. Reference vessel diameter (RVD) assessed with IVUS was measured at the most normal-looking sections within 10 mm of the distal margins of the lesion. Intravascular ultrasound–assessed RVD was calculated from the cross-sectional area of the external elastic membrane (EEM), considering the cross-section as a circle. Vessel diameter was evaluated immediately after successful wire crossing before any intervention. If IVUS failed to cross the lesion directly, balloon angioplasty with smaller size (balloon diameter <3 mm) was allowed. Intravascular ultrasound measurement of the vessel diameter was performed by a clinical engineer from each participating hospital. The types and sizes of the balloon for predilatation were determined based on IVUS measurements. After the successful predilatation, one of the two DCBs, IN.PACT Admiral (Medtronic, Minneapolis, MN) with 3.5 μg/mm2 of paclitaxel or Lutonix (BD/Bard, Tempe, AZ) with 2.0 μg/mm2 of paclitaxel, was utilized at the discretion of the operator. The size of the DCB was selected based on IVUS measurement. Drug-coated balloon treatment was performed to exceed the proximal and distal margins of the lesion segment by 5 mm to ensure that the margins of the predilated vessel were covered. If multiple DCBs were needed to cover the full lesion length, the balloons were positioned to ensure overlap of the treated area. Since atherectomy devices were not commercially available in Japan during the study period, they were not used in this study population.
Follow-up Protocol
All participants were scheduled to visit their center for follow-up. Evaluations of ischemic symptoms and the ankle-brachial index were regularly conducted, along with the duplex ultrasound (DUS). Patients were scheduled for follow-up at 1 and 3 months postoperatively, and every 3 months thereafter. If the symptoms recurred with restenosis as diagnosed by the DUS assessment, a follow-up angiography was scheduled.
Dual antiplatelet therapy (100 mg/day aspirin with 75 mg/day clopidogrel or 3.75 mg/day prasugrel) was prescribed for at least 1 week prior to endovascular treatment (EVT) and continued for at least 1 month after EVT. Subsequent therapies were prescribed at the discretion of the treating physicians.
Definition
Restenosis is defined as a peak systolic velocity ratio >2.4 based on DUS findings. The severity of the lesion calcification was classified by Peripheral Arterial Calcium Scoring Systems (PACSS) into 5 groups as follows: no visible calcium at the target lesion site (PACSS, grade 0); unilateral calcification <5 cm (PACSS, grade 1); unilateral calcification ≥5 cm (PACSS, grade 2); bilateral calcification <5 cm (PACSS, grade 3); and bilateral calcification ≥5 cm (PACSS, grade 4). 13 The circumferential grade of calcium was determined by IVUS at the area in which calcification was most extensively distributed circumferentially. 14 The number of below-the-knee runoff vessels was counted as 0–3 based on the anterior tibial, peroneal, and posterior tibial arteries without significant stenosis, assessed using digital subtraction angiography.
Outcome Measure
The outcome measure was restenosis. Early and late restenosis were classified by using the cutoff period of 6 months after the procedure. 15
Statistical Analyses
Continuous variables are given as mean ± standard deviation, and discrete variables are given as frequency (percentage). Continuous and discrete data were compared between groups using unpaired Student’s t-tests and Fisher’s exact tests, respectively. The cumulative incidence restenosis rates after DCB were assessed using the Kaplan-Meier method, and the rates were reported as estimate ± standard error. Predictors associated with restenosis were investigated using the Cox proportional hazard model, and the results are presented as hazard ratio (HR) and 95% confidence interval (CI). Cox proportional-hazards regression analysis was used to determine the associations of clinical, anatomical, and procedural characteristics with restenosis. Multivariate Cox regression analysis was performed to determine the predictors of restenosis. Predictors with significant results (p<0.05) in the univariate analyses were entered into the multivariate Cox regression analysis. SPSS statistics package software (Version 27; IBM, Armonk, NY) was used for all analyses.
Results
Baseline Patient Characteristics
The baseline patient characteristics are summarized in Table 1. The mean age of the patients was 74.3±8.6 years, and 71.2% of the participants were male. The prevalence of diabetes mellitus and hemodialysis was 59.3% and 37.1%, respectively. More than one-third of the patients (41.6%) presented with chronic limb-threatening ischemia (CLTI).
Baseline Patient Characteristics.
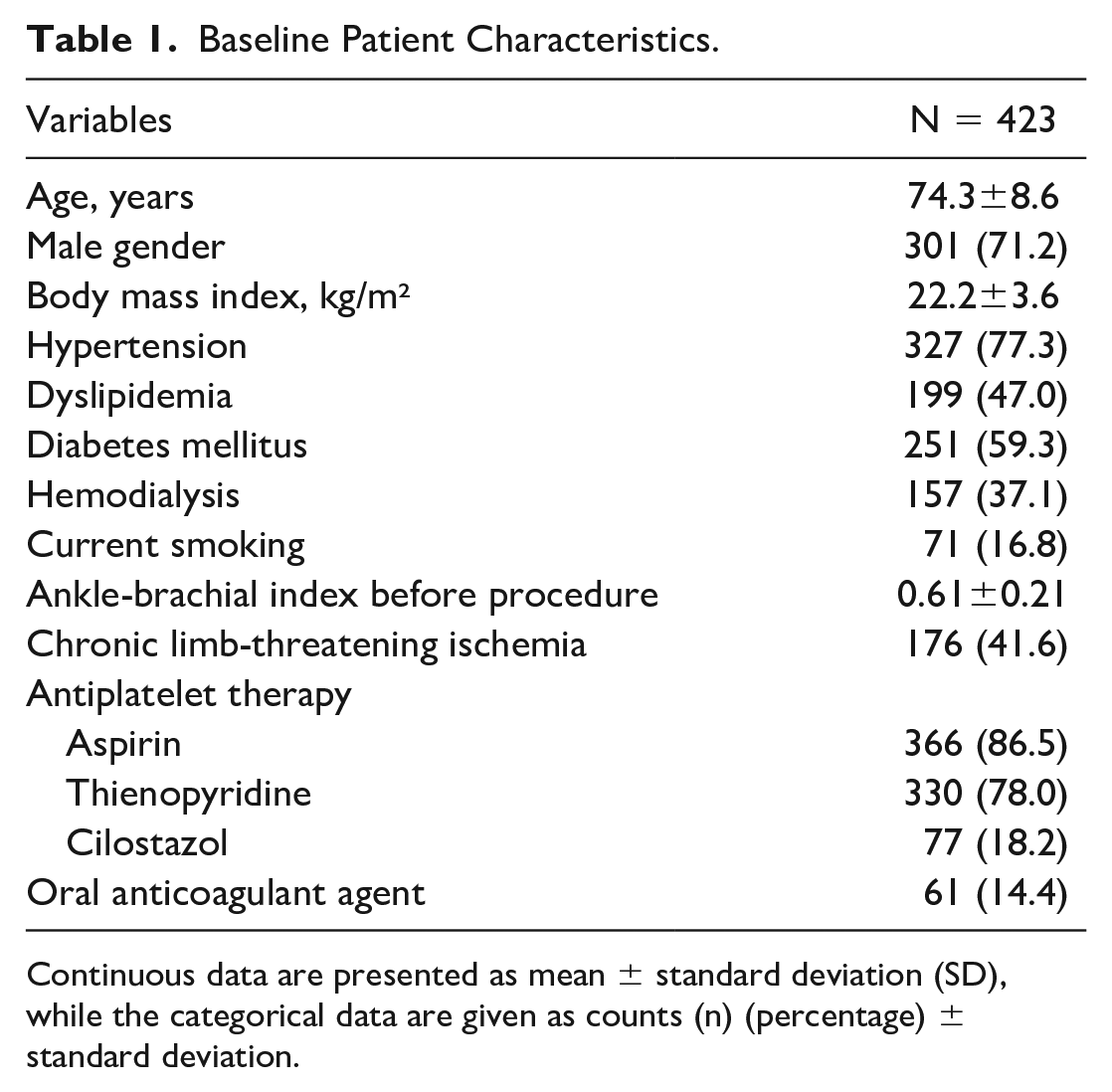
Continuous data are presented as mean ± standard deviation (SD), while the categorical data are given as counts (n) (percentage) ± standard deviation.
Baseline Lesion and Procedural Characteristics
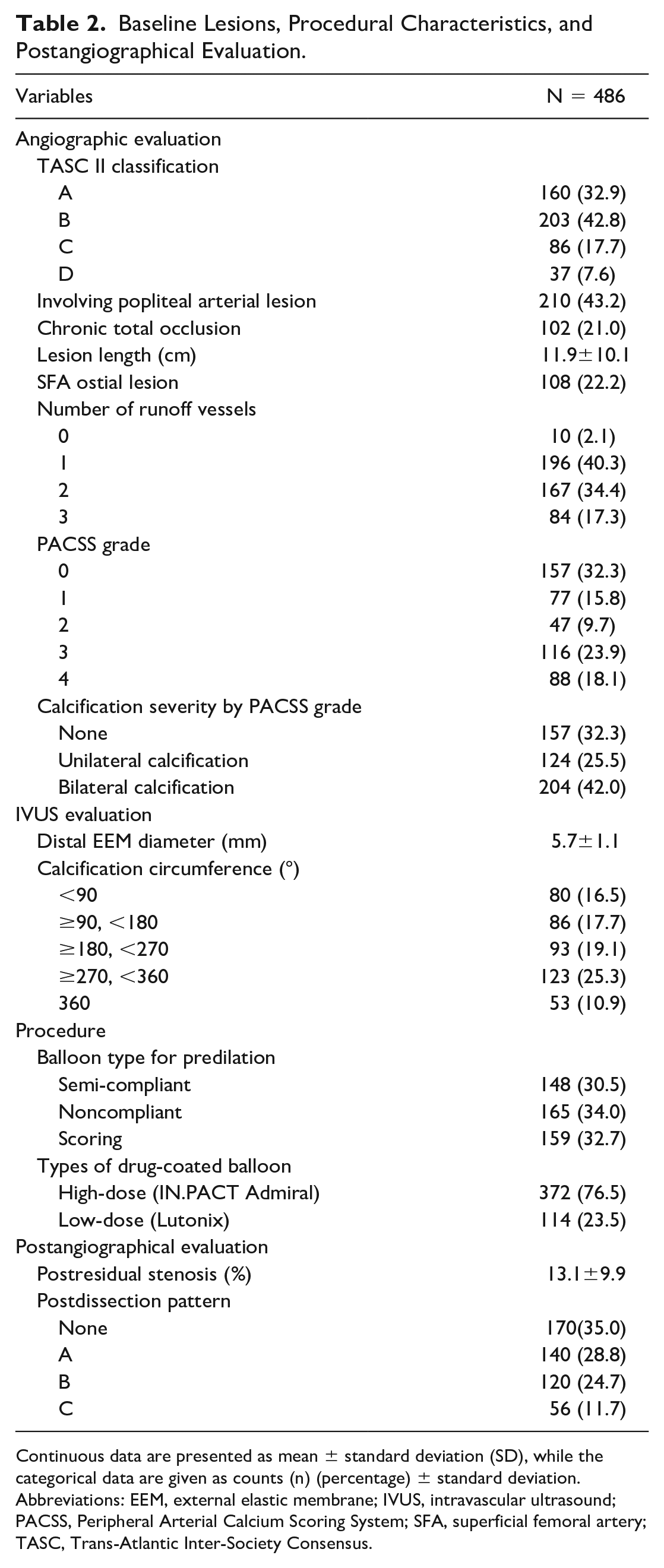
The baseline lesion and procedural characteristics are shown in Table 2. The frequencies of chronic total occlusion (CTO), superficial femoral artery (SFA) ostial lesions, and lesions involving the popliteal artery were 21.0%, 22.2%, and 43.2%, respectively. The mean lesion length was 11.9±10.1 cm. Unilateral and bilateral calcifications were observed in 25.5% (PACSS grade 1: 15.8%, PACSS grade 2: 9.7%) and 42.0% (PACSS grade 3: 23.9%, PACSS grade 4: 18.1%) of the lesions, respectively. The mean distal EEM diameter assessed by IVUS was 5.7±1.1 mm. Of the total 486 lesions, predilation was performed in 472 lesions. Direct DCB angioplasty was performed in the remaining 14 lesions. The type and frequency of balloons used for predilation were semi-compliant, noncompliant, and scoring balloon in 148 (30.5%), 165 (34.0%), and 159 (32.7%) lesions, respectively. A total of 114 lesions (23.5%) were treated with low-dose DCB (Lutonix; BD/Bard), and the remaining 372 lesions (76.5%) were treated with high-dose DCB (IN.PACT Admiral; Medtronic).
Baseline Lesions, Procedural Characteristics, and Postangiographical Evaluation.
Continuous data are presented as mean ± standard deviation (SD), while the categorical data are given as counts (n) (percentage) ± standard deviation.
Abbreviations: EEM, external elastic membrane; IVUS, intravascular ultrasound; PACSS, Peripheral Arterial Calcium Scoring System; SFA, superficial femoral artery; TASC, Trans-Atlantic Inter-Society Consensus.
Outcome Measure
During the mean follow-up period of 25.3±12.1 months, early and late restenosis were observed in 31 and 168 lesions, respectively. The Kaplan-Meier estimates of the 6, 12, 18, and 24 month incidence of restenosis were 7.4%±2.4%, 20.9%±3.9%, 29.9%±4.5%, and 38.4%±5.1%, respectively (Supplementary Figure 1). Also, the target lesion revascularization rate at 6, 12, 18, and 24 months were 3.5%±1.8%, 8.2%±2.5%, 13.0%±3.3%, and 18.4%±3.9% (Supplementary Figure 2), and the major amputation rate at 6, 12, 18, and 24 months were 0.0%±0.0%, 1.2%±0.9%, 2.3%±1.6%, and 4.1%±2.0%, respectively (Supplementary Figure 3).
Risk Factors for Early and Late Restenosis
Table 3 demonstrates the association between the baseline characteristics and early restenosis within 6 months after DCB treatment. After the multivariate analysis, CTO (HR, 2.29; 95% CI, 1.07–4.92; p=0.033) and SFA ostial lesion (HR, 2.73; 95% CI, 1.28–5.80; p=0.009) were significantly associated with early restenosis. In addition, the dissection grade was more severe in SFA ostial lesions than in non-SFA ostial lesions (the frequency of grade B or C dissection: 47.2% in lesion with SFA ostium versus 33.1% in lesion without SFA ostium, p=0.033). The cumulative restenosis rate within 6 months increased with the accumulation of the risk factors of early restenosis (Figure 1).
Predictors of Early Restenosis Within 6 Months After DCB Treatment.
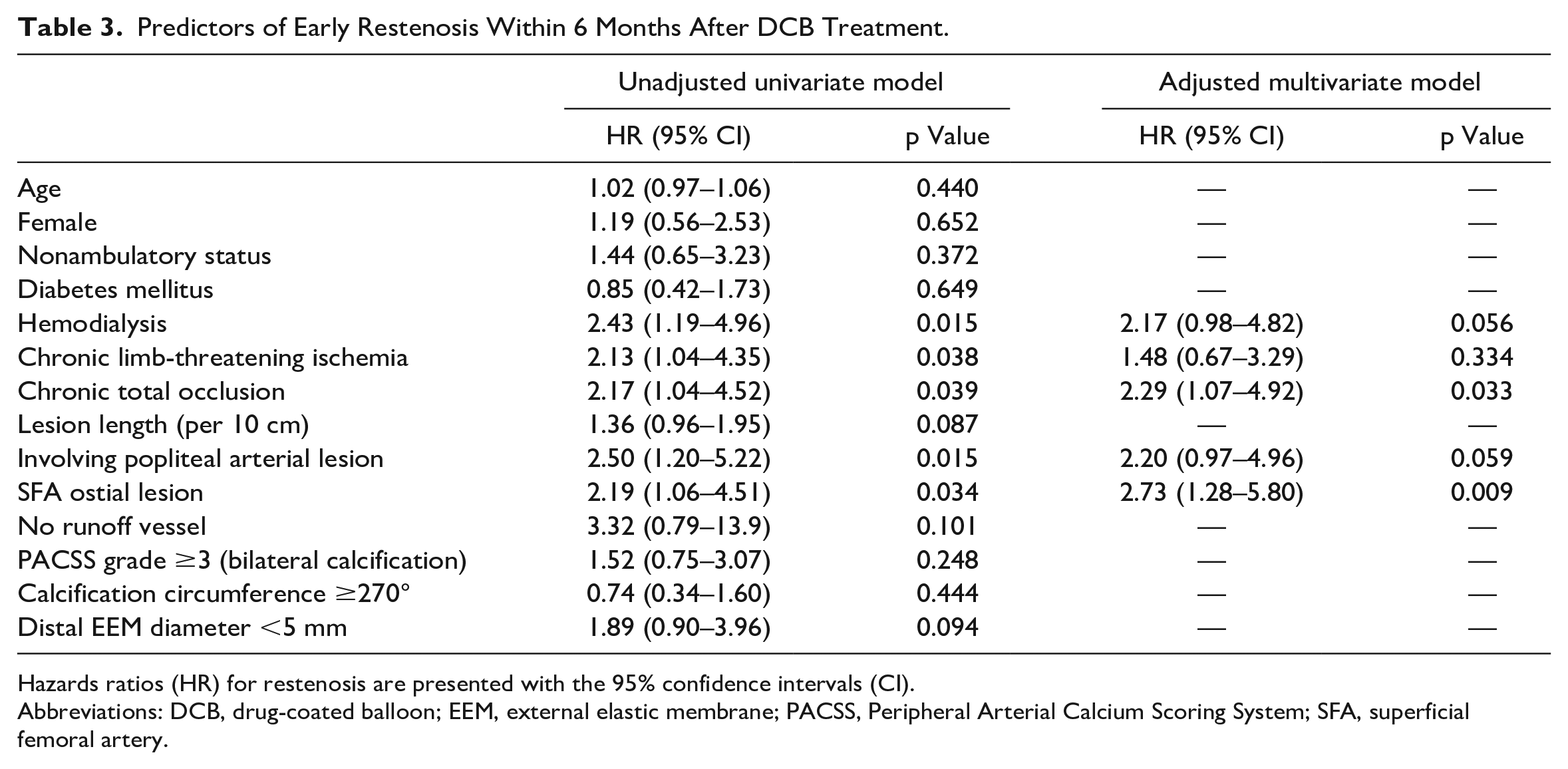
Hazards ratios (HR) for restenosis are presented with the 95% confidence intervals (CI).
Abbreviations: DCB, drug-coated balloon; EEM, external elastic membrane; PACSS, Peripheral Arterial Calcium Scoring System; SFA, superficial femoral artery.
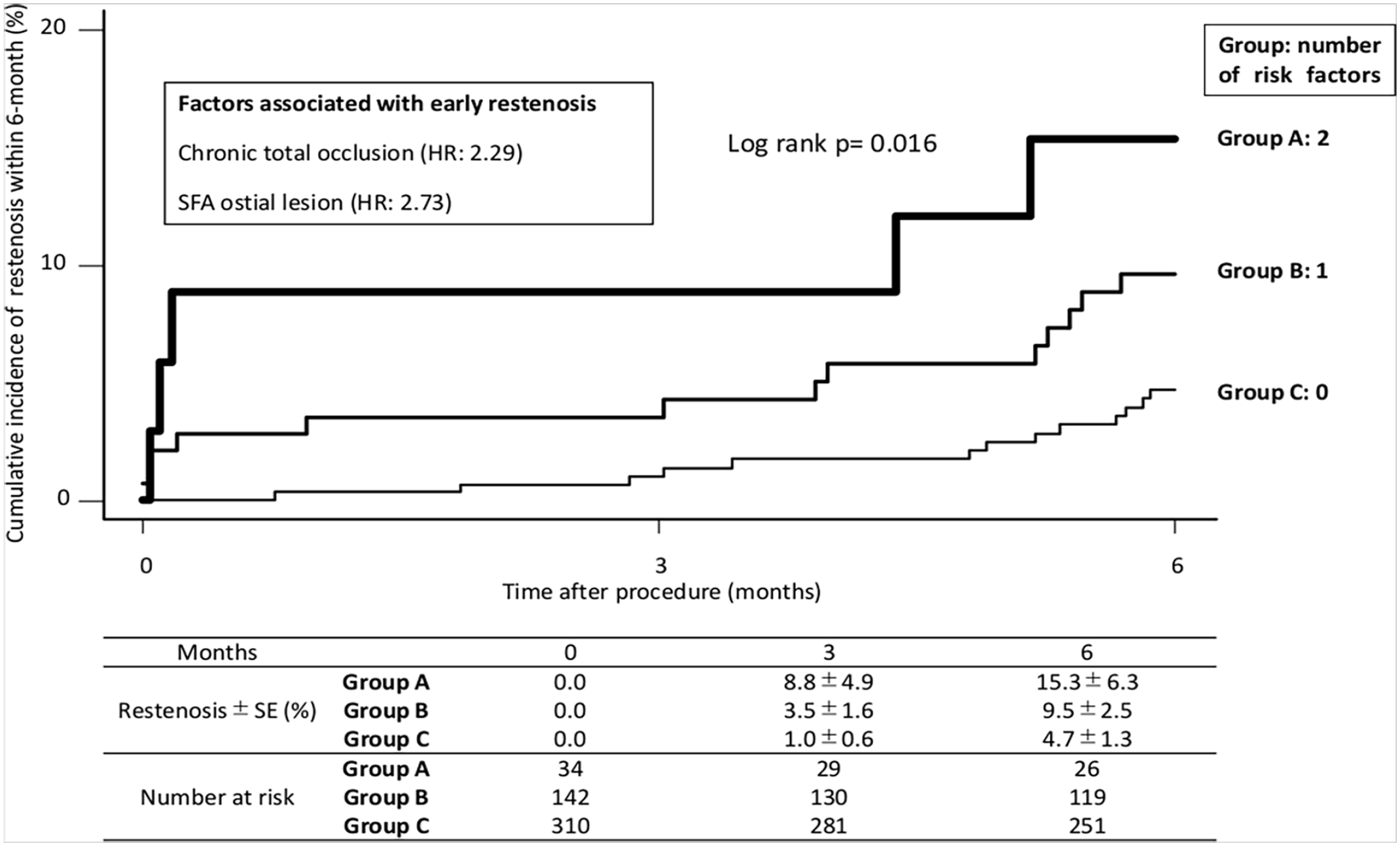
Cumulative restenosis rate within 6 months stratified by a number of risk factors associated with early restenosis. From multivariate analysis, the risk factors associated with early restenosis were chronic total occlusion and SFA ostial lesion. Lesions were assigned to groups (A, B, C) based on the number of multivariate risk factors. The cumulative incidence of restenosis within 6 months significantly increased with the accumulation of the risk factors (p=0.016). SFA, superficial femoral artery.
Table 4 demonstrates the association between the baseline characteristics and late restenosis 6 months after the procedure. The multivariate analysis revealed that calcification circumference over 270° (HR, 1.67; 95% CI, 1.17–2.37; p=0.004), distal EEM diameter under 5 mm (HR, 1.90; 95% CI, 1.29–2.79; p=0.001), and popliteal arterial lesion (HR, 1.54; 95% CI, 1.08–2.21; p=0.017) were significantly associated with late restenosis. In addition, popliteal artery lesions had significantly smaller vessel diameters (p<0.001) and had more lesions with severe calcification (p<0.001) than SFA lesions. The cumulative restenosis rate after 6 months increased with the accumulation of these risk factors (Figure 2).
Predictors of Late Restenosis 6 Months After DCB Treatment.
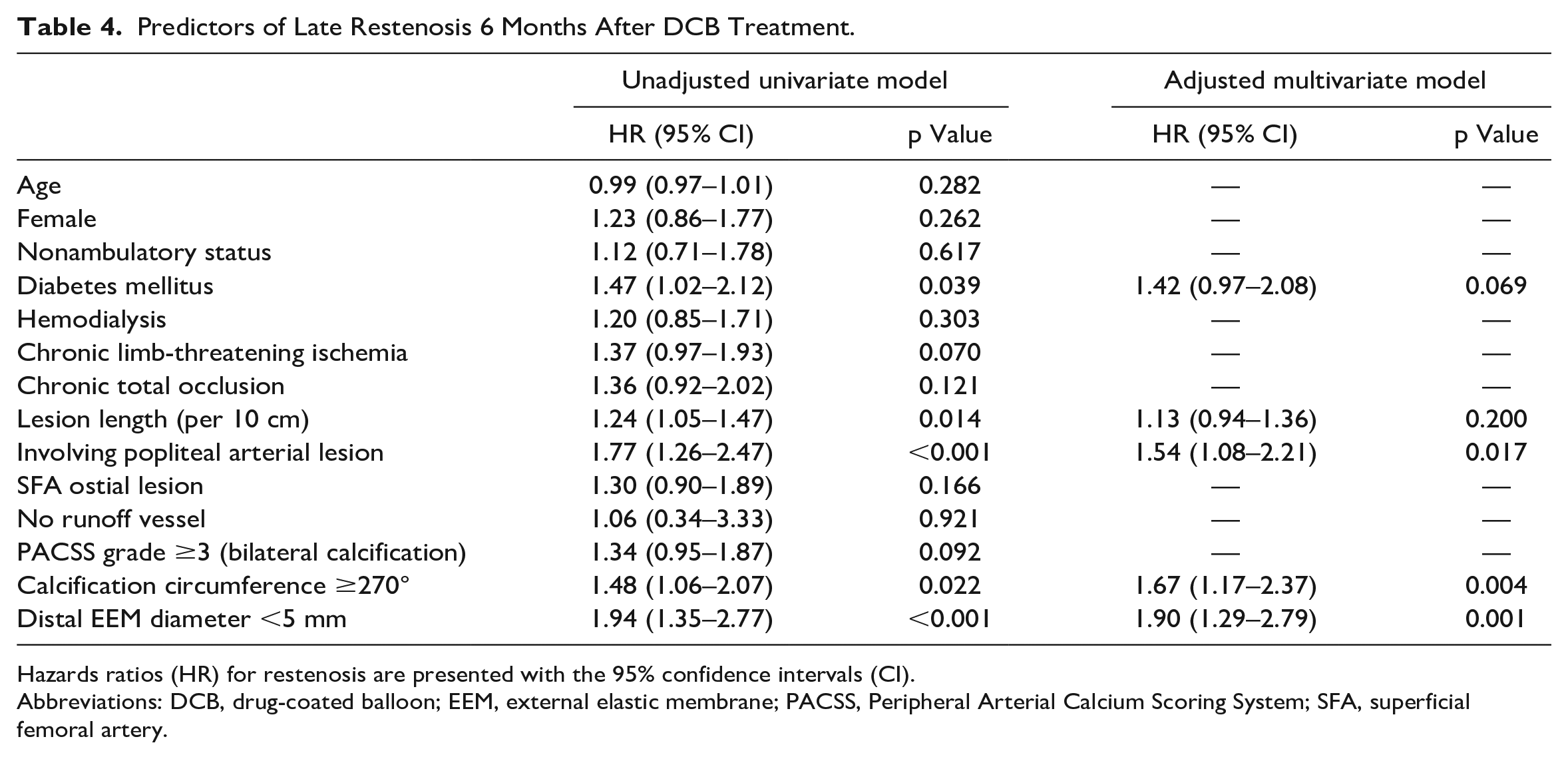
Hazards ratios (HR) for restenosis are presented with the 95% confidence intervals (CI).
Abbreviations: DCB, drug-coated balloon; EEM, external elastic membrane; PACSS, Peripheral Arterial Calcium Scoring System; SFA, superficial femoral artery.
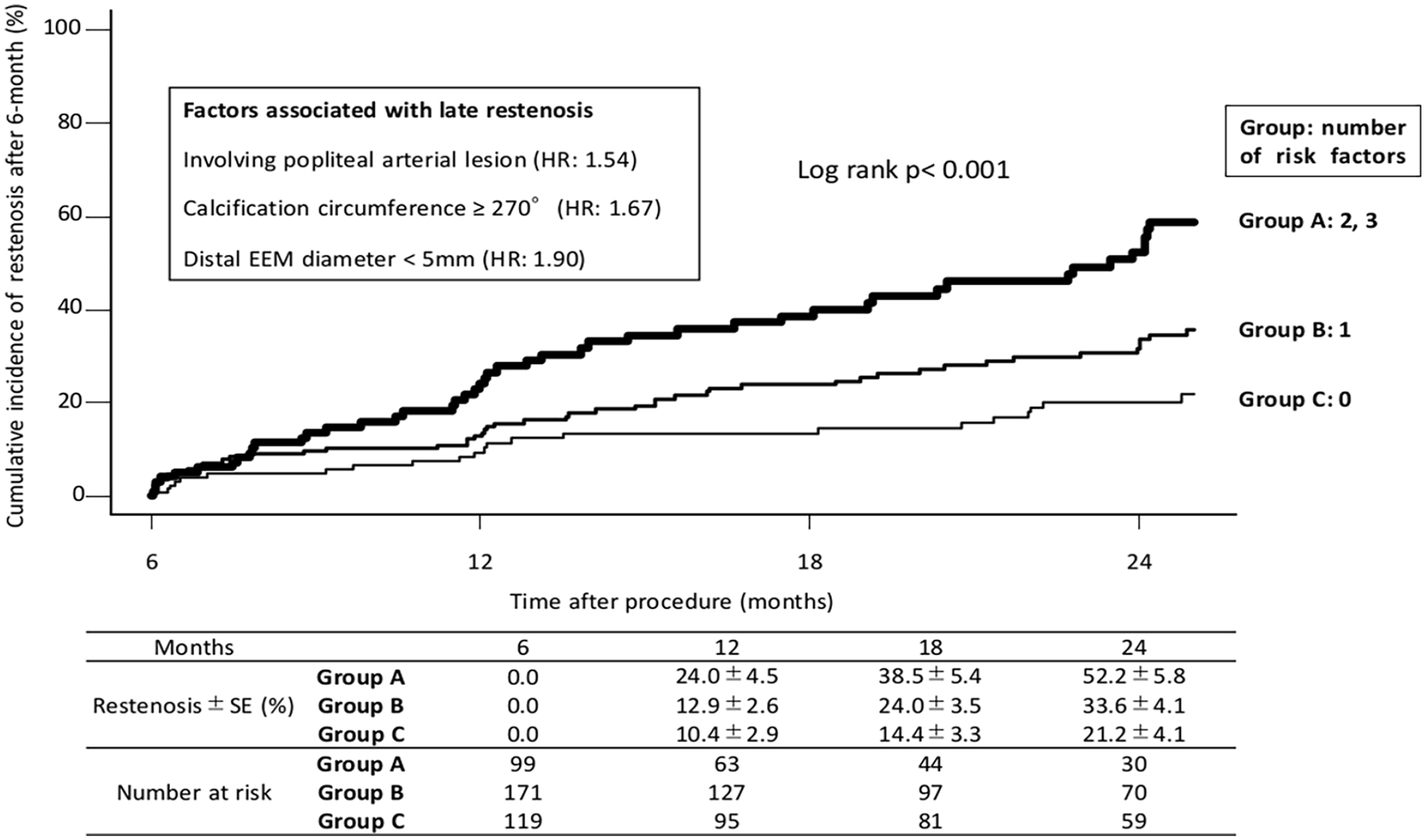
Cumulative restenosis rate after 6 months stratified by a number of risk factors associated with late restenosis. From multivariate analysis, the risk factors associated with late restenosis were lesions involving popliteal arterial lesion, calcification circumference over 270°, and distal EEM diameter under 5 mm. Lesions were assigned to groups (A, B, C) based on the number of multivariate risk factors. The cumulative incidence of restenosis after 6 months significantly increased with the accumulation of risk factors (p<0.001). EEM, external elastic membrane; HR, hazards ratios.
The overall predictors of restenosis are listed in Supplementary Table 1. The predictors of restenosis after a multivariate analysis in the overall cohort were CTO, SFA ostial lesion, involving popliteal arterial lesion, and distal EEM diameter under 5 mm.
Cumulative Incidence of Restenosis Between Low-Dose DCB and High-Dose DCB
The difference in restenosis rate between low-dose DCB and high-dose DCB treatment was compared. In terms of early restenosis, there was no difference between low-dose and high-dose DCB groups (Figure 3A). However, late restenosis rate was significantly higher in the low-dose DCB group than that in the high-dose DCB group (Figure 3B).
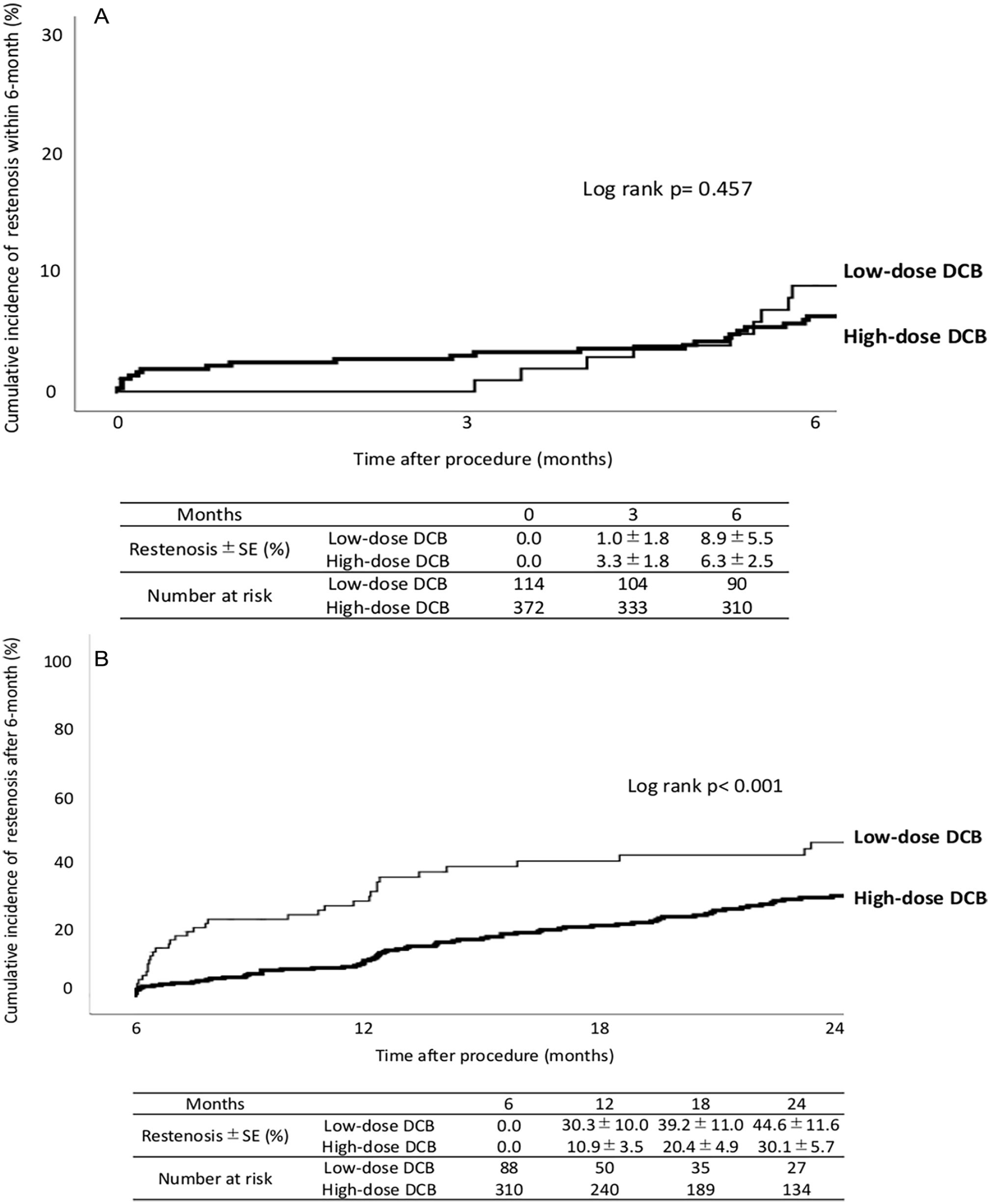
(A) Early restenosis rate within 6 months between low-dose and high-dose drug-coated balloon angioplasty for patients with femoropopliteal lesions. (B) Late restenosis rate after 6 months between low-dose and high-dose drug-coated balloon angioplasty for patients with femoropopliteal lesions. There was no difference in early restenosis rate between low-dose and high-dose drug-coated balloon treatment. Late restenosis rate was significantly higher in low-dose drug-coated balloon group than that in the high-dose drug-coated balloon group (p<0.001).
Discussion
Summary of the Current Study
The current study revealed that CTO and SFA ostial lesion were significantly associated with early restenosis, while calcification circumference over 270°, distal EEM diameter under 5 mm assessed by IVUS, and popliteal arterial lesion were significantly associated with late restenosis. To the best of our knowledge, this is the first study to identify the different predictors of early and late restenosis following DCB treatment in real-world FP practice.
Previous Reports on Factors Associated With DCB Treatment
Clinical trials reported the superiority of DCB in primary patency over noncoated angioplasty for the treatment of FP lesions. However, primary patency did not differ between DCB and noncoated angioplasty within 6 months; the superiority of DCB over noncoated angioplasty in primary patency appeared 6 months after the treatment.1,5 This shows that the antirestenosis effect of paclitaxel would not be manifested until 6 months after the treatment. Accordingly, early restenosis within 6 months after the DCB therapy could be attributed to “balloon failure” rather than “DCB failure,” whereas late restenosis would reflect failure of the drug technology.
Factors Associated With Early Restenosis
Previous studies reported that the female gender, lesion length, CLTI, CTO, smaller distal reference vessel, popliteal lesions, and heavily calcified lesions were factors associated with restenosis after DCB treatment for the FP lesions.8–12 The current study revealed that CTO and SFA ostial lesions were significantly associated with early restenosis within 6 months following DCB treatment. Generally, CTO lesions are known as a challenging phenotype to achieve optimal outcome for EVT. The higher grade of plaque burden would lead to the presence of elastic recoil, which is speculated as a main mechanism of early restenosis. Chronic total occlusion lesions might be a factor that strongly affects the acute outcomes given the high provisional stenting rate in the treatment of CTO lesions. 9 To overcome early restenosis in CTO lesions, deployment of scaffolds would be beneficial in preventing vessel recoil and could help in reducing the risk of early restenosis. On the other hand, to our knowledge, SFA ostial lesions have never been reported as an associated factor after DCB treatment although they have been reported to be an independent predictor of loss of patency after stent treatment in FP lesions. 16 Atherosclerosis is often developed at the femoral bifurcation caused by the shearing stress to the vessel wall associated with the anatomy of this particular location.17,18 In the current study, the dissection pattern did not show a significant association with early restenosis. However, the dissection grade was more severe in SFA ostial lesions than in non-SFA ostial lesions. The postangioplasty dissections have been reported to be associated with both short- and long-term adverse outcomes, with severe dissections correlated with worse outcomes.19–21 The speculated mechanism of early restenosis occurrence in SFA ostial lesions might be attributed to vessel dissection. Scaffold implantation might be effective especially in cases in which the dissection grade of SFA ostium is severe to avoid early restenosis in lesions involving SFA ostium.
Factors Associated With Late Restenosis
In our study, the calcification severity, smaller vessel diameter, and involving popliteal arterial lesions were significantly associated with late restenosis. These risk factors overlapped with those reported in previous studies. Schmidt et al 8 reported that severe calcifications were responsible for significantly lower primary patency and were independent risk factors for restenosis. Severe calcification alters the morphology and the compliance of the vessel wall. An increased calcium burden limits the drug uptake in the arterial wall and decrease the antiproliferative effect of paclitaxel.14,22 To overcome severe calcification, the use of atherectomy devices and also intravascular lithotripsy may improve the efficiency of drug penetration.23,24 Debulking techniques might further expand the application of DCBs in severely calcified lesions and lead to better clinical and radiological outcomes in “leave nothing behind” strategies. 22
A smaller vessel diameter has been reported as an independent predictor of restenosis after DCB treatment, as well as any scaffolding, and was also significant in the current study.22,25 In addition, previous studies showed that the lesions that are located exclusively on the SFA had significantly higher primary patency than the lesions encompassing the popliteal artery.9,26 The popliteal artery has unique anatomical characteristics and is subjected to significant biomechanical forces that result from the repetitive flexion and extension of the knee joint. 27 Clinical outcomes of DCB angioplasty alone for isolated popliteal lesion have been reported to be suboptimal.28,29 We speculated that the reason why popliteal arterial lesions have a higher risk of restenosis is due to a different multifactorial component and a more complex anatomical background than SFA lesions. In practice, the current study revealed that popliteal arterial lesions had significantly smaller vessel diameters (p<0.001) and had more lesions with severe calcification (p<0.001), suggesting that the difference in lesion severity between popliteal arterial lesions and SFA lesions had an association with this result.
How Can We Intervene to Resolve Early and Late Restenosis?
Early restenosis within 6 months indicates “balloon failure” and would potentially result from recoil, which is mainly caused by CTO or severe dissection related with SFA ostial lesions. To avoid recoil in those high-risk lesions, primary stent implantation might be required. Nonstenting angioplasty, regardless of the drug technology, might render the issue of recoil difficult to address. On the other hand, late restenosis after 6 months would be attributed to “DCB failure,” with inadequate drug uptake into the arterial wall. The risk of late restenosis might be minimized by the use of atherectomy devices and large-sized DCBs, which possibly increase the homogeneity of the drug application into the vessel wall and enhance the effectiveness of DCB.
Study Limitations
The present study has some limitations. First, this was a multicenter, retrospective study with a limited sample size, so there may have been selection bias. Moreover, only Japanese patients with FP lesions were included. Thus, the results need to be validated in other ethnic groups. Second, this was a nonblinded study, that is, the angiographic or IVUS analysis was not assessed by a blinded committee and also was not analyzed by an independent core laboratory, and there could have been an unintentional lack of blindness and bias in the analysis. However, determination of these findings was based on the agreement between the operator and a clinical engineer who were experienced in conducting clinical studies on FP endovascular devices in each participating centers. We believe that these accumulated experiences minimize the variability. Third, atherectomy devices were not used because they were not reimbursed and were not available during this period in Japan. Finally, since this study evaluated patients treated by DCB without a control group, the true advantage of DCB over noncoated balloon treatment and factors associated with restenosis in each treatment can only be evaluated by RCTs.
Conclusion
The current study revealed that the factors associated with late restenosis differed from those associated with early restenosis in the real-world FP-DCB practice. Chronic total occlusion and SFA ostial lesions were associated with early restenosis, while severe calcification, a smaller vessel, and popliteal arterial lesions were associated with late restenosis.
Supplemental Material
sj-docx-1-jet-10.1177_15266028231186717 – Supplemental material for Factors Associated With Early and Late Restenosis Following Drug-Coated Balloon Treatment for Patients With Femoropopliteal Lesions
Supplemental material, sj-docx-1-jet-10.1177_15266028231186717 for Factors Associated With Early and Late Restenosis Following Drug-Coated Balloon Treatment for Patients With Femoropopliteal Lesions by Taku Toyoshima, Osamu Iida, Mitsuyoshi Takahara, Shin Okamoto, Takayuki Ishihara, Kiyonori Nanto, Takuya Tsujimura, Yosuke Hata, Naoko Higashino, Sho Nakao, Tomofumi Tsukizawa, Kunihiko Nishian, Masahiko Fujihara, Daizo Kawasaki and Toshiaki Mano in Journal of Endovascular Therapy
Supplemental Material
sj-docx-2-jet-10.1177_15266028231186717 – Supplemental material for Factors Associated With Early and Late Restenosis Following Drug-Coated Balloon Treatment for Patients With Femoropopliteal Lesions
Supplemental material, sj-docx-2-jet-10.1177_15266028231186717 for Factors Associated With Early and Late Restenosis Following Drug-Coated Balloon Treatment for Patients With Femoropopliteal Lesions by Taku Toyoshima, Osamu Iida, Mitsuyoshi Takahara, Shin Okamoto, Takayuki Ishihara, Kiyonori Nanto, Takuya Tsujimura, Yosuke Hata, Naoko Higashino, Sho Nakao, Tomofumi Tsukizawa, Kunihiko Nishian, Masahiko Fujihara, Daizo Kawasaki and Toshiaki Mano in Journal of Endovascular Therapy
Supplemental Material
sj-tif-3-jet-10.1177_15266028231186717 – Supplemental material for Factors Associated With Early and Late Restenosis Following Drug-Coated Balloon Treatment for Patients With Femoropopliteal Lesions
Supplemental material, sj-tif-3-jet-10.1177_15266028231186717 for Factors Associated With Early and Late Restenosis Following Drug-Coated Balloon Treatment for Patients With Femoropopliteal Lesions by Taku Toyoshima, Osamu Iida, Mitsuyoshi Takahara, Shin Okamoto, Takayuki Ishihara, Kiyonori Nanto, Takuya Tsujimura, Yosuke Hata, Naoko Higashino, Sho Nakao, Tomofumi Tsukizawa, Kunihiko Nishian, Masahiko Fujihara, Daizo Kawasaki and Toshiaki Mano in Journal of Endovascular Therapy
Supplemental Material
sj-tif-4-jet-10.1177_15266028231186717 – Supplemental material for Factors Associated With Early and Late Restenosis Following Drug-Coated Balloon Treatment for Patients With Femoropopliteal Lesions
Supplemental material, sj-tif-4-jet-10.1177_15266028231186717 for Factors Associated With Early and Late Restenosis Following Drug-Coated Balloon Treatment for Patients With Femoropopliteal Lesions by Taku Toyoshima, Osamu Iida, Mitsuyoshi Takahara, Shin Okamoto, Takayuki Ishihara, Kiyonori Nanto, Takuya Tsujimura, Yosuke Hata, Naoko Higashino, Sho Nakao, Tomofumi Tsukizawa, Kunihiko Nishian, Masahiko Fujihara, Daizo Kawasaki and Toshiaki Mano in Journal of Endovascular Therapy
Supplemental Material
sj-tif-5-jet-10.1177_15266028231186717 – Supplemental material for Factors Associated With Early and Late Restenosis Following Drug-Coated Balloon Treatment for Patients With Femoropopliteal Lesions
Supplemental material, sj-tif-5-jet-10.1177_15266028231186717 for Factors Associated With Early and Late Restenosis Following Drug-Coated Balloon Treatment for Patients With Femoropopliteal Lesions by Taku Toyoshima, Osamu Iida, Mitsuyoshi Takahara, Shin Okamoto, Takayuki Ishihara, Kiyonori Nanto, Takuya Tsujimura, Yosuke Hata, Naoko Higashino, Sho Nakao, Tomofumi Tsukizawa, Kunihiko Nishian, Masahiko Fujihara, Daizo Kawasaki and Toshiaki Mano in Journal of Endovascular Therapy
Footnotes
Acknowledgements
The authors also would like to express their appreciation to Mr Naoya Kurata, Ms Yuko Yazu, and Ms Aya Nakata for their expertise in performing the IVUS examinations.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: O.I. received honoraria from Medtronic and Becton Dickinson.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.