
Abstract
Objective:
The purpose of this study was to evaluate the technical feasibility, safety, and early outcomes of a snare-less, endovascular abdominal aortic aneurysm repair (EVAR)-first technique (SET) for iliac branch endoprosthesis (IBE) placement.
Methods:
We retrospectively reviewed all patients who received IBEs between July 2018 and March 2022. Patients were divided into 2 categories based on method of IBE deployment: SET or Standard. Primary endpoints were technical success, major adverse events, mortality, reintervention, internal iliac artery (IIA) patency, and freedom from IIA branch instability. Technical success was defined by successful deployment of both the EVAR and the IBE with maintained patency of the IIA and no stent graft migration.
Results:
There were 20 patients (90% male, median age 72 [65.4-74.5] years) who underwent IBE placement. Among these, 5 (33.3%) underwent SET to treat 5 common iliac artery (CIA)/IIA aneurysms, while the remaining 15 (66.7%) underwent standard IBE deployment with through-and-through femoral access (n=13) or trans-brachial access (n=2) to treat 19 CIA/IIA aneurysms. Overall median renal to iliac bifurcation length was 169 (152-177) mm, with 9 patients falling short of the minimum of 165 mm for on-label IBE placement. Median contrast used was 148 (120-201) mL, fluoroscopy time 42.8 (35.0-49.8) minutes, estimated blood loss 200 (100-275) mL, and procedure time 192 (167-246) minutes, with no significant differences between the 2 groups. Technical success was achieved in 100% of cases. At 30 days, there were no mortalities or major adverse events in either group; there were 100% IIA patency, no IIA instability, and no reinterventions in both groups. Median follow-up in the SET group was 5.7 (5.5-6.2) months, with 1 death at 6 months and 1 type 1B endoleak at 6 months requiring reintervention. Median follow-up for the Standard group was 1.6 (0.8-2.1) years with 2 non–aneurysm-related deaths and no reinterventions at 1 year.
Conclusions:
SET for IBE is a safe and effective approach that decreases technical complexity and mitigates anatomic barriers to IBE placement.
Clinical Impact
SET for IBE is a safe and effective approach to IBE placement that decreases technical complexity. A critical component to this technique is a large bore sheath with a stiff steerable tip. Importantly, this approach also mitigates anatomic barriers to IBE placement, expanding applicability of IBE technology to patients who may be otherwise ineligible.
Keywords
Background
Maintaining patency to the internal iliac artery (IIA) during aorto-iliac aneurysm repair is recommended to decrease complication rates related to pelvic ischemia.1,2 Iliac branch devices are now the preferred option for IIA preservation in the context of aneurysmal aorto-iliac disease. In the United States, the Gore Excluder iliac branch endoprosthesis (IBE; W. L. Gore & Associates, Inc, Flagstaff, Arizona) remains the only Food and Drug Administration (FDA)–approved device, while in Canada and Europe, the Cook Zenith iliac side-branched stent graft (Cook Medical, Bloomington, Indiana) and the E-iliac Stent Graft System (JOTEC GmbH, Hechingen, Germany) are also commercially available. Manufacturers’ instructions for use (IFU) of each graft require specific anatomic criteria. For IBE technology in particular, anatomical constraints exclude greater than 50% of patients, most commonly because of common iliac artery (CIA)/IIA unsuitability or inadequate renal to iliac bifurcation length.3–7 All 3 grafts also require snaring of a wire from the contralateral groin for through-and-through femoral access. In patients who have had previous open or endovascular aorto-bi-iliac reconstruction, a raised and narrow aortic bifurcation makes this maneuver challenging.
In the past, our group has addressed IBE-ineligible anatomy with various techniques to preserve IIA patency. Most recently, we described pairing the AFX2 endograft (Endologix, Inc, Irvine, California) with the IBE as an off-label solution to overcome the renal to iliac bifurcation length requirement.8,9 However, this technique still requires through-and-through wire access, and patients must still meet specific anatomic criteria for AFX2 placement.
We have since evolved our strategy to a much simpler snare-less, EVAR-first technique (SET) for IBE which is compatible with any aortic endograft, eliminates the need for through-and-through wire access, and removes the renal-to-iliac bifurcation length requirement. Furthermore, this technique allows for placement of IBEs in patients who have previously undergone open or endovascular aortic repair, without brachial/axillary access or through-and-through access. We describe our early experience here.
Materials and Methods
This study was approved by the institutional review board at the Yale School of Medicine. All patients who underwent IBE placement from July 2018 to March 2022 were retrospectively reviewed. Patient demographics and clinical and operative data were abstracted from medical records. Preoperative and postoperative computed tomography (CT) scans were reviewed to obtain anatomic measurements and evaluated for postoperative graft–related complications. Patients were divided into 2 categories based on method of IBE deployment: SET or Standard.
Snare-Less, EVAR-First Technique (SET) Group
Standard percutaneous EVAR is first performed using an aortic endograft of choice, with iliac limb extensions to bilateral iliac bifurcations (Figure 1A–F). Ipsilateral to the target CIA/IIA aneurysm, the IBE is advanced retrograde via femoral access over a Lunderquist Extra-Stiff wire (Cook Medical) and partially deployed until the side branch is released, per manufacturer’s protocol. Adequate overlap into the previously placed EVAR limb extension is ensured. From the contralateral groin, a Heli-FX Guide 22 or 28 mm steerable sheath (Medtronic Aortic, Inc, Santa Rosa, California) is advanced and positioned at the aortic endograft flow-divider. The tip is angled 180° (Figure 1B). Through the Heli-FX, a Glidewire (Terumo Medical Corporation, Somerset, New Jersey) and the Berenstein catheter are advanced over the flow-divider and used to select the side branch followed by the native IIA (Figure 1C). Wire and catheter are advanced well into an IIA branch, and exchange is made for a Rosen wire (Cook Medical) or a flexible-tip Amplatz Super Stiff wire (Boston Scientific Corporation, Boston, Massachusetts). A Viabahn Balloon-Expandable Endoprosthesis (VBX; W. L. Gore & Associates, Inc) is advanced through the Heli-FX over the stiff wire and positioned and deployed into the IIA or IIA branch, ensuring adequate distal seal. A second VBX is deployed if needed for adequate overlap into the IBE side branch. Self-expanding Viabahn Endoprosthesis (W.L. Gore & Associates, Inc) is used in cases of significant IIA tortuosity. The remainder of the IBE is deployed into the external iliac artery (EIA), and an additional EIA stent is added if necessary for adequate distal seal within the EIA (Figure 1D). Kissing balloon angioplasty of the IIA and EIA is performed (Figure 1E). Reliant (Medtronic Aortic, Inc) balloon angioplasty of the IBE and EVAR limb overlap segment is performed.

(A) Initial aortic angiography of a 45 mm right common iliac artery (CIA) aneurysm; (B) after standard endovascular abdominal aortic aneurysm repair (EVAR) is performed, the iliac branch endoprosthesis (IBE) is deployed on the ipsilateral side to release the side branch; the Heli-FX Guide steerable sheath is then inserted from the contralateral groin, and the stiff tip is angled 180° to traverse the endograft flow-divider; (C) in left anterior oblique projection, the side branch and native internal iliac artery (IIA) are selected; (D) after exchange for a stiff wire with an atraumatic tip, a balloon-expandable stent is deployed into the IIA with adequate overlap into the side branch; (E) kissing balloon angioplasty of the external and internal iliac arteries is performed; (F) completion angiography demonstrates exclusion of the CIA aneurysm with preservation of the IIA.
Standard Group
Patients in this group underwent standard IBE deployment per manufacturer protocol using a through-and-through femoral wire if they did not have a pre-existing aortic graft. Those who had undergone previous open or endovascular aortic repair underwent unilateral femoral access for IBE delivery and brachial/axillary access for IIA cannulation and stent graft delivery.
Follow-up
Routine postoperative imaging protocol was computed tomography angiography (CTA) with venous delay at 1, 6, and 12 months, followed by annual non-contrast CT and ultrasound sonography (US). Primary endpoints were technical success, major adverse events, mortality, reintervention, IIA patency, and freedom from IIA branch instability. Technical success was defined by successful deployment of both the EVAR and the IBE with maintained patency of the IIA and no stent graft migration. Major adverse events included mortality, myocardial infarction, stroke, renal failure, bleeding requiring transfusion, respiratory failure, and bowel ischemia. Internal iliac artery branch instability was a composite outcome, which included branch occlusion, stenosis, component separation, endoleak, and the need for any branch-related reintervention. 10
Statistics
Continuous variables were described using medians and interquartile range (IQR). Categorical variables are presented in numbers (percentage). Comparison of independent groups was performed using the Mann-Whitney U test for continuous variables or the Fischer exact test for categorical variables. Follow-up time for endoleak, reintervention, and death were defined as the time from the index operation to the date of the outcome, date of death, or date of lost to follow-up. Lost to follow-up was defined as missing 1 or more scheduled imaging studies with no further radiological or clinical follow-up. All follow-up data mentioned are based on radiological follow-up, except for mortality, which is based on clinical follow-up. Analyses were performed using R software version 4.1.1 (The R Foundation, Vienna, Austria).
Results
Between July 2018 and March 2022, 20 patients (90% male, median age 72 [65.4-74.5] years) underwent IBE placement. Among these, 5 (33.3%) underwent SET to treat 5 CIA/IIA aneurysms, while the remaining 15 (66.7%) underwent standard IBE deployment with through-and-through femoral access (n=13) or trans-brachial access (n=2) to treat 19 CIA/IIA aneurysms. SET was initially developed in May 2021 for treatment of a 4 cm IIA aneurysm in a patient with previous contralateral IIA coil embolization and aortic endograft in place. Because of the ease and simplicity of the technique, it was subsequently used in all IBE cases from that timepoint forward.
Patients in both groups had similar demographics, comorbidities, and anatomical aorto-iliac characteristics. Median renal to iliac bifurcation length was 169 mm, with 9 patients falling short of the minimum of 165 mm for on-label IBE placement. There were 3 patients with previous EVAR in place (2 Standard, 1 SET) and 1 patient with a previous open aorto-bi-iliac repair (Standard) (Table 1).
Baseline Characteristics (Standard Technique vs SET for IBE Deployment).
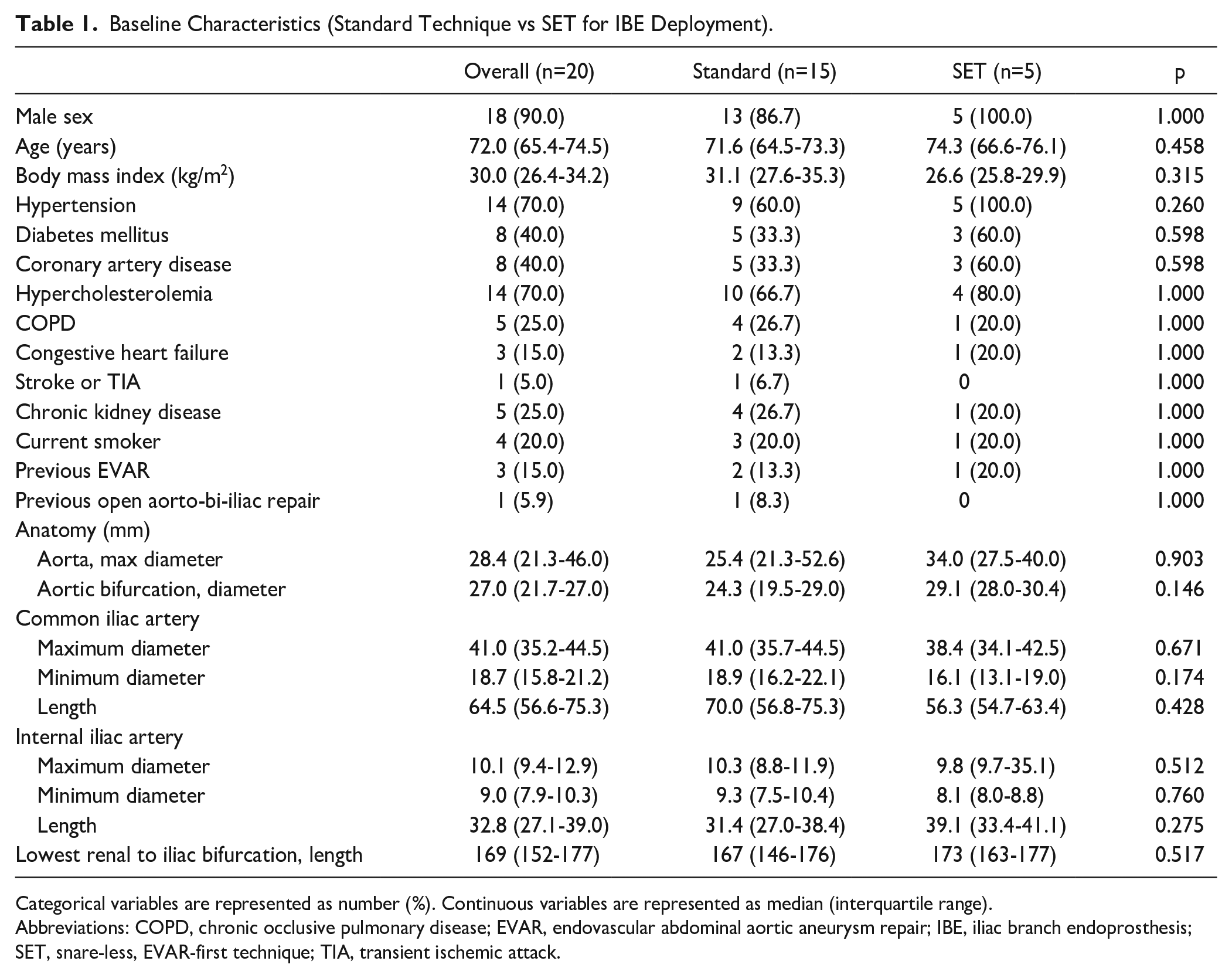
Categorical variables are represented as number (%). Continuous variables are represented as median (interquartile range).
Abbreviations: COPD, chronic occlusive pulmonary disease; EVAR, endovascular abdominal aortic aneurysm repair; IBE, iliac branch endoprosthesis; SET, snare-less, EVAR-first technique; TIA, transient ischemic attack.
Operative details are shown in Table 2. Median contrast used was 148 (120-201) mL, fluoroscopy time was 42.8 (35.0-49.8) minutes, estimated blood loss was 200 (100-275) mL, and procedure time was 192 (167-246) minutes, with no significant differences between the 2 groups. Technical success was achieved in 100% of cases. There were 2 patients in the Standard group who underwent planned brachial access. One had a prior EVAR in place and underwent IBE placement for treatment of a type 1B endoleak. The other had an open aorto-bi-iliac graft in place and had developed a large CIA pseudoaneurysm. In each of these patients, the IIA was selected and treated from the brachial artery without through-and-through femoral access. Both procedures were performed prior to development of SET for IBE. One patient in the standard group who had a previous AFX2 endograft in place from 6 years prior underwent IBE deployment per protocol via snaring a through wire.
Operative Details (Standard Technique vs SET for IBE Deployment).
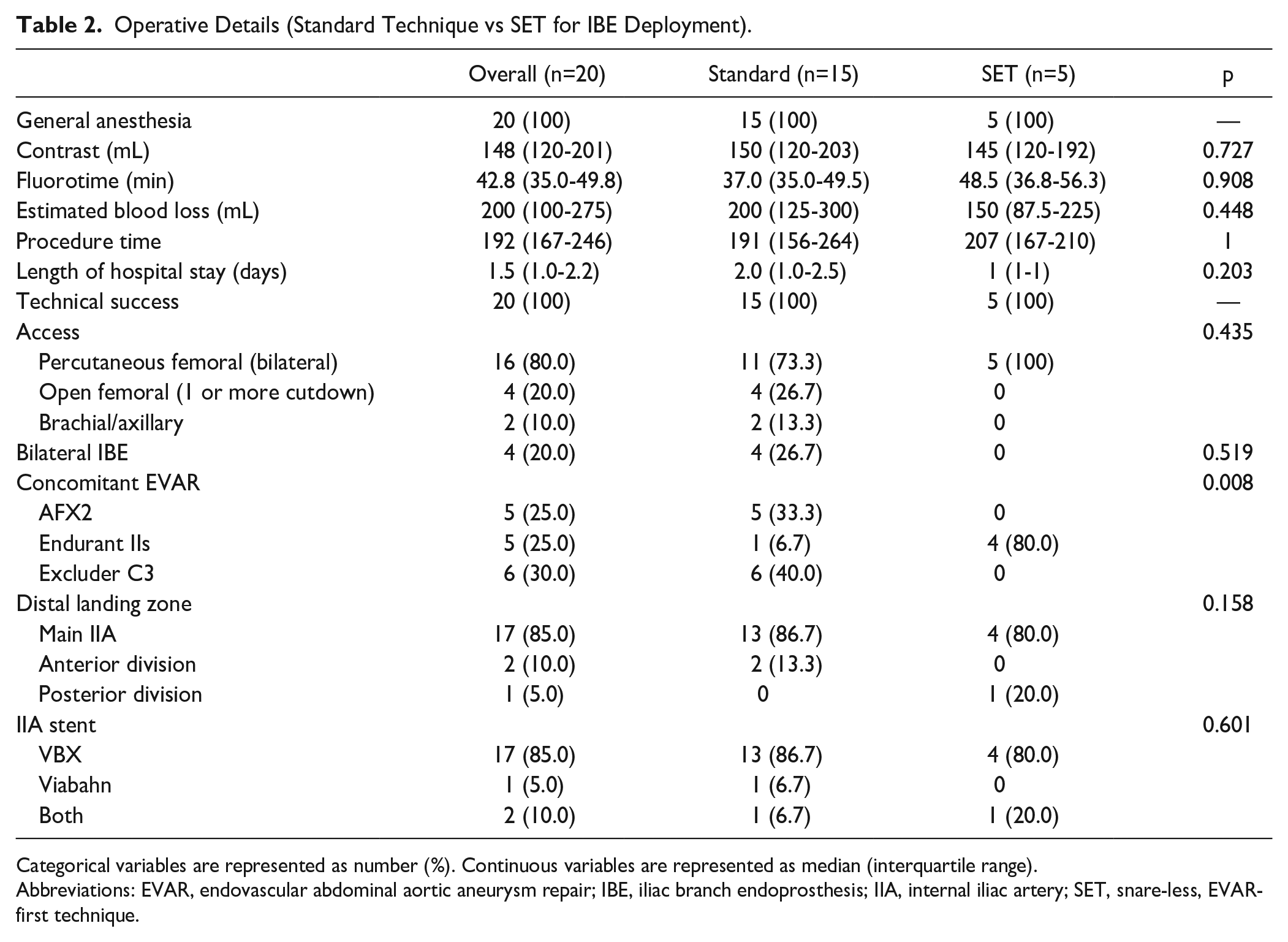
Categorical variables are represented as number (%). Continuous variables are represented as median (interquartile range).
Abbreviations: EVAR, endovascular abdominal aortic aneurysm repair; IBE, iliac branch endoprosthesis; IIA, internal iliac artery; SET, snare-less, EVAR-first technique.
In patients who underwent concomitant EVAR at the time of IBE, all SET patients received Endurant IIs endografts followed by IBE without snaring, 5 standard patients received AFX2 followed by IBE with snaring, 1 standard patient received Endurant IIs after IBE placement, and 6 standard patients received Excluder C3 after IBE placement (as recommended by the manufacturer). When the IIA was not a suitable distal landing zone, stenting was extended into either the anterior or posterior branch. The stent graft of choice for IIA stenting was VBX.
30-Day Follow-up
At 30 days, there were no mortalities or major adverse events in either group. There were 100% IIA patency, no IIA instability, and no reinterventions.
Subsequent Follow-up
Median follow-up in the SET group was 5.7 (5.5-6.2) months. One patient in the SET group died at 6 months postoperative, cause unknown. He had a CTA 1 month prior to his death demonstrating complete thrombosis of his left CIA aneurysm and patent IIA and branches with no endoleak. One patient developed a type 1B endoleak at 6 months and is scheduled for IIA limb extension. The remaining 3 patients in the SET group each have radiological follow-up of 5 to 6 months demonstrating patent IIA, no IIA instability, and no endoleaks.
Median follow-up for the Standard group was 1.6 years [IQR=0.8-2.1]. One patient developed a type 1B endoleak with CIA expansion at 3 months; however, given her worsening dementia and functional status, her family elected for hospice care. She ultimately died 3 months later, reportedly from complications related to worsening dementia. Another patient died after hemorrhagic stroke 7 months postoperative. He had a scan 1 month prior to his death which demonstrated patent IIA with no IIA endoleak. In the remaining 13 patients, there were no deaths or major adverse events within the first year. Imaging at 1 year for these surviving 13 patients demonstrated patent IIA and branches with no IIA instability. There were no reinterventions.
Discussion
SET for IBE yielded comparable results in the short term when compared to standard deployment. Technical success rates were high without increased overall procedure time, contrast usage, or fluoroscopy time. We now favor this technique for all IBE placements as it opens the applicability of IBE technology to more patients, and it eliminates the need for a through wire, decreasing the complexity of the procedure.
Heli-FX Guide
The critical piece in this technique is the use of a steerable sheath with a stiff, deflectable tip that makes a wide 180° turn—in this case, the Heli-FX Guide (originally designed for use with EndoAnchor technology). This is a 16F sheath with a 62 cm working length and a tip that is sturdy enough and wide enough to allow passage of a large VBX on a 180° turn. In our experience, the deflected tips on the Destino (Oscor, Palm Harbor, Florida) and TourGuide (Medtronic Aortic, Inc) steerable sheaths make angles that are too acute and lack adequate stiffness to allow a 7 to 8F balloon-mounted stent to stably make a sharp hairpin turn.
Benefits of EVAR Before IBE
As we have previously described, placement of an EVAR prior to IBE placement creates a “docking limb” in which to land the main body of the IBE.8,9 In the past, when placing EVAR before IBE, we limited ourselves to placement of an AFX2 endograft because it preserved the native aortic bifurcation, allowing us to proceed with snaring and standard deployment of the IBE. Patients who received this approach had to be anatomically suited for the AFX2 endograft. The purpose of through-and-through femoral access is to create a platform stiff enough to allow up-and-over advancement of a large bore sheath into the iliac side branch. In SET for IBE, with a stiff sheath tip that deflects across the aortic bifurcation to easily support wire, catheter, and stent passage, there is no further need for through- wire access. EVAR can be placed first, and the IBE landed anywhere within the iliac limb. This subsequently eliminates the renal-to-iliac bifurcation length requirement for IBE.
SET for IBE also eliminates the need for upper extremity access in cases where patients present with an EVAR already in place. While other techniques have been reported to address the challenge of groin-only access to place an IBE within a pre-existing aortic endograft, these complex solutions are not practical for routine use.11–13 For example, Dawson et al describes a “push-and-pull” maneuver that requires mating one sheath into another from opposite groins over a through wire, then moving both sheaths together as a unit to traverse the flow-divider. The technique is described in numerous panels that appear to add complexity to IBE placement. SET follows the same concept of protecting the flow-divider, done simply via a well-supported steerable sheath.
Limitations of this study include the small sample size in the SET group. While the feasibility of SET is promising in this limited study, a larger experience would further solidify our findings. In addition, our experience is exclusively with VBX and Viabahn stents. VBX is the senior author’s preferred balloon-expandable stent. Other balloon-expandable stent grafts available in the United States tend to be more rigid and less able to handle tortuosity; with non-VBX stent grafts, we have on occasion experienced separation of the stent from its mounted balloon prior to deployment. We further acknowledge that this technique does hinge on the Heli-FX, which may not be available in all countries. Finally, we add that given the novelty of the technique, available follow-up for the SET group is short, but the method of IIA stent delivery (via a snared vs non-snared platform) is unlikely to have an impact on long-term metrics for IIA stability.
Conclusions
SET for IBE is a safe and effective approach to IBE placement that decreases technical complexity. A critical component to this technique is a large bore sheath with a stiff steerable tip. Importantly, this approach also mitigates anatomic barriers to IBE placement, expanding applicability of IBE technology to patients who may be otherwise ineligible.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Naiem Nassiri is a proctor, on the advisory board and consultant for Terumo Aortic, Inc, Medtronic Aortic, Inc, and Endologix, Inc. He is also a consultant for W. L. Gore & Associates, Inc.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.