
Abstract
Background:
Venous leg ulcer (VLU) disease constitutes the most severe form of chronic venous insufficiency. We performed a network meta-analysis and meta-regression to investigate the efficacy and safety of the various available interventions in the treatment of VLU.
Methods:
We conducted a systematic research corresponding to the instructions by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement for studies reporting on surgical or endovenous interventions for the treatment of VLU. Following data extraction, we performed a Bayesian network meta-analysis and meta-regression. Primary endpoints included VLU healing and recurrence. The secondary endpoint was postintervention complications.
Results:
Seventeen studies evaluating the impact of compression monotherapy, radiofrequency ablation (RFA), endovenous laser ablation (EVLA), sclerotherapy, and saphenous vein surgery on VLU treatment, consisting of 2156 patients (2186 VLU) were included. When compared to compression monotherapy, RFA was the only treatment displaying a statistically-significant impact on ulcer healing, odds ratio (OR) 5.80 (95% credibility interval (CI): 1.08–35.07), while EVLA, RR 0.06 (95% CI: 0.00–0.57), sclerotherapy, RR 0.07 (95% CI: 0.00–0.68) and RFA, RR 0.12 (95% CI: 0.01–0.91) were the 3 interventions reducing VLU recurrence. EVLA (SUCRA, 69.65) ranked as the most efficient intervention concerning ulcer recurrence reduction. Regarding postintervention complications, EVLA was the only intervention displaying a statistically-significant increased risk compared to compression monotherapy, RR 14.3 (95% CI: 2.03–172.56). Meta-regression analysis exploring the impact of perforator treatment on VLU failed to predict healing, β = −0.27 (95% CI: −2.55 to 1.85), recurrence, β = −0.02 (95% CI: −2.96 to 2.75) and complication outcomes, β = −0.089 (95% CI: −3.13 to 2.85). During sensitivity analysis, RFA and sclerotherapy failed to sustain their effects on ulcer healing and ulcer recurrence, respectively. In addition, sclerotherapy displayed statistically-significant inferior outcomes compared to both EVLA and RFA regarding ulcer recurrence.
Conclusion:
This is the first network meta-analysis examining the effect of various interventions on VLU disease. While we have demonstrated the efficacy of RFA and ELVA in ulcer recurrence prevention, our results regarding the impact of RFA and sclerotherapy on VLU healing and recurrence, respectively, should be interpreted with caution. In addition, this review raises questions concerning the value of surgery and perforator interventions in the treatment of VLU. Further research through randomized controlled trials is required.
Clinical impact
Our review has revealed the significant efficacy of endovenous laser ablation (EVLA) and radiofrequency ablation (RFA) in effectively reducing the incidence of ulcer recurrence when compared to compression monotherapy. These outcomes hold the potential to provide relevant insights to both medical practitioners and patients, thereby informing a more prudent and enlightened decision-making approach. Such informed decisions, aimed at mitigating the recurring occurrence of venous leg ulcers, carry profound significance given the considerable socioeconomic implications associated with this medical condition.
Introduction
Venous leg ulcer (VLU) disease results from superficial and/or deep venous insufficiency (reflux and/or obstruction). It is the most severe form of chronic venous insufficiency (CVI) and the most common cause of lower limb ulceration. The lifetime risk of VLU has been estimated at 1%–2%, while its prevalence increases markedly with age. 1
Traditionally, the mainstay treatment of VLU has been compression therapy (class of recommendation: 1, level of evidence: a), with surgical interventions serving an ancillary role (class of recommendation: 2, level of evidence: c). 2 Despite its widespread use, compression therapy is associated with low levels of patient concordance, mediocre healing (ranging from 40% to 70%), and high recurrence outcomes (up to 70%), while its use is contra-indicated in patients with an ankle branchial index (ABI) of <0.6. 3
Over the past 25 years, a variety of endovenous modalities have emerged in the treatment of CVI grades 2–6, according to the CEAP classification (Clinical-Etiological-Anatomical-Pathophysiological). Endovenous ablation techniques have been found to be highly safe and effective and are now widely used instead of surgical ligation and stripping.
Although recently-published guidelines have underlined the importance of treating superficial venous reflux in regard to VLU healing (class of recommendation: 1, level of evidence: b) and recurrence (class of recommendation: 1, level of evidence: a), they have not provided guidance regarding the application of the various available interventions in terms of their effectiveness and safety. 3
In the light of these developments, we performed a network meta-analysis to investigate the safety and efficacy of various interventions in the therapy of VLU disease. In addition, we conducted a network meta-regression to explore the effect of perforator treatment on clinical and surgical outcomes.
Methods
Eligibility Criteria
We included the following studies:
Reporting on either surgical or endovenous treatment of incompetent great saphenous veins (GSV) followed by compression therapy for the treatment of CEAP 5 and 6 venous insufficiency, with or without the addition of perforator vein treatment.
Randomized control trials (RCTs) and comparative cases series (CCS) provide either raw data or Kaplan–Meier curves with number of patients at risk and number of events at time intervals.
In cases of multiple publications from the same institution, the publications with the largest number of patients were included.
We excluded studies:
Not involving ablation of GSV but describing alternative treatments such as light therapy, ointment applications, laser therapy, grafts, platelet-rich plasma, exercise.
Reporting on combined procedures in the same limb (eg, saphenofemoral junction ligation surgery and foam sclerotherapy).
Did not employ concomitant compression therapy.
Reported on additional interventions apart from surgical or endovenous vein ablation (eg, skin grafting)
Reported exclusively on perforator interventions.
Investigating treatment of VLU exclusively on diabetic patients.
Including fewer than 10 patients per treatment arm.
Holding multi-arm comparisons consequently failing to form a “closed loop” not allowing for the evaluation of the consistency assumption (open loop networks are inconsistent by definition). 4
Information Sources and Search Strategy
We conducted a systematic review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and the PRISMA for Network Meta-Analyses (PRISMA-NMA) extension (Supplementary Figure 1—PRISMA Flow Diagram). 5 Two investigators, V.B. and A.B., independently conducted a systematic search on Scopus, Medline (via PubMed), and Web of Science for articles published by May 2022. We used a structured vocabulary with keywords. There were neither language nor demographic limitations (Supplementary Table 1—Search strategy).
Selection and Data Collection Process
V.B. and A.B. evaluated the titles and abstracts of publications returned by the search. Publications that met the inclusion criteria were obtained in their entirety and analyzed by both researchers utilizing the same terms. Additional literature items were sought by closely studying the references of the retrieved studies and relevant systematic reviews. Where there was a disagreement regarding a publication, a consensus was reached through discussion with a third researcher, A.K.
Data Items
Primary endpoints included VLU healing at a median follow-up of 12 months (range 1–60) and ulcer recurrence at a median follow-up of 16.4 months (range 6–61). The secondary endpoint included postoperative complications. VLU healing was defined as complete reepithelization of the leg without visual evidence of skin discontinuity by the end of follow-up. Ulcer recurrence was defined as any break in the skin between the knee and the malleolus following ulcer healing by the end of follow-up.
Complications included surgical site infection, lymphorea, hematoma, thrombophlebitis, nerve injury, skin burns, skin necrosis, visual disturbances, dyspnea, and deep vein thrombosis (DVT).
Effect Measures and Synthesis Methods
We conducted a Bayesian network meta-analysis utilizing the Markov chain Monte Carlo simulation with vague priors. We implemented the generalized linear model with 4 chains, burn-ins of 50 000 iterations followed by 100 000 iterations with 10 000 adaptations. Network geometry was assessed using network plots with the size of the nodes being proportional to the number of subjects included in the intervention and the thickness of the arms corresponding to the number of the included studies in the comparison. Model selection between fixed and random effect models was based on leverage plot examination and the evaluation of the deviance information criterion (DIC). Model convergence was evaluated employing trace and Gelman-Rubin-Brooks plot examination. Model inconsistency was assessed using leverage and posterior deviance plots, DIC calculations, and the node-splitting technique where p values ≤0.05 signified statistically-significant differences between direct and indirect evidence. Studies introducing severe amounts of inconsistency in the model consequently resulting in violation of the inconsistency and transitivity assumptions were excluded successively according to their corresponding p values until the model reached consistency. NMA outcomes were displayed using league table heatmaps as either odds ratios (OR) or risk ratios (RR) accompanied by their corresponding 95% credibility intervals (CIs). While RR and OR are distinct measures of effect and they are not to be confused with one another, they are both valid methods of presenting intervention outcomes. We proceeded to effect estimate selection, aspiring to maximize clinical relevance. In that spirit, ulcer healing was presented as the odds of the event occurring (healing) while ulcer recurrence and complication outcomes were presented as the risk of experiencing the event. Intervention rankings were processed employing the surface under the cumulative ranking (SUCRA) score, while they were visualized using SUCRA plots. We performed a network meta-regression using perforator interventions as a covariate and exchangeable treatment-interaction model priors. Meta-regression model choice and Markov Chain Monte Carlo algorithm parameters were similar for both network meta-analysis and meta-regression. Regression results were presented through regression line plots.6,7
The risk of bias for the included studies was assessed by 2 researchers, V.B. and A.B., using the Risk of Bias in Non-Randomized Studies—of Interventions (ROBINS-I) and the revised Cochrane risk-of-bias tool for randomized trials.8,9 Disagreements between the 2 investigators were resolved through consultation with a third reviewer, A.K. We performed 2 types of sensitivity analysis for all outcomes. One excluding all studies displaying high, serious, and critical risk of bias and one excluding all non-RCTs (including only RCTs).
Results
Baseline Study Characteristics
Seventeen studies, 8 RCTs, 2 prospective comparative studies, and 7 retrospective comparative case series including 2186 VLUs (2156 patients) met the inclusion criteria.10–26 The included studies featured 5 interventions. Four studies compared surgery to compression, 3 compression to sclerotherapy, 3 sclerotherapy to endovenous laser ablation (EVLA), 2 EVLA to radiofrequency ablation (RFA), 3 surgery to RFA, 1 compression to RFA, 1 compression to EVLA, 1 RFA to sclerotherapy, and 1 surgery to sclerotherapy (Table 1).
Baseline Study Characteristics.
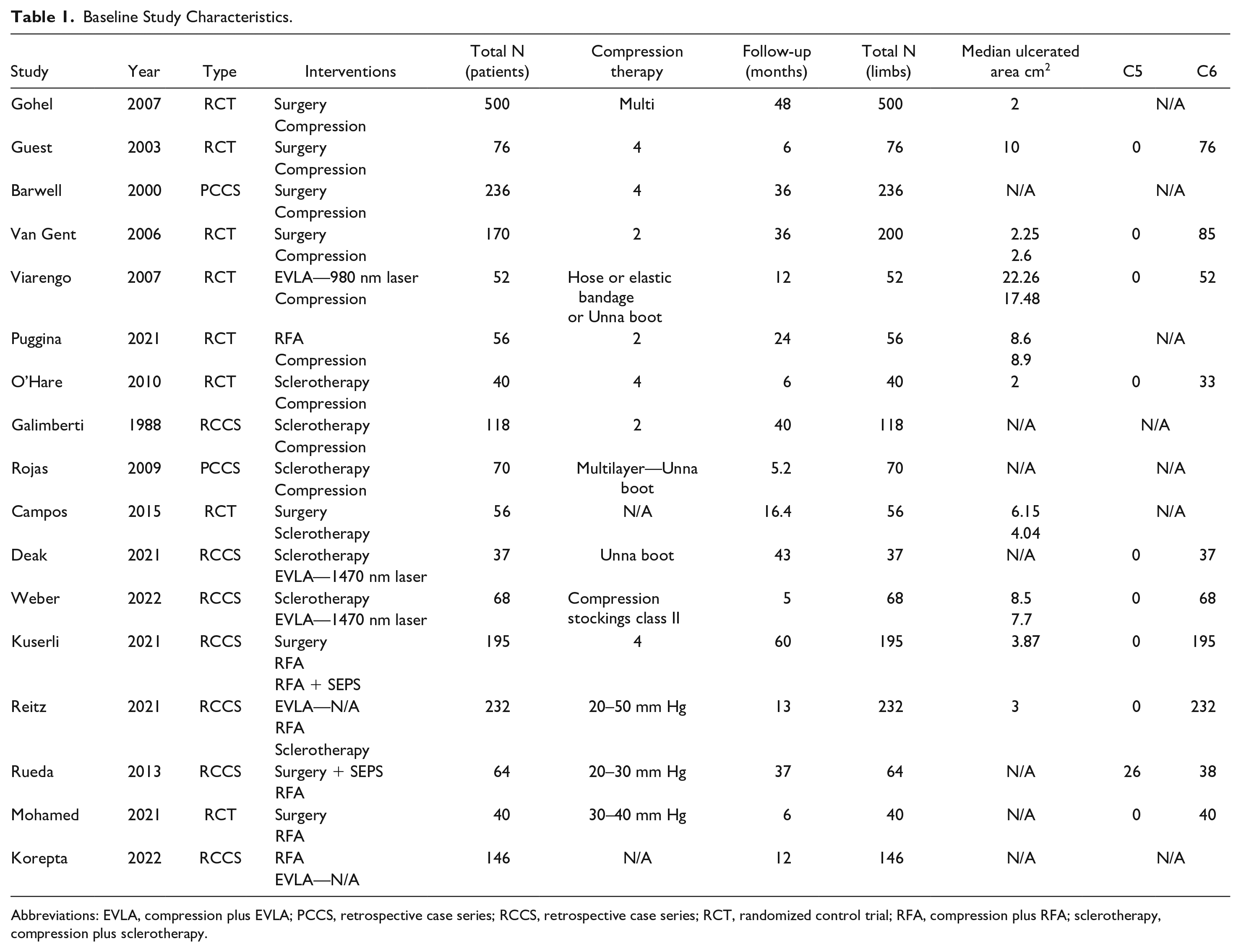
Abbreviations: EVLA, compression plus EVLA; PCCS, retrospective case series; RCCS, retrospective case series; RCT, randomized control trial; RFA, compression plus RFA; sclerotherapy, compression plus sclerotherapy.
Risk of Bias
The overall risk of bias for the included RCTs was low to moderate with 2 of 7 studies portraying a high risk of bias.10,11,13–16,19,25 The overall risk of bias for comparative studies was moderate to high, with 3 of 10 studies displaying a serious risk of bias and 1 study introducing a critical risk of bias to the analysis12,17,18,20–24,26 (Supplementary Figures 2 and 3).
Network Meta-Analysis
Following DIC values and leverage plot analyses, we implemented random effects model network meta-analysis for all 3 endpoints.
VLU Healing
The VLU healing network included 16 studies with 2130 VLU (Figure 1A).10–13,15–26 RFA, OR 5.80 (95% CI: 1.08–35.07), was the only intervention displaying statistically significantly improved healing outcomes compared with compression monotherapy (Figure 2). SUCRA probability ranking for interventions most likely to benefit ulcer healing ranked RFA as first (SUCRA, 58.26), followed by sclerotherapy (SUCRA, 22.12) and EVLA (SUCRA, 17.69) (Supplementary Figure 4). Meta-regression analysis failed to display a statistically-significant relationship between ulcer healing and perforator treatment, β = −0.27 (95% CI: −2.55 to 1.85) (Supplementary Figure 5A).
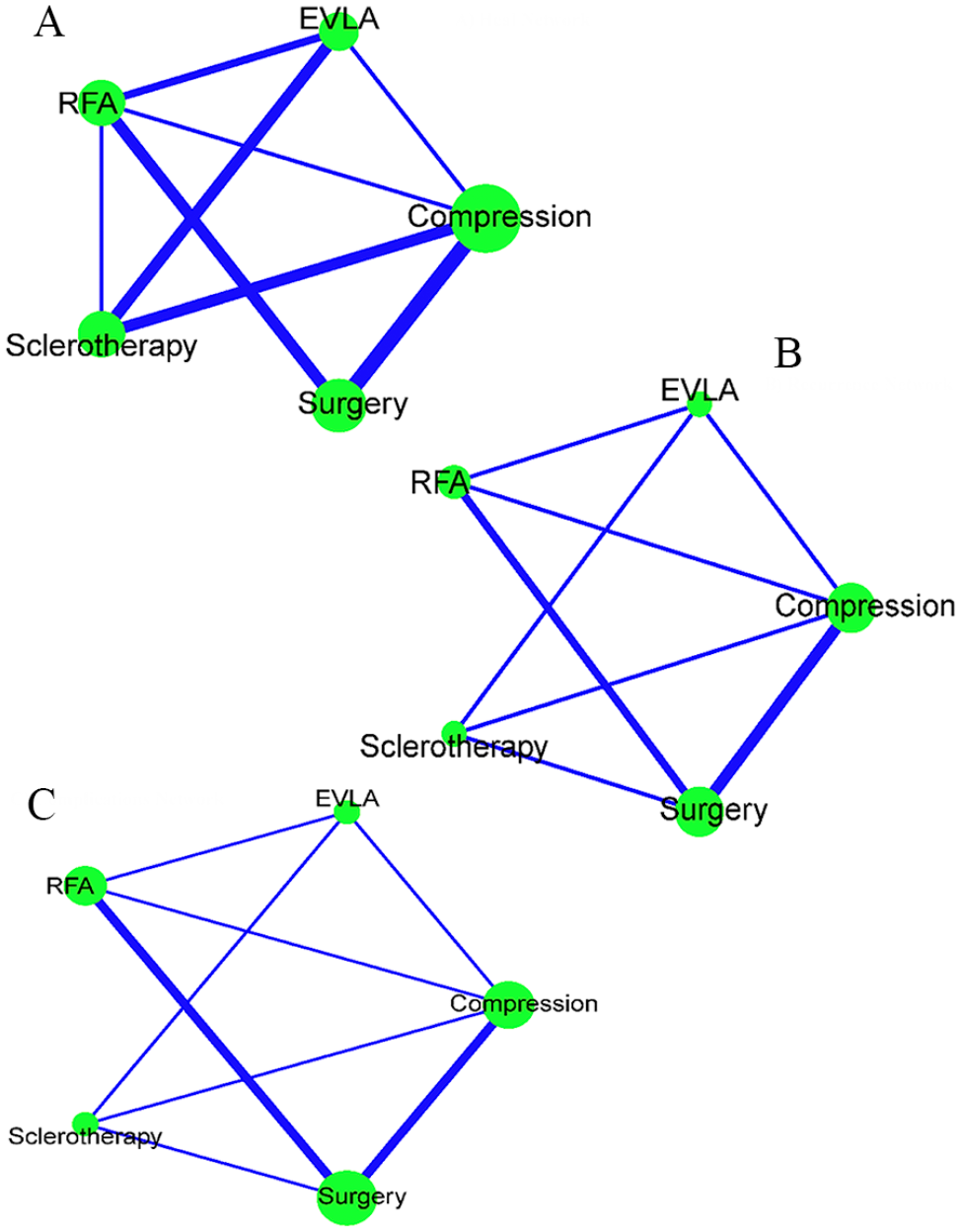
(A) Heal network, (B) recurrence network, and (C) complications network.
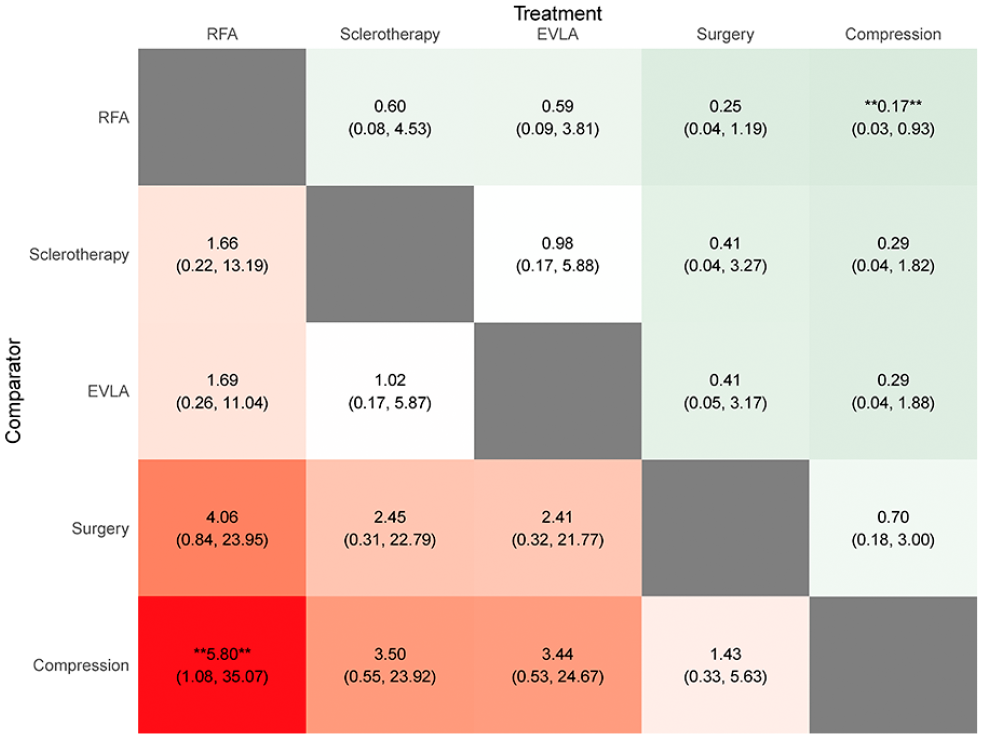
League table odds ratio (OR) heal rate—the values in each cell represent the relative treatment effect and 95% credible intervals of the treatment on the top, compared with the treatment on the left. A double asterisk indicates statistical significance.
VLU Recurrence
The VLU recurrence network included 12 studies and 1728 VLU (Figure 1B).10,12–17,19,21,22,24,26 When compared to compression monotherapy EVLA, RR 0.06 (95% CI: 0.00–0.57), RFA, RR 0.12 (95% CI: 0.01–0.91), and sclerotherapy, RR 0.07 (95% CI: 0.00–0.68) significantly reduced the risk of VLU recurrence (Figure 3). SUCRA probability ranking ranked EVLA (SUCRA, 69.65) first, sclerotherapy (SUCRA, 16.02) second, and RFA (SUCRA, 13.19) third as the interventions most likely to reduce VLU recurrence (Figure 4A). Regression analysis displayed a nonstatistically-significant relationship between perforator treatment and VLU recurrence, β = −0.02 (95% CI: −2.96 to 2.75) (Supplementary Figure 5B).
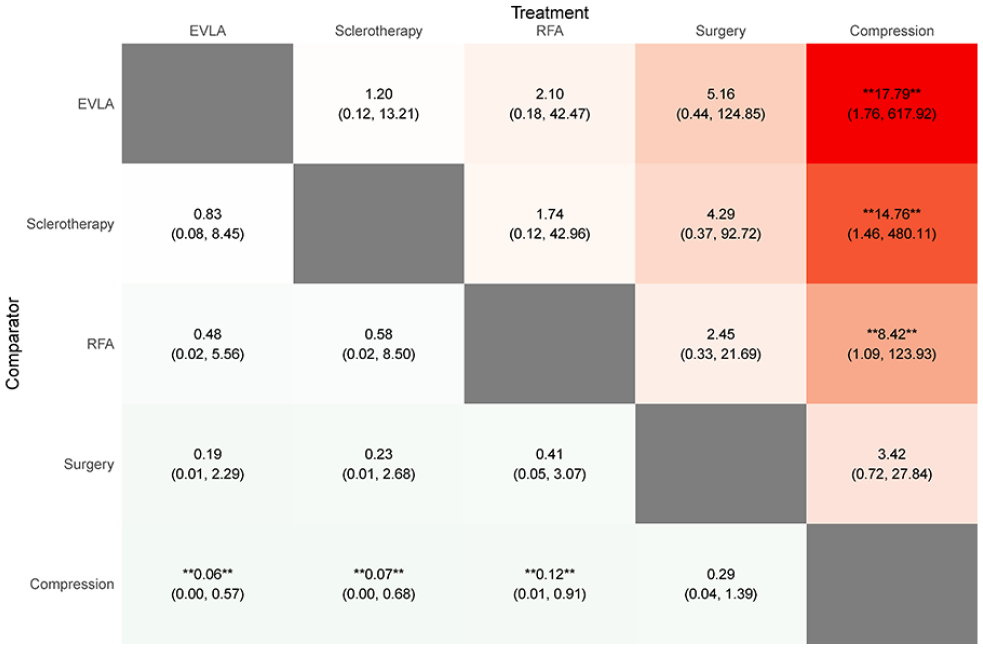
League table risk ratio (RR) ulcer recurrence—The values in each cell represent the relative treatment effect and 95% credible intervals of the treatment on the top, compared to the treatment on the left. A double asterisk indicates statistical significance.
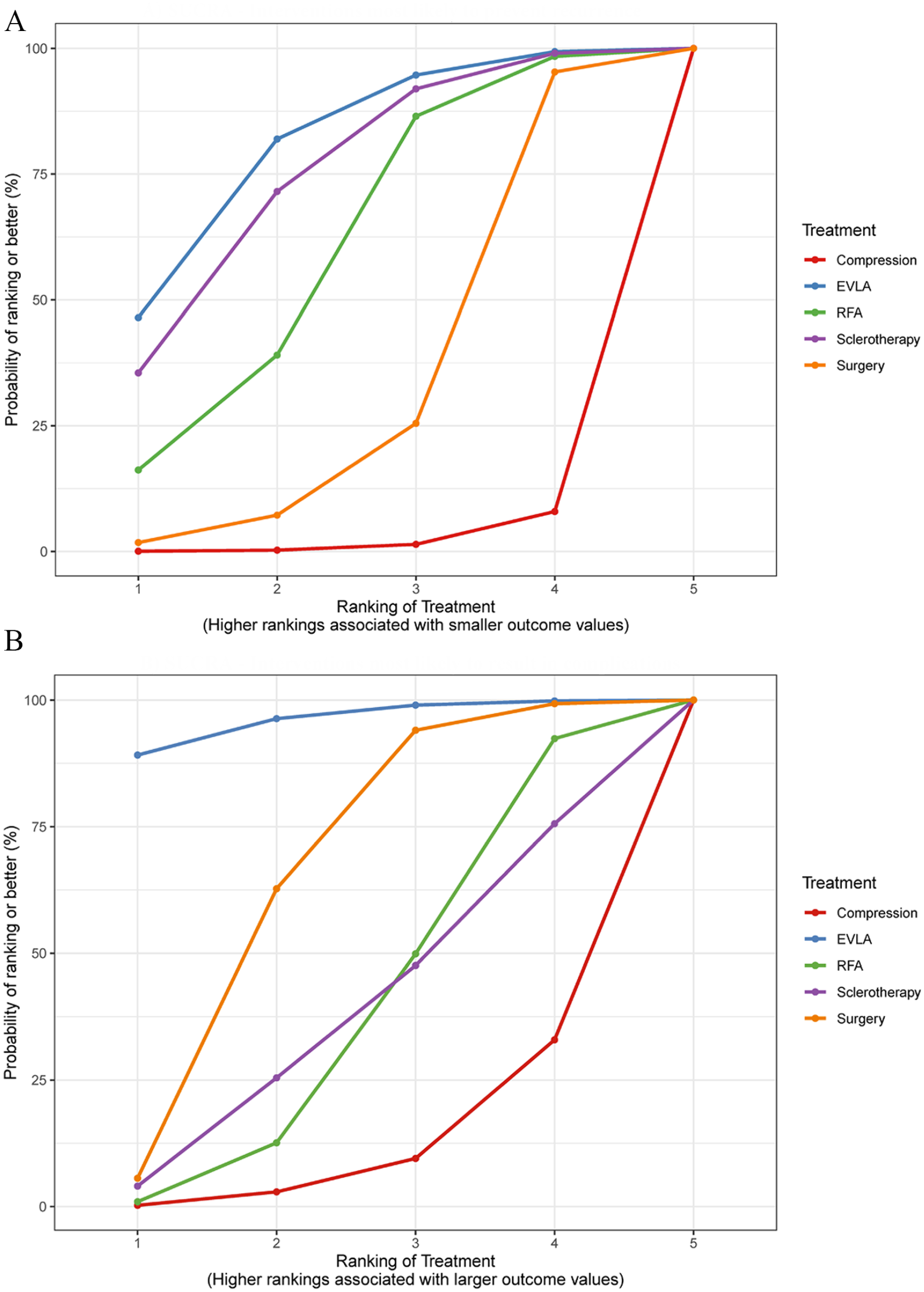
(A) Surface under the cumulative ranking curve (SUCRA) recurrence. (B) Surface under the cumulative ranking curve (SUCRA) complications.
Complications
The complications network comprised 12 studies including 1529 patients (Figure 1C).10–12,14–16,19,21,22,24–26 EVLA displayed a statistically-significant increased risk for postintervention complications compared to both compression therapy RR 14.3 (95% CI: 2.03–172.56) and RFA RR 6.51 (95% CI: 1.02–85.59), (Figure 5). SUCRA rankings, classified EVLA (SUCRA, 89.13), surgery (SUCRA, 5.61), and sclerotherapy (SUCRA, 4.06) as the 3 interventions most likely to result in complications (Figure 4B). The regression model did not display a statistically-significant relationship between perforator interventions and complications, β = −0.089 (95% CI: −3.13 to 2.85) (Supplementary Figure 5C).
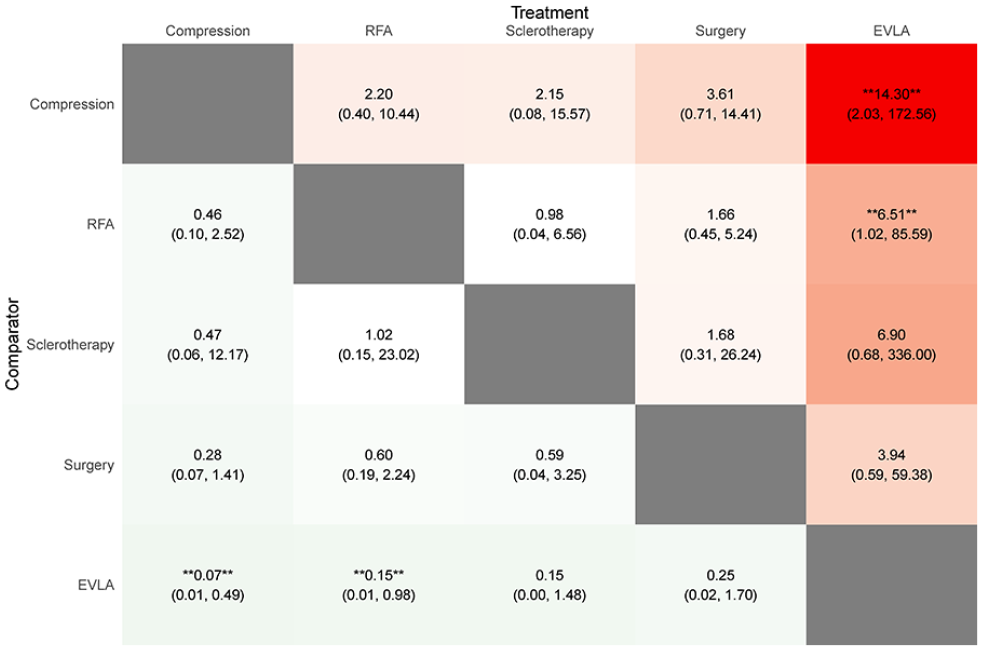
League table risk ratio (RR) complications—The values in each cell represent the relative treatment effect and 95% credible intervals of the treatment on the top, compared to the treatment on the left. A double asterisk indicates statistical significance.
Sensitivity Analysis
During sensitivity analysis, the exclusion of high-risk bias studies produced consistent networks for all 3 outcomes. While the statistically-significant superior outcomes of RFA compared to compression monotherapy did not persist, both EVLA and RFA sustained their statistically-significant effect on ulcer recurrence reduction. In addition, EVLA remained the only intervention potentially increasing the likelihood of post-intervention complications. Interestingly, and while sclerotherapy failed to retain its effect on ulcer recurrence, it additionally displayed statistically-significant inferior outcomes regarding ulcer healing and ulcer recurrence compared to both EVLA and RFA. Sensitivity analysis, including only RCT, produced open-loop networks for which the consistency assumption could not be assessed, not allowing for further inferences to be made (Supplementary Table 2—Sensitivity analysis).
Discussion
Our analysis has displayed improved healing outcomes for RFA compared to compression monotherapy, with an OR of 5.80. EVLA (RR 0.06), sclerotherapy (RR 0.07), and RFA (RR 0.12) significantly reduced VLU recurrence. EVLA was the intervention most likely to reduce recurrence (SUCRA, 69.65), followed by sclerotherapy (SUCRA, 16.02) and RFA (SUCRA, 13.19). Patients undergoing EVLA plus compression therapy for VLU were about 14 times more likely (RR 14.3) to experience postintervention complications compared to compression alone while they faced an almost sevenfold increased risk when compared to RFA (RR 6.51). All 3 regression models regarding healing, recurrence and complications failed to display a statistically-significant relationship between perforator treatment and outcomes. Sensitivity analysis displayed a failure of both RFA and sclerotherapy to sustain their effect on ulcer healing and ulcer recurrence, respectively.
VLU disease is a complex pathophysiological entity. Applying various forms of compression therapy to diminish ambulatory venous hypertension (AVH) has served as the primary treatment for VLU. However, the often-poor patient compliance has led to mediocre healing rates, while the temporary alleviation of venous hypertension fails to address the problem at its core, resulting in high recurrence rates. 27 Surgical and endovenous interventions aim for the durable mitigation of AVH through the abolition of superficial reflux, but debate continues as to the preferred methods and procedures.
The first RCT investigating the impact of superficial venous surgery on VLU healing, published almost 20 years ago, did not manage to establish a therapeutic relationship. 11 A more recently-published RCT replicated the outcomes of earlier research, as it also failed to demonstrate any improvement in VLU healing through the incorporation of superficial venous surgery alongside compression therapy. 10 Our results are in line with these findings confirming the nonsignificant impact of surgery (ligation and/or stripping of saphenous vein) on ulcer healing compared to conservative therapy. In addition, none of the included studies comparing sclerotherapy plus compression to compression monotherapy displayed statistically-significant differences between the two in terms of healing outcomes.
Regarding EVLA and RFA, a void in high-quality studies investigating their role in ulcer healing is apparent. Our review included 2 studies comparing EVLA and RFA with compression monotherapy. Although the one study showed improved VLU healing outcomes for EVLA at 12 months (81.5% for EVLA versus 24% compression only) this result portrayed a high degree of disagreement between direct and indirect evidence during node-splitting (p<0.01), while the study itself carried a high risk of bias. 14 The second study investigating the efficacy of RFA did not showcase an improvement in VLU healing following RFA treatment. While our analysis displayed a statistically-significant impact of RFA on VLU healing, the borderline statistically-significant result (95% CI: 1.08–35.07) accompanied by the sensitivity analysis outcomes, where RFA failed to sustain its positive impact on healing, produces skepticism about the true effect of RFA on VLU healing pressing for a cautious reading of these results. 15 Ultimately, our analysis which encompassed ulcer sizes ranging from 2 to 22.26 cm2, was unable to determine the potential effect of ulcer size on ulcer healing outcomes due to the limited data presented (only 5 studies reported on specific ulcer area measurements).
In contrast to VLU healing, the beneficial effect of superficial venous interventions on VLU recurrence is widely known, with contemporary guidelines issuing recommendations that mirror this reality (class of recommendation: 1, level of evidence: a). The present study suggests a nearly 90% risk reduction in VLU recurrence for EVLA, RFA, or sclerotherapy when compared to compression monotherapy. While EVLA displayed both the highest risk reduction and the highest SUCRA score, nonstatistically-significant differences between the 3 interventions were observed. The one intervention that failed to significantly reduce ulcer recurrence was saphenous vein ligation and/or stripping. Although 2 of the 3 studies (all of which had a low risk of bias) comparing surgery to compression displayed a significant reduction in recurrence following surgery, surgical group recurrence estimates were considerable. This pattern of non-negligible recurrence was evident through the entire spectrum of comparisons involving surgery.10,12 As it is well documented, recurrence following superficial venous surgery for the treatment of venous insufficiency can be significant, ranging from 40 to 80%. The high recurrence outcomes observed in superficial venous surgery, which are widely attributed to neovascularization, could serve in elucidating our results.28,29
While several disease-specific characteristics, such as ulcer surface dimensions, type of compression, and disease duration, have been previously identified as influential in ulcer healing following compression therapy, it is crucial to consider the impact of follow-up duration as an important parameter. Notably, the reported 6-month compression therapy healing rates which vary widely and range from 35 to 75% escalate to up to 92% by 12 months of follow-up.30–32 The above information may aid in the interpretation of the seemingly contradictory outcomes of the primary and sensitivity analyses where RFA and sclerotherapy have displayed inconsistency regarding healing and recurrence outcomes, respectively.
In our study among the 9 studies investigating compression monotherapy, 4 had a mean follow-up duration of up to 12 months (3 up to 6 months), whereas only 2 of the 6 studies examining RFA interventions reported a follow-up duration of up to 12 months (1 up to 6 months).
During the sensitivity analysis, 3 of the 4 studies focusing on short-term compression outcomes were excluded. Furthermore, one RFA study with an average follow-up duration of 37 months was also excluded due to high risk of bias ultimately ensuring a more balanced comparison concerning follow-up duration between the 2 interventions. Consequently, the findings derived from the primary analysis potentially indicate an inclination toward a swifter healing trajectory illustrated by RFA interventions, characterized by a greater proportion of ulcer healing within a shorter follow-up duration as compared to compression. This observation implies that the superiority of RFA stems from its capacity to expedite the healing process, rather than signifying its overall efficacy to be significantly higher. Moreover, this hypothesis aligns with prior research that has documented accelerated healing rates for endovenous interventions in general and RFA in particular when compared to compression monotherapy.15,33
Similarly, within the subset of 7 studies evaluating sclerotherapy, 3 studies had a follow-up duration limited to 6 months imposing constraints on the comprehensive assessment of ulcer recurrence. However, during sensitivity analysis, 2 of the 3 studies with short-term follow-up were excluded (due to high risk of bias). This exclusion ultimately enabled an ulcer recurrence estimation within a more realistic timeframe.
Of the 5 interventions included in our network, only EVLA was associated with a significant increase in complications compared to both compression monotherapy and RFA. Although our analysis was not stratified based on potential complications, our findings are in agreement with a recently-published network meta-analysis. The analysis reported an elevated risk of post-intervention paresthesia and pigmentation induration, along with higher levels of intra-operative pain, associated with the implementation of EVLA. 34 Further along, an RCT comparing RFA to EVLA, including 450 patients, demonstrated a significant increase in adverse event occurrence (including pain) between RFA and EVLA of 41.8% versus 70.5%. 35 In our definition of postoperative complications, we decided to proceed with the inclusion of only objective adverse events, thus excluding pain from the endpoint.
Despite the aforementioned findings it is of importance to underline that the inferiority of EVLA to RFA demonstrated by our model should be interpreted with caution. The lack of direct evidence (one study of low bias comparing EVLA to RFA) portrayed by the wide confidence intervals and the borderline statistical significance (95% CI: 1.02–85.9) prevents the extraction of definite conclusions. On the other hand, the safety of RFA is apparent since it ranked as the safest intervention, second only to compression monotherapy.
Given the lack of available evidence, most guidelines only provide limited support in the treatment of perforators for VLU disease (class of recommendation: IIb, level of evidence: c). However, Gent et al in their study of 94 lesions treated with ligation, stripping, and subfascial endoscopic perforator surgery (SEPS), displayed statistically-significant differences favoring perforator surgery. Similarly, in a recently-published RCT where RFA was employed, authors demonstrated a 2-year ulcer recurrence estimate of 12.9% for treated perforators versus 33.3% for untreated (p≤0.004).36,37
In our review, 9 studies including 1063 patients treated incompetent perforators utilizing a variety of techniques ranging from RFA and EVLA to sclerotherapy and SEPS. Although all 3 regression models failed to identify a relationship between outcomes and the treatment of perforators, the recurrence regression model suggested a tendency toward a lower risk of ulcer recurrence with the treatment of perforators.
Limitations
The major limitation of our study is the scarcity of direct comparisons, which resulted in wide confidence intervals. Moreover, in an effort to present statistically robust results, we excluded one-arm comparisons in favor of examining and realizing the consistency and transitivity assumptions, leaving out a study comparing Conservatrice Hémodynamique de l’Insuffisance Veineuse en Ambulatoire (CHIVA) to compression. One study investigating EVLA versus surgery and one study investigating surgery versus compression were also removed from the heal rate endpoint analysis due to their substantial contribution to inconsistency.19,38,39 The EVLA versus surgery study reported solely on healing rate outcomes and consequently was removed altogether from the review. Additional potential sources of bias are the inclusion of both RCTs and comparative studies (7 retrospective studies) as well as our failure to incorporate gray literature exploration in our search protocol. Last, we were unable to identify comparable studies describing the application of nonthermal ablation methods (cyanoacrylate glue and mechanochemical ablation) in the treatment of VLU, and as a result, these novel modalities are not included in this review.
Conclusion
While we have demonstrated the efficacy of RFA and ELVA in ulcer recurrence prevention, our results regarding the impact of RFA and sclerotherapy on VLU healing and recurrence respectively should be interpreted with caution. Albeit this review raises questions concerning the value of both saphenous vein surgery and perforator treatment in VLU, we have observed a trend toward recurrence risk reduction following perforator interventions. Further research is warranted through randomized controlled trials.
Supplemental Material
sj-docx-6-jet-10.1177_15266028231193978 – Supplemental material for A Systematic Review Network Meta-Analysis and Meta-Regression on Surgical and Endovenous Interventions for the Treatment of Lower Limb Venous Ulcer Disease
Supplemental material, sj-docx-6-jet-10.1177_15266028231193978 for A Systematic Review Network Meta-Analysis and Meta-Regression on Surgical and Endovenous Interventions for the Treatment of Lower Limb Venous Ulcer Disease by Vangelis Bontinis, Kiriakos Ktenidis, Alkis Bontinis, Andreas Koutsoumpelis, Constantine N Antonopoulos, Argirios Giannopoulos, Vasileios Rafailidis, Angeliki Chorti and Andrew W Bradbury in Journal of Endovascular Therapy
Supplemental Material
sj-docx-7-jet-10.1177_15266028231193978 – Supplemental material for A Systematic Review Network Meta-Analysis and Meta-Regression on Surgical and Endovenous Interventions for the Treatment of Lower Limb Venous Ulcer Disease
Supplemental material, sj-docx-7-jet-10.1177_15266028231193978 for A Systematic Review Network Meta-Analysis and Meta-Regression on Surgical and Endovenous Interventions for the Treatment of Lower Limb Venous Ulcer Disease by Vangelis Bontinis, Kiriakos Ktenidis, Alkis Bontinis, Andreas Koutsoumpelis, Constantine N Antonopoulos, Argirios Giannopoulos, Vasileios Rafailidis, Angeliki Chorti and Andrew W Bradbury in Journal of Endovascular Therapy
Supplemental Material
sj-tif-1-jet-10.1177_15266028231193978 – Supplemental material for A Systematic Review Network Meta-Analysis and Meta-Regression on Surgical and Endovenous Interventions for the Treatment of Lower Limb Venous Ulcer Disease
Supplemental material, sj-tif-1-jet-10.1177_15266028231193978 for A Systematic Review Network Meta-Analysis and Meta-Regression on Surgical and Endovenous Interventions for the Treatment of Lower Limb Venous Ulcer Disease by Vangelis Bontinis, Kiriakos Ktenidis, Alkis Bontinis, Andreas Koutsoumpelis, Constantine N Antonopoulos, Argirios Giannopoulos, Vasileios Rafailidis, Angeliki Chorti and Andrew W Bradbury in Journal of Endovascular Therapy
Supplemental Material
sj-tiff-2-jet-10.1177_15266028231193978 – Supplemental material for A Systematic Review Network Meta-Analysis and Meta-Regression on Surgical and Endovenous Interventions for the Treatment of Lower Limb Venous Ulcer Disease
Supplemental material, sj-tiff-2-jet-10.1177_15266028231193978 for A Systematic Review Network Meta-Analysis and Meta-Regression on Surgical and Endovenous Interventions for the Treatment of Lower Limb Venous Ulcer Disease by Vangelis Bontinis, Kiriakos Ktenidis, Alkis Bontinis, Andreas Koutsoumpelis, Constantine N Antonopoulos, Argirios Giannopoulos, Vasileios Rafailidis, Angeliki Chorti and Andrew W Bradbury in Journal of Endovascular Therapy
Supplemental Material
sj-tiff-3-jet-10.1177_15266028231193978 – Supplemental material for A Systematic Review Network Meta-Analysis and Meta-Regression on Surgical and Endovenous Interventions for the Treatment of Lower Limb Venous Ulcer Disease
Supplemental material, sj-tiff-3-jet-10.1177_15266028231193978 for A Systematic Review Network Meta-Analysis and Meta-Regression on Surgical and Endovenous Interventions for the Treatment of Lower Limb Venous Ulcer Disease by Vangelis Bontinis, Kiriakos Ktenidis, Alkis Bontinis, Andreas Koutsoumpelis, Constantine N Antonopoulos, Argirios Giannopoulos, Vasileios Rafailidis, Angeliki Chorti and Andrew W Bradbury in Journal of Endovascular Therapy
Supplemental Material
sj-tiff-4-jet-10.1177_15266028231193978 – Supplemental material for A Systematic Review Network Meta-Analysis and Meta-Regression on Surgical and Endovenous Interventions for the Treatment of Lower Limb Venous Ulcer Disease
Supplemental material, sj-tiff-4-jet-10.1177_15266028231193978 for A Systematic Review Network Meta-Analysis and Meta-Regression on Surgical and Endovenous Interventions for the Treatment of Lower Limb Venous Ulcer Disease by Vangelis Bontinis, Kiriakos Ktenidis, Alkis Bontinis, Andreas Koutsoumpelis, Constantine N Antonopoulos, Argirios Giannopoulos, Vasileios Rafailidis, Angeliki Chorti and Andrew W Bradbury in Journal of Endovascular Therapy
Supplemental Material
sj-tiff-5-jet-10.1177_15266028231193978 – Supplemental material for A Systematic Review Network Meta-Analysis and Meta-Regression on Surgical and Endovenous Interventions for the Treatment of Lower Limb Venous Ulcer Disease
Supplemental material, sj-tiff-5-jet-10.1177_15266028231193978 for A Systematic Review Network Meta-Analysis and Meta-Regression on Surgical and Endovenous Interventions for the Treatment of Lower Limb Venous Ulcer Disease by Vangelis Bontinis, Kiriakos Ktenidis, Alkis Bontinis, Andreas Koutsoumpelis, Constantine N Antonopoulos, Argirios Giannopoulos, Vasileios Rafailidis, Angeliki Chorti and Andrew W Bradbury in Journal of Endovascular Therapy
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.